The European Perspective on the Management of Acute Major Hemorrhage and Coagulopathy after Trauma: Summary of the 2019 Updated European Guideline

Abstract
:1. Introduction
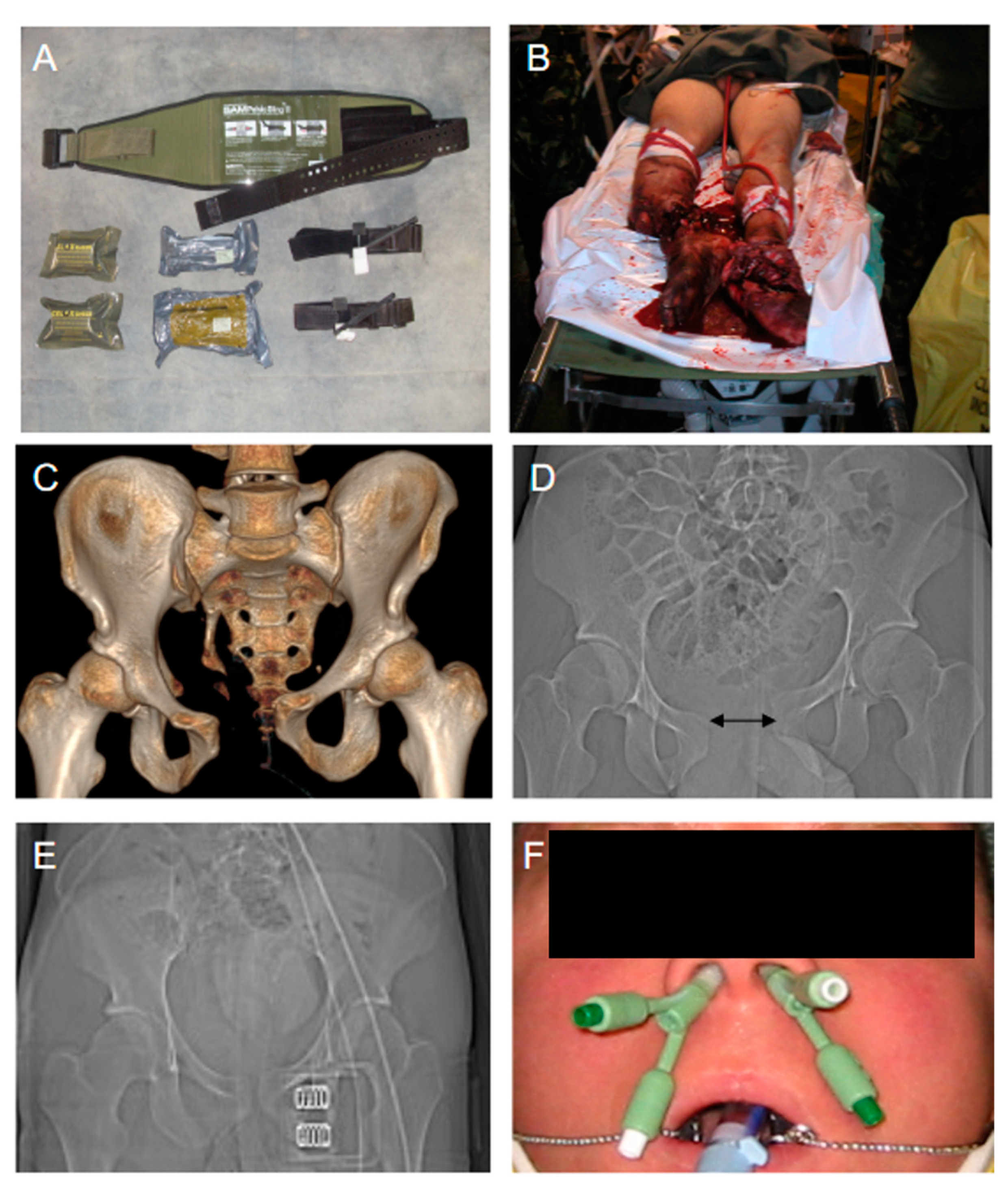
2. Prehospital Management of Trauma Hemorrhage
- Application of tourniquets.
- Limitation of prehospital transport time < 60 min.
