Contributing Factors to Perinatal Outcome in Pregnancies with Gestational Diabetes—What Matters Most? A Retrospective Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
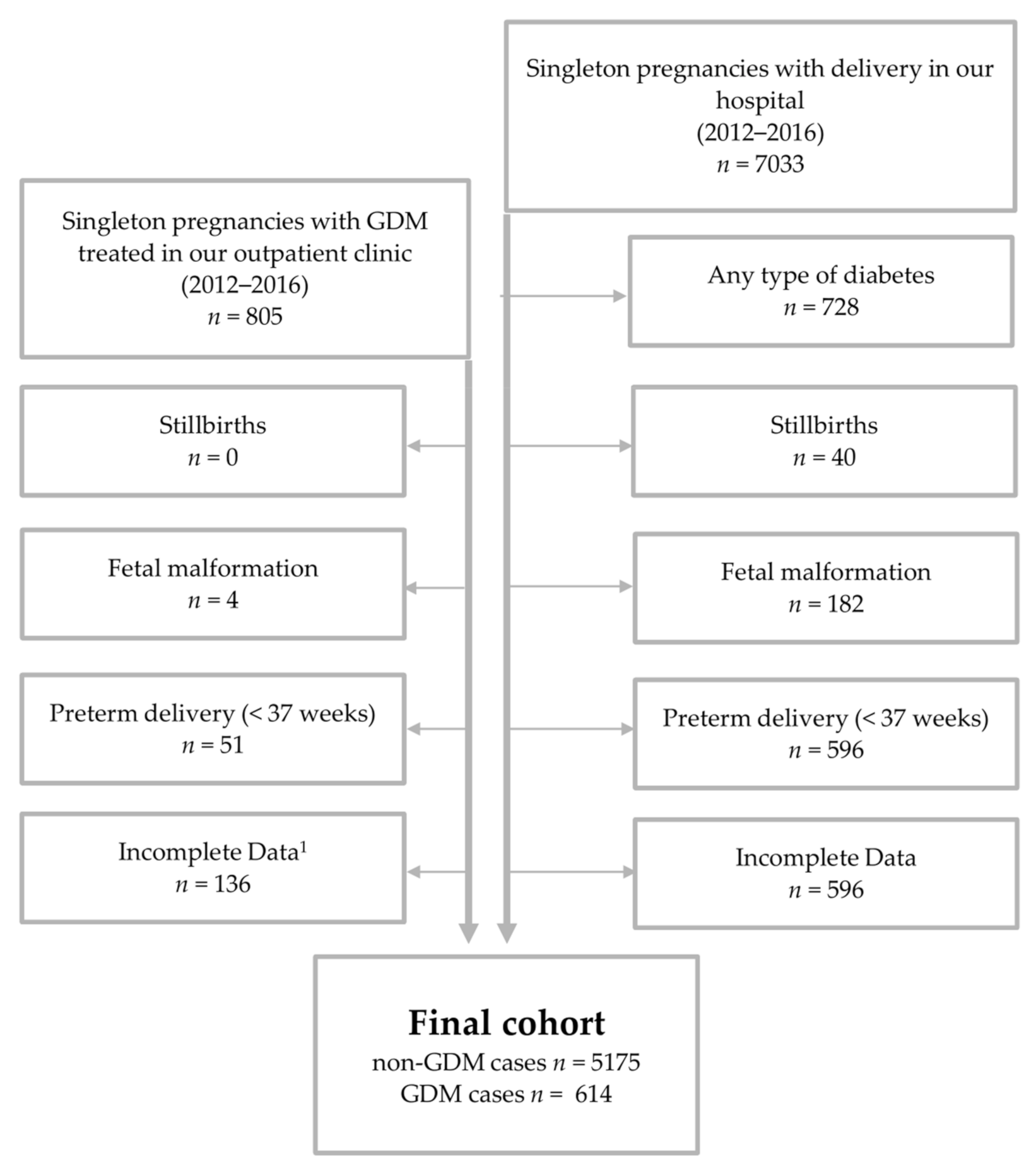
2.1. Study Population
2.2. Study Outcomes and Measures
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Perinatal Outcomes
3.3. Independent Contributions of BMI, GWG and GDM on Perinatal Outcome
3.4. Subgroup Characteristics
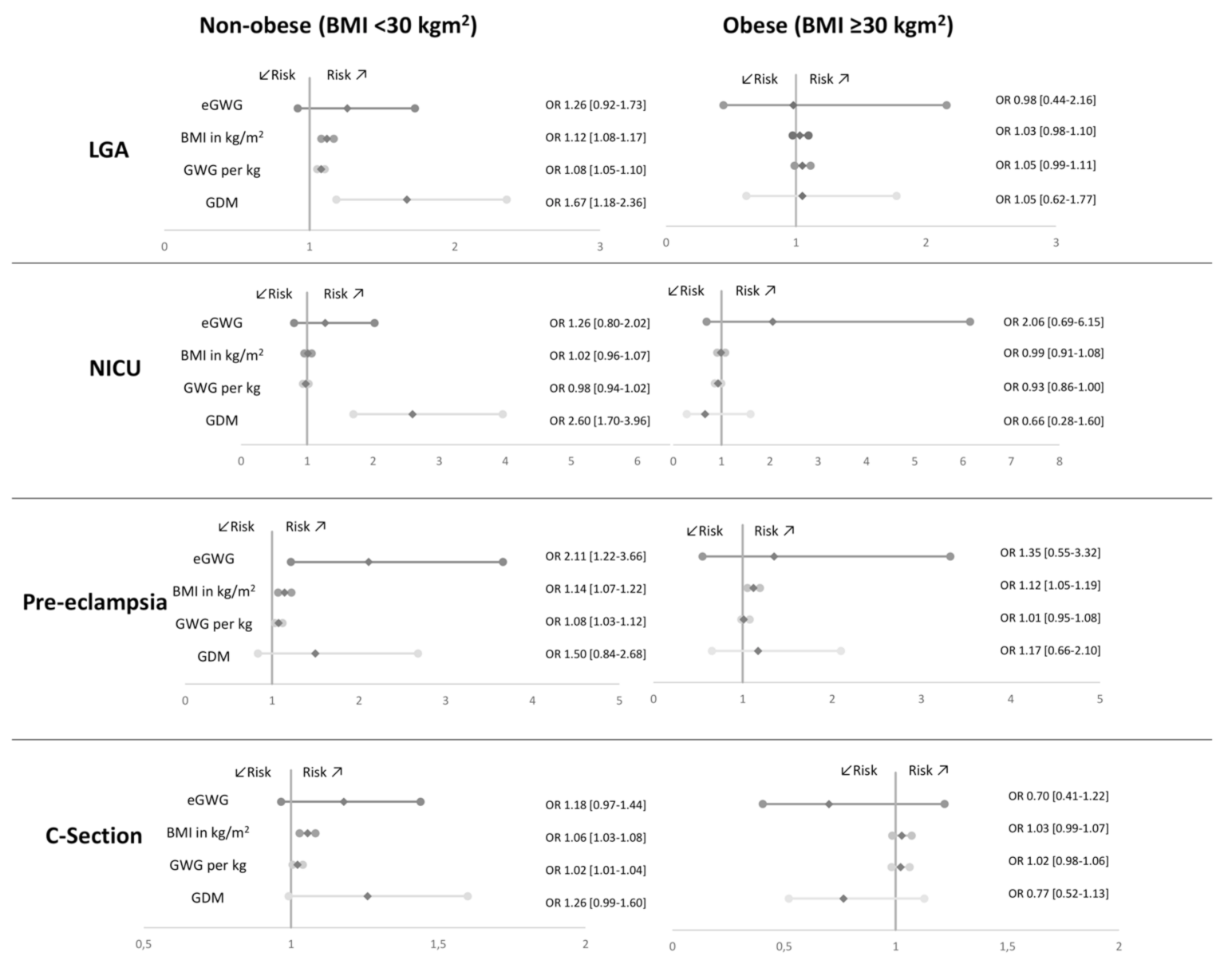
3.5. Contributing Factors in Subgroups
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Melchior, H.; Kurch-Bek, D.; Mund, M. The prevalence of gestational diabetes. Dtsch. Arztebl. Int. 2017, 114, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IQTIG. Bundesauswertung zum Erfassungsjahr 2017—Geburtshilfe -Qualitätsindikatoren; IQTIG—Institut für Qualitätssicherung und Transparenz im Gesundheitswesen: Berlin, Germany, 2018. [Google Scholar]
- Behboudi-Gandevani, S.; Amiri, M.; Bidhendi Yarandi, R.; Ramezani Tehrani, F. The impact of diagnostic criteria for gestational diabetes on its prevalence: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalano, P.M.; McIntyre, H.D.; Cruickshank, J.K.; McCance, D.R.; Dyer, A.R.; Metzger, B.E.; Lowe, L.P.; Trimble, E.R.; Coustan, D.R.; Hadden, D.R.; et al. The hyperglycemia and adverse pregnancy outcome study: Associations of GDM and obesity with pregnancy outcomes. Diabetes Care 2012, 35, 780–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, K.M.; Gale, C.; Hyde, M.J.; Santhakumaran, S.; Modi, N. Diabetes in pregnancy and infant adiposity: Systematic review and meta-analysis. Arch. Dis. Child Fetal Neonatal Ed. 2017, 102, F65–F72. [Google Scholar] [CrossRef] [PubMed]
- Khambalia, A.Z.; Algert, C.S.; Bowen, J.R.; Collie, R.J.; Roberts, C.L. Long-term outcomes for large for gestational age infants born at term. J. Paediatr. Child Health 2017, 53, 876–881. [Google Scholar] [CrossRef]
