
Intravenous Tranexamic Acid Has Benefit for Reducing Blood Loss after Open-Wedge High Tibial Osteotomy: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Methods
2.1. Surgical Technique
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, H.J.; Shin, J.Y.; Lee, H.J.; Park, K.H.; Jung, C.H.; Kyung, H.S. Can medial stability be preserved after open wedge high tibial osteotomy? Knee Surg. Relat. Res. 2020, 32, 51. [Google Scholar] [CrossRef]
- Na, Y.G.; Lee, B.K.; Choi, J.U.; Lee, B.H.; Sim, J.A. Change of joint-line convergence angle should be considered for accurate alignment correction in high tibial osteotomy. Knee Surg. Relat. Res. 2021, 33, 4. [Google Scholar] [CrossRef]
- Ogbemudia, A.O.; Bafor, A.; West-Osemwengie, L. Reactionary haemorrhage reduction with adrenaline infiltration in proximal tibial osteotomy: A randomized clinical study of safety and efficacy. Arch. Orthop. Trauma Surg. 2012, 132, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Jung, K.H.; Chang, S.W.; Jang, S.M.; Park, K.B. Trends in knee surgery research in the official journal of the Korean Knee Society during the period 1999–2018: A bibliometric review. Knee Surg. Relat. Res. 2020, 32, 28. [Google Scholar] [CrossRef] [PubMed]
- Suh, D.W.; Kyung, B.S.; Han, S.B.; Cheong, K.; Lee, W.H. Efficacy of Tranexamic Acid for Hemostasis in Patients Undergoing High Tibial Osteotomy. J. Knee Surg. 2018, 31, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Pape, D.; Dueck, K.; Haag, M.; Lorbach, O.; Seil, R.; Madry, H. Wedge volume and osteotomy surface depend on surgical technique for high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.; Liu, J.; Zhang, J.; Jiang, J.; Dang, X.; Shi, Z. Tranexamic acid is beneficial for blood management of high tibial osteotomy: A randomized controlled study. Arch. Orthop. Trauma Surg. 2020. [Google Scholar] [CrossRef]
- Palanisamy, J.V.; Das, S.; Moon, K.H.; Kim, D.H.; Kim, T.K. Intravenous Tranexamic Acid Reduces Postoperative Blood Loss After High Tibial Osteotomy. Clin. Orthop. Relat. Res. 2018, 476, 2148–2154. [Google Scholar] [CrossRef]
- Duivenvoorden, T.; van Diggele, P.; Reijman, M.; Bos, P.K.; van Egmond, J.; Bierma-Zeinstra, S.M.A.; Verhaar, J.A.N. Adverse events and survival after closing- and opening-wedge high tibial osteotomy: A comparative study of 412 patients. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 895–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.B.; In, Y.; Oh, K.J.; Song, K.Y.; Yun, S.T.; Jang, K.M. Complications Associated With Medial Opening-Wedge High Tibial Osteotomy Using a Locking Plate: A Multicenter Study. J. Arthroplast. 