Dermatological Manifestations in Inflammatory Bowel Diseases

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Experimental Section
3. Classification
- Specific manifestations with the same histological features of the underlying IBD;
- Mucocutaneous disorders associated with IBDs;
- Reactive manifestations of IBDs due to immunological mechanisms triggered by common antigens shared by gut bacteria and skin;
- Mucocutaneous conditions secondary to the treatment of IBDs;
- Manifestations due to nutritional malabsorption.
3.1. Specific Manifestations with the Same Histological Features of the Underlying Inflammatory Bowel Disease
3.1.1. Continuous/Contiguous Lesions
3.1.2. Metastatic Crohn’s Disease
3.2. Mucocutaneous Disorders Associated with IBD
3.2.1. Aphthous Stomatitis
3.2.2. Erythema Nodosum
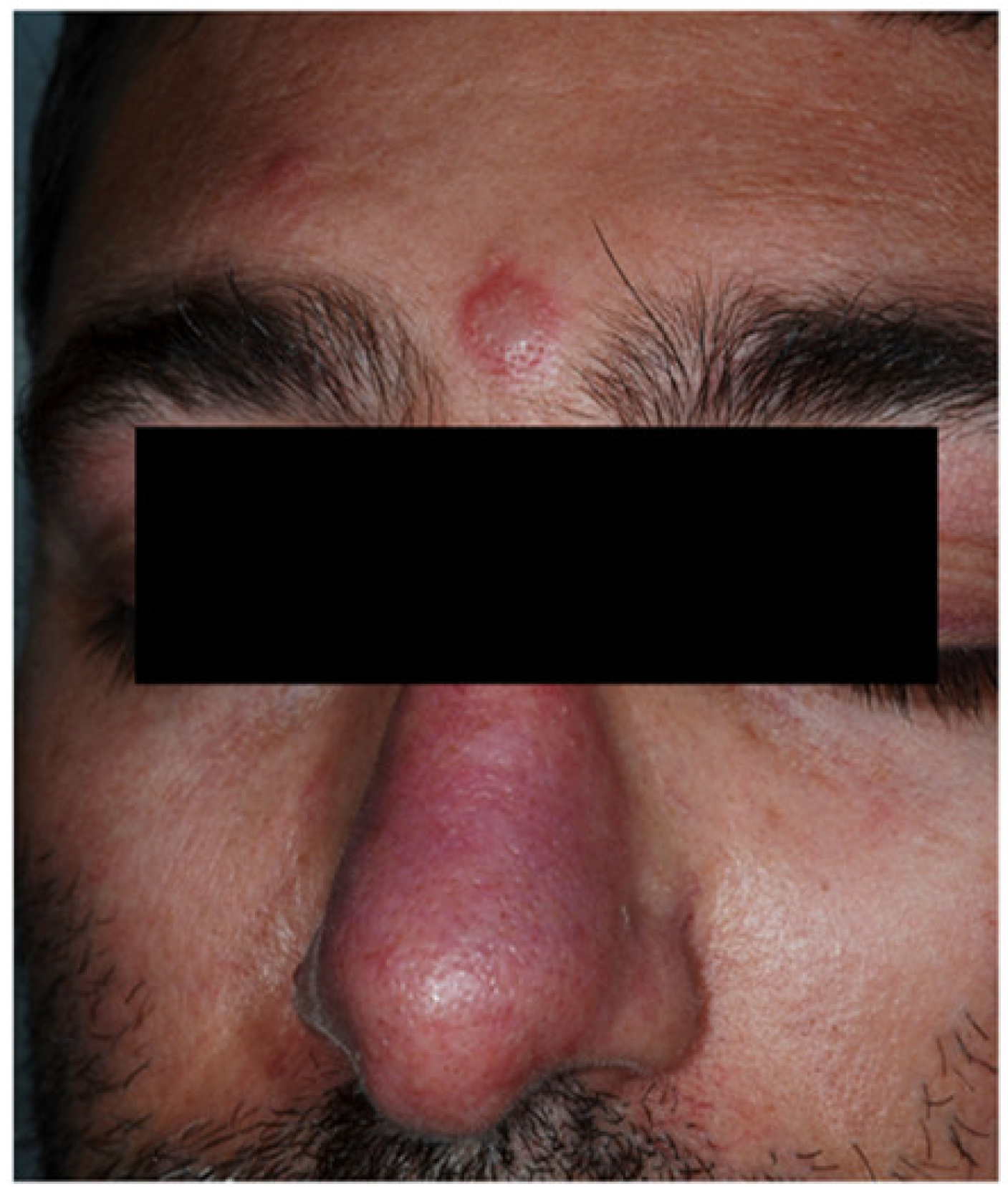
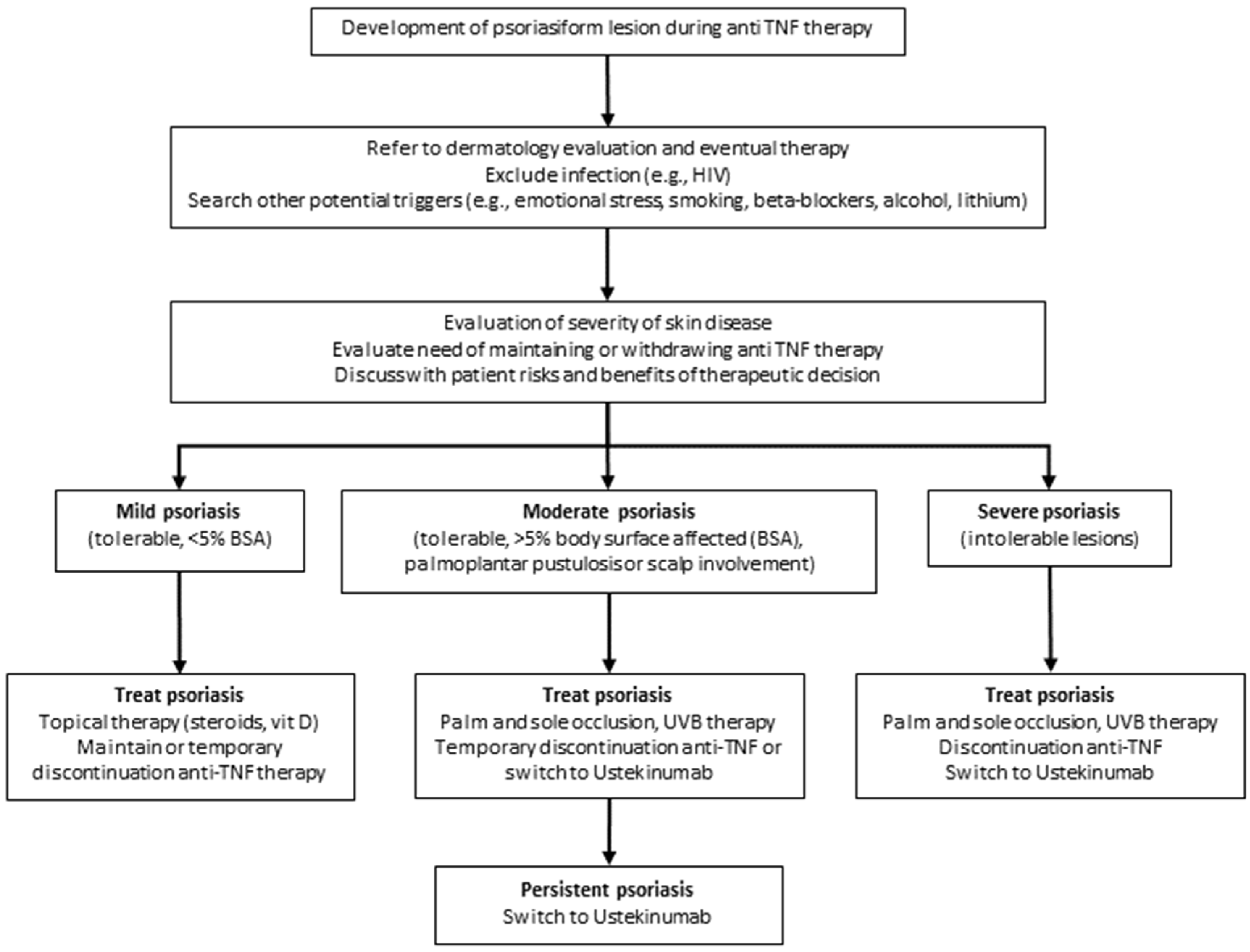
3.2.3. Psoriasis
3.2.4. Epidermolysis Bullosa Acquisita
3.3. Reactive Mucocutaneous Manifestation of IBD
3.3.1. Pyoderma Gangrenosum
3.3.2. Sweet’s Syndrome
3.3.3. Bowel-Associated Dermatosis-Arthritis Syndrome
3.3.4. Aseptic Abscess Syndrome
3.3.5. Pyodermatitis–pyostomatitis Vegetans
3.3.6. SAPHO and PAPA Syndromes
3.4. Mucocutaneous Conditions Secondary to IBD Treatment
3.4.1. Adverse Mucocutaneous Reactions
3.4.2. Infectious Complications
3.4.3. Skin Cancers
3.5. Manifestations Due to Nutritional Malabsorption
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Harbord, M.; Annese, V.; Vavricka, S.R.; Allez, M.; Acosta, M.B.-D.; Boberg, K.M.; Burisch, J.; De Vos, M.; De Vries, A.-M.; Dick, A.D.; et al. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. J. Crohn’s Colitis 2016, 10, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, S.R.; Brun, L.; Ballabeni, P.; Pittet, V.; Vavricka, B.M.P.; Zeitz, J.; Rogler, G.; Schoepfer, A.M. Frequency and risk factors for extraintestinal manifestations in the Swiss inflammatory bowel disease Cohort. Am. J. Gastroenterol. 2011, 106, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Rankin, G.B.; Watts, H.D.; Melnyk, C.S.; Kelley, M.L., Jr. National cooperative Crohn’s disease study: Extraintestinal manifestations and perianal complications. Gastroenterology 1979, 77, 914–920. [Google Scholar] [CrossRef]
- Veloso, F.T.; Carvalho, J.; Magro, F. Immune-related systemic manifestations of inflammatory bowel disease. A prospective study of 792 patients. J. Clin. Gastroenterol. 1996, 23, 29–34. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Blanchard, J.F.; Rawsthorne, P.; Yu, N. The prevalence of extraintestinal diseases in inflammatory bowel disease: A population-based study. Am. J. Gastroenterol. 2001, 96, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Ricart, E.; Panaccione, R.; Loftus, E.V., Jr.; Tremaine, W.J.; Harmsen, W.S.; Zinsmeister, A.R.; Sandborn, W.J. Autoimmune disorders and extraintestinal manifestations in first-degree familial and sporadic inflammatory bowel disease: A case-control study. Inflamm. Bowel Dis. 2004, 10, 207–214. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Wajda, A.; Blanchard, J.F. The clustering of other chronic inflammatory diseases in inflammatory bowel disease: A population-based study. Gastroenterology 2005, 129, 827–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenstein, A.J.; Janowitz, H.D.; Sachar, D.B. The extra-intestinal complications of Crohn’s disease and ulcerative colitis: A study of 700 patients. Medicine 1976, 55, 401–412. [Google Scholar] [CrossRef]
