
Finite Mixture Models Based on Pain Intensity, Functional Disability and Psychological Distress Composite Assessment Allow Identification of Two Distinct Classes of Persistent Spinal Pain Syndrome after Surgery Patients Related to Their Quality of Life

 , ,
, ,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and PREDIBACK Study Description
2.2. Patient Selection
2.2.1. Inclusion Criteria
2.2.2. Non-Inclusion Criteria
2.3. Demographic Variables Encoding
2.4. Clinical Outcome Measurements
2.4.1. Health-Related Quality of Life
2.4.2. Pain Intensity
2.4.3. Functional Disability
2.4.4. Psychological Distress: Anxiety/Depression and Coping Strategies
2.5. Statistical Analysis
2.5.1. Measurements Internal Consistency
2.5.2. Correlation between EQ-5D, NPRS, ODI and HADS Depression Scores
2.5.3. Clustering of the Impact of Pain Intensity, Functional Disability and Depression on HRQoL
2.5.4. Baseline Characteristics Influencing Class Membership
3. Results
3.1. Study Population
3.2. Measurement Internal Consistency
3.3. Baseline Characteristics and Outcomes
3.4. Correlation between EQ-5D and ODI, NPRS and HADS Depression
3.5. Standard 1-Class Mixed Effects Model Results
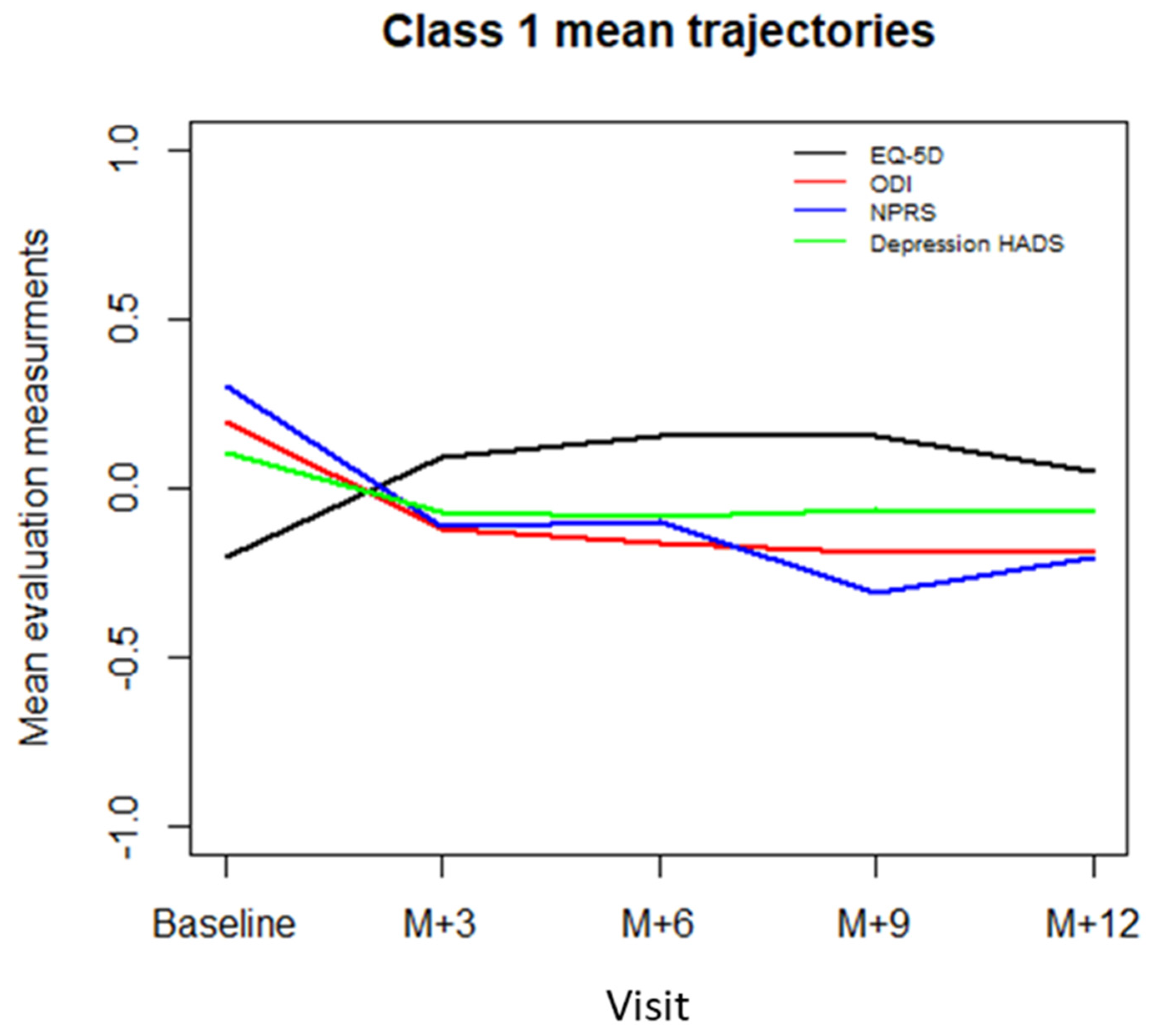
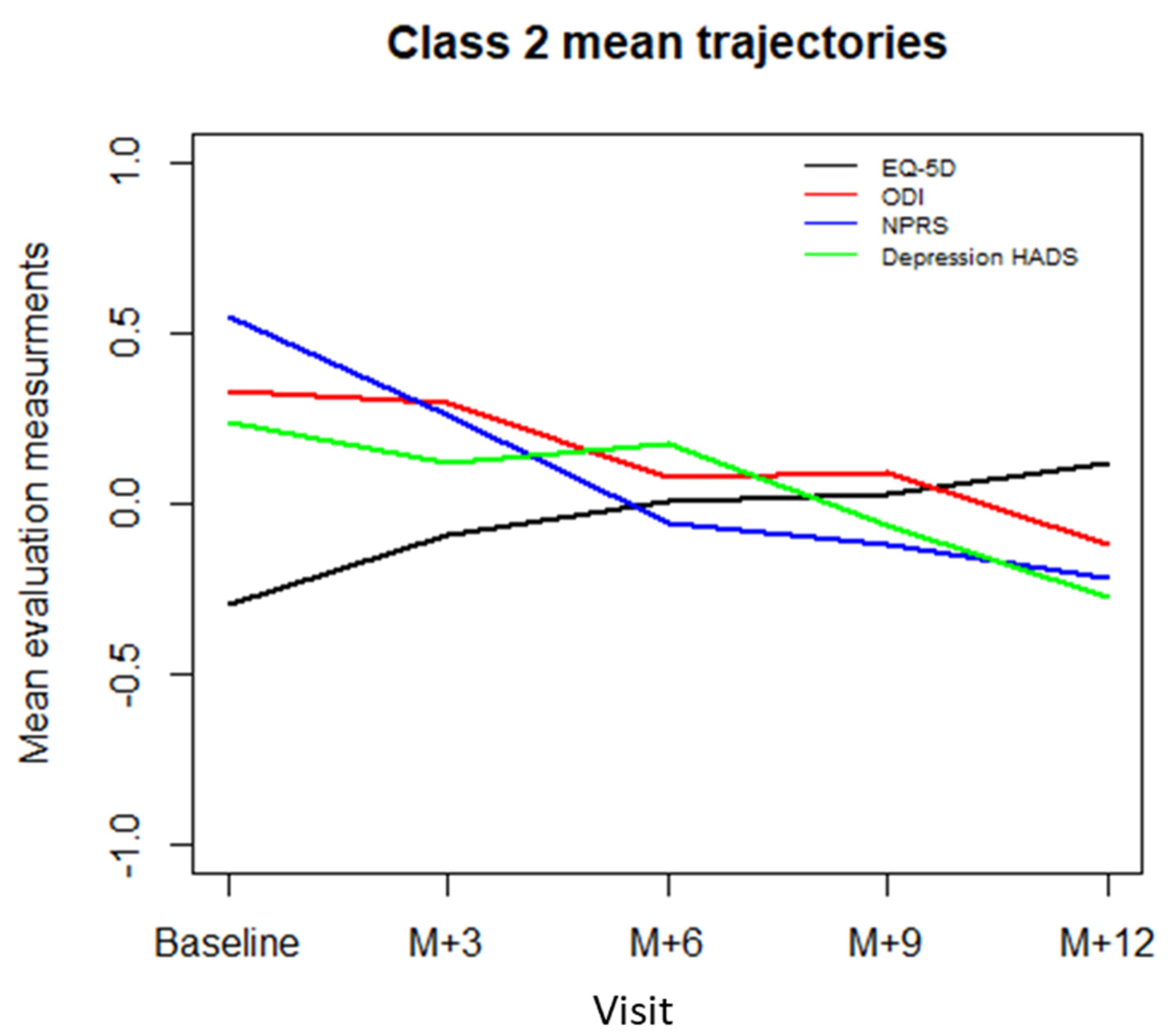
3.6. Two-Class Mixed Model Results
3.7. Relationship between Baseline Characteristics and Classes
3.8. The Relationship between Level of Education, Perceived Arduous Working Conditions and Coping Strategies
4. Discussion
4.1. A need for Multidimentional Composite Pain Assessment to Represent HRQoL Heterogeneity
4.2. Characterisation of HRQoL Classes
4.3. Study Strengths and Limitations
4.4. Therapeutical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Christelis, N.; Simpson, B.; Russo, M.; Stanton-Hicks, M.; Barolat, G.; Thomson, S.; Schug, S.; Baron, R.; Buchser, E.; Carr, D.B.; et al. Persistent Spinal Pain Syndrome: A Proposal for Failed Back Surgery Syndrome and ICD-11. Pain Med. 2021, 22, 807–818. [Google Scholar] [CrossRef]
