
Airway Abnormalities in Adult Mucopolysaccharidosis and Development of Salford Mucopolysaccharidosis Airway Score

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Assessment
2.4. SMAS
3. Results
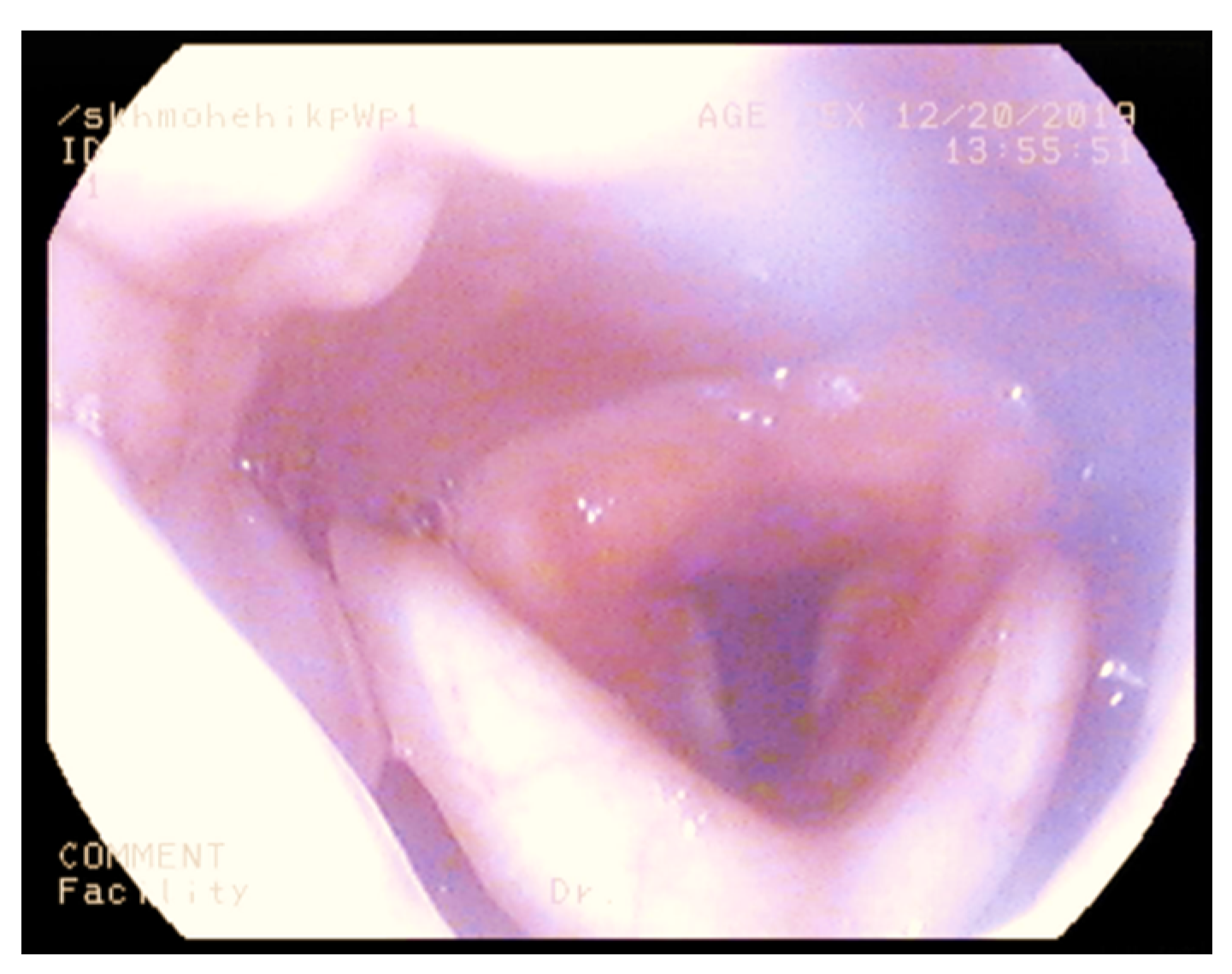
3.1. Nasendoscopy
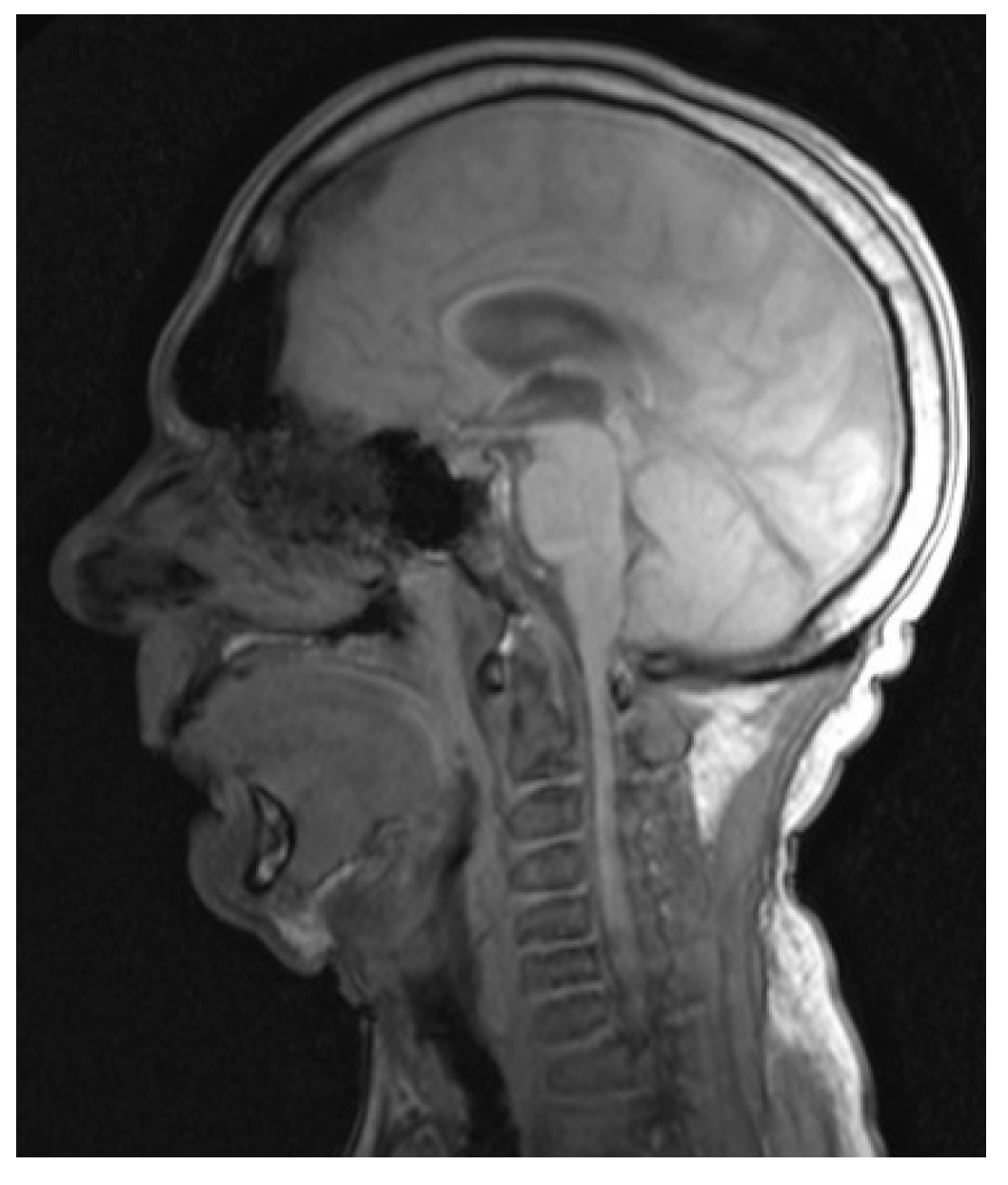
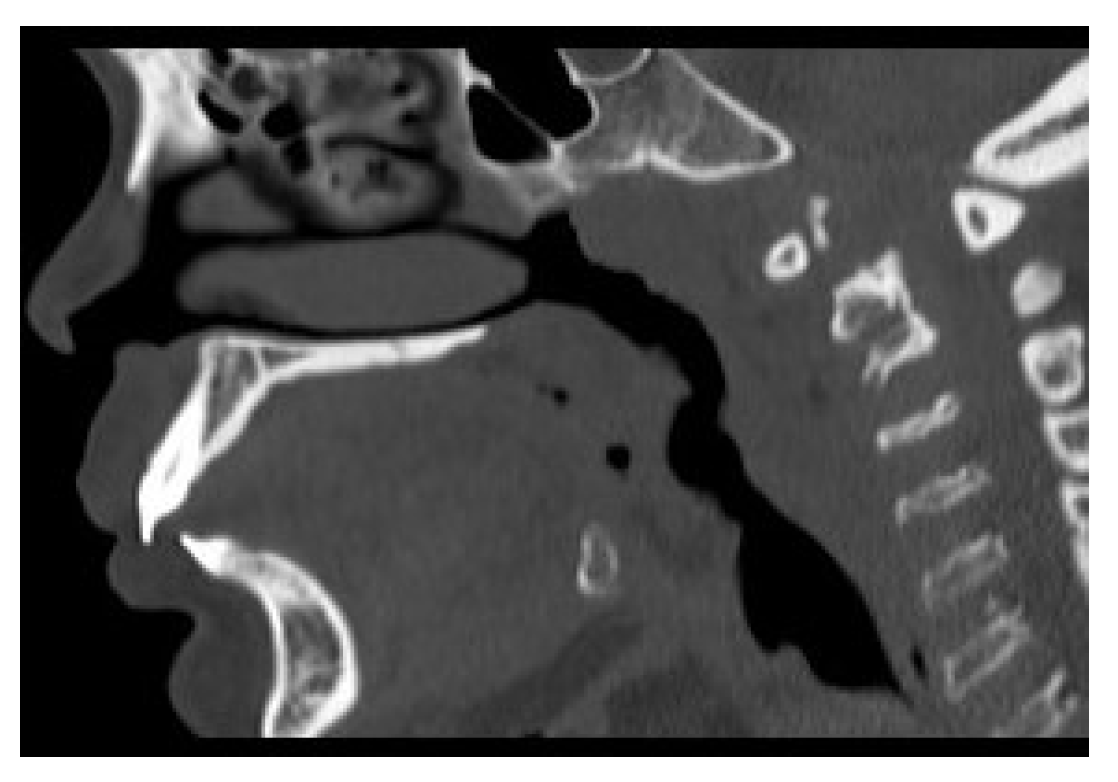
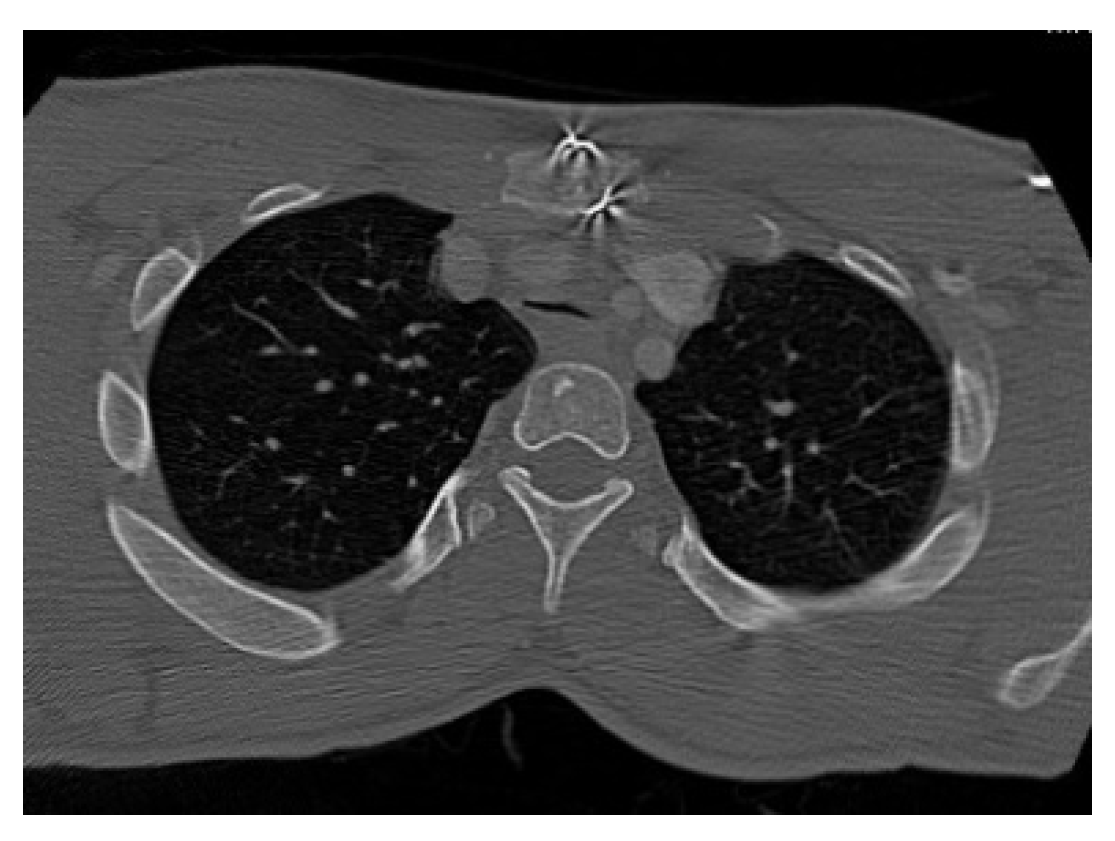
3.2. Cross-Sectional Imaging
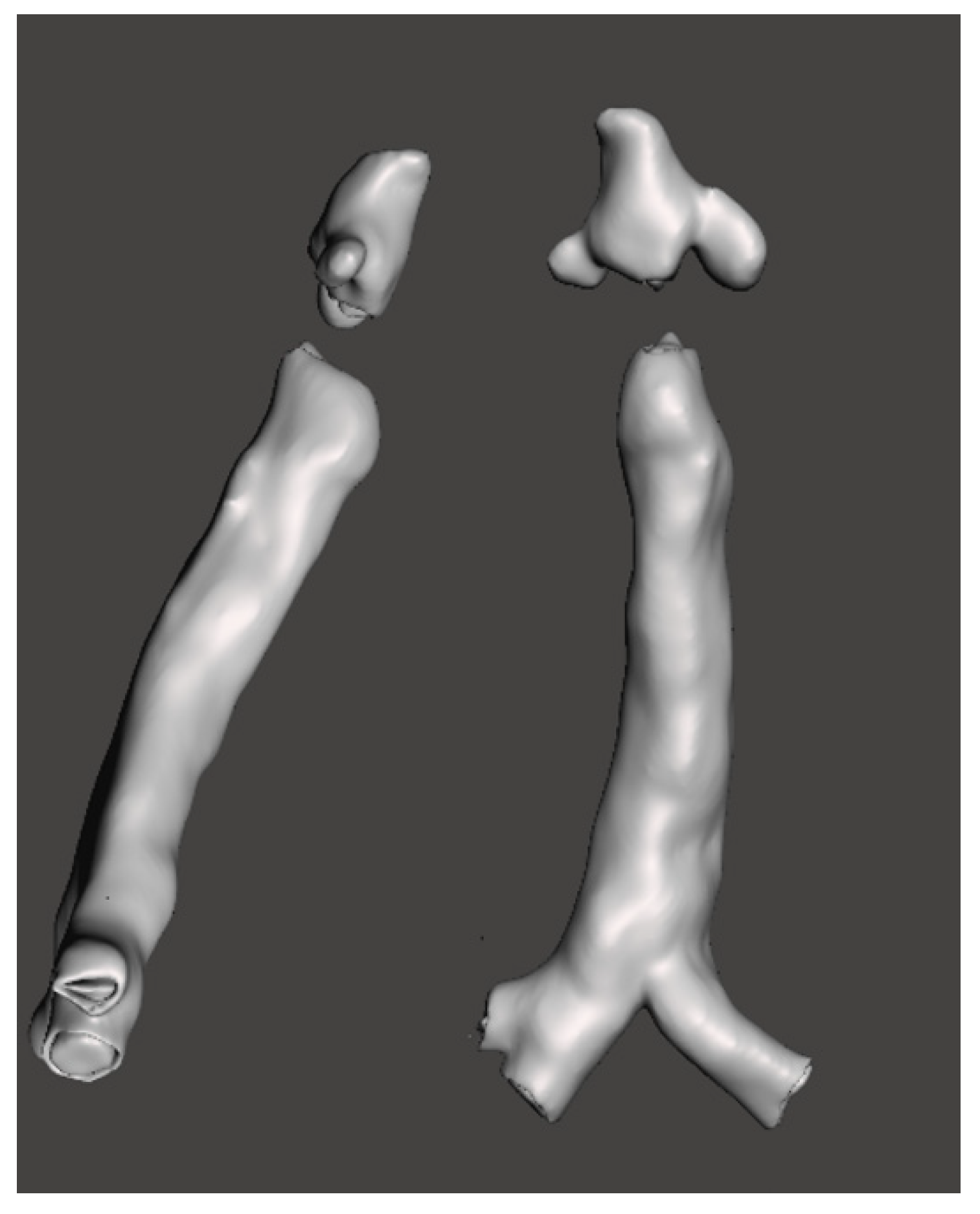
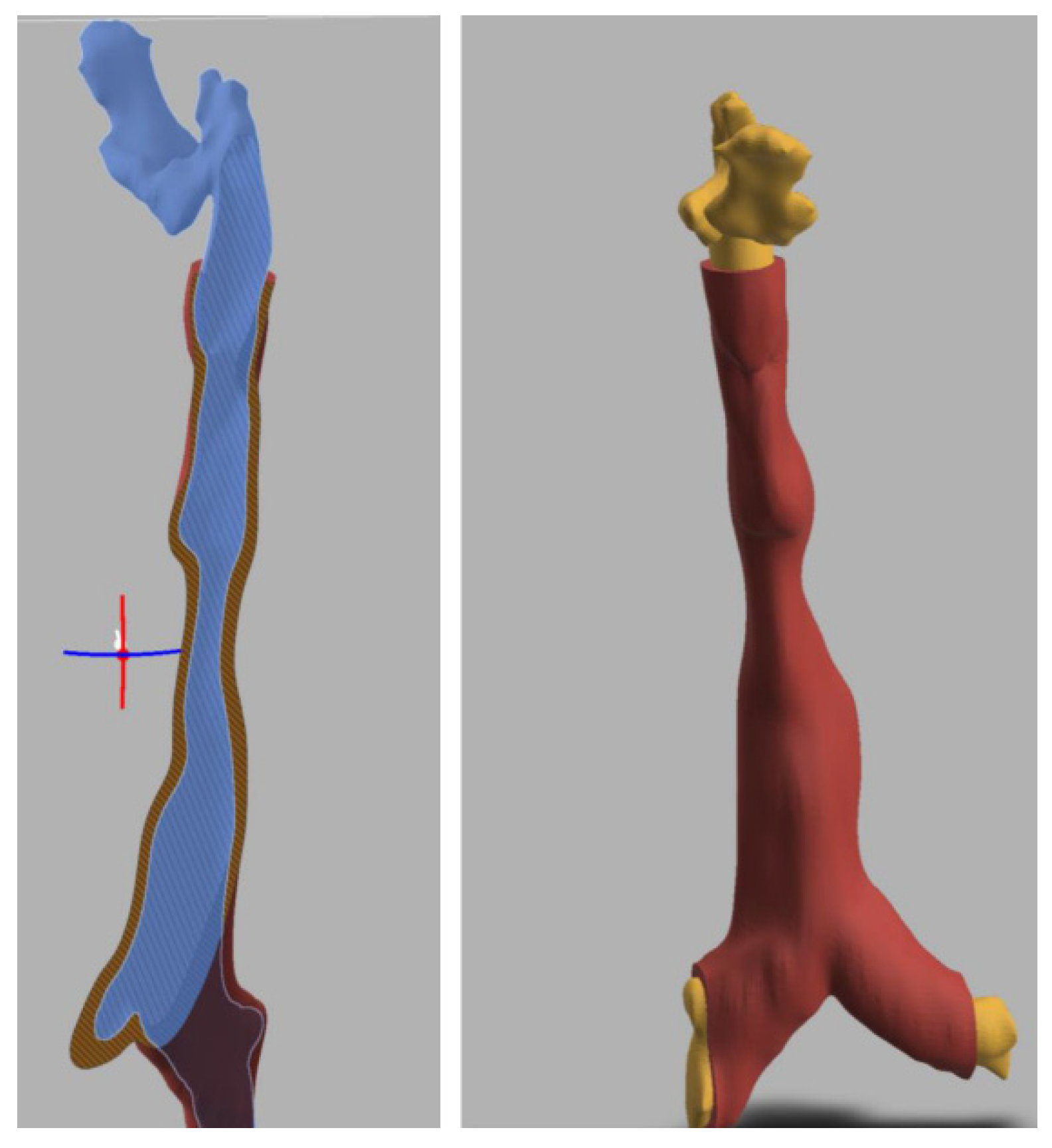
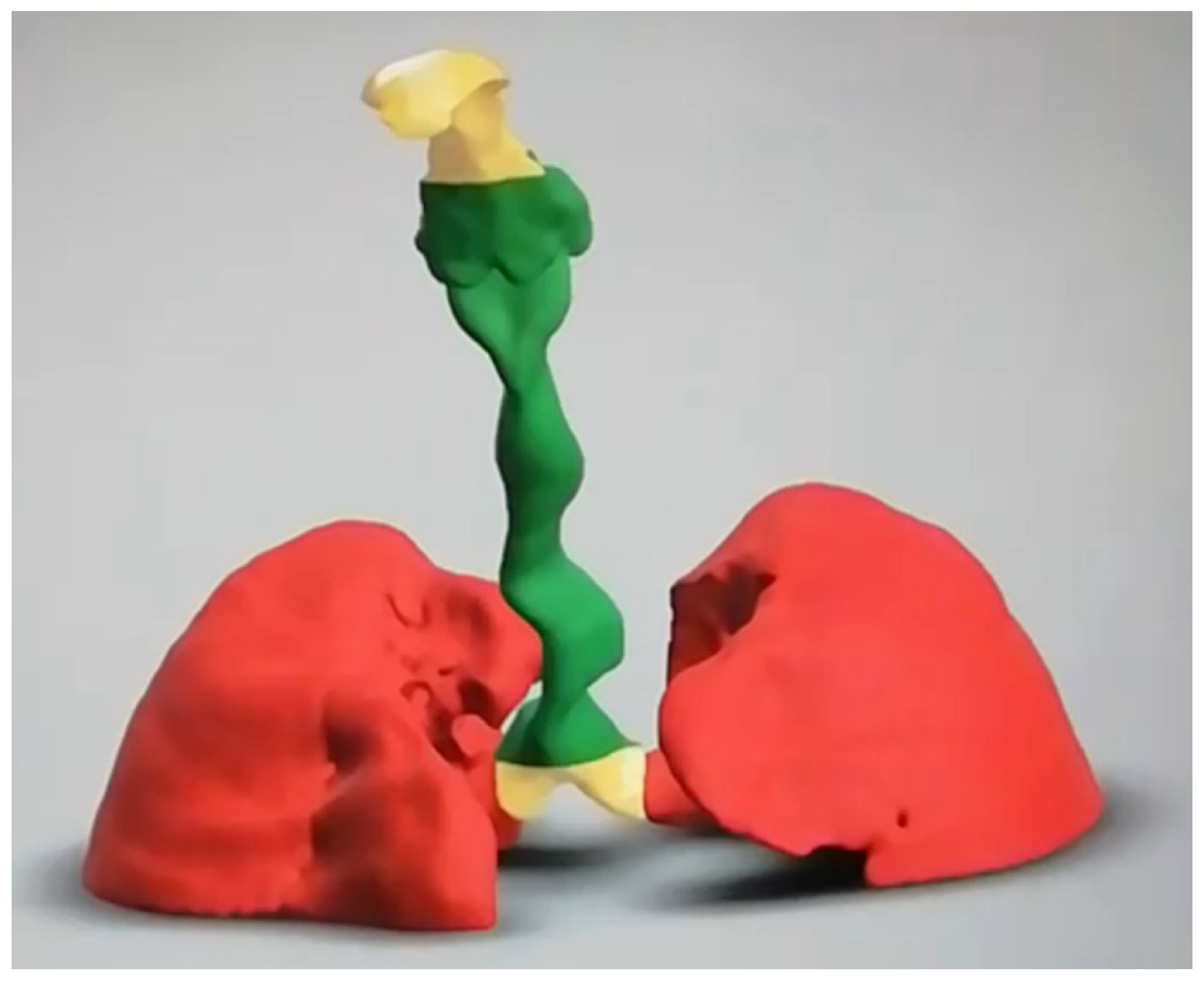
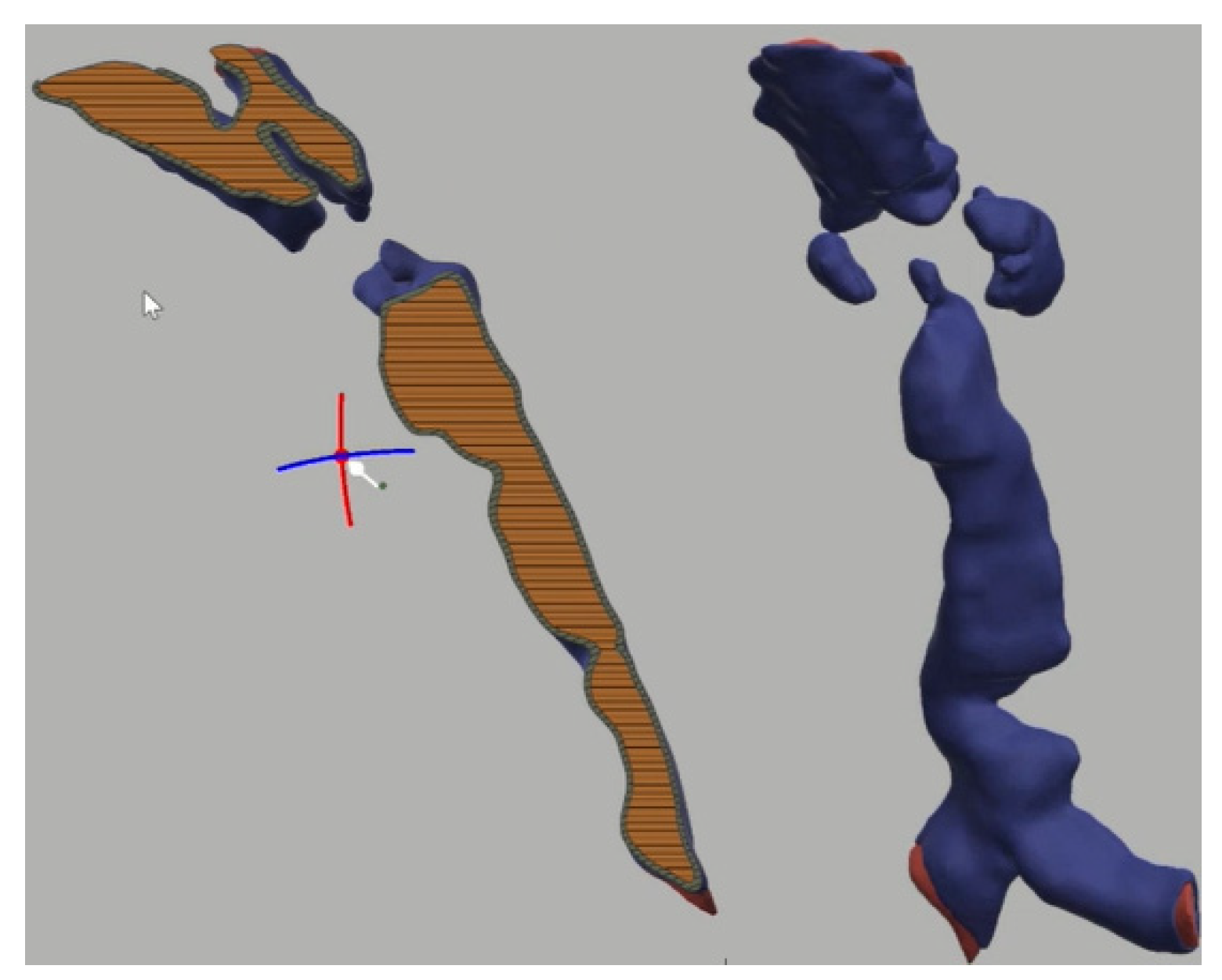
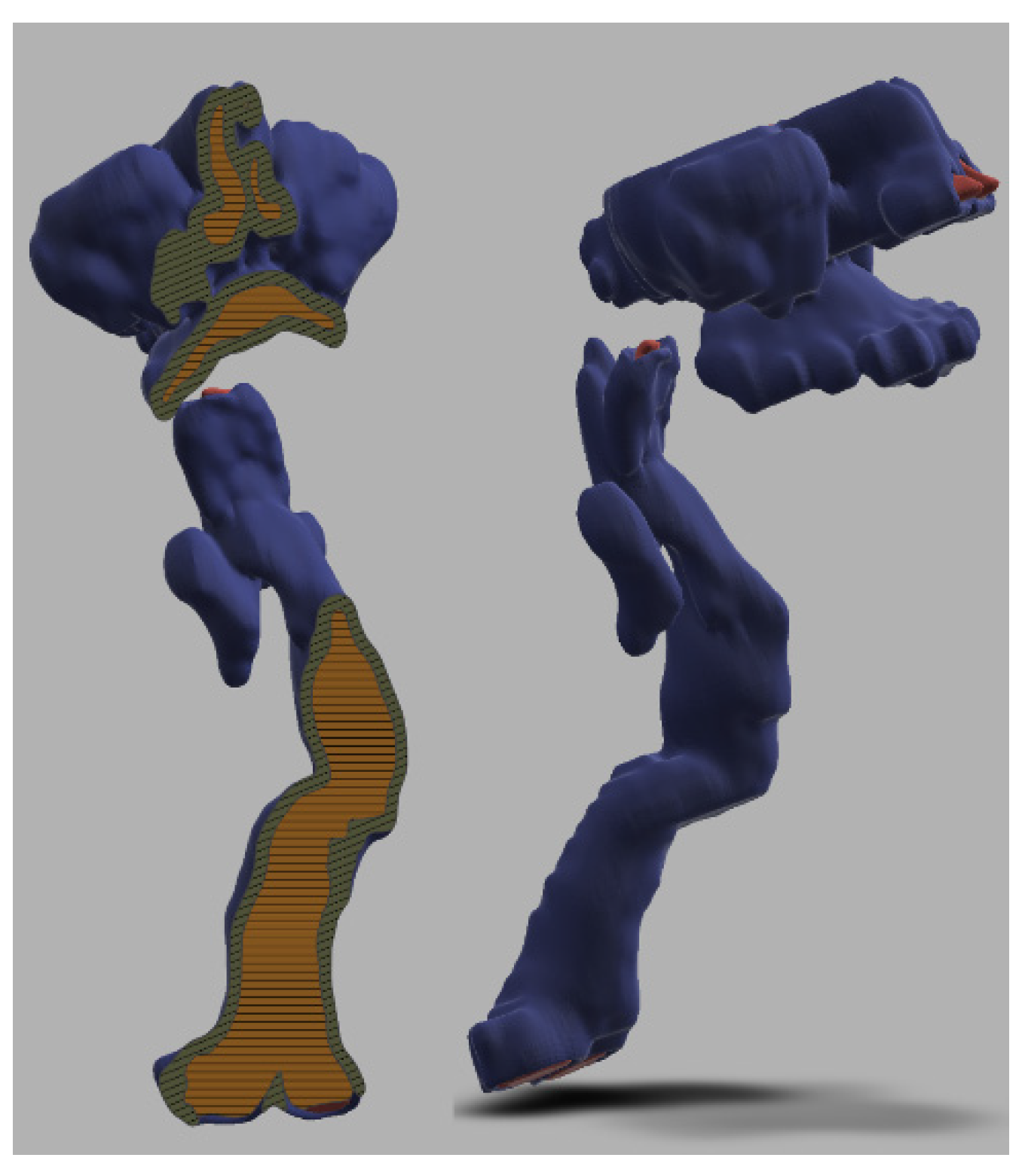
3.3. 3-Dimensional Reconstruction (3D) and Virtual Endoscopy (VE)
3.4. Salford Mucopolysaccharidosis Airway Score (SMAS)
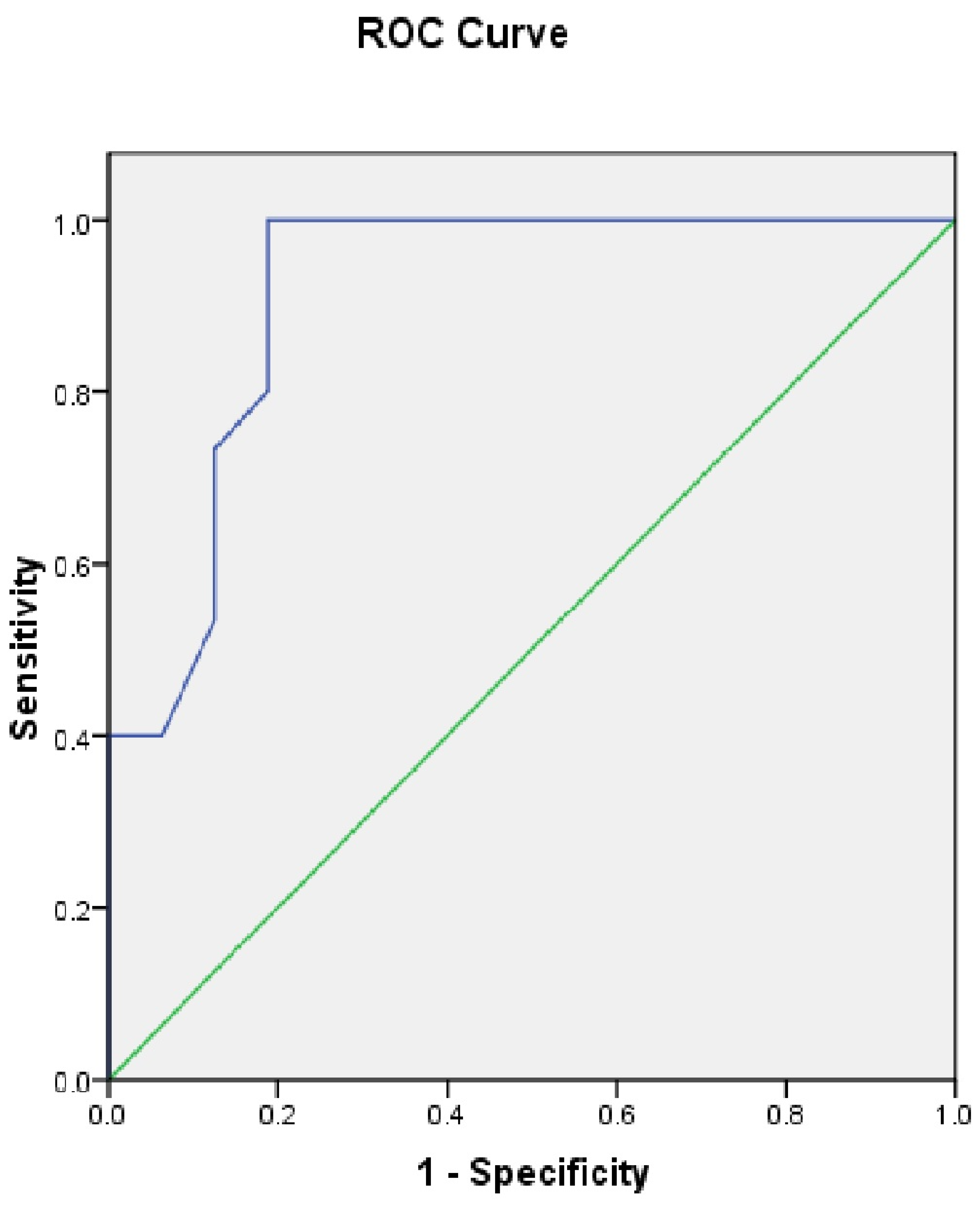