- Weissmann-Brenner, A.; Simchen, M.J.; Zilberberg, E.; Kalter, A.; Weisz, B.; Achiron, R.; Dulitzky, M. Maternal and neonatal outcomes of large for gestational age pregnancies. Acta Obs. Gynecol Scand. 2012, 91, 844–849. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Skilton, M.R.; Siitonen, N.; Würtz, P.; Viikari, J.S.; Juonala, M.; Seppälä, I.; Laitinen, T.; Lehtimäki, T.; Taittonen, L.; Kähönen, M.; et al. High birth weight is associated with obesity and increased carotid wall thickness in young adults: The cardiovascular risk in young Finns study. Arter. Thromb. Vasc. Biol. 2014, 34, 1064–1068. [Google Scholar] [CrossRef] [Green Version]
- Muche, A.A.; Olayemi, O.O.; Gete, Y.K. Effects of gestational diabetes mellitus on risk of adverse maternal outcomes: A prospective cohort study in Northwest Ethiopia. BMC Pregnancy Childbirth 2020, 20, 73. [Google Scholar] [CrossRef]
- Fadl, H.E.; Ostlund, I.K.; Magnuson, A.F.; Hanson, U.S. Maternal and neonatal outcomes and time trends of gestational diabetes mellitus in Sweden from 1991 to 2003. Diabet. Med. 2010, 27, 436–441. [Google Scholar] [CrossRef]
- Waters, T.P.; Dyer, A.R.; Scholtens, D.M.; Dooley, S.L.; Herer, E.; Lowe, L.P.; Oats, J.J.; Persson, B.; Sacks, D.A.; Metzger, B.E.; et al. Maternal and neonatal morbidity for women who would be added to the diagnosis of GDM using IADPSG criteria: A secondary analysis of the hyperglycemia and adverse pregnancy outcome study. Diabetes Care 2016, 39, 2204–2210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, K.E.; Grivell, R.M.; Yelland, L.N.; Dodd, J.M. The influence of maternal BMI and gestational diabetes on pregnancy outcome. Diabetes Res. Clin. Pr. 2015, 108, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Kleinwechter, H.; Schäfer-Graf, U.; Bührer, C.; Hoesli, I.; Kainer, F.; Kautzky-Willer, A.; Pawlowski, B.; Schunck, K.; Somville, T.; Sorger, M.; et al. Gestational diabetes mellitus (GDM) diagnosis, therapy and follow-up care: Practice guideline of the German Diabetes Association (DDG) and the German Association for Gynaecologyand Obstetrics (DGGG). Exp. Clin. Endocrinol. Diabetes 2014, 122, 395–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blomberg, M. Maternal and neonatal outcomes among obese women with weight gain below the new Institute of Medicine recommendations. Obs. Gynecol. 