- Rigoard, P.; Gatzinsky, K.; Deneuville, J.-P.; Duyvendak, W.; Naiditch, N.; Van Buyten, J.-P.; Eldabe, S. Optimizing the Management and Outcomes of Failed Back Surgery Syndrome: A Consensus Statement on Definition and Outlines for Patient Assessment. Pain Res. Manag. 2019, 2019, 3126464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalone, L.; Zucco, F.; Lavano, A.; Costantini, A.; Rose, M.D.; Poli, P.; Fortini, G.; Demartini, L.; Simone, E.D.; Menardo, V.; et al. Benefits in Pain Perception, Ability Function and Health-Related Quality of Life in Patients with Failed Back Surgery Syndrome Undergoing Spinal Cord Stimulation in a Clinical Practice Setting. Health Qual. Life Outcomes 2018, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Goudman, L.; Smedt, A.D.; Putman, K.; Moens, M. Long-Term Quality of Life and Work Status after High-Dose Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome: A Secondary Analysis of Real-World Data. J. Neurosurg. Spine 2020, 34, 440–448. [Google Scholar] [CrossRef]
- De Jaeger, M.; Goudman, L.; Putman, K.; De Smedt, A.; Rigoard, P.; Geens, W.; Moens, M. The Added Value of High Dose Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome after Conversion from Standard Spinal Cord Stimulation. J. Clin. Med. 2020, 9, 3126. [Google Scholar] [CrossRef]
- Castelli, L.; Tesio, V.; Colonna, F.; Molinaro, S.; Leombruni, P.; Bruzzone, M.; Fusaro, E.; Sarzi-Puttini, P.; Torta, R. Alexithymia and Psychological Distress in Fibromyalgia: Prevalence and Relation with Quality of Life. Clin. Exp. Rheumatol. 2012, 30, 70–77. [Google Scholar] [PubMed]
- Davies, M.; Brophy, S.; Williams, R.; Taylor, A. The Prevalence, Severity, and Impact of Painful Diabetic Peripheral Neuropathy in Type 2 Diabetes. Diabetes Care 2006, 29, 1518–1522. [Google Scholar] [CrossRef] [Green Version]
- Hasenbring, M.I.; Plaas, H.; Fischbein, B.; Willburger, R. The Relationship between Activity and Pain in Patients 6 Months after Lumbar Disc Surgery: Do Pain-Related Coping Modes Act as Moderator Variables? Eur. J. Pain 2006, 10, 701–709. [Google Scholar] [CrossRef]
