Semi-Quantitative Characterization of Post-Transplant Lymphoproliferative Disorder Morphological Subtypes with [18F]FDG PET/CT

 ,
,  ,
,
Abstract
:1. Introduction
2. Research Design
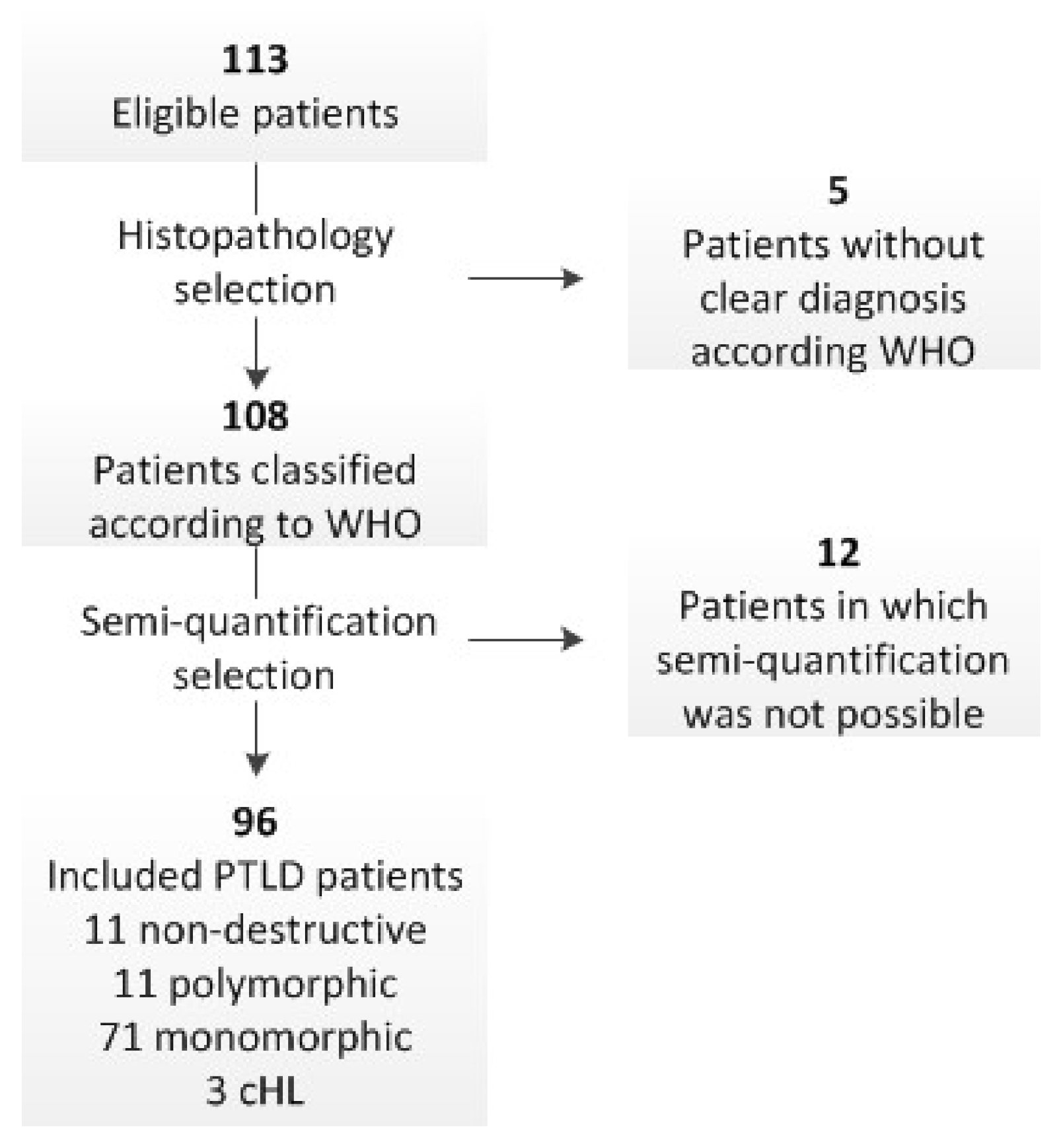
2.1. Patient Selection
2.2. [18F]FDG PET/CT Acquisition
2.3. [18F]FDG PET/CT Semi-Quantification
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
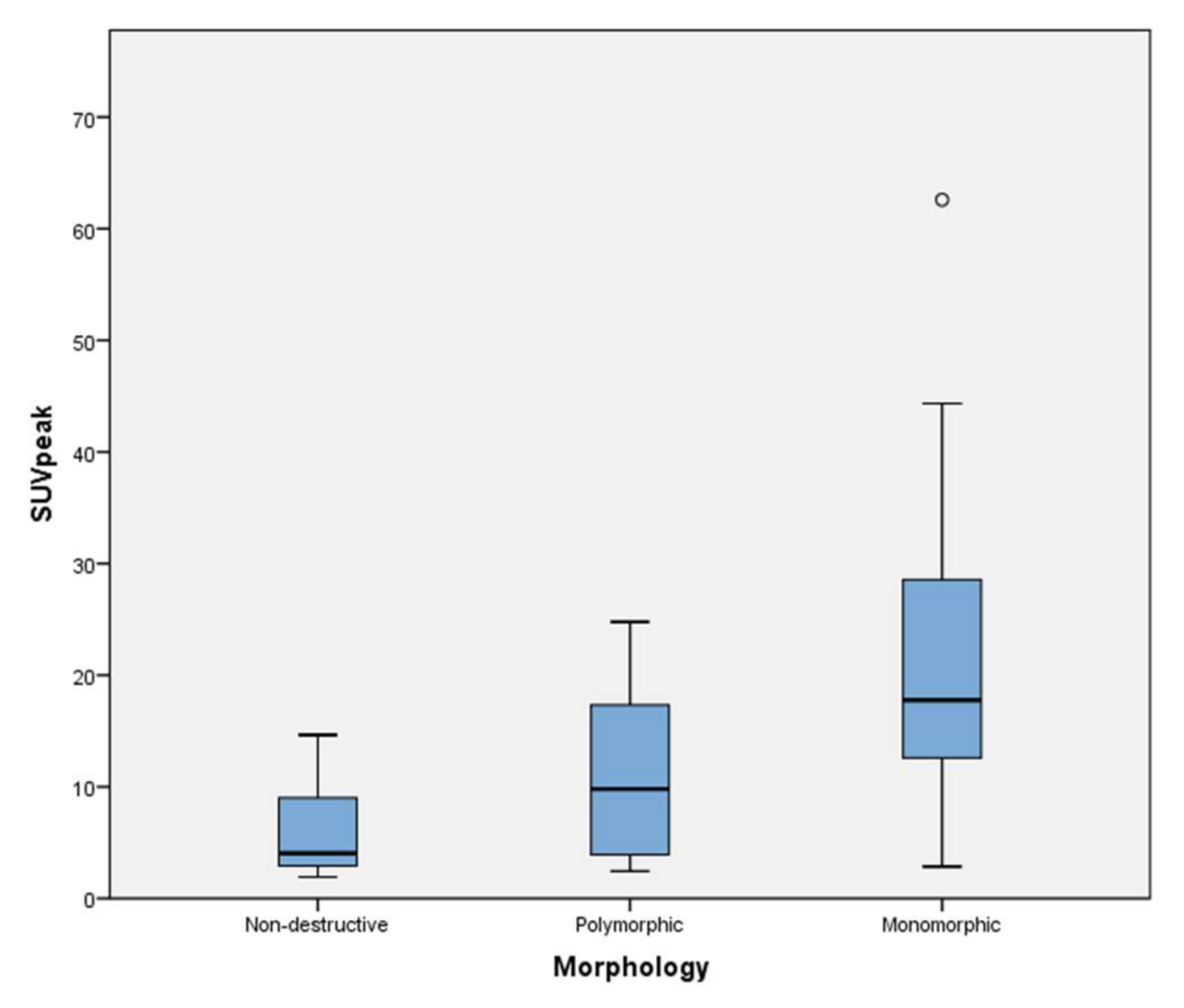
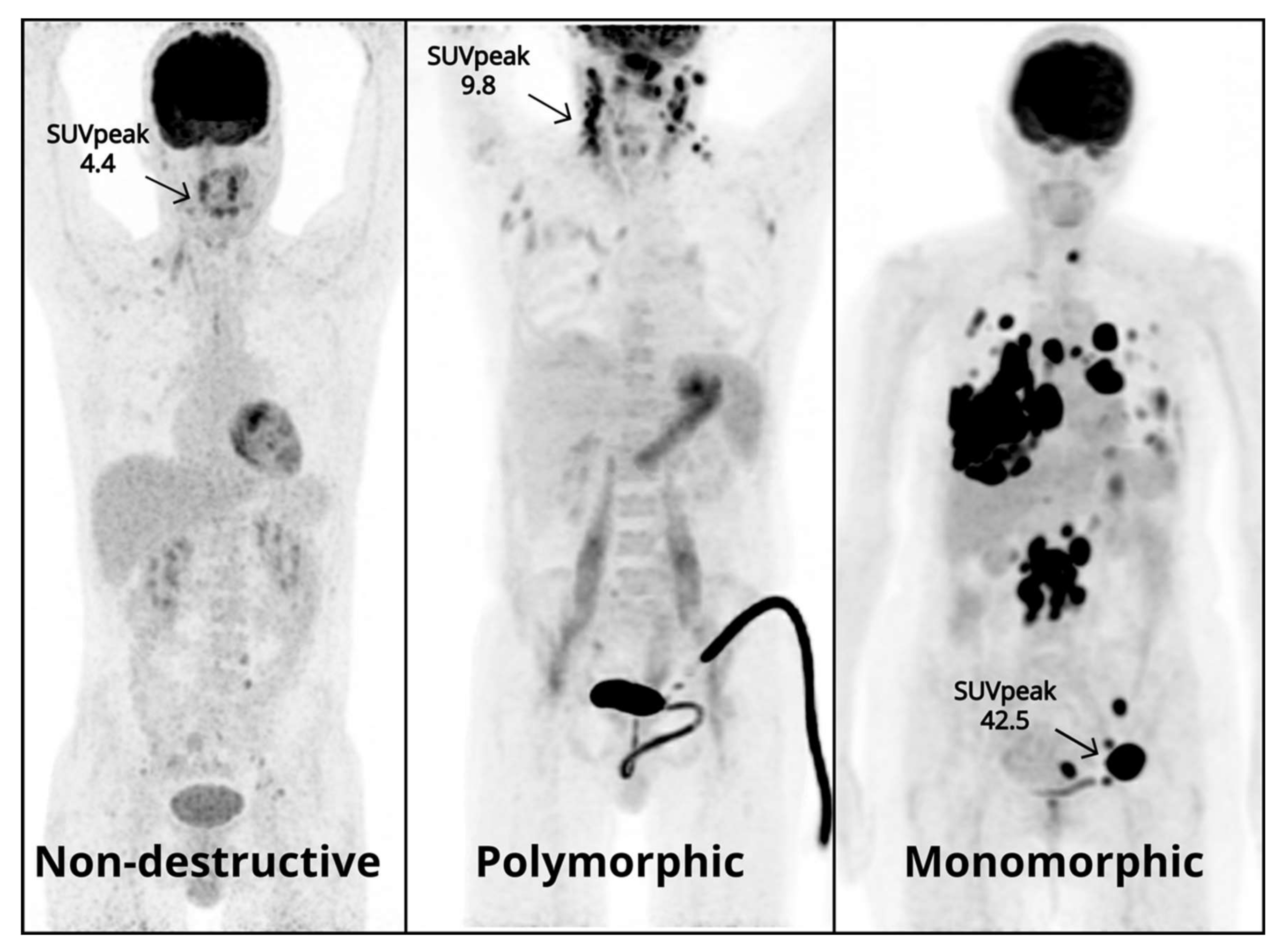
3.2. Semi-Quantitative Measurements
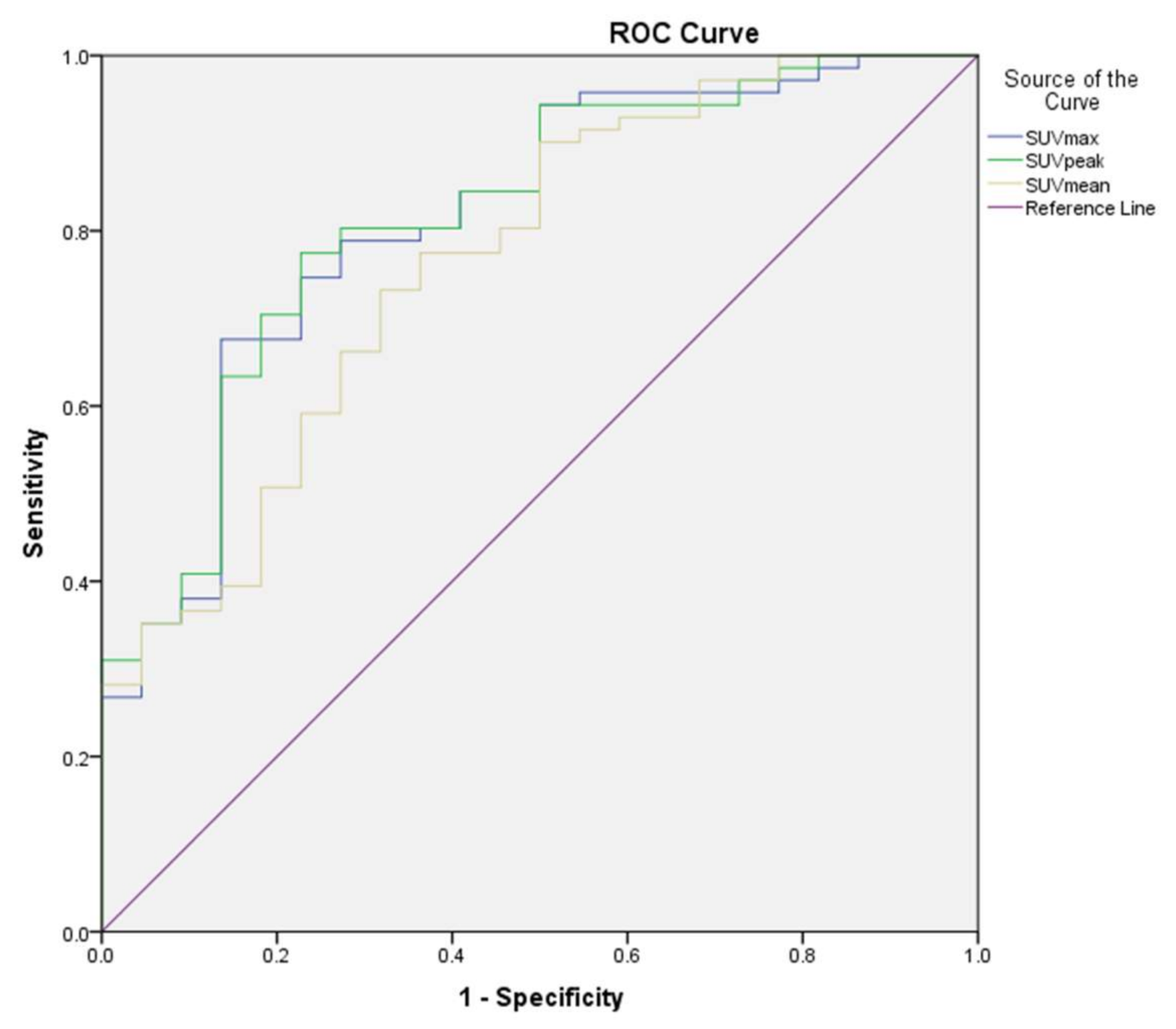
3.3. Receiver Operating Characteristic Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Faull, R.J.; Hollett, P.; McDonald, S.P. Lymphoproliferative Disease after Renal Transplantation in Australia and New Zealand. Transplantation 2005, 80, 193–197. [Google Scholar] [CrossRef]
- Dharnidharka, V.R.; Ruzinova, M.B.; Chen, C.; Parameswaran, P.; O’Gorman, H.; Goss, C.W.; Gu, H.; Storch, G.A.; Wylie, K. Metagenomic analysis of DNA viruses from posttransplant lymphoproliferative disorders. Cancer Med. 2019, 8, 1013–1023. [Google Scholar] [CrossRef]