2019, 34, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.S.; Kim, O.G.; Seo, J.H.; Kim, D.H.; Kim, Y.G.; Lee, I.S. Complications and Short-Term Outcomes of Medial Opening Wedge High Tibial Osteotomy Using a Locking Plate for Medial Osteoarthritis of the Knee. Knee Surg. Relat. Res. 2016, 28, 289–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodacre, T.; Ricketts, M.; Evans, J.T.; Pavlou, G.; Schranz, P.; Hockings, M.; Toms, A. Complications associated with opening wedge high tibial osteotomy—A review of the literature and of 15 years of experience. Knee 2016, 23, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Giber, D.; Dubory, A.; Auregan, J.C. Safety of simultaneous versus staged bilateral opening-wedge high tibial osteotomy with locked plate and immediate weight bearing. Int. Orthop. 2020, 44, 109–117. [Google Scholar] [CrossRef]
- Kim, K.I.; Kim, H.J.; Kim, G.B.; Bae, S.H. Tranexamic acid is effective for blood management in open-wedge high tibial osteotomy. Orthop. Traumatol. Surg. Res. 2018, 104, 1003–1007. [Google Scholar] [CrossRef]
- Bjerke-Kroll, B.T.; Sculco, P.K.; McLawhorn, A.S.; Christ, A.B.; Gladnick, B.P.; Mayman, D.J. The increased total cost associated with post-operative drains in total hip and knee arthroplasty. J. Arthroplast. 2014, 29, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Hill, G.E.; Frawley, W.H.; Griffith, K.E.; Forestner, J.E.; Minei, J.P. Allogeneic blood transfusion increases the risk of postoperative bacterial infection: A meta-analysis. J. Trauma 2003, 54, 908–914. [Google Scholar] [CrossRef]
- Eubanks, J.D. Antifibrinolytics in major orthopaedic surgery. J. Am. Acad. Orthop. Surg. 2010, 18, 132–138. [Google Scholar] [CrossRef]
- Gillette, B.P.; Kremers, H.M.; Duncan, C.M.; Smith, H.M.; Trousdale, R.T.; Pagnano, M.W.; Sierra, R.J. Economic impact of tranexamic acid in healthy patients undergoing primary total hip and knee arthroplasty. J. Arthroplast. 2013, 28, 137–139. [Google Scholar] [CrossRef]
- Henry, D.A.; Carless, P.A.; Moxey, A.J.; O’Connell, D.; Stokes, B.J.; Fergusson, D.A.; Ker, K. Anti-fibrinolytic use for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst. Rev. 2011, Cd001886. [Google Scholar]
- Kagoma, Y.K.; Crowther, M.A.; Douketis, J.; Bhandari, M.; Eikelboom, J.; Lim, W. Use of antifibrinolytic therapy to reduce transfusion in patients undergoing orthopedic surgery: A systematic review of randomized trials. Thromb. Res. 2009, 123, 687–696. [Google Scholar] [CrossRef]
- Zufferey, P.J.; Miquet, M.; Quenet, S.; Martin, P.; Adam, P.; Albaladejo, P.; Mismetti, P.; Molliex, S. Tranexamic acid in hip fracture surgery: A randomized controlled trial. Br. J. Anaesth. 2010, 104, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.C.; Byun, S.J. High tibial osteotomy. Knee Surg. Relat. Res. 2012, 24, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisawa, Y.; Masuhara, K.; Shiomi, S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop. Clin. N. Am. 1979, 10, 585–608. [Google Scholar] [CrossRef]
- Kim, M.S.; Son, J.M.; Koh, I.J.; Bahk, J.H.; In, Y. Intraoperative adjustment of alignment under valgus stress reduces outliers in patients undergoing medial opening-wedge high tibial osteotomy. Arch. Orthop. Trauma Surg. 2017, 137, 1035–1045. [Google Scholar] [CrossRef] [PubMed]
