Assessing the Role of Pericardial Fat as a Biomarker Connected to Coronary Calcification—A Deep Learning Based Approach Using Fully Automated Body Composition Analysis

 ,
,  and
and
Abstract
:1. Introduction
1.1. Distinguishing Epicardial and Paracardial Adipose Tissue
1.2. EAT and the Relationship to Coronary Calcification
1.3. PAT Accumulation as a Potential Sign of Cardiovascular Risk in Postmenopausal Women
1.4. AI for Clinical Biomarker Extraction
2. Experimental Section
2.1. Study Design and Study Population
2.2. Dual Source Computed Tomography Examinations and Coronary Calcium Scoring
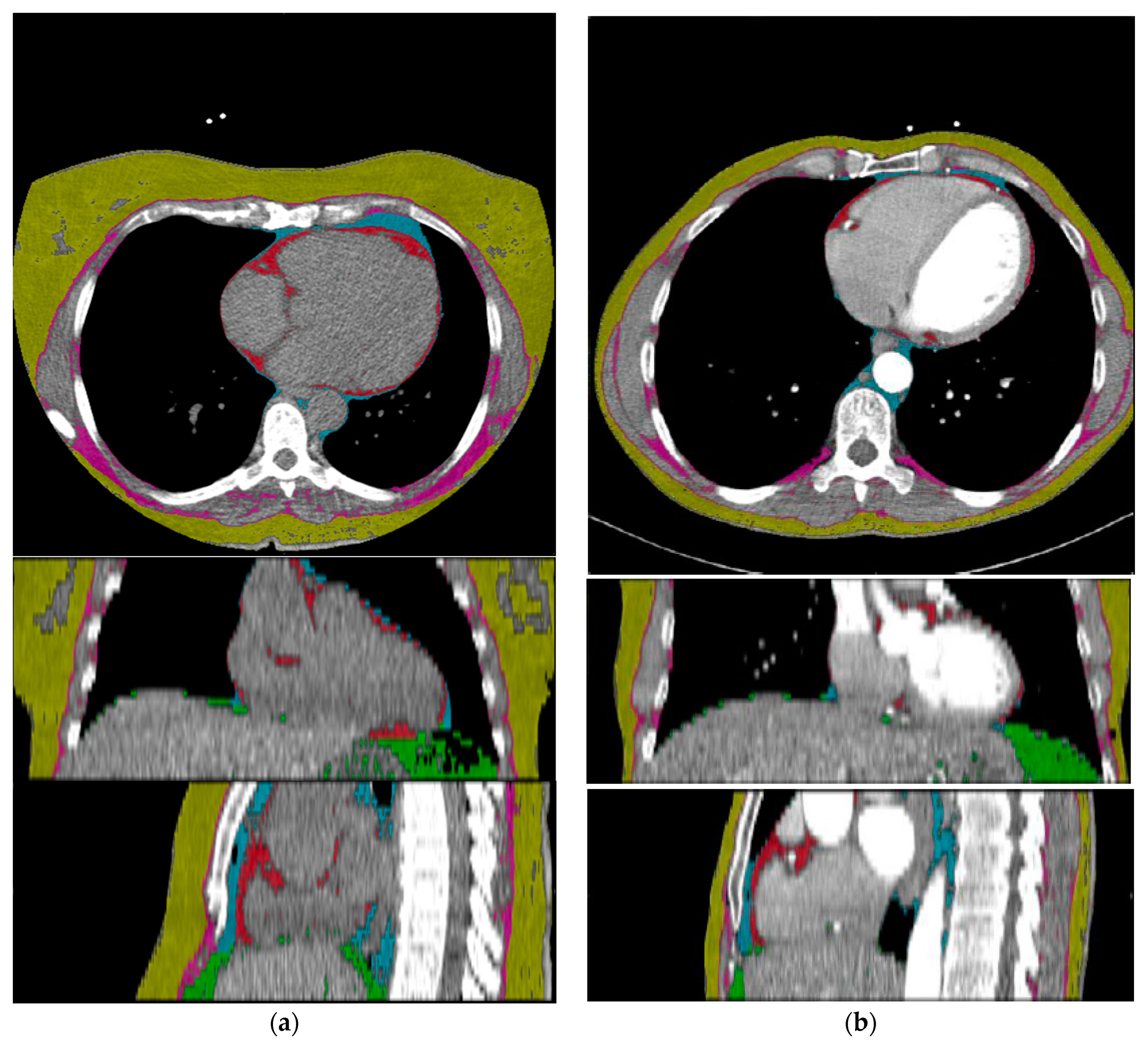
2.3. Deep Learning Architecture
2.4. Quantification of Epicardial Adipose Tissue
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. DL-Network Performance in Tissue Quantification
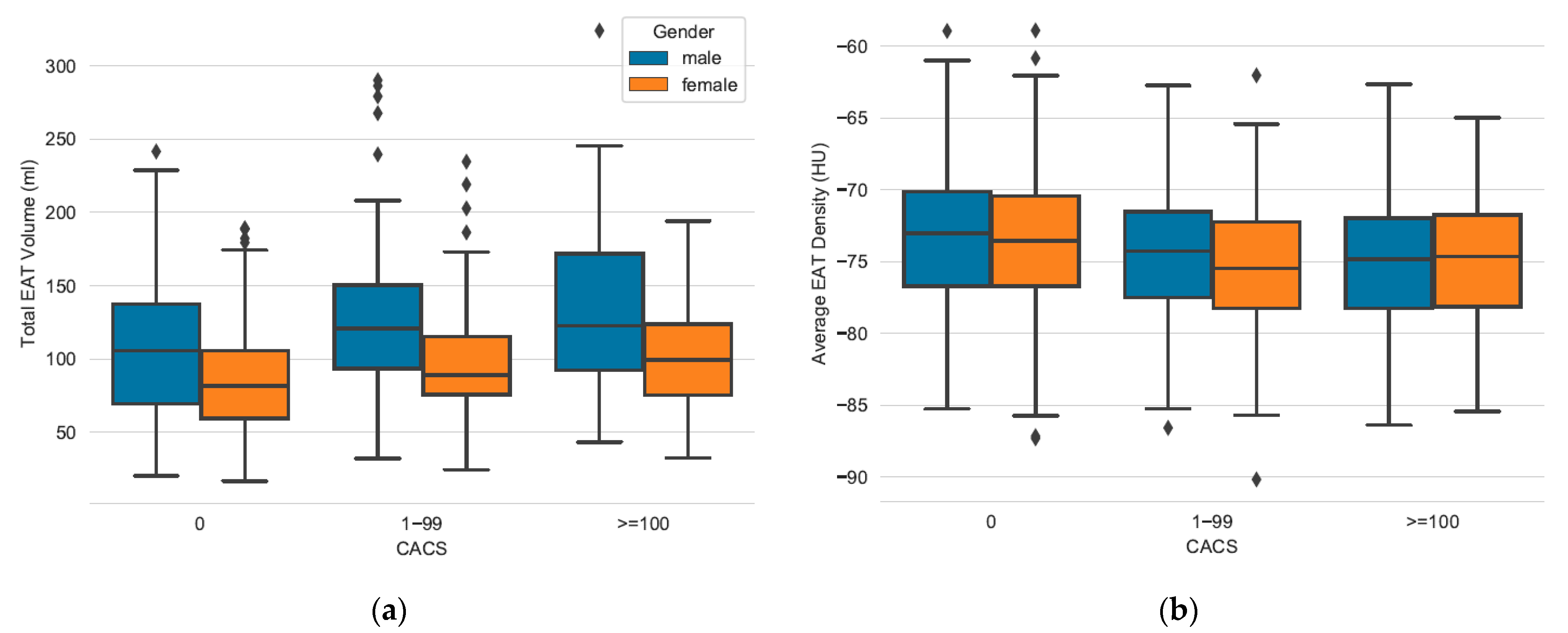
3.3. Measuring EAT and PAT in Relation to CACS
3.4. Secondary Findings: Age Based Comparison of Female Patients between Pericardial Fat and CACS Categories
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BCA | Body Composition Analysis |
| BMI | Body Mass Index |
| CAC | Coronary Artery Calcification |
| CACS | Coronary Artery Calcium Score |
| CAD | Coronary Artery Disease |
| CNN | Computed Neural Network |
| DL | Deep Learning |
| DT | Dunn’s Post Test |
| EAT | Epicardial Adipose Tissue |
| KW-Test | Kruskal-Wallis Test |
| MACE | Major Adverse Cardiac Event |
| PAT | Paracardial Adipose Tissue |
References
- Le Jemtel, T.H.; Samson, R.; Ayinapudi, K.; Singh, T.; Oparil, S. Epicardial Adipose Tissue and Cardiovascular Disease. Curr. Hypertens Rep. 2019, 21, 36. [Google Scholar] [CrossRef] [PubMed]
- Mahabadi, A.A.; Lehmann, N.; Kälsch, H.; Bauer, M.; Dykun, I.; Kara, K.; Moebus, S.; Jöckel, K.H.; Erbel, R.; Möhlenkamp, S. Association of Epicardial Adipose Tissue and Left Atrial Size on Non-Contrast Ct with Atrial Fibrillation: The Heinz Nixdorf Recall Study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Goeller, M.; Achenbach, S.; Marwan, M.; Doris, M.K.; Cadet, S.; Commandeur, F.; Chen, X.; Slomka, P.J.; Gransar, H.; Cao, J.J.; et al. Epicardial Adipose Tissue Density and Volume Are Related to Subclinical Atherosclerosis, Inflammation and Major Adverse Cardiac Events in Asymptomatic Subjects. J. Cardiovasc. Comput. Tomogr. 