Validation and Usefulness of SMAS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Difficult Airway Assessment Questionnaire
- 1.
- Mouth opening.
- More than 5 cm = 0 score
- 4–5 cm = 1
- 3–4 cm = 2
- Less than 3 cm = 3
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 2.
- Teeth protrusion.
- Non-protruding = 0 score
- Mild protrusion = 1
- Moderate protrusion = 2
- Severe protrusion = 3 *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 3.
- Cervical spine mobility, stability on clinical examination.
- Unrestricted = 0 score
- 60–90 degrees flexion = 1
- 30–60 degrees flexion = 2
- Less than 30 degrees flexion or unstable or fixed = 3 *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 4.
- Tongue bulkiness on examination and scan.
- Normal = 0 score
- Mild = 1 (tongue fills floor of the mouth)
- Moderate = 2 (tongue fills between 1/3 to 1/2 of oral cavity)
- Severe = 3 (tongue fills more than 1/2 of oral cavity) *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 5.
- Modified Mallampati grade.
- Grade 1 = 0 score
- Grade 2 = 1
- Grade 3 = 2
- Grade 4 = 3 *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 6.
- Thyromental distance on clinical examination.
- More than 6 cm = 0 score
- 5–6 cm = 1
- 4-5 cm = 2
- Less than 4 cm = 3 *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 7.
- Larynx height-distance between epiglottis and soft palate on nasendoscopy/scan.
- More than 4 cm = 0 score
- 3–4 cm = 1
- 2–3 cm = 2
- Less than 2 cm = 3
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 8.
- Epiglottis bulkiness on nasendoscopy / scan.