- Langley, P.; Pérez Hernández, C.; Margarit Ferri, C.; Ruiz Hidalgo, D.; Lubián López, M. Pain, Health Related Quality of Life and Healthcare Resource Utilization in Spain. J. Med. Econ. 2011, 14, 628–638. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Abraira, V.; Zamora, J.; Teresa Gil del Real, M.; Llobera, J.; Fernández, C.; Bauza, J.R.; Bauza, K.; Coll, J.; Cuadri, M.; et al. Correlation between Pain, Disability, and Quality of Life in Patients with Common Low Back Pain. Spine 2004, 29, 206–210. [Google Scholar] [CrossRef]
- Rapti, E.; Damigos, D.; Apostolara, P.; Roka, V.; Tzavara, C.; Lionis, C. Patients with Chronic Pain: Evaluating Depression and Their Quality of Life in a Single Center Study in Greece. BMC Psychol. 2019, 7, 86. [Google Scholar] [CrossRef]
- Proust-Lima, C.; Philipps, V.; Liquet, B. Estimation of Extended Mixed Models Using Latent Classes and Latent Processes: The R Package Lcmm. J. Stat. Softw. 2017, 78, 1–56. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Campbell, P.; Strauss, V.Y.; Foster, N.E.; Jordan, K.P.; Dunn, K.M. Trajectories and Predictors of the Long-Term Course of Low Back Pain: Cohort Study with 5-Year Follow-Up. Pain 2018, 159, 252–260. [Google Scholar] [CrossRef]
- Dunn, K.M.; Jordan, K.; Croft, P.R. Characterizing the Course of Low Back Pain: A Latent Class Analysis. Am. J. Epidemiol. 2006, 163, 754–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and Preliminary Testing of the New Five-Level Version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obradovic, M.; Lal, A.; Liedgens, H. Validity and Responsiveness of EuroQol-5 Dimension (EQ-5D) versus Short Form-6 Dimension (SF-6D) Questionnaire in Chronic Pain. Health Qual. Life Outcomes 2013, 11, 110. [Google Scholar] [CrossRef] [Green Version]
- Tran, B.X.; Ohinmaa, A.; Nguyen, L.T. Quality of Life Profile and Psychometric Properties of the EQ-5D-5L in HIV/AIDS Patients. Health Qual. Life Outcomes 2012, 10, 132. [Google Scholar] [CrossRef] [Green Version]