- Burgdorf, W. Cutaneous manifestations of Crohn’s disease. J. Am. Acad. Dermatol. 1981, 5, 689–695. [Google Scholar] [CrossRef]
- Palamaras, I.; El-Jabbour, J.; Pietropaolo, N.; Thomson, P.; Mann, S.; Robles, W.; Stevens, H.P. Metastatic Crohn’s disease: A review. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1033–1043. [Google Scholar] [CrossRef]
- Larsen, S.; Bendtzen, K.; Nielsen, O.H. Extraintestinal manifestations of inflammatory bowel disease: Epidemiology, diagnosis, and management. Ann. Med. 2010, 42, 97–114. [Google Scholar] [CrossRef] [PubMed]
- Yüksel, I.; Başar, O.; Ataseven, H.; Ertuğrul, I.; Arhan, M.; Ibiş, M.; Dağli, U.; Demirel, B.T.; Ulker, A.; Seçilmiş, S.; et al. Mucocutaneous manifestations in inflammatory bowel disease. Inflamm. Bowel Dis. 2009, 15, 546–550. [Google Scholar] [CrossRef]
- Danese, S.; Semeraro, S.; Papa, A.; Roberto, I.; Scaldaferri, F.; Fedeli, G.; Gasbarrini, G.; Gasbarrini, A. Extraintestinal manifestations in inflammatory bowel disease. World J. Gastroenterol. 2005, 11, 7227–7236. [Google Scholar] [CrossRef]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. ECCO. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: Part 1: Diagnosis and medical management. J. Crohn’s Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stingeni, L.; Neve, D.; Bassotti, G.; Simonetti, S.; Bianchi, L.; Hansel, K. Cutaneous Crohn’s disease successfully treated with adalimumab. J. Eur. Acad. Dermatol. Venereol. 2016, 30, e72–e74. [Google Scholar] [CrossRef]
- Veloso, F.T.; Cardoso, V.; Fraga, J.; Carvalho, J.; Dias, L.M. Spontaneous umbilical fistula in Crohn’s disease. J. Clin. Gastroenterol. 1989, 11, 197–200. [Google Scholar] [CrossRef]
- Mountain, J.C. Cutaneous ulceration in Crohn’s disease. Gut 1970, 11, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Marzano, A.V.; Borghi, A.; Stadnicki, A.; Crosti, C.; Cugno, M. Cutaneous manifestations in patients with inflammatory bowel diseases: Pathophysiology, clinical features, and therapy. Inflamm. Bowel Dis. 2014, 20, 213–227. [Google Scholar] [CrossRef]
- Giudici, F.; Maggi, L.; Santi, R.; Cosmi, L.; Annunziato, F.; Nesi, G.; Barra, G.; Bassotti, G.; De Palma, R.; Tonelli, F. Perianal Crohn’s disease and hidradenitis suppurativa: A possible common immunological scenario. Clin. Mol. Allergy 2015, 13, 12. [Google Scholar] [CrossRef] [Green Version]
- Aberumand, B.; Howard, J.; Howard, J. Metastatic Crohn’s disease: An approach to an uncommon but important cutaneous disorder. BioMed Res. Int. 2017, 2017, 8192150. [Google Scholar] [CrossRef] [Green Version]
- Keyal, U.; Liu, Y.; Bhatta, A.K. Dermatologic manifestations of inflammatory bowel disease: A review. Discov. Med. 2018, 25, 225–233. [Google Scholar] [PubMed]
- Chatterjee, D.; Bhattacharjee, R.; Khullar, G.; Kumaran, S.; De, D.; Saikia, U.N.; Radotra, B.D. Metastatic Crohn disease: A clinicohistological appraisal from a tertiary care center in India. Am. J. Dermatopathol. 2020, 42, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Sbeit, W.; Kadah, A.; Mahamid, M.; Karayanni, H.; Mari, A.; Tali, S.; Srouji, S.; Khoury, T. Oral manifestations of inflammatory bowel disease: The neglected piece of the puzzle. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1422–1431. [Google Scholar] [CrossRef]