- Early use of blood products.
3. Rapid Transport to Specialized Trauma Centers
4. In-Hospital Management of Traumatic Bleeding and Coagulopathy
4.1. Clinical Assessment and Immediate Surgical Bleeding Control
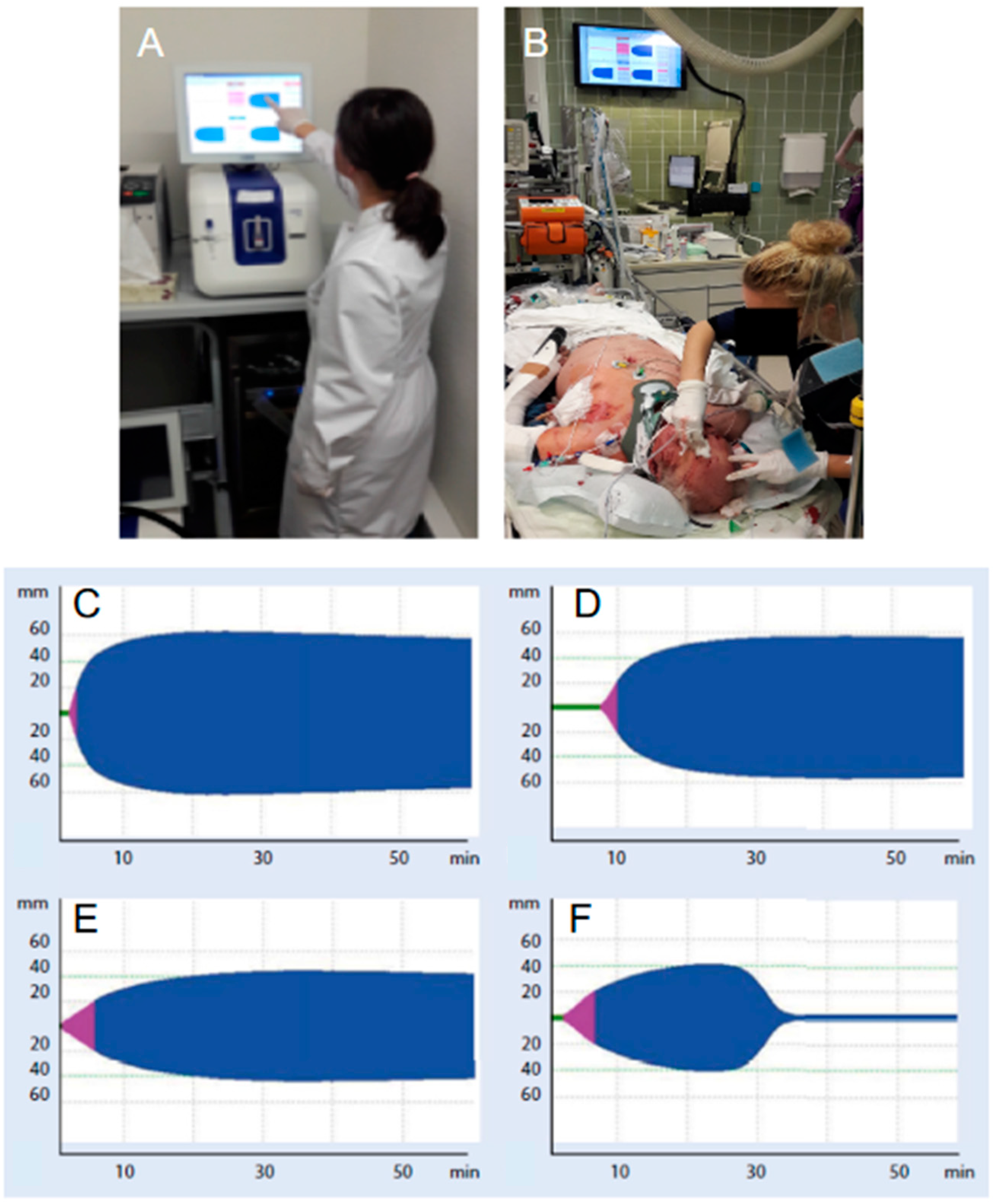
4.2. Rapid Detection and Diagnosis of Coagulopathies
4.3. Acute “Goal-Directed” Coagulation Therapies
5. Hyperfibrinolysis and Tranexamic Acid (TXA)
6. Fibrinogen and Coagulation Factors
7. Bleeding Trauma Patients on Preinjury Anticoagulants
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cannon, J.W. Hemorrhagic Shock. N. Engl. J. Med. 2018, 378, 370–379. [Google Scholar] [CrossRef]
- Schoeneberg, C.; Schilling, M.; Hussmann, B.; Schmitz, D.; Lendemans, S.; Rucholtz, S. Preventable and potentially preventable deaths in severely injured patients: A retrospective analysis including patterns of errors. Eur. J. Trauma Emerg. Surg. 2017, 43, 481–489. [Google Scholar] [CrossRef]
- Oyeniyi, B.T.; Fox, E.E.; Scerbo, M.; Tomasek, J.S.; Wade, C.E.; Holcomb, J.B. Trends in 1029 trauma deaths at a level 1 trauma center: Impact of a bleeding control bundle of care. Injury 2017, 48, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fröhlich, M.; Mutschler, M.; Caspers, M.; Nienaber, U.; Jäcker, V.; Driessen, A.; Bouillon, B.; Maegele, M. Trauma-induced coagulopathy upon emergency room arrival: Still a significant problem despite increased awareness and management? Eur. J. Trauma Emerg. Surg. 2019, 45, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.; Cardenas, J.C.; Wade, C.E.; Holcomb, J.B. Advances in the under-standing of trauma-induced coagulopathy. Blood 2016, 128, 1043–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kornblith, L.; Moore, H.; Cohen, M. Trauma-induced coagulopathy: Past, present and future. J. Thromb. Haemost. 2019, 17, 852–862. [Google Scholar] [CrossRef] [PubMed]
- AWMF. S3-Leitlinie Polytrauma/Schwerverletzten-Behandlung Register-Nr. 012/019. Available online: www.awmf.org/leitlinien/detail/ll/012-019.html (accessed on 30 May 2019).
- Spahn, D.R.; Bouillon, B.; Černý, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Maegele, M.; Nardi, G.; Riddez, L.; et al. The European guideline on management of major bleeding and coagulopathy following trauma: Fifth edition. Crit. Care 2019, 23, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, R.; Kerby, J.; Kalkwarf, K.; Van Belle, G.; Fox, E.E.; Cotton, B.A.; Cohen, M.J.; Schreiber, M.A.; Brasel, K.; Bulger, E.M.; et al. Earlier time to hemostasis is associated with decreased mortality and role of complications: Results from the pragmatic randomized optimal platelet and plasma ratio trial. J. Trauma Acute Care Surg. 2019, 87, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, N.; Driessen, A.; Fröhlich, M.; Stürmer, E.K.; Maegele, M. and TACTIC partners. Diversity in clinical man-agement and protocols for the treatment of major bleeding trauma patients across European level I trauma centres. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 74. [Google Scholar] [CrossRef]