- Normal= 0 score (filling less than less than 1/3 of oropharynx)
- Mild bulkiness = 1 (filling 1/3–1/2 of oropharynx)
- Moderate bulkiness = 2 (filling 1/2 to complete oropharynx)
- Severe bulkiness = 3 (filling the entire oropharynx) *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 9.
- Supraglottis bulkiness on nasendoscopy/scan.
- Normal= 0 score (filling less than less than 1/3 of supraglottis)
- Mild bulkiness = 1 (filling 1/3–1/2 of supraglottis)
- Moderate bulkiness = 2 (filling 1/2 to complete supraglottis)
- Severe bulkiness = 3 (filling the entire supraglottis) *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 10.
- Glottis bulkiness on nasendoscopy.
- Normal = 0 score (filling less than less than 1/3 of glottis)
- Mild bulkiness = 1 (filling 1/3–1/2 of glottis)
- Moderate bulkiness = 2 (filling 1/2 to complete glottis)
- Severe bulkiness = 3 (filling the entire glottis) *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 11.
- Subglottis diameter at cricoid level on CT scan.
- More than 7 mm = 0 score
- 6–7 mm = 1
- 5–6 mm = 2
- Less than 5 mm = 3 *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 12.
- Tracheomalacia or stenosis (degree of lumen collapse) on CT scan.
- No malacia = 0 score
- 50–75% lumen collapse = 1
- 75–99% lumen collapse = 2
- 100% lumen collapse = 3 *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 13.
- Tracheal tortuosity on CT scan.
- None = 0 score
- Tortuosity present = 3
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 14.
- FEV1% in last one year.