- Zunt, S.L. Recurrent aphthous stomatitis. Dermatol. Clin. 2003, 21, 33–39. [Google Scholar] [CrossRef]
- Lehman, J.S.; Rogers, R.S., 3rd. Acute oral ulcers. Clin. Dermatol. 2016, 34, 470–474. [Google Scholar] [CrossRef]
- Turkcapar, N.; Toruner, M.; Soykan, I.; Aydintug, O.T.; Cetinkaya, H.; Duzgun, N.; Ozden, A.; Duman, M. The prevalence of extraintestinal manifestations and HLA association in patients with inflammatory bowel disease. Rheumatol. Int. 2006, 26, 663–668. [Google Scholar] [CrossRef]
- Vavricka, S.R.; Gubler, M.; Gantenbein, C.; Spoerri, M.; Froehlich, F.; Seibold, F.; Protic, M.; Michetti, P.; Straumann, A.; Fournier, N.; et al. Swiss IBD Cohort Study Group. Anti-TNF Treatment for extraintestinal manifestations of inflammatory bowel disease in the Swiss IBD cohort study. Inflamm. Bowel Dis. 2017, 23, 1174–1181. [Google Scholar] [CrossRef]
- Lebwohl, M.; Lebwohl, O. Cutaneous manifestations of inflammatory bowel disease. Inflamm. Bowel Dis. 1998, 4, 142–148. [Google Scholar] [CrossRef]
- Timani, S.; Mutasim, D.F. Skin manifestations of inflammatory bowel disease. Clin. Dermatol. 2008, 26, 265–273. [Google Scholar] [CrossRef]
- Mir-Madjlessi, S.H.; Taylor, J.S.; Farmer, R.G. Clinical course and evolution of erythema nodosum and pyoderma gangrenosum in chronic ulcerative colitis: A study of 42 patients. Am. J. Gastroenterol. 1985, 80, 615–620. [Google Scholar]
- Greuter, T.; Vavricka, S.R. Extraintestinal manifestations in inflammatory bowel disease–Epidemiology, genetics, and pathogenesis. Expert Rev. Gastroenterol. Hepatol. 2019, 4, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, P.E.; Pardi, D.S. Extraintestinal manifestations of inflammatory bowel disease: Focus on the musculoskeletal, dermatologic, and ocular manifestations. Med. Gen. Med. 2007, 9, 55. [Google Scholar]
- Freeman, H.J. Erythema nodosum and pyoderma gangrenosum in 50 patients with Crohn’s disease. Can. J. Gastroenterol. 2005, 19, 603–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, D.; Rukkannagari, S.; Kethu, S. Pathogenesis and clinical approach to extraintestinal manifestations of inflammatory bowel disease. Minerva Gastroenterol. Dietol. 2007, 53, 233–248. [Google Scholar]
- Leung, A.K.C.; Leong, K.F.; Lam, J.M. Erythema nodosum. World J. Pediatr. 2018, 14, 548–554. [Google Scholar] [CrossRef]
- Wolf, N.; Quaranta, M.; Prescott, N.J.; Allen, M.; Smith, R.; Burden, A.D.; Worthington, J.; Griffiths, C.E.; Mathew, C.G.; Barker, J.N.; et al. Psoriasis is associated with pleiotropic susceptibility loci identified in type II diabetes and Crohn disease. J. Med. Genet. 2008, 45, 114–116. [Google Scholar] [CrossRef]
- Duerr, R.H.; Taylor, K.D.; Brant, S.R.; Rioux, J.D.; Silverberg, M.S.; Daly, M.J.; Steinhart, A.H.; Abraham, C.; Regueiro, M.; Griffiths, A.; et al. A genome-wide association study identifies IL23R as an inflammatory bowel disease gene. Science 2006, 1, 1461–1463. [Google Scholar] [CrossRef] [Green Version]
- Rahier, J.F.; Buche, S.; Peyrin-Biroulet, L.; Bouhnik, Y.; Duclos, B.; Louis, E.; Papay, P.; Allez, M.; Cosnes, J.; Cortot, A.; et al. Groupe d’Etude Thérapeutique des Affections Inflammatoires du Tube Digestif (GETAID). Severe skin lesions cause patients with inflammatory bowel disease to discontinue anti-tumor necrosis factor therapy. Clin. Gastroenterol. Hepatol. 2010, 8, 1048–1055. [Google Scholar] [CrossRef]