2018, 12, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazurek, T.; Zhang, L.; Zalewski, A.; Mannion, J.D.; Diehl, J.T.; Arafat, H.; Sarov-Blat, L.; O’Brien, S.; Keiper, E.A.; Johnson, A.G.; et al. Human Epicardial Adipose Tissue Is a Source of Inflammatory Mediators. Circulation 2003, 108, 2460–2466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M. Epicardial Adipose Tissue May Mediate Deleterious Effects of Obesity and Inflammation on the Myocardium. J. Am. Coll. Cardiol. 2018, 71, 2360–2372. [Google Scholar] [CrossRef]
- Villasante Fricke, A.C.; Iacobellis, G. Epicardial Adipose Tissue: Clinical Biomarker of Cardio-Metabolic Risk. Int. J. Mol. Sci. 2019, 20, 5989. [Google Scholar] [CrossRef] [Green Version]
- El Khoudary, S.R.; Shields, K.J.; Janssen, I.; Budoff, M.J.; Everson-Rose, S.A.; Powell, L.H.; Matthews, K.A. Postmenopausal Women with Greater Paracardial Fat Have More Coronary Artery Calcification Than Premenopausal Women: The Study of Women’s Health across the Nation (Swan) Cardiovascular Fat Ancillary Study. J. Am. Heart Assoc. 2017, 6, e004545. [Google Scholar] [CrossRef]
- Bertaso, A.G.; Bertol, D.; Duncan, B.B.; Foppa, M. Epicardial Fat: Definition, Measurements and Systematic Review of Main Outcomes. Arq. Bras. Cardiol. 2013, 101, 18–28. [Google Scholar] [CrossRef]
- Iacobellis, G.; Willens, H.J. Echocardiographic Epicardial Fat: A Review of Research and Clinical Applications. J. Am. Soc. Echocardiogr. 2009, 22. [Google Scholar] [CrossRef]
- Iacobellis, G.; Corradi, D.; Sharma, A.M. Epicardial Adipose Tissue: Anatomic, Biomolecular and Clinical Relationships with the Heart. Nat. Clin. Pract. Cardiovasc. Med. 2005, 10, 536–543. [Google Scholar] [CrossRef]
- Iacobellis, G. Epicardial and Pericardial Fat: Close, but Very Different. Obesity 2009, 17, 625. [Google Scholar] [CrossRef] [PubMed]
- Marchington, J.M.; Mattacks, C.A.; Pond, C.M. Adipose Tissue in the Mammalian Heart and Pericardium: Structure, Foetal Development and Biochemical Properties. Comp. Biochem. Physiol. B 1989, 94, 225–232. [Google Scholar] [CrossRef]
- Forouzandeh, F.; Chang, S.M.; Muhyieddeen, K.; Zaid, R.R.; Trevino, A.R.; Xu, J.; Nabi, F.; Mahmarian, J.J. Does Quantifying Epicardial and Intrathoracic Fat with Noncontrast Computed Tomography Improve Risk Stratification Beyond Calcium Scoring Alone? Circ. Cardiovasc. Imaging 2013, 6, 58–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, C.X.; Ganesan, A.N.; Selvanayagam, J.B. Epicardial Fat and Atrial Fibrillation: Current Evidence, Potential Mechanisms, Clinical Implications, and Future Directions. Eur. Heart J. 2017, 38, 1294–1302. [Google Scholar] [CrossRef] [Green Version]