- Marcelis, L.; Tousseyn, T. The Tumor Microenvironment in Post-Transplant Lymphoproliferative Disorders. Cancer Microenviron. 2019, 12, 3–16. [Google Scholar] [CrossRef]
- Oertel, S.H.; Verschuuren, E.; Reinke, P.; Zeidler, K.; Papp-Váry, M.; Babel, N.; Trappe, R.U.; Jonas, S.; Hummel, M. Anagnostopoulos, Effect of Anti-CD 20 Antibody Rituximab in Patients with Post-Transplant Lymphoproliferative Disorder (PTLD). Arab. Archaeol. Epigr. 2005, 5, 2901–2906. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. (Eds.) World Health Organ Calssification Tumours Haematop Lymphoid Tissues, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017; pp. 453–462. [Google Scholar]
- Chiou, F.K.; Sharif, K.; Perera, T.; Muiesan, P.; Vickers, M.; Beath, S.; Morland, B.; Mirza, D.; Gupte, G. Poorer Long-Term Survival Associ-ated with Monomorphic Post-Transplant Lymphoproliferative Disorder After Solid Organ Transplantation in Children. Transplantation 2018, 102, S457–S458. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Hassan, A.; Paessler, M.E.; Frater, J.L.; Kreisel, F.H. Pathologic and Clinical Features of Hodgkin Lymphoma—Like Posttransplant Lymphoproliferative Disease. Int. J. Surg. Pathol. 2009, 18, 278–285. [Google Scholar] [CrossRef]