- Pietrzak, D.; Pietrzak, A.; Krasowska, D.; Borzęcki, A.; Franciszkiewicz-Pietrzak, K.; Polkowska-Pruszyńska, B.; Baranowska, M.; Reich, K. Digestive system in psoriasis: An update. Arch. Dermatol. Res. 2017, 309, 679–693. [Google Scholar] [CrossRef] [Green Version]
- Collamer, A.N.; Battafarano, D.F. Psoriatic skin lesions induced by tumor necrosis factor antagonist therapy: Clinical features and possible immunopathogenesis. Semin. Arthritis Rheum. 2010, 40, 233–240. [Google Scholar] [CrossRef]
- Ludwig, R.J.; Müller, S.; Marques Ad Recke, A.; Schmidt, E.; Zillikens, D.; Möller, S.; Ibrahim, S.M. Identification of quantitative trait loci in experimental epidermolysis bullosa acquisita. J. Investig. Dermatol. 2012, 132, 1409–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasperkiewicz, M.; Sadik, C.D.; Bieber, K.; Ibrahim, S.M.; Manz, R.A.; Schmidt, E.; Zillikens, D.; Ludwig, R.J. Epidermolysis Bullosa Acquisita: From pathophysiology to novel therapeutic options. J. Investig. Dermatol. 2016, 136, 24–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hundorfean, G.; Neurath, M.F.; Sitaru, C. Autoimmunity against type VII collagen in inflammatory bowel disease. J. Cell Mol. Med. 2010, 14, 2393–2403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plumptre, I.; Knabel, D.; Tomecki, K. Pyoderma gangrenosum: A review for the gastroenterologist. Inflamm. Bowel Dis. 2018, 24, 2510–2517. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Fanoni, D.; Antiga, E.; Quaglino, P.; Caproni, M.; Crosti, C.; Meroni, P.L.; Cugno, M. Expression of cytokines, chemokines and other effector molecules in two prototypic autoinflammatory skin diseases, pyoderma gangrenosum and Sweet’s syndrome. Clin. Exp. Immunol. 2014, 178, 48–56. [Google Scholar] [CrossRef]
- Antiga, E.; Maglie, R.; Volpi, W.; Bianchi, B.; Berti, E.; Marzano, A.V.; Caproni, M. T helper type 1-related molecules as well as interleukin-15 are hyperexpressed in the skin lesions of patients with pyoderma gangrenosum. Clin. Exp. Immunol. 2017, 189, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Marzano, A.V.; Lipsker, D.; Cugno, M. Editorial: Neutrophil-mediated skin diseases: Immunology and genetics. Front. Immunol. 2019, 10, 2377. [Google Scholar] [CrossRef]
- Maverakis, E.; Marzano, A.V.; Le, S.T.; Callen, J.P.; Brüggen, M.C.; Guenova, E.; Dissemond, J.; Shinkai, K.; Langan, S.M. Pyoderma gangrenosum. Nat. Rev. Dis. Primers 2020, 6, 81. [Google Scholar] [CrossRef]
- Wallach, D.; Vignon-Pennamen, M.D. From acute febrile neutrophilic dermatosis to neutrophilic disease: Forty years of clinical research. J. Am. Acad. Dermatol. 2006, 55, 1066–1071. [Google Scholar] [CrossRef]
- Marzano, A.V.; Borghi, A.; Wallach, D.; Cugno, M. A comprehensive review of neutrophilic diseases. Clin. Rev. Allergy Immunol. 2018, 54, 114–130. [Google Scholar] [CrossRef]