2011, 117, 1065–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Sharma, A.J.; Sappenfield, W.; Wilson, H.G.; Salihu, H.M. Association of maternal body mass index, excessive weight gain, and gestational diabetes mellitus with large-for-gestational-age births. Obs. Gynecol 2014, 123, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Xu, L.; Wu, M.L.; Huang, S.H.; Cao, X.J. Maternal pre-pregnancy body mass index, gestational weight gain influence birth weight. Women Birth 2018, 31, e20–e25. [Google Scholar] [CrossRef]
- Blackwell, S.C.; Landon, M.B.; Mele, L.; Reddy, U.M.; Casey, B.M.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; Sciscione, A.; et al. Relationship between excessive gestational weight gain and neonatal adiposity in women with mild gestational diabetes mellitus. Obs. Gynecol. 2016, 128, 1325–1332. [Google Scholar] [CrossRef] [Green Version]
- Miao, M.; Dai, M.; Zhang, Y.; Sun, F.; Guo, X.; Sun, G. Influence of maternal overweight, obesity and gestational weight gain on the perinatal outcomes in women with gestational diabetes mellitus. Sci. Rep. 2017, 7, 305. [Google Scholar] [CrossRef]
- Rasmussen, K.M.; Catalano, P.M.; Yaktine, A.L. New guidelines for weight gain during pregnancy: What obstetrician/gynecologists should know. Curr. Opin. Obstet. Gynecol. 2009, 21, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Ben-Haroush, A.; Hadar, E.; Chen, R.; Hod, M.; Yogev, Y. Maternal obesity is a major risk factor for large-for-gestational-infants in pregnancies complicated by gestational diabetes. Arch. Gynecol. Obs. 2009, 279, 539–543. [Google Scholar] [CrossRef]