- Abraham, T.M.; Pedley, A.; Massaro, J.M.; Hoffmann, U.; Fox, C.S. Association between Visceral and Subcutaneous Adipose Depots and Incident Cardiovascular Disease Risk Factors. Circulation 2015, 132, 1639–1647. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, E.; McElhinney, P.A.; Commandeur, F.; Chen, X.; Cadet, S.; Goeller, M.; Razipour, A.; Gransar, H.; Cantu, S.; Miller, R.J.H.; et al. Deep Learning-Based Quantification of Epicardial Adipose Tissue Volume and Attenuation Predicts Major Adverse Cardiovascular Events in Asymptomatic Subjects. Circ. Cardiovasc. Imaging 2020, 13, e009829. [Google Scholar] [CrossRef]
- Lu, M.T.; Park, J.; Ghemigian, K.; Mayrhofer, T.; Puchner, S.B.; Liu, T.; Fleg, J.L.; Udelson, J.E.; Truong, Q.A.; Ferencik, M.; et al. Epicardial and Paracardial Adipose Tissue Volume and Attenuation—Association with High-Risk Coronary Plaque on Computed Tomographic Angiography in the Romicat Ii Trial. Atherosclerosis 2016, 251, 47–54. [Google Scholar] [CrossRef] [Green Version]
- El Khoudary, S.R.; Shields, K.J.; Janssen, I.; Hanley, C.; Budoff, M.J.; Barinas-Mitchell, E.; Everson-Rose, S.A.; Powell, L.H.; Matthews, K.A. Cardiovascular Fat, Menopause, and Sex Hormones in Women: The Swan Cardiovascular Fat Ancillary Study. J. Clin. Endocrinol. Metab. 2015, 100, 3304–3312. [Google Scholar] [CrossRef]
- Koitka, S.; Kroll, L.; Malamutmann, E.; Oezcelik, A.; Nensa, F. Fully Automated Body Composition Analysis in Routine Ct Imaging Using 3d Semantic Segmentation Convolutional Neural Networks. Eur. Radiol. 2020. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Graffy, P.M.; Zea, R.; Lee, S.J.; Liu, J.; Sandfort, V.; Summers, R.M. Automated Ct Biomarkers for Opportunistic Prediction of Future Cardiovascular Events and Mortality in an Asymptomatic Screening Population: A Retrospective Cohort Study. Lancet Digit. Health. 2020, 2, e192–e200. [Google Scholar] [CrossRef]