- Ahn, C.; Negus, D.; Huang, W. Pyoderma gangrenosum: A review of pathogenesis and treatment. Expert Rev. Clin. Immunol. 2018, 14, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Maverakis, E.; Ma, C.; Shinkai, K.; Fiorentino, D.; Callen, J.P.; Wollina, U.; Marzano, A.V.; Wallach, D.; Kim, K.; Schadt, C.; et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: A Delphi consensus of international experts. JAMA Dermatol. 2018, 154, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Weenig, R.H.; Davis, M.D.; Dahl, P.R.; Su, W.P. Skin ulcers misdiagnosed as pyoderma gangrenosum. N. Engl. J. Med. 2002, 347, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Garcovich, S.; De Simone, C.; Berti, E.; Marzano, A.V. Drug management of neutrophilic dermatoses. Expert Rev. Clin. Pharmacol. 2017, 10, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Becuwe, C.; Delaporte, E.; Colombel, J.F.; Piette, F.; Cortot, A.; Bergoend, H. Sweet’s syndrome associated with Crohn’s disease. Acta Derm. Venereol. 1989, 69, 444–445. [Google Scholar]
- Nischal, K.C.; Khopkar, U. An approach to the diagnosis of neutrophilic dermatoses: A histopathological perspective. Indian J. Dermatol. Venereol. Leprol. 2007, 73, 222–230. [Google Scholar] [CrossRef]
- Marzano, A.V.; Ishak, R.S.; Saibeni, S.; Crosti, C.; Meroni, P.L.; Cugno, M. Autoinflammatory skin disorders in inflammatory bowel diseases, pyoderma gangrenosum and Sweet’s syndrome: A comprehensive review and disease classification criteria. Clin. Rev. Allergy Immunol. 2013, 45, 202–210. [Google Scholar] [CrossRef]
- Cox, N.H.; Palmer, J.G. Bowel-associated dermatitis-arthritis syndrome associated with ileo-anal pouch anastomosis, and treatment with mycophenolate mofetil. Br. J. Dermatol. 2003, 149, 1296–1297. [Google Scholar] [CrossRef]
- Tromm, A.; May, D.; Almus, E.; Voigt, E.; Greving, I.; Schwegler, U.; Griga, T. Cutaneous manifestations in inflammatory bowel disease. Z. Gastroenterol. 2001, 39, 137–144. [Google Scholar] [CrossRef]
- Andre, M.; Aumaitre, O.; Marcheix, J.C.; Piette, J.C. Aseptic systemic abscesses preceding diagnosis of Crohn’s disease by three years. Dig. Dis. Sci. 1995, 40, 525–527. [Google Scholar] [CrossRef]
- Dodd, E.M.; Howard, J.R.; Dulaney, E.D.; Rosenthal, S.I.; Wanna, M.R.; Farah, R.S. Pyodermatitis-pyostomatitis vegetans associated with asymptomatic inflammatory bowel disease. Int. J. Dermatol. 2017, 562, 1457–1459. [Google Scholar] [CrossRef] [PubMed]
- Stingeni, L.; Tramontana, M.; Bassotti, G.; Bianchi, L.; Lisi, P. Pyodermatitis-pyostomatitis vegetans and antibullous pemphigoid antigen 180 autoantibodies: A casual association? Br. J. Dermatol. 2015, 172, 811–813. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.; Patro, S. Pyodermatitis-pyostomatitis Vegetans. Indian J. Dermatol. 2017, 62, 434–436. [Google Scholar] [CrossRef] [PubMed]
- Tharwat, S.; Eltoraby, E.E. Pyodermatitis-pyostomatitis vegetans associated with autoimmune hepatitis: Unreported co-existence. Gastroenterol. Hepatol. Bed Bench 2020, 13, 188–190. [Google Scholar] [PubMed]
- Cugno, M.; Borghi, A.; Marzano, A.V. PAPA, PASH and PAPASH Syndromes: Pathophysiology, presentation and treatment. Am. J. Clin. Dermatol. 2017, 18, 555–562. [Google Scholar] [CrossRef]
- Schäffler, H.; Blattmann, T.; Findeisen, A.; Meinel, F.G.; Meyer-Bahlburg, A.; Lamprecht, G.; Steinmüller-Magin, L.; Trauzeddel, R.; Emmert, S. PAPA syndrome with Crohn’s disease and primary sclerosing cholangitis/autoimmune hepatitis overlap syndrome. Hautarzt 2019, 70, 116–122. [Google Scholar] [CrossRef]
- Marzano, A.V.; Borghi, A.; Meroni, P.L.; Crosti, C.; Cugno, M. Immune-mediated inflammatory reactions and tumors as skin side effects of inflammatory bowel disease therapy. Autoimmunity 2014, 47, 146–153. [Google Scholar] [CrossRef]