- Fuller, G.; Bouamra, O.; Woodford, M.; Jenks, T.; Stanworth, S.; Allard, S.; Coats, T.J.; Brohi, K.; Lecky, F. Recent massive blood transfusion practice in England and Wales: View from a trauma registry. Emerg. Med. J. 2012, 29, 118–123. [Google Scholar] [CrossRef]
- Etchill, E.; Sperry, J.; Zuckerbraun, B.; Alarcon, L.; Brown, J.; Schuster, K.; Kaplan, L.; Piper, G.; Peitzman, A.; Neal, M. The confusion continues: Results from an American Association for the Surgery in Trauma survey on massive transfusion practices among United States trauma centers. Transfusion 2016, 56, 2478–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunn, A.; Fischer, P.; Sing, R.; Templin, M.; Avery, M.; Christmas, A.B. Improvement of treatment outcomes after implementation of a massive transfusion protocol: A level 1 trauma center experience. Am. Surg. 2017, 83, 394–398. [Google Scholar] [CrossRef]
- Bawazeer, M.A.; Ahmed, N.; Izadi, H.; McFarlan, A.; Nathens, A.B.; Pavenski, K. Compliance with a massive transfusion protocol (MTP) impacts patient outcome. Injury 2015, 46, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Hwang, K.; Kwon, J.; Cho, J.; Heo, Y.; Lee, J.C.-J.; Jung, K. Implementation of Trauma Center and Massive Transfusion Protocol Improves Outcomes for Major Trauma Patients: A Study at a Single Institution in Korea. World J. Surg. 2018, 42, 2067–2075. [Google Scholar] [CrossRef] [PubMed]
- Spahn, D.; Cerny, V.; Coats, T.; Duranteau, J.; Fernandez-Mondejar, E.; Gordini, G.; Stahel, P.F.; Hunt, B.J.; Komadina, R.; Neugebauer, E.A.M.; et al. Management of bleeding following major trauma: A European guideline. Crit. Care 2007, 11, R17. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Gutterman, D.; Baumann, M.H.; Addrizzo-Harris, D.; Hylek, E.M.; Philipps, B.; Raskob, G.; Zelman Lewis, S.; Schünemann, H. Grading strength of recommendations and quality of evidence in clinical guidelines: Report from an American College of Chest Physicians task force. Chest 2006, 129, 174–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helm, M.; Kulla, M.; Ströhr, A.; Josse, F.; Hossfeld, B. Prähospitales Management Traumatischer Blutungen: Maßnahmen gGemäß der S3-Leitlinie Polytrauma zur Lokalen Blutungskontrolle. Notfall Rettungsmedizin. 2018. Available online: www.springermedizin.de/praehospitales-management-traumatischerblutungen/15781652 (accessed on 30 May 2019).
- Kulla, M.; Bernhard, M.; Hink, D.; Schweigkofler, U.; Helm, M.; Hossfeld, B. Treatment options for the critical bleeding in the out-of-hospital setting. Der Notarzt. 2015, 31, 47–53. [Google Scholar]
- Smith, A.A.; Ochoa, J.E.; Wong, S.; Beatty, S.; Elder, S.; Guidry, C.; McGrew, P.; McGuiness, C.; Duchesne, J.; Schroll, R. Prehospital tourniquet use in penetrating extremity trauma: Decreased blood transfusions and limb complications. J. Trauma Acute Care Surg. 2019, 86, 43–51. [Google Scholar] [CrossRef]
- Felix, S.; Hanschen, M.; Biberthaler, P. Blutungskontrolle bei Beckenverletzungen. Trauma Berufskrankh 2016, 18, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Culemann, U.; Ostern, H.J.; Pohlemann, T. Current treatment of pelvic ring fractures. Unfallchirurg 2014, 117, 145–159. [Google Scholar] [CrossRef]