- Commandeur, F.; Goeller, M.; Razipour, A.; Cadet, S.; Hell, M.M.; Kwiecinski, J.; Chen, X.; Chang, H.J.; Marwan, M.; Achenbach, S.; et al. Fully Automated Ct Quantification of Epicardial Adipose Tissue by Deep Learning: A Multicenter Study. Radiol. Artif. Intell. 2019, 1, e190045. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of Coronary Heart Disease Using Risk Factor Categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achenbach, S.; Barkhausen, J.; Beer, M.; Beerbaum, P.; Dill, T.; Eichhorn, J.; Fratz, S.; Gutberlet, M.; Hoffmann, M.; Huber, A.; et al. Konsensusempfehlungen Der Drg/Dgk/Dgpk Zum Einsatz Der Herzbildgebung Mit Computertomographie Und Magnetresonanztomographie. Kardiologe 2012, 6, 105–125. [Google Scholar] [CrossRef]
- Greenland, P.; LaBree, L.; Azen, S.P.; Doherty, T.M.; Detrano, R.C. Coronary Artery Calcium Score Combined with Framingham Score for Risk Prediction in Asymptomatic Individuals. JAMA 2004, 291, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausleiter, J.; Meyer, T.; Hadamitzky, M.; Huber, E.; Zankl, M.; Martinoff, S.; Kastrati, A.; Schömig, A. Radiation Dose Estimates from Cardiac Multislice Computed Tomography in Daily Practice: Impact of Different Scanning Protocols on Effective Dose Estimates. Circulation 2006, 113, 1305–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of Coronary Artery Calcium Using Ultrafast Computed Tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Mahabadi, A.A.; Berg, M.H.; Lehmann, N.; Kälsch, H.; Bauer, M.; Kara, K.; Dragano, N.; Moebus, S.; Jöckel, K.H.; Erbel, R.; et al. Association of Epicardial Fat with Cardiovascular Risk Factors and Incident Myocardial Infarction in the General Population: The Heinz Nixdorf Recall Study. J. Am. Coll Cardiol. 2013, 61, 1388–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arad, Y.; Goodman, K.J.; Roth, M.; Newstein, D.; Guerci, A.D. Coronary Calcification, Coronary Disease Risk Factors, C-Reactive Protein, and Atherosclerotic Cardiovascular Disease Events: The St. Francis Heart Study. J. Am. Coll. Cardiol. 2005, 46, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Aubrey, J.; Esfandiari, N.; Baracos, V.E.; Buteau, F.A.; Frenette, J.; Putman, C.T.; Mazurak, V.C. Measurement of Skeletal Muscle Radiation Attenuation and Basis of Its Biological Variation. Acta Physiol. 2014, 210, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J. Scipy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [Green Version]
- Dunn, O.J. Multiple Comparisons Using Rank Sums. Technometrics 1964, 6, 241–252. [Google Scholar] [CrossRef]