- Trappe, R.; Oertel, S.; Leblond, V.; Mollee, P.; Sender, M.; Reinke, P.; Neuhaus, R.; Lehmkuhl, H.; Horst, H.A.; Salles, G.; et al. Sequential treatment with rituxi-mab followed by CHOP chemotherapy in adult B-cell post-transplant lymphoproliferative disorder (PTLD): The prospective international multicentre phase 2 PTLD-1 trial. Lancet Oncol. 2012, 13, 196–206. [Google Scholar] [CrossRef]
- Ballova, V.; Muoio, B.; Albano, D.; Bertagna, F.; Canziani, L.; Ghielmini, M.; Ceriani, L.; Treglia, G. Diagnostic Performance of 18F-FDG PET or PET/CT for Detection of Post-Transplant Lymphoproliferative Disorder: A Systematic Review and a Bivariate Meta-Analysis. Diagnostics 2020, 10, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montes de Jesus, F.M.; Kwee, T.C.; Nijland, M.; Kahle, X.U.; Huls, G.; Dierckx, R.A.J.O.; van Meerten, T.; Gheysens, O.; Dierickx, D.; Vergote, V.; et al. Performance of advanced imaging modalities at diagnosis and treatment response evaluation of patients with post-transplant lymphoproliferative disorder: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2018, 132, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Keppler, J.S.; Conti, P.S. A Cost Analysis of Positron Emission Tomography. Am. J. Roentgenol. 2001, 177, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Montes de Jesus, F.M.; Kwee, T.C.; Kahle, X.U.; Nijland, M.; van Meerten, T.; Huls, G.; Dierckx, R.A.J.O.; Rosati, S.; Diepstra, A.; van der Bij, W.; et al. Diagnostic per-formance of FDG-PET/CT of post-transplant lymphoproliferative disorder and factors affecting diagnostic yield. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 529–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montes de Jesus, F.M.; Glaudemans, A.W.J.M.; Tissing, W.J.; Dierckx, R.A.J.O.; Rosati, S.; Diepstra, A.; Noordzij, W.; Kwee, T.C. 18 F-FDG PET/CT in the Diagnostic and Treatment Evaluation of Pediatric Posttransplant Lymphoprolifera-tive Disorders. J. Nucl. Med. 2020, 61, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Dierickx, D.; Tousseyn, T.; Requilé, A.; Verscuren, R.; Sagaert, X.; Morscio, J.; Wlodarska, I.; Herreman, A.; Kuypers, D.; Van Cleemput, J.; et al. The accuracy of positron emission tomography in the detection of posttransplant lymphoproliferative disorder. Haematologica 2012, 98, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Ngeow, J.Y.Y.; Quek, R.H.H.; Ng, D.C.E.; Hee, S.W.; Tao, M.; Lim, L.C.; Tan, Y.H.; Lim, S.T. High SUV uptake on FDG–PET/CT predicts for an aggressive B-cell lymphoma in a prospective study of primary FDG–PET/CT staging in lymphoma. Ann. Oncol. 2009, 20, 1543–1547. [Google Scholar] [CrossRef]
- Chihara, D.; Oki, Y.; Onoda, H.; Taji, H.; Yamamoto, K.; Tamaki, T.; Morishima, Y. High maximum standard uptake value (SUVmax) on PET scan is associated with shorter survival in patients with diffuse large B cell lymphoma. Int. J. Hematol. 2011, 93, 502–508. [Google Scholar] [CrossRef]
- Takehana, C.S.; Twist, C.J.; Mosci, C.; Quon, A.; Mittra, E.; Iagaru, A. 18F-FDG PET/CT in the management of patients with post-transplant lymphoproliferative disorder. Nucl. Med. Commun. 2014, 35, 276–281. [Google Scholar] [CrossRef]
- Vali, R.; Punnett, A.; Bajno, L.; Moineddin, R.; Shammas, A. The value of 18 F-FDG PET in pediatric pa-tients with post-transplant lymphoproliferative disorder at initial diagnosis. Pediatr. Transplant. 2015, 19, 932–939. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3067. [Google Scholar] [CrossRef]
- Boellaard, R.; Oyen, W.J.G.; Hoekstra, C.J.; Hoekstra, O.S.; Visser, E.P.; Willemsen, A.T.; Arends, B.; Verzijlbergen, F.J.; Zijlstra, J.; Paans, A.M.; et al. The Netherlands protocol for standardisation and quantification of FDG whole body PET studies in multi-centre trials. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 2320–2333. [Google Scholar] [CrossRef] [Green Version]
- Boellaard, R.; Willemsen, A.; Arends, B.; Visser, E.P. EARL Procedure for Assessing PET/CT System Specific Patient FDG Activity Preparations for Quantitative FDG PET/ct Studies. Available online: http://earl.eanm.org/html/img/pool/EARL-procedure-for-optimizing-FDG-activity-for-quantitative-FDG-PET-studies_version_1_1.pdf (accessed on 15 June 2020).