- Barquiel, B.; Herranz, L.; Hillman, N.; Burgos, M.A.; Grande, C.; Tukia, K.M.; Bartha, J.L.; Pallardo, L.F. HbA1c and gestational weight gain are factors that influence neonatal outcome in mothers with gestational diabetes. J. Womens Health 2016, 25, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, S.; Iuchi, T.; Goto, A.; Katanoda, K.; Iida, S.; Oikawa, Y.; Namba, A.; Isshiki, M.; Inoue, I.; Kamei, Y.; et al. Weight control before and during pregnancy for patients with gestational diabetes mellitus. J. Diabetes Investig. 2019, 10, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Weschenfelder, F.; Lehmann, T.; Schleussner, E.; Groten, T. Gestational weight gain particularly affects the risk of large for gestational age infants in non-obese mothers. Geburtshilfe Frauenheilkd 2019, 79, 1183–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aiken, C.E.M.; Hone, L.; Murphy, H.R.; Meek, C.L. Improving outcomes in gestational diabetes: Does gestational weight gain matter? Diabet. Med. 2019, 36, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M.; Shankar, K. Obesity and pregnancy: Mechanisms of short term and long term adverse consequences for mother and child. BMJ 2017, 356, j1. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, L.; Baştuğ, O.; Kurtoğlu, S. Maternal obesity and its short and long term maternal and infantile effects. J. Clin. Res. Pediatr. Endocrinol. 2015, 8, 114. [Google Scholar] [CrossRef] [PubMed]
- Duckitt, K.; Harrington, D. Risk factors for pre-eclampsia at antenatal booking: Systematic review of controlled studies. BMJ 2005, 330, 565. [Google Scholar] [CrossRef] [Green Version]
- Trogstad, L.; Magnus, P.; Stoltenberg, C. Pre-eclampsia: Risk factors and causal models. Best Pr. Res. Clin. Obs. Gynaecol. 2011, 25, 329–342. [Google Scholar] [CrossRef]
- IADPSG. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676. [Google Scholar] [CrossRef] [Green Version]
- WHO. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. Available online: https://apps.who.int/iris/bitstream/handle/10665/85975/WHO_NMH_MND_13.2_eng.pdf?sequence=1 (accessed on 27 February 2020).