- More than > 80% = 0 score
- 60–79% = 1
- 40–59% = 2
- Less than 40% = 3
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 15.
- FVC% in last one year.
- More than 80% = 0 score
- 60–79% = 1
- 40–59% = 2
- Less than 40% = 3 *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 16.
- The above questions helps me in holistic airway assessment (contains all criteria to assess a difficult airway) *
- Strongly agree
- Agree
- Neutral
- Disagree
- Strongly disagree
- 17.
- Please use the space below to make any comments
References
- Mehta, A.B.; Winchester, B. Lysosomal Storage Disorders: A Practical Guide; Wiley-Blackwell: Chicester, UK, 2012. [Google Scholar]
- Neufeld, E.; Muenzer, J. The Mucopolysaccharidoses. In The Metabolic and Molecular Bases of Inherited Diseases, 8th ed.; Scriver, C.R., Beaudet, A.L., Sly, W.S., Valle, D., Childs, R., Kinzler, K.W., Eds.; McGraw-Hill: New York, NY, USA, 2001; pp. 3421–3452. [Google Scholar]
- Muenzer, J. Overview of the mucopolysaccharidoses. Rheumatology 2011, 50, v4–v12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, B.M.; Sprung, J.; Weingarten, T.N.; Warner, M.E. Anesthesia for patients with mucopolysaccharidoses: Comprehensive review of the literature with emphasis on airway management. Bosn. J. Basic Med. Sci. 2018, 18, 1. [Google Scholar] [CrossRef] [Green Version]
- Braunlin, E.A.; Harmatz, P.R.; Scarpa, M.; Furlanetto, B.; Kampmann, C.; Loehr, J.P.; Ponder, K.P.; Roberts, W.C.; Rosenfeld, H.M.; Giugliani, R. Cardiac disease in patients with mucopolysaccharidosis: Presentation, diagnosis and management. J. Inherit. Metab. Dis. 2011, 34, 1183–1197. [Google Scholar] [CrossRef] [Green Version]
- Valayannopoulos, V.; Nicely, H.; Harmatz, P.; Turbeville, S. Mucopolysaccharidosis vi. Orphanet J. Rare Dis. 2010, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Berger, K.I.; Fagondes, S.C.; Giugliani, R.; Hardy, K.A.; Lee, K.S.; McArdle, C.; Scarpa, M.; Tobin, M.J.; Ward, S.A.; Rapoport, D.M. Respiratory and sleep disorders in mucopolysaccharidosis. J. Inherit. Metab. Dis. 2013, 36, 201–210. [Google Scholar] [CrossRef]
- Muhlebach, M.S.; Wooten, W.; Muenzer, J. Respiratory manifestations in mucopolysaccharidoses. Paediatr. Respir. Rev. 2011, 12, 133–138. [Google Scholar] [CrossRef]
- Tsara, V.; Amfilochiou, A.; Papagrigorakis, J.; Georgopoulos, D.; Liolios, E.; Kadiths, A.; Koudoumnakis, E.; Aulonitou, E.; Emporiadou, M.; Tsakanikos, M. Guidelines for diagnosing and treating sleep related breathing disorders in adults and children (Part 3: Obstructive sleep apnea in children, diagnosis and treatment). Hippokratia 2010, 14, 57. [Google Scholar]
- Dalewski, B.; Kamińska, A.; Syrico, A.; Kałdunska, A.; Pałka, Ł.; Sobolewska, E. The Usefulness of Modified Mallampati Score and CT Upper Airway Volume Measurements in Diagnosing OSA among Patients with Breathing-Related Sleep Disorders. Appl. Sci. 2021, 11, 3764. [Google Scholar] [CrossRef]
- Huang, H.-H.; Lee, M.-S.; Shih, Y.-L.; Chu, H.-C.; Huang, T.-Y.; Hsieh, T.-Y. Modified Mallampati classification as a clinical predictor of peroral esophagogastroduodenoscopy tolerance. BMC Gastroenterol. 2011, 11, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thurtell, M.J.; Bruce, B.B.; Rye, D.B.; Newman, N.J.; Biousse, V. The Berlin questionnaire screens for obstructive sleep apnea in idiopathic intracranial hypertension. J. Neuro-Ophthalmol. 2011, 31, 316–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wraith, J.E. The first 5years of clinical experience with laronidase enzyme replacement therapy for mucopolysaccharidosis I. Expert Opin. Pharmacother. 2005, 6, 489–506. [Google Scholar] [CrossRef] [PubMed]
- Wraith, J.E.; Beck, M.; Lane, R.; Van Der Ploeg, A.; Shapiro, E.; Xue, Y.; Kakkis, E.D.; Guffon, N. Enzyme replacement therapy in patients who have mucopolysaccharidosis I and are younger than 5 years: Results of a multinational study of recombinant human α-L-iduronidase (laronidase). Pediatrics 2007, 120, e37–e46. [Google Scholar] [CrossRef]
- Hendriksz, C.J.; Giugliani, R.; Harmatz, P.; Mengel, E.; Guffon, N.; Valayannopoulos, V.; Parini, R.; Hughes, D.; Pastores, G.M.; Lau, H.A. Multi-domain impact of elosulfase alfa in Morquio A syndrome in the pivotal phase III trial. Mol. Genet. Metab. 2015, 114, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Hendriksz, C.J.; Burton, B.; Fleming, T.R.; Harmatz, P.; Hughes, D.; Jones, S.A.; Lin, S.-P.; Mengel, E.; Scarpa, M.; Valayannopoulos, V. Efficacy and safety of enzyme replacement therapy with BMN 110 (elosulfase alfa) for Morquio A syndrome (mucopolysaccharidosis IVA): A phase 3 randomised placebo-controlled study. J. Inherit. Metab. Dis. 2014, 37, 979–990. [Google Scholar] [CrossRef] [Green Version]
- Clarke, L.A.; Wraith, J.E.; Beck, M.; Kolodny, E.H.; Pastores, G.M.; Muenzer, J.; Rapoport, D.M.; Berger, K.I.; Sidman, M.; Kakkis, E.D. Long-term efficacy and safety of laronidase in the treatment of mucopolysaccharidosis I. Pediatrics 2009, 123, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Harmatz, P.; Giugliani, R.; Schwartz, I.V.D.; Guffon, N.; Teles, E.L.; Miranda, M.C.S.; Wraith, J.E.; Beck, M.; Arash, L.; Scarpa, M. Long-term follow-up of endurance and safety outcomes during enzyme replacement therapy for mucopolysaccharidosis VI: Final results of three clinical studies of recombinant human N-acetylgalactosamine 4-sulfatase. Mol. Genet. Metab. 2008, 94, 469–475. [Google Scholar] [CrossRef]
- Aldenhoven, M.; Wynn, R.F.; Orchard, P.J.; O’Meara, A.; Veys, P.; Fischer, A.; Valayannopoulos, V.; Neven, B.; Rovelli, A.; Prasad, V.K. Long-term outcome of Hurler syndrome patients after hematopoietic cell transplantation: An international multicenter study. Blood J. Am. Soc. Hematol. 2015, 125, 2164–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arn, P.; Bruce, I.A.; Wraith, J.E.; Travers, H.; Fallet, S. Airway-related symptoms and surgeries in patients with mucopolysaccharidosis I. Ann. Otol. Rhinol. Laryngol. 2015, 124, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Pal, A.R.; Mercer, J.; Jones, S.A.; Bruce, I.A.; Bigger, B.W. Substrate accumulation and extracellular matrix remodelling promote persistent upper airway disease in mucopolysaccharidosis patients on enzyme replacement therapy. PLoS ONE 2018, 13, e0203216. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, K.; Ellwood, J.; Walker, R.W. Mucopolysaccharidosis type I (Hurler syndrome) and anesthesia: The impact of bone marrow transplantation, enzyme replacement therapy, and fiberoptic intubation on airway management. Pediatric Anesth. 2012, 22, 745–751. [Google Scholar] [CrossRef]