- Vartiainen, P.; Mäntyselkä, P.; Heiskanen, T.; Hagelberg, N.; Mustola, S.; Forssell, H.; Kautiainen, H.; Kalso, E. Validation of EQ-5D and 15D in the Assessment of Health-Related Quality of Life in Chronic Pain. Pain 2017, 158, 1577–1585. [Google Scholar] [CrossRef]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of Four Pain Intensity Rating Scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Couper, J.; Davies, J.B.; O’Brien, J.P. The Oswestry Low Back Pain Disability Questionnaire. Physiotherapy 1980, 66, 271–273. [Google Scholar]
- Lee, C.-P.; Fu, T.-S.; Liu, C.-Y.; Hung, C.-I. Psychometric Evaluation of the Oswestry Disability Index in Patients with Chronic Low Back Pain: Factor and Mokken Analyses. Health Qual. Life Outcomes 2017, 15, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vianin, M. Psychometric Properties and Clinical Usefulness of the Oswestry Disability Index. J. Chiropr. Med. 2008, 7, 161–163. [Google Scholar] [CrossRef] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The Validity of the Hospital Anxiety and Depression Scale. An Updated Literature Review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Turk, D.C.; Dworkin, R.H.; Trudeau, J.J.; Benson, C.; Biondi, D.M.; Katz, N.P.; Kim, M. Validation of the Hospital Anxiety and Depression Scale in Patients with Acute Low Back Pain. J. Pain 2015, 16, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Sagheer, M.A.; Khan, M.F.; Sharif, S. Association between Chronic Low Back Pain, Anxiety and Depression in Patients at a Tertiary Care Centre. J. Pak. Med. Assoc. 2013, 63, 688–690. [Google Scholar] [PubMed]
- Irachabal, S.; Koleck, M.; Rascle, N.; Bruchon-Schweitzer, M. Pain coping strategies: French adaptation of the coping strategies questionnaire (CSQ-F). Encephale 2008, 34, 47–53. [Google Scholar] [CrossRef]
- Efron, B. Bootstrap Methods: Another Look at the Jackknife. Ann. Stat. 1979, 7, 1–26. [Google Scholar] [CrossRef]
- Proust, C.; Jacqmin-Gadda, H. Estimation of Linear Mixed Models with a Mixture of Distribution for the Random Effects. Comput. Methods Programs Biomed. 2005, 78, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, G. Estimating the Dimension of a Model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Ballantyne, J.C.; Sullivan, M.D. Intensity of Chronic Pain--The Wrong Metric? N. Engl. J. Med. 2015, 373, 2098–2099. [Google Scholar] [CrossRef]