- Aide, N.; Lasnon, C.; Veit-Haibach, P.; Sera, T.; Sattler, B.; Boellaard, R. EANM/EARL harmonization strate-gies in PET quantification: From daily practice to multicentre oncological studies. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Kaalep, A.; Sera, T.; Oyen, W.; Krause, B.J.; Chiti, A.; Liu, Y.; Boellaard, R. EANM/EARL FDG-PET/CT accreditation-summary results from the first 200 accredited imaging systems. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 412–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleves, M.A. Comparative Assessment of Three Common Algorithms for Estimating the Variance of the Area under the Nonparametric Receiver Operating Characteristic Curve. Stata J. Promot. Commun. Stat. Stata 2002, 2, 280–289. [Google Scholar] [CrossRef] [Green Version]
- Dierickx, D.; Tousseyn, T.; Gheysens, O. How I treat posttransplant lymphoproliferative disorders. Blood 2015, 126, 2274–2283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radhakrishnan, R.K.; Mittal, B.R.; Gorla, A.K.R.; Basher, R.K.; Sood, A.; Bal, A.; Kalra, N.; Khandelwal, N.; Singh, N. Digambar Behera 4 Real-time intraprocedural 18F-FDG PET/CT-guided biopsy using automated robopsy arm (ARA) in the diagnostic evaluation of tho-racic lesions with prior inconclusive biopsy results: Initial experience from a tertiary health care centre. Br. J. Radiol. 2017, 90, 20170258. [Google Scholar] [CrossRef] [PubMed]
- Broccoli, A.; Nanni, C.; Cappelli, A.; Bacci, F.; Gasbarrini, A.; Zanoni, L.; Brocchi, S.; Spagnolo, S.; Piovani, C.; Argnani, L.; et al. Pet/Ct-Guided Biopsy For The Diagnosis Of Lymphoma. Hematol. Oncol. 2017, 35, 425. [Google Scholar] [CrossRef] [Green Version]
- Menter, T.; Juskevicius, D.; Alikian, M.; Steiger, J.; Dirnhofer, S.; Tzankov, A.; Naresh, K.N. Mutational landscape of B-cell post-transplant lymphoproliferative disorders. Br. J. Haematol. 2017, 178, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Morscio, J.; Dierickx, D.; Tousseyn, T. Molecular Pathogenesis of B-Cell Posttransplant Lymphoprolif-erative Disorder: What Do We Know So Far? Clin. Dev. Immunol. 2013, 2013, 150835. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-W.; Lin, C.-Y.; Ho, C.-M.; Chang, Y.-S.; Yang, S.-F.; Kao, C.; Chang, J.-G. Genetic Alterations in Colorectal Cancer Have Different Patterns on 18F-FDG PET/CT. Clin. Nucl. Med. 2015, 40, 621–626. [Google Scholar] [CrossRef]
- Voorhees, T.J.; Kannan, K.K.; Galeotti, J.; Grover, N.; Vaidya, R.; Moore, D.T.; Montgomery, N.D.; Beaven, A.; Dittus, C. Identification of high-risk monomorphic post-transplant lymphoproliferative disorder following solid organ transplantation. Leuk. Lymphoma 2021, 62, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.; Bowles, K.; Bradley, J.A.; Emery, V.; Featherstone, C.; Gupte, G.; Marcus, R.; Parameshwar, J.; Ramsay, A.; Newstead, C. Diagnosis of post-transplant lymphoproliferative disorder in solid organ transplant recipients-BCSH and BTS Guidelines. Br. J. Haematol. 2010, 149, 675–692. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.; Tan, X.; Ke, Q.; Cen, H. Prognostic value of baseline metabolic tumor volume and total lesion gly-colysis in patients with lymphoma: A meta-analysis. Woloschak GE, editor. PLoS ONE 2019, 14, e0210224. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at Diagnosis (Years) | |