- Katz, J.A.; Avram, M.J. 4th National Audit Project of the Royal College of Anaesthetists and The Difficult Airway Society: Major Complications of Airway Management in the United Kingdom: Report and Findings. J. Am. Soc. Anesthesiol. 2012, 116, 496. [Google Scholar] [CrossRef] [Green Version]
- Apfelbaum, J.; Hagberg, C.; Caplan, R.; Blitt, C.; Connis, R.; Nickinovich, D.; Benumof, J.; Berry, F. American Society of Anesthesiologists Task Force on Management of the Difficult Airway Practice guidelines for management of the difficult airway: An updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2013, 118, 251–270. [Google Scholar] [PubMed] [Green Version]
- Roth, D.; Pace, N.; Lee, A.; Hovhannisyan, K.; Warenits, A.; Arrich, J.; Herkner, H. Bedside tests for predicting difficult airways: An abridged Cochrane diagnostic test accuracy systematic review. Anaesthesia 2019, 74, 915–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallampati, S.R.; Gatt, S.P.; Gugino, L.D.; Desai, S.P.; Waraksa, B.; Freiberger, D.; Liu, P.L. A clinical sign to predict difficult tracheal intubation; a prospective study. Can. Anaesth. Soc. J. 1985, 32, 429–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.; Spiegelhalter, D.; Robertson, J.; Lesser, P. Predicting difficult intubation. BJA Br. J. Anaesth. 1988, 61, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Crawley, S.; Dalton, A. Predicting the difficult airway. BJA Educ. 2015, 15, 253–257. [Google Scholar] [CrossRef]
- Cattano, D.; Killoran, P.; Iannucci, D.; Maddukuri, V.; Altamirano, A.; Sridhar, S.; Seitan, C.; Chen, Z.; Hagberg, C. Anticipation of the difficult airway: Preoperative airway assessment, an educational and quality improvement tool. Br. J. Anaesth. 2013, 111, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittenborg, M.; Gyepes, M.; Crocker, D. Tracheal dynamics in infants with respiratory distress, stridor, and collapsing trachea. Radiology 1967, 88, 653–662. [Google Scholar] [CrossRef]
- Murgu, S.D.; Colt, H.G. Description of a multidimensional classification system for patients with expiratory central airway collapse. Respirology 2007, 12, 543–550. [Google Scholar] [CrossRef]
- Boiselle, P.M.; O’Donnell, C.R.; Bankier, A.A.; Ernst, A.; Millet, M.E.; Potemkin, A.; Loring, S.H. Tracheal collapsibility in healthy volunteers during forced expiration: Assessment with multidetector CT. Radiology 2009, 252, 255–262. [Google Scholar] [CrossRef]
- Baroni, R.H.; Feller-Kopman, D.; Nishino, M.; Hatabu, H.; Loring, S.H.; Ernst, A.; Boiselle, P.M. Tracheobronchomalacia: Comparison between end-expiratory and dynamic expiratory CT for evaluation of central airway collapse. Radiology 2005, 235, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Murgu, S.D.; Colt, H.G. Treatment of adult tracheobronchomalacia and excessive dynamic airway collapse. Treat. Respir. Med. 2006, 5, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Svetanoff, W.J.; Jennings, R.W. Updates on surgical repair of tracheobronchomalacia. J. Lung Health Dis. 2018, 2, 17–23. [Google Scholar] [CrossRef]
- Pizarro, C.; Davies, R.R.; Theroux, M.; Spurrier, E.A.; Averill, L.W.; Tomatsu, S. Surgical reconstruction for severe tracheal obstruction in Morquio A syndrome. Ann. Thorac. Surg. 2016, 102, e329–e331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenth, J.J.; Thompson, G.; Fullwood, C.; Wilkinson, S.; Jones, S.; Bruce, I. The characterisation of pulmonary function in patients with mucopolysaccharidoses IVA: A longitudinal analysis. Mol. Genet. Metab. Rep. 2019, 20, 100487. [Google Scholar] [CrossRef]
- Taylor, M.; Khan, S.; Stapleton, M.; Wang, J.; Chen, J.; Wynn, R.; Yabe, H.; Chinen, Y.; Boelens, J.J.; Mason, R.W. Hematopoietic stem cell transplantation for mucopolysaccharidoses: Past, present, and future. Biol. Blood Marrow Transplant. 2019, 25, e226–e246. [Google Scholar] [CrossRef]
- Concolino, D.; Deodato, F.; Parini, R. Enzyme replacement therapy: Efficacy and limitations. Ital. J. Pediatrics 2018, 44, 117–126. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MPS Type (Eponym) | Incidence per 105 Live Births; Inheritance Pattern | Typical Age at Diagnosis | Typical Life Expectancy If Untreated | Enzyme Deficiency | GAG |
|---|---|---|---|---|---|
| MPS I Hurler (H) MPS I Hurler–Scheie (H-S) MPS I Scheie (S) | 0.11–1.67; AR | H: <1 year H-S: 3–8 years S: 10–20 years | H: death in childhood H-S: death in teens or early adulthood S: normal to slightly reduced lifespan | α-L-iduronidase | DS, HS |
| MPS II (Hunter) | 0.1–1.07; XR | 1–2 years when rapidly progressing | rapidly progressing: death < 15 years slowly progressing: death in adulthood | iduronate-2-sulfatase | DS, HS |
| MPS III (Sanfilippo) A-B-C-D | 0.39–1.89; AR | 4–6 years | death in puberty or early adulthood | heparan sulfamidase (A) N-acetyl-α-D-glucosaminidase (B) acetyl-CoA-α-glucosaminidase N-acetyltransferase (C) N-acetylglucosamine-6-sulfatase (D) | HS |
| MPS IV (Morquio) A-B | 0.15–0.47; AR | 1–3 years | death in childhood- middle age | N-acetylgalactosamine-6-sulfatase (A) β-galactosidase (B) | CS, KS (A) KS (B) |
| MPS VI (Maroteaux-Lamy) | 0–0.38; AR | rapidly progressing: 1–9 years slowly progressing: >5 years | rapidly progressing: death in 2nd–3rd decade slowly progressing: death in 4–5th decade | N-acetylgalactosamine-4-sulfatase | DS |
| tblMPS VII (Sly) | 0–0.29; AR | neonatal to adulthood | death in infancy- 4th decade ** | β-D-glucuronidase | CS, DS, HS |
| MPS IX (Natowicz) * | unknown | adolescence | unknown | hyaluronidase | CS |
| S. No. | Parameter | Measure | Score | Final Score |
|---|---|---|---|---|
| MPS Type | ||||
| 1 | Mouth opening | >5 cm | 0 | |
| 4–5 cm | 1 | |||
| 3–4 cm | 2 | |||
| <3 cm | 3 | |||
| 2 | Teeth protrusion on clinical exam and scans | Non-protruding | 0 | |
| Mild | 1 | |||
| Moderate | 2 | |||
| Severe | 3 | |||
| 3 | Cervical spine mobility, stability | unrestricted | 0 | |
| 60–90 degrees flexion | 1 | |||
| 30–60 degrees flexion | 2 | |||
| <30 degrees or unstable | 3 | |||