- Sullivan, M.D.; Ballantyne, J.C. Must We Reduce Pain Intensity to Treat Chronic Pain? Pain 2016, 157, 65–69. [Google Scholar] [CrossRef]
- Dorfman, D.; George, M.C.; Robinson-Papp, J.; Rahman, T.; Tamler, R.; Simpson, D.M. Patient Reported Outcome Measures of Pain Intensity: Do They Tell Us What We Need to Know? Scand. J. Pain 2016, 11, 73–76. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The Biopsychosocial Approach to Chronic Pain: Scientific Advances and Future Directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef] [PubMed]
- Naiditch, N.; Billot, M.; Moens, M.; Goudman, L.; Cornet, P.; Le Breton, D.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; et al. Persistent Spinal Pain Syndrome Type 2 (PSPS-T2), a Social Pain? Advocacy for a Social Gradient of Health Approach to Chronic Pain. J. Clin. Med. 2021, 10, 2817. [Google Scholar] [CrossRef] [PubMed]
- Crombez, G.; Eccleston, C.; Van Damme, S.; Vlaeyen, J.W.S.; Karoly, P. Fear-Avoidance Model of Chronic Pain: The Next Generation. Clin. J. Pain 2012, 28, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Clinical Excellence Spinal Cord Stimulation for Chronic Pain of Neuropathic or Ischaemic Origin. Available online: https://www.nice.org.uk/guidance/ta159 (accessed on 21 July 2021).
- Rigoard, P.; Billot, M.; Ingrand, P.; Durand-Zaleski, I.; Roulaud, M.; Peruzzi, P.; Hieu, P.D.; Voirin, J.; Raoul, S.; Page, P.; et al. How Should we Use Multicolumn Spinal Cord Stimulation to Optimize Back Pain Spatial Neural Targeting? A Prospective, Multicenter, Randomized, Double-Blind, Controlled Trial ( ESTIMET Study). Neuromodulation Technol. Neural Interface 2021, 24, 86–101. [Google Scholar] [CrossRef]
- Centers for Medicare & Medicaid Services National Coverage Determination (NCD) for Electrical Nerve Stimulators. Available online: https://www.cms.gov/medicare-coverage-database/view/ncd.aspx?NCDId=240 (accessed on 21 July 2021).