- Garcovich, S.; De Simone, C.; Genovese, G.; Berti, E.; Cugno, M.; Marzano, A.V. Paradoxical skin reactions to biologics in patients with rheumatologic disorders. Front Pharmacol. 2019, 10, 282. [Google Scholar] [CrossRef]
- Nigam, G.B.; Bhandare, A.P.; Antoniou, G.A.; Limdi, J.K. Systematic review and meta-analysis of dermatological reactions in patients with inflammatory bowel disease treated with anti-tumour necrosis factor therapy. Eur. J. Gastroenterol. Hepatol. 2020, 2020. [Google Scholar] [CrossRef]
- Fiorino, G.; Danese, S.; Pariente, B.; Allez, M. Paradoxical immune-mediated inflammation in inflammatory bowel disease patients receiving anti-TNF-α agents. Autoimmun. Rev. 2014, 13, 15–19. [Google Scholar] [CrossRef]
- Lindhaus, C.; Tittelbach, J.; Elsner, P. Cutaneous side effects of TNF-alpha inhibitors. J. Dtsch. Dermatol. Ges. 2017, 15, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Mocci, G.; Marzo, M.; Papa, A.; Armuzzi, A.; Guidi, L. Dermatological adverse reactions during anti-TNF treatments: Focus on inflammatory bowel disease. J. Crohn’s Colitis 2013, 7, 769–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segaert, S.; Hermans, C. Clinical signs, pathophysiology and management of cutaneous side effects of anti-tumor necrosis factor agents. Am. J. Clin. Dermatol. 2017, 186, 771–787. [Google Scholar] [CrossRef] [PubMed]
- Cullen, G.; Kroshinsky, D.; Cheifetz, A.S.; Korzenik, J.R. Psoriasis associated with anti-tumour necrosis factor therapy in inflammatory bowel disease: A new series and a review of 120 cases from the literature. Aliment. Pharmacol. Ther. 2011, 34, 1318–1327. [Google Scholar] [CrossRef]
- Guerra, I.; Pérez-Jeldres, T.; Iborra, M.; Algaba, A.; Monfort, D.; Calvet, X.; Chaparro, M.; Mañosa, M.; Hinojosa, E.; Minguez, M.; et al. Spanish GETECCU group (ENEIDA project). Incidence, clinical characteristics, and management of psoriasis induced by anti-TNF therapy in patients with inflammatory bowel disease: A nationwide cohort study. Inflamm. Bowel Dis. 2016, 22, 894–901. [Google Scholar] [CrossRef]
- Weizman, A.V.; Sharma, R.; Afzal, N.M.; Xu, W.; Walsh, S.; Stempak, J.M.; Nguyen, G.C.; Croitoru, K.; Steinhart, A.H.; Silverberg, M.S. Stricturing and fistulizing Crohn’s disease is associated with anti-tumor necrosis factor-induced psoriasis in patients with inflammatory bowel disease. Dig. Dis. Sci. 2018, 63, 2430–2438. [Google Scholar] [CrossRef]
- Puig, L. Paradoxical reactions: Anti-tumor necrosis factor alpha agents, ustekinumab, secukinumab, ixekizumab, and others. Curr. Probl. Dermatol. 2018, 53, 49–63. [Google Scholar] [CrossRef]
- Tillack, C.; Ehmann, L.M.; Friedrich, M.; Laubender, R.P.; Papay, P.; Vogelsang, H.; Stallhofer, J.; Beigel, F.; Bedynek, A.; Wetzke, M.; et al. Anti-TNF antibody-induced psoriasiform skin lesions in patients with inflammatory bowel disease are characterised by interferon-γ-expressing Th1 cells and IL-17A/IL-22-expressing Th17 cells and respond to anti-IL-12/IL-23 antibody treatment. Gut 2014, 63, 567–577. [Google Scholar] [CrossRef] [Green Version]
- Afzali, A.; Wheat, C.L.; Hu, J.K.; Olerud, J.E.; Lee, S.D. The association of psoriasiform rash with anti-tumor necrosis factor (anti-TNF) therapy in inflammatory bowel disease: A single academic center case series. J. Crohn’s Colitis 2014, 8, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Hansel, K.; Bianchi, L.; Tramontana, M.; Balato, A.; Scala, E.; Brozzi, J.; Stingeni, L. Immediate local and systemic hypersensitivity due to etanercept and adalimumab. J. Allergy Clin. Immunol. Pract. 2019, 7, 726–727. [Google Scholar] [CrossRef]