| 4 | Tongue bulkiness on examination and Scan | Normal | 0 | |
| Mild (filling less than 1/3 of floor mouth) | 1 | |||
| Moderate (filling 1/3 to 1/2 of oral cavity) | 2 | |||
| Severe (filling more than 1/2 of oral cavity) | 3 | |||
| 5 | Modified Mallampati grade [11] | 1 | 0 | |
| 2 | 1 | |||
| 3 | 2 | |||
| 4 | 3 | |||
| 6 | Thyromental distance | >6 cm | 0 | |
| 5–6 cm | 1 | |||
| 4–5 cm | 2 | |||
| <4 cm | 3 | |||
| 7 | Larynx height epiglottis to soft palate | >4 cm | 0 | |
| 3–4 cm | 1 | |||
| 2–3 cm | 2 | |||
| <2 cm | 3 | |||
| 8 | Epiglottis bulkiness | Normal (filling less than 1/3 of oropharynx) | 0 | |
| Mild (filling 1/3 to 1/2 of oropharynx) | 1 | |||
| Moderate (filling 1/2 to complete oropharynx) | 2 | |||
| Severe (Filling entire oropharynx) | 3 | |||
| 9 | Supraglottis bulkiness | Normal (filling less than 1/3 of laryngopharynx) | 0 | |
| Mild (filling 1/3 to 1/2 of laryngopharynx) | 1 | |||
| Moderate (filling ½ to complete laryngopharynx) | 2 | |||
| Severe (filling entire oropharynx) | 3 | |||
| 10 | Glottis bulkiness | Normal (filling less than 1/3 of glottis) | 0 | |
| Mild (filling 1/3 to 1/2 of glottis) | 1 | |||
| Moderate (filling 1/2 to complete glottis) | 2 | |||
| Severe (filling entire glottis) | 3 | |||
| 11 | Subglottis diameter at cricoid level | >7 mm | 0 | |
| 6–7 mm | 1 | |||
| 5–6 mm | 2 | |||
| <5 mm | 3 | |||
| 12 | Tracheomalacia or tracheal stenosis (degree of narrowing) | No narrowing | 0 | |
| 50–75% lumen narrowing | 1 | |||
| 75–99% lumen narrowing | 2 | |||
| 100% lumen narrowing | 3 | |||
| 13 | Tracheal tortuosity | None | 0 | |
| present | 3 | |||
| 14 | FEV1% | >80% | 0 | |
| 60–79% | 1 | |||
| 40–59% | 2 | |||
| <40% | 3 | |||
| 15 | FVC% | >80% | 0 | |
| 60–79% | 1 | |||
| 40–59% | 2 | |||
| <40% | 3 |
| MPS Type | Number | Age in Years and Number of Patients | Sex |
|---|---|---|---|
| 1 | 9 | 23–27 = 5 31–32 = 2 39 = 1 43 = 1 | Females = 3 Males = 6 |
| 2 | 12 | 20–27 = 7 29–33 = 5 | All males |
| 3 | 2 | 19–21 = 2 | Both females |
| 4 | 5 | 19, 21, 23, 33, 41 | Females = 4 Male = 1 |
| 6 | 2 | 27, 38 | Female = 1, Male = 1 |
| 7 | 1 | 31 | Male |
| MPS Type | Airway Findings | Relevant Airway Challenges |
|---|---|---|
| 1 | Protruding teeth, large tongue, high larynx, moderately bulky supraglottis, narrow subglottis | Learning difficulties, poor vision |
| 2 | Protruding teeth, large tongue, high larynx, very bulky supraglottis, narrow subglottis, tracheobronchomalacia | Cervical spine instability, short neck |
| 3 | Large tongue, malacia of supraglottis | Learning difficulties |
| 4 | Large tongue, protruding teeth, large jaw, moderately bulky supraglottis, large epiglottis, tortuous trachea with tracheomalacia | Short neck, hypermobility |
| 6 | Large tongue, protruding teeth, large jaw, large epiglottis, tortuous trachea with tracheomalacia | Short neck, c-spine problems, kyphoscoliosis |
| 7 | Slightly protruding teeth, high larynx, narrow subglottis, tortuous trachea | Kyphoscoliosis |
| Patient Number | MPS Type | Sex | Age in Years | SMAS | Score Percentage | Associated Abnormality | Therapy | Mutation |
|---|---|---|---|---|---|---|---|---|
| 1 | I | M | 39.1 | 20 | 51.3 | HSCT | p.(Trp402Ter), p.(Leu218Pro) | |
| 2 | I | M | 31.3 | 15 | 33.3 | HSCT | p.(Leu490Pro), p.(Leu490Pro) | |
| 3 | I | M | 25.9 | 23 | 51.1 | HSCT | p.(Trp402Ter), p.(Trp402Ter) | |
| 4 | I | M | 25.7 | 10 | 22.2 | HSCT | p.(Gln70Ter), p.(Gln70Ter) | |
| 5 | I | M | 32.2 | 24 | 53.3 | HSCT | p.(Trp402Ter), p.(Ser633Leu) | |
| 6 | I | M | 26.7 | 31 | 68.9 | OSA | ERT | hom L490P, exon 10 IDUA gene |
| 7 | I | F | 23.0 | 10 | 22.2 | ERT | N/A | |
| 8 | I | F | 43.0 | 29 | 64.4 | OSA | ERT | N/A |
| 9 | I | F | 24.0 | 20 | 48.7 | ERT | N/A | |
| 10 | II | M | 30.1 | 40 | 88.9 | TRACH | ERT | c.1152delT, exon 8 IDS gene |
| 11 | II | M | 31.7 | 36 | 80 | OSA | ERT | N/A |
| 12 | II | M | 29.1 | 35 | 77.8 | OSA | ERT | N/A |
| 13 | II | M | 20.7 | 32 | 82.1 | OSA | ERT | c.1528insT |
| 14 | II | M | 33.0 | 40 | 88.9 | TRACH | ERT STOPPED | N/A |
| 15 | II | M | 32.9 | 34 | 75.6 | OSA | ERT | N/A |
| 16 | II | M | 25.2 | 32 | 82.1 | OSA | ERT | N/A |
| 17 | II | M | 26.3 | 11 | 24.4 | ERT | T14gT, exon4 IDS gene | |
| 18 | II | M | 23.7 | 21 | 46.7 | ERT | N/A | |
| 19 | II | M | 20.9 | 31 | 79.5 | OSA | ERT | N/A |
| 20 | II | M | 26.9 | 29 | 64.4 | OSA | ERT | missense mutation in N63D, exon 2, IDS gene |
| 21 | II | M | 23.3 | 14 | 31.1 | ERT | N/A | |
| 22 | III | F | 19.6 | 9 | 30 | none | N/A | |
| 23 | III | F | 20.3 | 2 | 6.7 | none | hom c.234+1G>T, HGSNAT gene | |
| 24 | IV | F | 23.0 | 32 | 82.1 | OSA | none | N/A |
| 25 | IV | F | 21.1 | 28 | 71.7 | OSA | ERT? | N/A |
| 26 | IV | F | 41.1 | 38 | 84.4 | OSA | ERT STOPPED | hom c.871G>A p.(Ala291Thr) GALNS gene |
| 27 | IV | M | 33.5 | 27 | 60 | OSA | none | N/A |
| 28 | IV | M | 19.3 | 26 | 57.8 | OSA | ERT | N/A |
| 29 | VI | F | 27.3 | 30 | 66.7 | OSA | ERT | T442R/245delT |
| 30 | VI | M | 38.1 | 41 | 91.1 | TRACH | ERT paused | N/A |
| 31 | VII | M | 31.0 | 16 | 41.1 | none | c.526C>T p.(Leu176Phe), c.1820G>C p.(Gly607Ala) |
| Subtitle | Subtitle | Total Score |
|---|---|---|
| Height | Correlation coefficient | −0.438 |
| p-value | 0.014 | |
| Weight | Correlation coefficient | −0.168 |
| p-value | 0.367 | |
| Body Mass Index | Correlation coefficient | 0.340 |
| p-value | 0.061 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gadepalli, C.; Stepien, K.M.; Sharma, R.; Jovanovic, A.; Tol, G.; Bentley, A. Airway Abnormalities in Adult Mucopolysaccharidosis and Development of Salford Mucopolysaccharidosis Airway Score. J. Clin. Med. 2021, 10, 3275. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153275
Gadepalli C, Stepien KM, Sharma R, Jovanovic A, Tol G, Bentley A. Airway Abnormalities in Adult Mucopolysaccharidosis and Development of Salford Mucopolysaccharidosis Airway Score. Journal of Clinical Medicine. 2021; 10(15):3275. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153275
Chicago/Turabian StyleGadepalli, Chaitanya, Karolina M. Stepien, Reena Sharma, Ana Jovanovic, Govind Tol, and Andrew Bentley. 2021. "Airway Abnormalities in Adult Mucopolysaccharidosis and Development of Salford Mucopolysaccharidosis Airway Score" Journal of Clinical Medicine 10, no. 15: 3275. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10153275