- Lobenhoffer, P.; Agneskirchner, J.D. Improvements in surgical technique of valgus high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2003, 11, 132–138. [Google Scholar] [CrossRef]
- Konig, G.; Hamlin, B.R.; Waters, J.H. Topical tranexamic acid reduces blood loss and transfusion rates in total hip and total knee arthroplasty. J. Arthroplast. 2013, 28, 1473–1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadler, S.B.; Hidalgo, J.H.; Bloch, T. Prediction of blood volume in normal human adults. Surgery 1962, 51, 224–232. [Google Scholar]
- Bilbao, A.; Martín-Fernández, J.; Arenaza, J.; García, I.; Tomás-García, N.; Trujillo-Martín, E.; García-Perez, L. Validation of the EQ-5D-5L in patients with hip or knee osteoarthritis. Value Health 2017, 20, A760. [Google Scholar] [CrossRef]
- Carson, J.L.; Guyatt, G.; Heddle, N.M.; Grossman, B.J.; Cohn, C.S.; Fung, M.K.; Gernsheimer, T.; Holcomb, J.B.; Kaplan, L.J.; Katz, L.M.; et al. Clinical Practice Guidelines From the AABB: Red Blood Cell Transfusion Thresholds and Storage. JAMA 2016, 316, 2025–2035. [Google Scholar] [CrossRef]
- Viberg, B.; Gundtoft, P.H.; Schønnemann, J.; Pedersen, L.; Andersen, L.R.; Titlestad, K.; Madsen, C.F.; Lauritsen, J.; Overgaard, S. Introduction of national guidelines for restrictive blood transfusion threshold for hip fracture patients—A consecutive cohort study based on complete follow-up in national databases. J. Orthop. Surg. Res. 2018, 13, 116. [Google Scholar] [CrossRef]
- Kim, M.S.; Koh, I.J.; Lee, S.Y.; In, Y. Central sensitization is a risk factor for wound complications after primary total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3419–3428. [Google Scholar] [CrossRef]
- Bradley, K.E.; Ryan, S.P.; Penrose, C.T.; Grant, S.A.; Wellman, S.S.; Attarian, D.E.; Green, C.L.; Risoli, T., Jr.; Bolognesi, M.P. Tranexamic acid or epsilon-aminocaproic acid in total joint arthroplasty? A randomized controlled trial. Bone Jt. J. 2019, 101-b, 1093–1099. [Google Scholar]
- Stowers, M.D.J.; Aoina, J.; Vane, A.; Poutawera, V.; Hill, A.G.; Munro, J.T. Tranexamic Acid in Knee Surgery Study-A Multicentered, Randomized, Controlled Trial. J. Arthroplast. 2017, 32, 3379–3384. [Google Scholar] [CrossRef] [PubMed]
- Tsukada, S.; Kurosaka, K.; Nishino, M.; Maeda, T.; Hirasawa, N.; Matsue, Y. Intraoperative Intravenous and Intra-Articular Plus Postoperative Intravenous Tranexamic Acid in Total Knee Arthroplasty: A Placebo-Controlled Randomized Controlled Trial. J. Bone Jt. Surg. Am. 2020, 102, 687–692. [Google Scholar] [CrossRef]
- Choi, Y.; Koo, J.; Moon, S.W.; Yang, Y.; Son, J. Long-term Follow-up of Patellar Nonresurfacing in Total Knee Arthroplasty. Clin. Orthop. Surg. 2020, 12, 49–54. [Google Scholar] [CrossRef]
- Chon, J.; Jeon, T.; Yoon, J.; Jung, D.; An, C.-H. Influence of Patellar Tilt Angle in Merchant View on Postoperative Range of Motion in Posterior Cruciate Ligament-Substituting Fixed-Bearing Total Knee Arthroplasty. Clin. Orthop. Surg. 2019, 11, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Shin, W.C.; Song, M.K.; Han, H.-S.; Lee, M.C.; Ro, D.H. Which orally administered antithrombotic agent is most effective for preventing venous thromboembolism after total knee arthroplasty? A propensity score-matching analysis. Knee Surg. Relat. Res. 2021, 33, 10. [Google Scholar] [CrossRef]