- Wendling, D.; Streit, G.; Toussirot, E.; Prati, C. Herpes zoster in patients taking TNFalpha antagonists for chronic inflammatory joint disease. Joint Bone Spine 2008, 75, 540–543. [Google Scholar] [CrossRef] [PubMed]
- Strangfeld, A.; Listing, J.; Herzer, P.; Liebhaber, A.; Rockwitz, K.; Richter, C.; Zink, A. Risk of herpes zoster in patients with rheumatoid arthritis treated with anti-TNF-alpha agents. JAMA 2009, 301, 737–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahier, J.F.; Magro, F.; Abreu, C.; Armuzzi, A.; Ben-Horin, S.; Chowers, Y.; Cottone, M.; de Ridder, L.; Doherty, G.; Ehehalt, R.; et al. European Crohn’s and Colitis Organisation (ECCO). Second European evidence-based consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. J. Crohn’s Colitis 2014, 8, 443–468. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Manifestations | Diagnostic Approach | Specific Treatment | General Treatment in Relation to IBD Activity or IBD Treatment |
|---|---|---|---|
| Specific manifestations | |||
| Continuous/contiguous Crohn’s disease | Refer to dermatologist/biopsy | Surgical approach | Control inflammation |
| Metastatic Crohn’s disease | Refer to dermatologist/biopsy | Surgical approach | Control inflammation |
| Disorders associated with IBD | |||
| Aphthous stomatitis | Refer to dermatologist/stomatologist | Topical corticosteroids, colchicine | Control inflammation |
| Erythema nodosum | Refer to dermatologist/rule out other causes of erythema nodosum | Pain management (NSAIDs, colchicine), bed rest, systemic corticosteroids | Control inflammation |
| Psoriasis | Refer to dermatologist | Topical corticosteroids/vitamin D derivatives, systemic retinoids, methotrexate, cyclosporine, TNF inhibitors, IL-12/IL-23 inhibitor (ustekinumab), IL-17 inhibitors, IL-23 inhibitors, apremilast | Control inflammation |
| Epidermolysis bullosa acquisita | Refer to dermatologist/biopsy and perform direct and indirect immunofluorescence test and ELISA | Systemic steroids ± steroid-sparing immunomodulating agents (dapsone) or immunosuppressants (azathioprine, mycophenolate mofetil) | Control inflammation |
| Reactive manifestations | |||
| Pyoderma gangrenosum | Refer to dermatologist/biopsy | Systemic corticosteroids, dapsone, cyclosporine, TNF inhibitors, IL-12/IL-23 inhibitor (ustekinumab), IL-1 receptor antagonist (anakinra), anti-IL-1β monoclonal antibody (canakinumab) | Control inflammation |
| Sweet’s syndrome | Refer to dermatologist/biopsy | Systemic corticosteroids | Control inflammation |
| Bowel-associated dermatosis-arthritis syndrome | Refer to dermatologist/rheumatologist | Systemic antibiotics, systemic corticosteroids | Control inflammation |
| Aseptic abscess ulcers | Refer to dermatologist/biopsy | Systemic corticosteroids | Control inflammation |
| Pyodermatitis–pyostomatitis vegetans | Refer to dermatologist/biopsy | Systemic steroids ± steroid-sparing agents, colchicine, systemic steroids, bisphosphonates, methotrexate, sulfasalazine, TNF inhibitors, IL-1 receptor antagonist (anakinra) | Control inflammation |
| SAPHO syndrome | Refer to dermatologist/rheumatologist | Systemic steroids, IL-1 receptor antagonist (anakinra) | Control inflammation |