- Daan, N.M.; Fauser, B.C. Menopause Prediction and Potential Implications. Maturitas 2015, 82, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Mancio, J.; Azevedo, D.; Saraiva, F.; Azevedo, A.I.; Pires-Morais, G.; Leite-Moreira, A.; Falcao-Pires, I.; Lunet, N.; Bettencourt, N. Epicardial Adipose Tissue Volume Assessed by Computed Tomography and Coronary Artery Disease: A Systematic Review and Meta-Analysis. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 490–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Numeric Value |
|---|---|
| No. of examined patients | 966 (334 male/632 female) |
| Age | 59.3 ± 9.6 years |
| BMI (kg/m2) | 26.9 ± 4.7 |
| CACS 0 | 526 (134 male/392 female) |
| CACS 1–99 | 293 (126 male/167 female) |
| CACS ≥100 | 147 (74 male/73 female) |
| CACS Category | Mean Value (b/m/f) | Standard Deviation (b/m/f) | 95%-CI (b/m/f) |
|---|---|---|---|
| Epicardial Adipose Tissue (EAT)vol (mL) | |||
| 0 | 90.44/108.1/84.44 | 38.39/46.28/33.29 | [87.15, 93.73]/[100.1, 115.91]/[81.13, 87.74] |
| 1–99 | 108.25/124.35/96.11 | 44.68/49.71/36.15 | [103.12, 113.39]/[115.58, 133.11]/[90.6, 101.63] |
| ≥100 | 118.25/134.07/102.21 | 50.61/57.55/36.29 | [110.0, 126.5]/[120.74, 147.4]/[93.74, 110.68] |
| EATatt (HU) | |||
| 0 | −73.48/−73.25/−73.56 | 4.72/4.72/4.73 | [−73.89, −73.08]/[−74.06, −72.45]/[−74.03, −73.09] |
| 1–99 | −74.95/−74.46/−75.32 | 4.59/4.6/4.57 | [−75.48, −74.42]/[−75.28, −73.65]/[−76.02, −74.62] |
| ≥100 | −75.08/−75.33/−74.83 | 5.03/5.41/4.64 | [−75.9, −74.26]/[−76.59, −74.08]/[−75.91, −73.742] |
| Paracardial Adipose Tissue (PAT)vol (mL) | |||
| 0 | 130.77/193.8/109.23 | 78.67/98.23/56.57 | [124.03, 137.51]/[177.02, 210.59]/[103.61, 114.85] |
| 1–99 | 171.76/223.51/132.72 | 93.77/99.62/66.55) | [160.99, 182.55]/[205.95, 241.08]/[122.56, 142.89] |
| ≥100 | 200.46/260.34/139.76 | 116.6/127.09/61.43 | [181.45, 219.47]/[230.89, 289.78]/[125.43, 154.1] |
| PATatt (HU) | |||
| 0 | −95.58/−97.78/−94.82 | 6.02/6.67/5.6 | [−96.09, −95.06]/[−98.92, −96.64]/[−95.38, −94.27] |
| 1–99 | −98.05/−99.88/−96.66 | 5.95/5.96/5.57 | [−98.73, −97.36]/[−100.93, −98.83]/[−97.51, −95.81] |
| ≥100 | −98.44/−100.93/−95.91 | 6.39/6.62/5.05 | [−99.48, −97.4]/[−102.47, −99.4]/[−97.09, −94.73] |
| BMI (m/kg2) | |||
| 0 | 26.49/27.7/26.06 | 4.8/4.29/4.91 | [26.02, 26.96]/[25.49, 26.62]/[26.88, 28.52] |
| 1–99 | 27.52/28.19/26.93 | 5.37/4.14/6.22 | [26.79, 28.26]/[25.76, 28.16]/[27.36, 29.02] |