- Jaeger, M.D.; Goudman, L.; Eldabe, S.; Dongen, R.V.; Smedt, A.D.; Moens, M. The Association between Pain Intensity and Disability in Patients with Failed Back Surgery Syndrome, Treated with Spinal Cord Stimulation. Disabil. Rehabil. 2021, 43, 2157–2163. [Google Scholar] [CrossRef]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Louis, P.-Y.; Yousri, S.; Roulaud, M.; Bouche, B.; Wood, C.; Page, P.; Lorgeoux, B.; et al. A Novel Multi-Dimensional Clinical Response Index Dedicated to Improve Pain Global Assessment in Patients with Persistent Spinal Pain Syndrome after Spinal Surgery, Based on a Real-Life Prospective Multicentric Study (PREDIBACK) and Machine Learning Techniques. Preprints 2021. [Google Scholar] [CrossRef]
- Goudman, L.; Moens, M. Moving Beyond a Pain Intensity Reporting: The Value of Goal Identification in Neuromodulation. Neuromodulation 2020, 23, 1057–1058. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Eldabe, S.; Rigoard, P.; Linderoth, B.; De Jaeger, M.; Moens, M.; Consortium, D. High-Dose Spinal Cord Stimulation for Patients with Failed Back Surgery Syndrome: A Multicenter Effectiveness and Prediction Study. Pain 2020, in press. [Google Scholar] [CrossRef]
- Kamper, S.J.; Apeldoorn, A.T.; Chiarotto, A.; Smeets, R.J.E.M.; Ostelo, R.W.J.G.; Guzman, J.; van Tulder, M.W. Multidisciplinary Biopsychosocial Rehabilitation for Chronic Low Back Pain. Cochrane Database Syst. Rev. 2014, CD000963. [Google Scholar] [CrossRef]
- Marris, D.; Theophanous, K.; Cabezon, P.; Dunlap, Z.; Donaldson, M. The Impact of Combining Pain Education Strategies with Physical Therapy Interventions for Patients with Chronic Pain: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Physiother. Theory Pract. 2021, 37, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, J.A.; Baliki, M.N.; Huang, L.; Baria, A.T.; Torbey, S.; Hermann, K.M.; Schnitzer, T.J.; Apkarian, A.V. Shape Shifting Pain: Chronification of Back Pain Shifts Brain Representation from Nociceptive to Emotional Circuits. Brain 2013, 136, 2751–2768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leclerc, A.; Gourmelen, J.; Chastang, J.-F.; Plouvier, S.; Niedhammer, I.; Lanoë, J.-L. Level of Education and Back Pain in France: The Role of Demographic, Lifestyle and Physical Work Factors. Int. Arch. Occup. Environ. Health 2009, 82, 643–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, R.S.; Geisser, M.E. Educational Achievement and Chronic Pain Disability: Mediating Role of Pain-Related Cognitions. Clin. J. Pain 2002, 18, 286–296. [Google Scholar] [CrossRef]
- Samulowitz, A.; Gremyr, I.; Eriksson, E.; Hensing, G. “Brave Men” and “Emotional Women”: A Theory-Guided Literature Review on Gender Bias in Health Care and Gendered Norms towards Patients with Chronic Pain. Pain Res. Manag. 2018, 2018, 6358624. [Google Scholar] [CrossRef]
- Naiditch, N.; Billot, M.; Goudman, L.; Cornet, P.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; Baron, S.; Nivole, K.; et al. Professional Status of Persistant Spinal Pain Syndrome Patients after Spinal Surgery (PSPS-T2): What Does Really Matter? A pro-Spective Study Introducing the Concept of “Adapted Profession-al Activity” Infering from Clinical, Psychological and Social influence. J. Clin. Med. 2021, Submitted. [Google Scholar]