- Lee, H.I.; Park, D.; Cho, J. Clinical and Radiological Results with Second-Look Arthroscopic Findings after Open Wedge High Tibial Osteotomy without Arthroscopic Procedures for Medial Meniscal Root Tears. Knee Surg. Relat. Res. 2018, 30, 34–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, O.S.; Lee, E.S.; Lee, Y.S. Disparity between Preoperative Target Correction Amount and Postoperative Correction Amount in Open Wedge High Tibial Osteotomy. Knee Surg. Relat. Res. 2019, 31, 126–131. [Google Scholar] [PubMed]
- Noh, J.H.; Kim, N.Y.; Song, K.I. Intraoperative patellar maltracking and postoperative radiographic patellar malalignment were more frequent in cases of complete medial collateral ligament release in cruciate-retaining total knee arthroplasty. Knee Surg. Relat. Res. 2021, 33, 9. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.H.; Oh, H.C.; Park, S.H.; Kim, J.K.; Kim, S.H. Does Obesity Affect Clinical and Radiological Outcomes in Minimally Invasive Total Knee Arthroplasty? Minimum 5-Year Follow-up of Minimally Invasive TKA in Obese Patients. Clin. Orthop. Surg. 2018, 10, 315–321. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | TXA Group (n = 37) | Control Group (n = 36) | p-Value |
|---|---|---|---|
| Age, mean (SD), y | 54.9 (9.2) | 55.3 (7.0) | 0.852 |
| Sex | 0.844 | ||
| Male | 10 (27.0%) | 9 (25.0%) | |
| Female | 27 (73.0%) | 27 (75.0%) | |
| Body mass index, mean (SD) | 26.1 (3.1) | 26.0 (5.3) | 0.96 |
| Comorbidities | |||
| Hypertension | 15 (40.5%) | 14 (38.9%) | 0.885 |
| Diabetes | 5 (13.5%) | 5 (13.9%) | 0.963 |
| Brain | 0 (0%) | 0 (0%) | 1 |
| Thyroid | 2 (5.6%) | 0 (0%) | 0.146 |
| Kidney | 0 (0%) | 1 (2.8%) | 0.307 |
| Lung | 1 (2.7%) | 0 (0%) | 0.321 |
| Smoking | 6 (16.2%) | 1 (2.8%) | 0.051 |
| Alcohol | 2 (5.4%) | 2 (5.6%) | 0.978 |
| ASA score | 0.254 | ||
| 1 | 10 (27.0%) | 14 (38.9%) | |
| 2 | 26 (70.3%) | 19 (52.8%) | |
| 3 | 1 (2.7%) | 3 (8.3%) | |
| KL grade | 0.832 | ||
| 2 | 15 (41.7%) | 14 (38.9%) | |
| 3 | 20 (55.6%) | 20 (55.6%) | |
| 4 | 1 (2.8%) | 2 (5.6%) | |
| Preoperative mechanical axis (MA, °) | Varus 6.9 (2.6) | Varus 6.7 (3.6) | 0.754 |
| Preoperative weight bearing line (%) | 17.0 (11.8) | 19.2 (14.9) | 0.477 |
| Postoperative MA (°) | Valgus 2.8 (2.6) | Valgus 2.6 (1.9) | 0.637 |
| Postoperative WBL (%) | 61.6 (7.0) | 60.9 (9.0) | 0.745 |
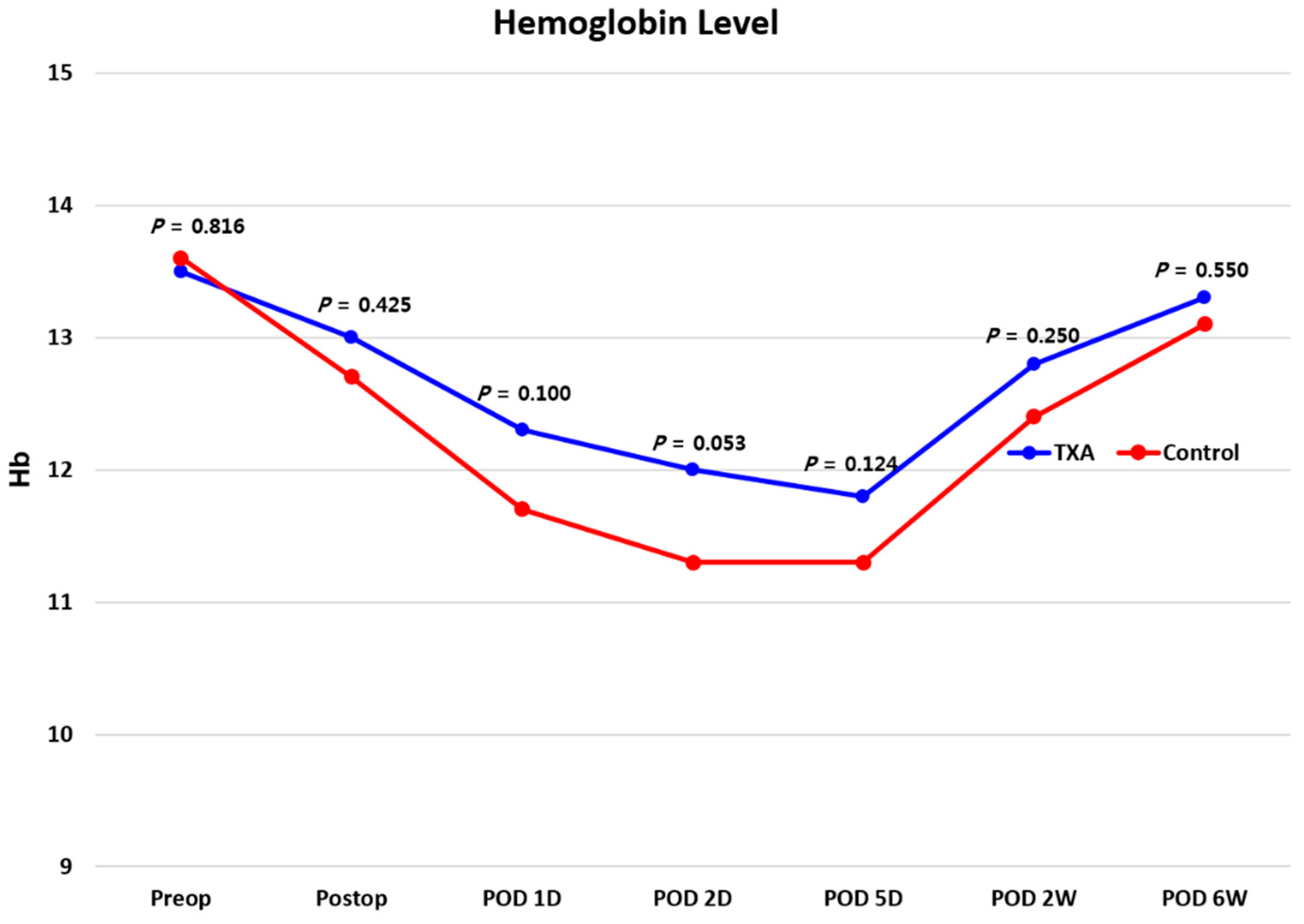
| Preoperative hemoglobin (d/dL) | 13.5 (1.3) | 13.6 (1.8) | 0.904 |
| Preoperative Hematocrit (%) | 40.9 (3.6) | 40.7 (5.2) | 0.848 |
| Preoperative blood platelet (×109/L) | 264.8 (58.8) | 243.7 (69.5) | 0.166 |
| Preoperative activated partial thromboplastin time (s) | 27.0 (2.3) | 27.4 (2.9) | 0.475 |
| TXA Group (n = 37) | Control Group (n = 36) | p-Value | |
|---|---|---|---|
