
The Impact of Using a Larger Forearm Artery for Percutaneous Coronary Interventions on Hand Strength: A Randomized Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
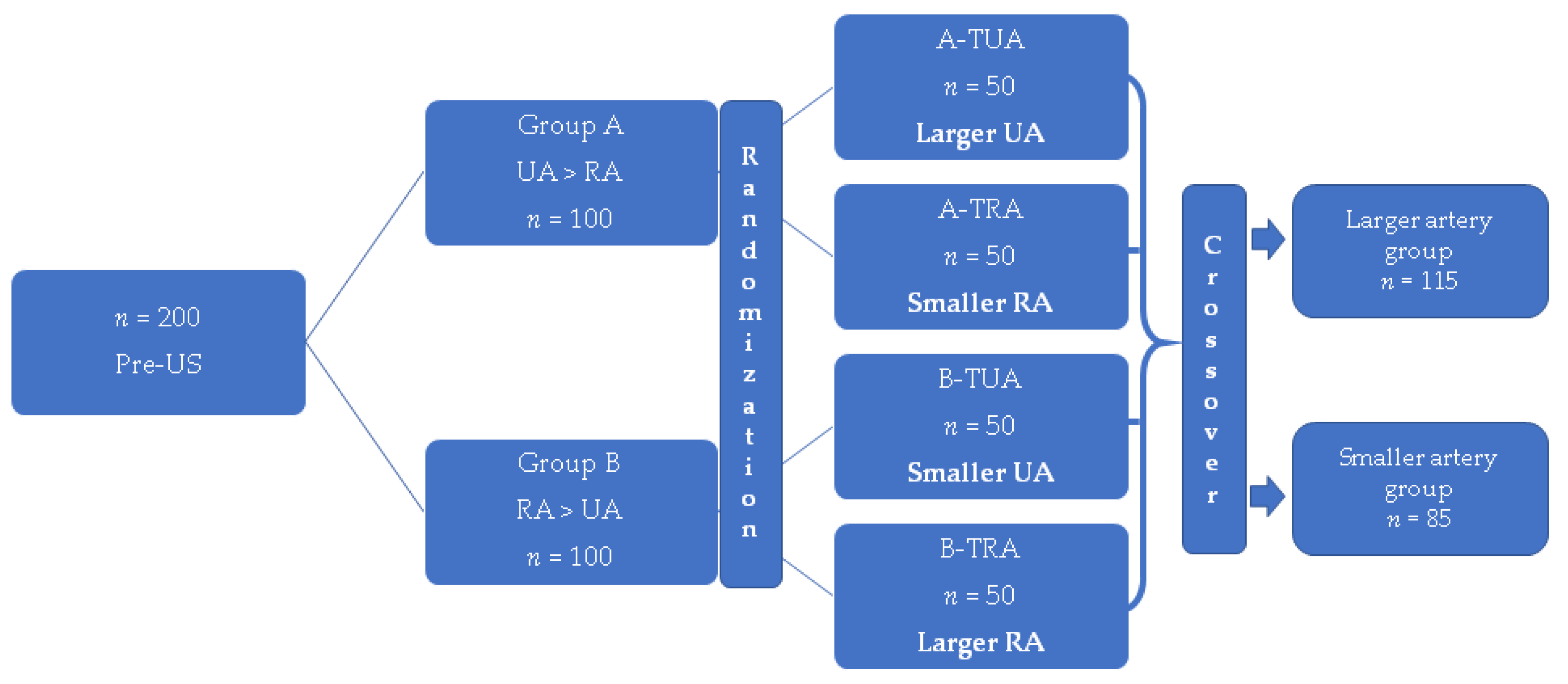
2.1. Study Design
2.1.1. Hand Grip Strength Measurements