- Hsu, S.-D.; Chen, C.-J.; Chou, Y.-C.; Wang, S.-H.; Chan, D.-C. Effect of Early Pelvic Binder Use in the Emergency Management of Suspected Pelvic Trauma: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esmer, E.; Esmer, E.; Derst, P.; Schulz, M.; Siekmann, H.; Delank, K.S. Influence of external pelvic stabilization on hemodynamically unstable pelvic fracture. Unfallchirurg 2017, 120, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Shackelford, S.A.; Del Junco, D.J.; Powell-Dunford, N.; Mazuchowski, E.L.; Howard, J.T.; Kotwal, R.S.; Gurney, J.; Butler, F.K.; Gross, K.; Stockinger, Z.T. Association of Prehospital Blood Product Transfusion During Medical Evacuation of Combat Casualties in Afghanistan With Acute and 30-Day Survival. JAMA 2017, 318, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Sperry, J.L.; Guyette, F.X.; Brown, J.B.; Yazer, M.H.; Triulzi, D.J.; Early-Young, B.J.; Adams, P.W.; Daley, B.J.; Miller, R.S.; Harbrecht, B.G.; et al. Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock. N. Engl. J. Med. 2018, 379, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.B.; Moore, E.E.; Chapman, M.P.; McVaney, K.; Bryskiewicz, G.; Blechar, R.; Chin, T.; Burlew, C.C.; Pieracci, F.; West, F.B.; et al. Plasma-first resuscitation to treat haemorrhagic shock during emergency ground transportation in an urban area: A randomized trial. Lancet 2018, 392, 283–291. [Google Scholar] [CrossRef]
- Fenger-Eriksen, C.; Fries, D.; David, J.S.; Bouzat, P.; Lance, M.D.; Grottke, O.; Spahn, D.R.; Schoechl, H.; Maegele, M. Pre-hospital plasma transfusion: A valuable coagulation support or an expensive fluid therapy? Crit. Care 2019, 23, 238. [Google Scholar] [CrossRef] [Green Version]
- Howard, J.T.; Kotwal, R.S.; Stern, C.A.; Janak, J.C.; Mazuchowski, E.L.; Butler, F.K.; Stockinger, Z.T.; Holcomb, B.R.; Bono, R.C.; Smith, D.J. Use of Combat Casualty Care Data to Assess the US Military Trauma System During the Afghanistan and Iraq Conflicts, 2001–2017. JAMA Surg. 2019, 154, 600–608. [Google Scholar] [CrossRef]
- Mutschler, M.; Nienaber, U.; Brockamp, T.; Wafaisade, A.; Wyen, H.; Peiniger, S.; Paffrath, T.; Bouillon, B.; Maegele, M. A critical reappraisal of the ATLS classification of hypovolaemic shock: Does it really reflect clinical reality? Resuscitation 2013, 84, 309–313. [Google Scholar] [CrossRef]
- American College of Surgeons Committee on Trauma. ATLS Student Manual, 10th ed.; American College of Surgeons: Chicago, IL, USA, 2018. [Google Scholar]
- Standl, T.G.; Annecke, T.; Cascorbi, I.; Heller, A.R.; Sabashnikov, A.; Teske, W. The Nomenclature, Definition and Distinction of Types of Shock. Dtsch. Aerzteblatt Online 2018, 115, 757–768. [Google Scholar] [CrossRef]
- Maegele, M. Moderne Gerinnungstherapie beim blutenden Schwerverletzten. Med. Klin. Intensivmed. Notfmed. 2019, 114, 400–409. [Google Scholar] [CrossRef]