- Higuchi, D. Adaptive and Maladaptive Coping Strategies in Older Adults with Chronic Pain after Lumbar Surgery. Int. J. Rehabil. Res. 2020, 43, 116–122. [Google Scholar] [CrossRef]
- Henry, S.G.; Bell, R.A.; Fenton, J.J.; Kravitz, R.L. Goals of Chronic Pain Management: Do Patients and Primary Care Physicians Agree and Does It Matter? Clin. J. Pain 2017, 33, 955–961. [Google Scholar] [CrossRef]
- Archer, K.R.; Devin, C.J.; Vanston, S.W.; Koyama, T.; Phillips, S.E.; Mathis, S.L.; George, S.Z.; McGirt, M.J.; Spengler, D.M.; Aaronson, O.S.; et al. Cognitive-Behavioral-Based Physical Therapy for Patients with Chronic Pain Undergoing Lumbar Spine Surgery: A Randomized Controlled Trial. J. Pain 2016, 17, 76–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnhoorn, K.J.; van de Meent, H.; van Dongen, R.T.M.; Klomp, F.P.; Groenewoud, H.; Samwel, H.; Nijhuis-van der Sanden, M.W.G.; Frölke, J.P.M.; Staal, J.B. Pain Exposure Physical Therapy (PEPT) Compared to Conventional Treatment in Complex Regional Pain Syndrome Type 1: A Randomised Controlled Trial. BMJ Open 2015, 5, e008283. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | n | % |
|---|---|---|
| Mean age (SD) | 53 (13) | |
| Gender | ||
| Male | 87 | 43.9 |
| Female | 111 | 56.1 |
| Professional status | ||
| In professional activity | 41 | 20.7 |
| Retired | 38 | 19.2 |
| Disability | 38 | 19.2 |
| Sick leave | 38 | 19.2 |
| Long-term illness | 16 | 8.1 |
| Unemployment | 7 | 3.5 |
| Without professional activity | 20 | 10.1 |
| Educational level | ||
| ≤12 years | 153/193 | 79.3 |
| >12 years | 40/193 | 20.7 |
| Number of spinal surgeries | ||
| 2 | 99 | 50.0 |
| 3 | 59 | 29.8 |
| 4 | 28 | 14.1 |
| 5 | 8 | 4.0 |
| 6+ | 4 | 2.0 |
| Neuropathic pain (DN4 * score ≥ 4) | ||
| Yes | 147/184 | 80 |
| No | 37/184 | 20 |
| Pain duration | ||
| ≤5 years | 46/198 | 23 |
| >5 years | 152/198 | 77 |
| Baseline | 12-Month Follow-Up | |||||
|---|---|---|---|---|---|---|
| Variables | ODI | NPRS | HADS Dep T | ODI | NPRS | HADS Dep T |
| EQ-5D | −0.66 *** | −0.35 *** | −0.44 *** | −0.77 *** | −0.55 *** | −0.56 *** |
| ODI | - | 0.44 *** | 0.40 *** | - | 0.54 *** | 0.57 *** |
| NPRS | - | - | 0.33 *** | - | - | 0.39 *** |
| Standard 1-Class Mixed Effects Model | Results of the Two-Class Mixture Model | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Class 1 Model | Class 2 Model | ||||||||
| Variables | Standardized Coefficient | Standard Error | p-Value | Standardized Coefficient | Standard Error | p-Value | Standardized Coefficient | Standard Error | p-Value |
| Intercept | −0.0029 | 0.037 | 0.93 | −0.0060 | 0.037 | 0.94 | - | - | - |
| ODI (%) | −0.48 | 0.034 | <0.0001 | −0.76 | 0.074 | <0.0001 | −0.11 | 0.095 | 0.23 |
| NPRS | −0.13 | 0.027 | <0.0001 | 0.039 | 0.041 | 0.46 | −0.35 | 0.065 | <0.0001 |
| HADS depression | −0.20 | 0.030 | <0.0001 | −0.19 | 0.044 | <0.0001 | −0.22 | 0.057 | 0.0001 |
| Variable | Mean (sd)/n(%) | Standardized Coefficients | 95% Confidence Interval | Adjusted p-Value | |
|---|---|---|---|---|---|
| Disability Class (n = 136) | Pain Intensity Class (n = 62) | ||||
| Intercept | - | - | −1.26 | [−1.79, −0.73] | <0.0001 |