| PAPA syndrome | Refer to dermatologist/rheumatologist/biopsy | Control inflammation | |
| Mucocutaneous conditions secondary to treatment of IBD | |||
| Adverse mucocutaneous reactions (injection site reactions, infusion reactions, paradoxical reactions, eczematiform and psoriasiform reaction, life-threatening disorders) | Refer to dermatologist | Different treatments according to the adverse mucocutaneous reaction | Consider to withdraw/change IBD treatment |
| Cutaneous infections | Refer to dermatologist | Systemic/topical antibiotics | Consider to withdraw/change IBD treatment |
| Cutaneous malignancies | Refer to dermatologist/biopsy | Surgical excision/topical treatment | Consider to withdraw/change IBD treatment |
| Cutaneous manifestations secondary to nutritional malabsorption | |||
| Stomatitis | Refer to dermatologist | Start supplementation | Start supplementation |
| Glossitis | Refer to dermatologist | Start supplementation | Start supplementation |
| Angular cheilitis | Refer to dermatologist | Start supplementation | Start supplementation |
| Pellagra | Refer to dermatologist | Start supplementation | Start supplementation |
| Scurvy | Refer to dermatologist | Start supplementation | Start supplementation |
| Purpura | Refer to dermatologist | Start supplementation | Start supplementation |
| Acrodermatitis enteropathica | Refer to dermatologist | Start supplementation | Start supplementation |
| Phrynoderma | Refer to dermatologist | Start supplementation | Start supplementation |
| Seborrheic-type dermatitis | Refer to dermatologist | Start supplementation | Start supplementation |
| Hair and nail abnormalities | Refer to dermatologist | Start supplementation | Start supplementation |
| Adverse mucocutaneous reactions |
| Injection site reactions |
| Infusion reactions |
| “Paradoxical” reactions |
| Eczematous and psoriasis-like reactions |
| Life-threatening disorders (urticaria-angioedema, anaphylaxis, Stevens Johnson syndrome, and toxic epidermal necrolysis) |
| Cutaneous infections |
| Bacterial (erysipelas, cellulitis, and abscesses) |
| Viral (herpes, cytomegalovirus, papillomavirus, etc.) |
| Fungal |
| Opportunistic infections |
| Cutaneous malignancies |
| Non-melanoma skin cancers (basal cell carcinomas, squamous cells carcinomas) |
| Cutaneous lymphomas (mycosis fungoides, Sézary syndrome) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonelli, E.; Bassotti, G.; Tramontana, M.; Hansel, K.; Stingeni, L.; Ardizzone, S.; Genovese, G.; Marzano, A.V.; Maconi, G. Dermatological Manifestations in Inflammatory Bowel Diseases. J. Clin. Med. 2021, 10, 364. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020364
Antonelli E, Bassotti G, Tramontana M, Hansel K, Stingeni L, Ardizzone S, Genovese G, Marzano AV, Maconi G. Dermatological Manifestations in Inflammatory Bowel Diseases. Journal of Clinical Medicine. 2021; 10(2):364. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020364
Chicago/Turabian StyleAntonelli, Elisabetta, Gabrio Bassotti, Marta Tramontana, Katharina Hansel, Luca Stingeni, Sandro Ardizzone, Giovanni Genovese, Angelo Valerio Marzano, and Giovanni Maconi. 2021. "Dermatological Manifestations in Inflammatory Bowel Diseases" Journal of Clinical Medicine 10, no. 2: 364. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10020364