- Gratz, J.; Güting, H.; Thorn, S.; Brazinova, A.; Görlinger, K.; Schäfer, N.; Schöchl, H.; Stanworth, S.; Maegele, M. Protocolised thromboelastometric-guided haemostatic management in patients with traumatic brain injury: A pilot study. Anaesthesia 2019, 74, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Wikkelsø, A.; Wetterslev, J.; Møller, A.M.; Afshari, A. Thromboelastography (TEG) or thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults or children with bleeding. Cochrane Database Syst. Rev. 2016, 22, CD007871. [Google Scholar] [CrossRef] [Green Version]
- Inaba, K.; Rizoli, S.; Veigas, P.V.; Callum, J.; Davenport, R.; Hess, J.; Maegele, M. Viscoelastic Testing in Trauma Consensus Panel. Consensus conference on viscoelastic test-based transfusion guidelines for early trauma resuscitation: Report of the panel. J. Trauma Acute Care Surg. 2015, 78, 1220–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gall, L.; Brohi, K.; Davenport, R.A. Diagnosis and treatment of hyperfibrinolydsis in trauma (A European perspective). Semin. Thromb. Hemost. 2017, 43, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Mannucci, P.M. The neverending success story of tranexamic acid in aquired bleeding. Haematologica 2020, 105, 1201–1205. [Google Scholar] [CrossRef]
- CRASH-2 Trial Collaborators; Shakur, H.; Roberts, I.; Bautista, R.; Caballero, J.; Coats, T.; Dewan, Y.; El-Sayed, H.; Gogichaishvili, T.; Gupta, S.; et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. Lancet 2010, 376, 23–32. [Google Scholar] [CrossRef]
- Guyette, F.X.; Brown, J.B.; Zenati, M.S.; Early-Young, B.J.; Adams, P.W.; Eastridge, B.J.; Nirula, R.; Vercruysse, G.A.; O’Keeffe, T.; Joseph, B.; et al. Tranexamic Acid During Prehospital Transport in Patients at Risk for Hemorrhage After Injury. JAMA Surg. 2020. [Google Scholar] [CrossRef]
- Rowell, S.E.; Meier, E.N.; McKnight, B.; Kannas, D.; May, S.; Sheehan, K.; Bulger, E.M.; Idris, A.H.; Christenson, J.; Morrison, L.J.; et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients with Moderate or Severe Traumatic Brain Injury. JAMA 2020, 324, 961–974. [Google Scholar] [CrossRef]
- Spinella, P.C.; Thomas, K.A.; Turnbull, I.R.; Fuchs, A.; Bochicchio, K.; Schuerer, D.; Reese, S.; Centeno, A.A.C.; Horn, C.B.; Baty, J.; et al. The Immunologic Effect of Early Intravenous Two and Four Gram Bolus Dosing of Tranexamic Acid Compared to Placebo in Patients With Severe Traumatic Bleeding (TAMPITI): A Randomized, Double-Blind, Placebo-Controlled, Single-Center Trial. Front. Immunol. 2020, 11. [Google Scholar] [CrossRef]
- Floccard, B.; Rugeri, L.; Faure, A.; Saint Denis, M.; Boyle, E.M.; Peguet, O.; Levrat, A.; Guillaume, C.; Marcotte, G.; Vulliez, A.; et al. Early coagulopathy in trauma patients: An on-scene and hospital admission study. Injury 2012, 43, 26–32. [Google Scholar] [CrossRef]