- WHO. Body mass index—BMI. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 15 December 2020).
- Institute of Medicine and National Research Council of the National Academies. Weight Gain During Pregnancy: Reexamining the Guidelines; The National Academies Press: Washington, DC, USA, 2009. [Google Scholar] [CrossRef]
- Voigt, M.; Fusch, C.; Olbertz, D.; Hartmann, K.; Rochow, N.; Renken, C.; Schneider, K. Analysis of the neonatal collective in the Federal Republic of Germany 12th report. Presentation of detailed percentiles for the body measurement of newborns. Geburtshilfe Frauenheilkd. 2006, 66, 956–970. [Google Scholar] [CrossRef]
- Ensenauer, R.; Brandlhuber, L.; Burgmann, M.; Sobotzki, C.; Zwafink, C.; Anzill, S.; Holdt, L.; Teupser, D.; Hasbargen, U.; Netz, H.; et al. Obese nondiabetic pregnancies and high maternal glycated hemoglobin at delivery as an indicator of offspring and maternal postpartum risks: The prospective PEACHES mother-child cohort. Clin. Chem. 2015, 61, 1381–1390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Kleinwechter, H.; Ratjen, I.; Demandt, N.; Nolte, A. Gestational diabetes mellitus according to WHO 2013 criteria—Quality analysis of 1074 singleton pregnancies from a specialized outpatient diabetes center (prospective cohort study 2012–2017). Diabetol. Stoffwechs. 2019, 14, 204–217. [Google Scholar] [CrossRef]
- Bianchi, C.; de Gennaro, G.; Romano, M.; Aragona, M.; Battini, L.; Del Prato, S.; Bertolotto, A. Pre-pregnancy obesity, gestational diabetes or gestational weight gain: Which is the strongest predictor of pregnancy outcomes? Diabetes Res. Clin. Pr. 2018, 144, 286–293. [Google Scholar] [CrossRef]
- Boerma, T.; Ronsmans, C.; Melesse, D.Y.; Barros, A.J.D.; Barros, F.C.; Juan, L.; Moller, A.-B.; Say, L.; Hosseinpoor, A.R.; Yi, M.; et al. Global epidemiology of use of and disparities in caesarean sections. Lancet 2018, 392, 1341–1348. [Google Scholar] [CrossRef]
- Liu, Y.; Hou, W.; Meng, X.; Zhao, W.; Pan, J.; Tang, J.; Huang, Y.; Tao, M.; Liu, F. Heterogeneity of insulin resistance and beta cell dysfunction in gestational diabetes mellitus: A prospective cohort study of perinatal outcomes. J. Transl. Med. 2018, 16, 289. [Google Scholar] [CrossRef]
- Barnes, R.A.; Wong, T.; Ross, G.P.; Griffiths, M.M.; Smart, C.E.; Collins, C.E.; MacDonald-Wicks, L.; Flack, J.R. Excessive weight gain before and during gestational diabetes mellitus management: What is the impact? Diabetes Care 2019. [Google Scholar] [CrossRef]
- Hutcheon, J.A.; Stephansson, O.; Cnattingius, S.; Bodnar, L.M.; Wikstrom, A.K.; Johansson, K. Pregnancy weight gain before diagnosis and risk of preeclampsia: A population-based cohort study in nulliparous women. Hypertension 2018, 72, 433–441. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Ness, R.B.; Harger, G.F.; Roberts, J.M. Inflammation and triglycerides partially mediate the effect of prepregnancy body mass index on the risk of preeclampsia. Am. J. Epidemiol. 2005, 162, 1198–1206. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Rogozińska, E.; Zamora, J.; Marlin, N.; Betrán, A.P.; Astrup, A.; Bogaerts, A.; Cecatti, J.G.; Dodd, J.M.; Facchinetti, F.; Geiker, N.R.W.; et al. Gestational weight gain outside the Institute of Medicine recommendations and adverse pregnancy outcomes: Analysis using individual participant data from randomised trials. BMC Pregnancy Childbirth 2019, 19, 322. [Google Scholar] [CrossRef] [PubMed]
- LifeCycle Project-Maternal Obesity and Childhood Outcomes Study Group. Association of gestational weight gain with adverse maternal and infant outcomes. JAMA 2019, 321, 1702–1715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GestDiab, 2017: Auswertung für Gestationsdiabetes. Available online: https://www.windiab.de/gestdiab/ (accessed on 17 April 2020).