| Drain output (mL) 0–24 h | 87.5 (101.1) | 225.7 (136.2) | <0.001 |
| Drain output (mL) 24–72 h | 83.3 (49.7) | 102.4 (104.7) | 0.326 |
| Total drain output (mL) | 170.8 (122.2) | 328.0 (194.0) | <0.001 |
| Total blood loss (mL) | 470.9 (236.0) | 739.3 (314.4) | <0.001 |
| Hemoglobin decrease | |||
| Preoperation to immediately postoperation | 0.5 (0.6) | 0.9 (0.7) | 0.008 |
| Preoperation to 1 day postoperation | 1.2 (0.8) | 1.9 (0.8) | 0.001 |
| Preoperation to 2 days postoperation | 1.5 (0.7) | 2.4 (1.0) | <0.001 |
| Preoperation to 5 days postoperation | 1.7 (0.9) | 2.4 (1.1) | 0.007 |
| TXA Group (n = 37) | Control Group (n = 36) | p-Value | |
|---|---|---|---|
| Wound complication | |||
| Wound dehiscence | 1 (2.7%) | 1 (2.8%) | 0.984 |
| Hematoma aspiration | 0 (0%) | 0 (0%) | 1.000 |
| Drainage occurring after day 5 postoperation | 0 (0%) | 1 (2.8%) | 0.307 |
| Suture granuloma | 0 (0%) | 0 (0%) | 1.000 |
| Additional antibiotics for redness | 0 (0%) | 1 (2.8%) | 0.984 |
| Superficial surgical-site infection | 1 (2.7%) | 0 (0%) | 0.321 |
| Authors | Group | No. of Patients | Total Blood Loss (mL) | Total Drainage Volume (mL) | Hemoglobin Reduction (Pre to Postoperative 2 Days) (g/dL) | Transfusion | Deep Vein Thrombosis | Wound Complication |
|---|---|---|---|---|---|---|---|---|
| Suh et al. [5] | TXA | 15 | 246.0 | 1.7 | NR | NR | 0 (0%) | |
| (2018) | Control | 15 | 377.2 | 1.2 | NR | NR | 1 (6.7%) | |
| Ni et al. [7] | TXA | 50 | 477.9 | 282.3 | 2.6 | 0 (0%) | 0 (0%) | 0 (0%) |
| (2020) | Control | 50 | 834.6 | 413.2 | 3.3 | 1 (2%) | 0 (0%) | 2 (4%) |
| Palanisamy et al. [8] | TXA | 66 | 372.0 | 315.0 | 1.3 | 0 (0%) | 0 (0%) | 0 (0%) |
| (2018) | Control | 86 | 635.0 | 537.0 | 2.2 | 0 (0%) | 0 (0%) | 2 (2.3%) |
| Kim et al. [14] | TXA | 77 | 502.4 | 269.3 | 2.3 | 0 (0%) | 0 (0%) | NR |
| (2018) | Control | 75 | 882.7 | 330.4 | 3.2 | 2 (2.6%) | 0 (0%) | NR |
| Our study (2021) | TXA | 37 | 470.9 | 170.8 | 1.5 | 0 (0%) | 23 (62.2%) | 2 (5.4%) |
| Control | 36 | 739.3 | 328.0 | 2.4 | 0 (0%) | 15 (41.7%) | 3 (8.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.-S.; Koh, I.-J.; Sung, Y.-G.; Park, D.-C.; Ha, W.-J.; In, Y. Intravenous Tranexamic Acid Has Benefit for Reducing Blood Loss after Open-Wedge High Tibial Osteotomy: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 3272. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153272
Kim M-S, Koh I-J, Sung Y-G, Park D-C, Ha W-J, In Y. Intravenous Tranexamic Acid Has Benefit for Reducing Blood Loss after Open-Wedge High Tibial Osteotomy: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(15):3272. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153272
Chicago/Turabian StyleKim, Man-Soo, In-Jun Koh, Yong-Gyu Sung, Dong-Chul Park, Won-Jun Ha, and Yong In. 2021. "Intravenous Tranexamic Acid Has Benefit for Reducing Blood Loss after Open-Wedge High Tibial Osteotomy: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 15: 3272. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153272