- Morrison, J.J.; Ross, J.D.; Dubose, J.J.; Jansen, J.O.; Midwater, M.; Rasmussen, T.E. Association of cryoprecipitate and tranexamic acid with improved survival following wartime injury: Findings from the MATTERs II Study. JAMA Surg. 2013, 148, 218–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juffermans, N.P.; Wirtz, M.R.; Balvers, K.; Baksaas-Aasen, K.; van Dieren, S.; Gaarder, T.; Naess, P.A.; Stanworth, S.; Johansson, P.I.; Stensballe, J.; et al. Towards patient-specific management of trauma hemorrhage: The effect of resuscitation therapy on parameters of thromboelastometry. J. Thromb. Haemost. 2019, 17, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, F.; Kozar, R.A. Fibrinogen Protects Against Barrier Dysfunction Through Maintaining Cell Surface Syndecan-1 In Vitro. Shock 2019, 51, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Maegele, M.; Grottke, O.; Schöchl, H.; Sakowitz, O.; Spannagl, M.; Koscielny, J. Direct oral anticoagulants in emergency trauma admissions—Perioperative management, and handling hemorrhage. Dtsch Arztebl. Int. 2016, 113, 575–582. [Google Scholar] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade of Recommendation | Benefit/Risk | Evidence |
|---|---|---|
| 1A Strong recommendation, high-quality evidence | Benefits clearly outweigh risks and vice versa | RCTs without important limitations; overwhelming evidence provided by observational studies |
| 1B Strong recommendation, moderate-quality evidence | Benefits clearly outweigh risks and vice versa | RCTs with important limitations, e.g., inconsistent results, methodological problems, being indirect, or being imprecise; strong evidence provided by observational studies |
| 1C Strong recommendation, (very) low-quality evidence | Benefits clearly outweigh risks and vice versa | Observational studies or case series |
| 2A Weak recommendation, high-quality evidence | Benefits balanced with risks | RCTs without important limitations; overwhelming evidence provided by observational studies |
| 2B Weak recommendation, moderate-quality evidence | Benefits balanced with risks and burden | RCTs with important limitations, e.g., inconsistent results, methodological problems, indirect or imprecise; strong evidence provided by observational studies |
| 2C Weak recommendation, (very) low-quality evidence | Uncertainty for benefits and risks; both maybe closely balanced | Observational studies or case series |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maegele, M. The European Perspective on the Management of Acute Major Hemorrhage and Coagulopathy after Trauma: Summary of the 2019 Updated European Guideline. J. Clin. Med. 2021, 10, 362. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020362
Maegele M. The European Perspective on the Management of Acute Major Hemorrhage and Coagulopathy after Trauma: Summary of the 2019 Updated European Guideline. Journal of Clinical Medicine. 2021; 10(2):362. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020362
Chicago/Turabian StyleMaegele, Marc. 2021. "The European Perspective on the Management of Acute Major Hemorrhage and Coagulopathy after Trauma: Summary of the 2019 Updated European Guideline" Journal of Clinical Medicine 10, no. 2: 362. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020362