{kind=link}
{kind=link}
| Entire Cohort (n = 5789) | Non-GDM (n = 5175) | GDM (n = 614) | p |
|---|---|---|---|
| Maternal age (years) | 30 (27–33) | 31 (28–35) | <0.001 * |
| Parity | 0 (0–0) | 1 (0–1) | <0.001 * |
| Prepregnancy BMI (kg/m2) | 22.5 (20.5–25.3) | 26.6 (23.0–32.2) | <0.001 * |
| BMI categories | 281 (5.4) | 5 (0.8) | <0.001 * |
| BMI < 18.5 kg/m2 (underweight) | 281 (5.4) | 5 (0.8) | |
| BMI 18.5–24.9 kg/m2 (normal weight) | 3514 (67.9) | 246 (40.1) | |
| BMI 25–29.9 kg/m2 (overweight) | 965 (18.6) | 158 (25.7) | |
| BMI 30–34.9 kg/m2 (obesity class I) | 291 (5.6) | 105 (17.1) | |
| BMI 35–39.9 kg/m2 (obesity class II) | 87 (1.7) | 68 (11.1) | |
| BMI ≥ 40 kg/m2 (obesity class III) | 37 (0.7) | 32 (5.2) | |
| GWG (kg) | 15 (11–18) | 12 (8.5–16.6) | <0.001 * |
| Excessive GWG | 2345 (45.3) | 280 (45.6) | 0.89 |
| MBG (mmol/l) | - | 5.8 (5.6–6.1) | |
| HbA1c at delivery in % | - | 5.5 (5.2–5.7) | - |
| HbA1c at delivery in mmol/mol | - | 37 (33–39) | - |
| Insulin treatment | - | 264 (43) | - |
| GA at delivery (weeks) | 39 (39–40) | 39 (38–40) | <0.001 * |
| Birth weight (g) | 3420 (3140–3720) | 3480 (3193–3790) | 0.002 * |
| LGA | 395 (7.6) | 77 (12.8) | <0.001 * |
| SGA | 451 (8.7) | 37 (6.1) | 0.03 * |
| APGAR 5 | 9 (9–10) | 9 (9-10) | 0.278 |
| NICU | 188 (3.6) | 40 (7.1) | <0.001 * |
| Pre-eclampsia | 142 (2.7) | 35 (6.8) | <0.001 * |
| Spontaneous Delivery | 3606 (69.7) | 403 (65.6) | 0.042 * |
| C-section (planned and emergency) | 1164 (22.5) | 182 (29.6) | <0.001 * |
| LGA a | NICU b | Pre-Eclampsia c | CS d | |||||
|---|---|---|---|---|---|---|---|---|
| OR (CI) | p | OR (CI) | p | OR (CI) | p | OR (CI) | p | |
| eGWG | 1.31 (0.99–1.74) | 0.06 | 1.39 (0.93–2.09) | 0.11 | 1.83 * (1.18–2.86) | <0.01 | 1.14 (0.94–1.37) | 0.18 |
| Prepregnancy BMI (kg/m2) | 1.06 * (1.04–1.09) | <0.01 | 1.01 (0.98–1.04) | 0.71 | 1.15 * (1.12–1.18) | <0.01 | 1.05 * (1.04–1.07) | <0.01 |
| GWG (per kg) | 1.07 * (1.05–1.10) | <0.01 | 0.97 (0.93–1.01) | 0.09 | 1.05 * (1.02–1.09) | <0.01 | 1.02 *(1.01–1.04) | 0.01 |
| GDM | 1.45 * (1.07–1.96) | 0.02 | 1.87 * (1.23–2.84) | <0.01 | 1.35 (0.88–2.07) | 0.18 | 1.10 (0.90–1.36) | 0.36 |
| Non-Obese BMI < 30 kg/m2 ( n = 5166) | Obese BMI ≥ 30 kg/m2 ( n = 623) | |||||
|---|---|---|---|---|---|---|
| Non-GDM (n = 4758) | GDM (n = 408) | p# | Non-GDM (n = 417) | GDM (n = 206) | p# | |