| ≥100 | 26.67/26.44/26.89 | 4.01/3.28/4.7 | [25.9, 27.45]/[25.12, 27.763]/[26.0, 27.78] |
| Age (years) | |||
| 0 | 53.8/50.13/55.06 | 9.87/9.92/9.55 | [52.96, 54.65]/[48.44, 51.83]/[54.11, 56.01] |
| 1–99 | 59.89/55.76/63.01 | 9.42/8.4/8.95 | [58.81, 60.97]/[54.27, 57.24]/[61.64, 64.38] |
| ≥100 | 64.19/61.51/66.91 | 9.43/9.67/8.4 | [62.65, 65.73]/[59.27, 63.75]/[64.95, 68.87] |
| Feature | Gender (b/m/f) | Kruskal-Wallis Test | Dunn’s Test CACS 0 vs. 1–99 | Dunn’s Test CACS 1–99 vs. >100 |
|---|---|---|---|---|
| EATvol (mL) | ||||
| Male | <0.01 | <0.01 | 0.37 | |
| Female | <0.001 | <0.001 | 0.18 | |
| Both | <0.001 | <0.001 | 0.08 | |
| EATatt (HU) | ||||
| Male | 0.02 | 0.06 | 0.35 | |
| Female | <0.001 | <0.001 | 0.40 | |
| Both | <0.001 | <0.001 | 0.98 | |
| PATvol (mL) | ||||
| Male | <0.001 | <0.01 | 0.10 | |
| Female | <0.001 | <0.001 | 0.29 | |
| Both | <0.001 | <0.001 | 0.05 | |
| PATatt (HU) | ||||
| Male | <0.01 | <0.01 | 0.38 | |
| Female | <0.001 | <0.001 | 0.38 | |
| Both | <0.001 | <0.001 | 0.84 | |
| BMI (m/kg2) | ||||
| Male | 0.18 | N/A | N/A | |
| Female | 0.35 | N/A | N/A | |
| Both | 0.03 | N/A | N/A | |
| Age (years) | ||||
| Male | <0.001 | <0.001 | <0.001 | |
| Female | <0.001 | <0.001 | <0.01 | |
| Both | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kroll, L.; Nassenstein, K.; Jochims, M.; Koitka, S.; Nensa, F. Assessing the Role of Pericardial Fat as a Biomarker Connected to Coronary Calcification—A Deep Learning Based Approach Using Fully Automated Body Composition Analysis. J. Clin. Med. 2021, 10, 356. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020356
Kroll L, Nassenstein K, Jochims M, Koitka S, Nensa F. Assessing the Role of Pericardial Fat as a Biomarker Connected to Coronary Calcification—A Deep Learning Based Approach Using Fully Automated Body Composition Analysis. Journal of Clinical Medicine. 2021; 10(2):356. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020356
Chicago/Turabian StyleKroll, Lennard, Kai Nassenstein, Markus Jochims, Sven Koitka, and Felix Nensa. 2021. "Assessing the Role of Pericardial Fat as a Biomarker Connected to Coronary Calcification—A Deep Learning Based Approach Using Fully Automated Body Composition Analysis" Journal of Clinical Medicine 10, no. 2: 356. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020356