| Age (years) | 52.01 (12.08) | 54.47 (13.41) | 0.28 | [−0.28, 0.84] | 0.31 |
| Gender (male) | 60/136 (44%) | 27/62 (44%) | −0.24 | [−0.73, 0.25] | 0.32 |
| Level of study (years) | 11.36 (3.14) | 9.47 (4.36) | −0.61 | [−1.15, −0.08] | 0.020 |
| Perceived physical job | |||||
| Working in a job perceived as physical | 17 (13%) | 9 (15%) | 0.08 | [−0.46, 0.63] | 0.77 |
| Working in a job not perceived as physical | 10 (7%) | 5 (8%) | 0.04 | [−0.48, 0.57] | 0.87 |
| Not in professional activity | 109 (80%) | 48 (77%) | − | - | |
| Global NPRS at baseline | 5.91 (1.41) | 6.47 (1.57) | 0.65 | [0.05, 1.24] | 0.029 |
| ODI percentage at baseline | 33.92 (10.83) | 34.98 (13.40) | −0.23 | [−0.86, 0.39] | 0.45 |
| HADS depression subscale | 8.44 (3.88) | 9.02 (3.83) | 0.88 | [0.17, 1.59] | 0.012 |
| HADS anxiety scale | 10.43 (3.79) | 9.03 (3.83) | −0.98 | [−1.70, −0.27] | 0.005 |
| CSQ catastrophizing scale | 14.17 (4.64) | 12.98 (4.18) | −0.60 | [−1.28, 0.07] | 0.07 |
| CSQ diversion | 12.68 (3.50) | 11.30 (3.72) | −0.44 | [−0.97, 0.08] | 0.09 |
| CSQ pain ignorance | 9.37 (3.23) | 9.27 (3.64) | −0.44 | [−0.96, 0.08] | 0.13 |
| CSQ pain reinterpretation | 6.03 (2.55) | 5.09 (1.71) | −0.51 | [−1.03, 0.02] | 0.12 |
| CSQ self-encouragement | 10.61 (2.78) | 10.08 (2.63) | 0.81 | [0.29, 1.34] | 0.011 |
| Pain duration (years) | 4.43 (5.92) | 4.64 (6.35) | −0.20 | [−0.73, 0.32] | 0.37 |
| Gender (male) x physical job * | |||||
| Male working in a physical job | 12/60 (20%) | 2/27 (7%) | −0.55 | [−1.08, −0.03] | 0.027 |
| Male working but not in a physical job | 3/60 (5%) | 2/27 (7%) | −0.17 | [−0.69, 0.36] | 0.53 |
| Male and not in professional activity | 45/60 (75%) | 23/27 (86%) | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ounajim, A.; Billot, M.; Louis, P.-Y.; Slaoui, Y.; Frasca, D.; Goudman, L.; Roulaud, M.; Naiditch, N.; Lorgeoux, B.; Baron, S.; et al. Finite Mixture Models Based on Pain Intensity, Functional Disability and Psychological Distress Composite Assessment Allow Identification of Two Distinct Classes of Persistent Spinal Pain Syndrome after Surgery Patients Related to Their Quality of Life. J. Clin. Med. 2021, 10, 4676. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204676
Ounajim A, Billot M, Louis P-Y, Slaoui Y, Frasca D, Goudman L, Roulaud M, Naiditch N, Lorgeoux B, Baron S, et al. Finite Mixture Models Based on Pain Intensity, Functional Disability and Psychological Distress Composite Assessment Allow Identification of Two Distinct Classes of Persistent Spinal Pain Syndrome after Surgery Patients Related to Their Quality of Life. Journal of Clinical Medicine. 2021; 10(20):4676. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204676
Chicago/Turabian StyleOunajim, Amine, Maxime Billot, Pierre-Yves Louis, Yousri Slaoui, Denis Frasca, Lisa Goudman, Manuel Roulaud, Nicolas Naiditch, Bertille Lorgeoux, Sandrine Baron, and et al. 2021. "Finite Mixture Models Based on Pain Intensity, Functional Disability and Psychological Distress Composite Assessment Allow Identification of Two Distinct Classes of Persistent Spinal Pain Syndrome after Surgery Patients Related to Their Quality of Life" Journal of Clinical Medicine 10, no. 20: 4676. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10204676