| Maternal age (years) | 30 (27–33) | 31 (28–35) | <0.001 * | 30 (26–33) | 31 (27–34) | 0.027 ‡ |
| Parity | 0 (0–1) | 1 (0–1) | 0.003 * | 1 (0–1) | 1 (0–2) | 0.24 |
| Prepregnancy BMI (kg/m2) | 22.1 (20.3–24.4) | 23.9 (21.7–26.6) | <0.001 * | 32.8 (31.1–35.5) | 34.8 (32.2–37.7) | <0.001 * |
| GWG (kg) | 15 (12–18) | 13.7 (9.8–17.3) | <0.001 * | 12 (7–16) | 9.3 (5–14) | <0.001 * |
| eGWG | 2079 (43.7) | 174 (42.6) | 0.716 | 266 (63.8) | 106 (51.5) | 0.004 * |
| HbA1c at time of delivery (%) | - | 5.5 (5.2–5.7) | - | - | 5.5 (5.3–5.7) | - |
| HbA1c at time of delivery (mmol/mol) | - | 37 (33–39) | 37 (34–39) | - | ||
| Insulin treatment (%) | - | 143 (35) | - | - | 121 (58.7) | - |
| GA at delivery (weeks) | 40 (39–40) | 39 (39–40) | 0.004 * | 39 (39–40) | 39 (38–40) | 0.001 * |
| Birth weight (g) | 3420 (3130–3705) | 3465 (3190–3790) | 0.026 * | 3500 (3175–3830) | 3520 (3220–3796) | 0.735 |
| LGA | 348 (7.3) | 52 (13.0) | <0.001 * | 47 (11.3) | 25 (12.4) | 0.690 |
| SGA | 421 (8.9) | 27 (6.7) | 0.166 | 30 (7.2) | 10 (5.0) | 0.383 |
| APGAR 5 | 9 (9–10) | 9 (9–10) | 0.327 | 9 (9–10) | 9 (9–10) | 0.684 |
| NICU | 163 (3.4) | 32 (8.4) | <0.001 * | 25 (6.0) | 8 (4.3) | 0.560 |
| Pre-eclampsia | 105 (2.2) | 14 (4.1) | 0.039 † | 37 (8.9) | 21 (12.6) | 0.220 |
| C-section | 1025 (21.5) | 119 (29.3) | 0.001 * | 139 (33.3) | 63 (30.6) | 0.525 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weschenfelder, F.; Hein, F.; Lehmann, T.; Schleußner, E.; Groten, T. Contributing Factors to Perinatal Outcome in Pregnancies with Gestational Diabetes—What Matters Most? A Retrospective Analysis. J. Clin. Med. 2021, 10, 348. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020348
Weschenfelder F, Hein F, Lehmann T, Schleußner E, Groten T. Contributing Factors to Perinatal Outcome in Pregnancies with Gestational Diabetes—What Matters Most? A Retrospective Analysis. Journal of Clinical Medicine. 2021; 10(2):348. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020348
Chicago/Turabian StyleWeschenfelder, Friederike, Friederike Hein, Thomas Lehmann, Ekkehard Schleußner, and Tanja Groten. 2021. "Contributing Factors to Perinatal Outcome in Pregnancies with Gestational Diabetes—What Matters Most? A Retrospective Analysis" Journal of Clinical Medicine 10, no. 2: 348. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020348