|---|---|
| Median | 50 |
| Range | 1–80 |
| IQR | 39 |
| Gender | |
| Male | 55 (58%) |
| Female | 40 (42%) |
| Transplanted organ | |
| Kidney | 32 (33.6%) |
| Lung | 21 (22.1%) |
| Liver | 17 (17.9%) |
| HSCT | 11 (11.6%) |
| Heart | 7 (7.4%) |
| Multi-organ | 7 (7.4%) |
| Histology | |
| Nondestructive | 11 (11.5%) |
| Polymorphic | 11 (11.5%) |
| Monomorphic | 71 (76%) |
| Diffuse Large B-cell | 50 (70.4%) |
| Plasmacytoma-like | 8 (11.3%) |
| Burkitt | 7 (9.9%) |
| T-cell | 1 (1.4%) |
| Other/Unclear | 5 (7%) |
| Classic Hodgkin Lymphoma | 3 (3%) |
| Semi-Quantification | Median | IQR | Min | Max |
|---|---|---|---|---|
| SUVmax | ||||
| Nondestructive (n = 11) | 5.1 | 6.8 | 2.5 | 17.7 |
| Polymorphic (n = 11) | 13.2 | 15.9 | 3.3 | 31.1 |
| Monomorphic (n = 71) | 20.9 | 16 | 3.4 | 69.3 |
| Classic Hodgkin Lymphoma (n = 3) | 7.6 | 6.2 | 10.2 | |
| SUVpeak | ||||
| Nondestructive (n = 11) | 4.1 | 6.1 | 1.9 | 14.6 |
| Polymorphic (n = 11) | 9.8 | 13.4 | 2.4 | 24.8 |
| Monomorphic (n = 71) | 17.8 | 16 | 2.9 | 62.6 |
| Classic Hodgkin Lymphoma (n = 3) | 6.7 | 4.2 | 9.4 | |
| SUVmean | ||||
| Nondestructive (n = 11) | 4 | 4.2 | 1.3 | 11.3 |
| Polymorphic (n = 11) | 6.2 | 6.1 | 2.2 | 12.9 |
| Monomorphic (n = 71) | 9.4 | 7.8 | 2.5 | 22.9 |
| Classic Hodgkin Lymphoma (n = 3) | 5.3 | 4.3 | 6.9 |
| Semi-Quantification | p-Value |
|---|---|
| SUVmax | |
| Nondestructive vs. Polymorphic | 0.41 |
| Nondestructive vs. Monomorphic | 0.01 |
| Polymorphic vs. Monomorphic | 0.06 |
| SUVpeak | |
| Nondestructive vs. Polymorphic | 0.52 |
| Nondestructive vs. Monomorphic | 0.01 |
| Polymorphic vs. Monomorphic | 0.04 |
| SUVmean | |
| Nondestructive vs. Polymorphic | 0.79 |
| Nondestructive vs. Monomorphic | 0.01 |
| Polymorphic vs. Monomorphic | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montes de Jesus, F.; Vergote, V.; Noordzij, W.; Dierickx, D.; Dierckx, R.; Diepstra, A.; Tousseyn, T.; Gheysens, O.; Kwee, T.; Deroose, C.; et al. Semi-Quantitative Characterization of Post-Transplant Lymphoproliferative Disorder Morphological Subtypes with [18F]FDG PET/CT. J. Clin. Med. 2021, 10, 361. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020361
Montes de Jesus F, Vergote V, Noordzij W, Dierickx D, Dierckx R, Diepstra A, Tousseyn T, Gheysens O, Kwee T, Deroose C, et al. Semi-Quantitative Characterization of Post-Transplant Lymphoproliferative Disorder Morphological Subtypes with [18F]FDG PET/CT. Journal of Clinical Medicine. 2021; 10(2):361. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020361
Chicago/Turabian StyleMontes de Jesus, Filipe, Vibeke Vergote, Walter Noordzij, Daan Dierickx, Rudi Dierckx, Arjan Diepstra, Thomas Tousseyn, Olivier Gheysens, Thomas Kwee, Christophe Deroose, and et al. 2021. "Semi-Quantitative Characterization of Post-Transplant Lymphoproliferative Disorder Morphological Subtypes with [18F]FDG PET/CT" Journal of Clinical Medicine 10, no. 2: 361. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020361