2.1.2. Hand Strength Reduction Incidence
2.1.3. Additional Complications
2.2. Statistical Analysis
3. Results
3.1. Hand Strength Reduction
3.2. Additional Complications
3.3. Visual Analog Scale for Pain
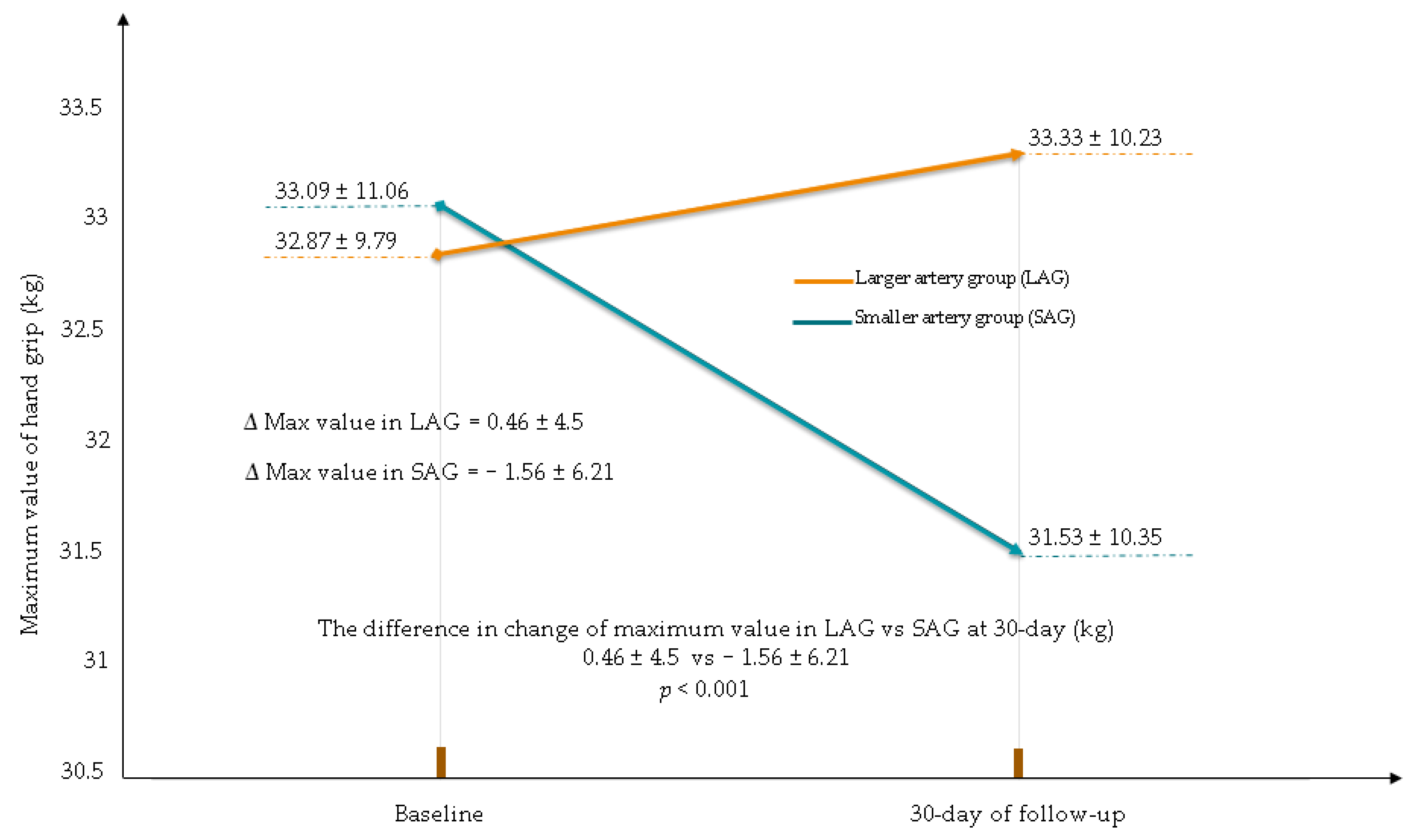
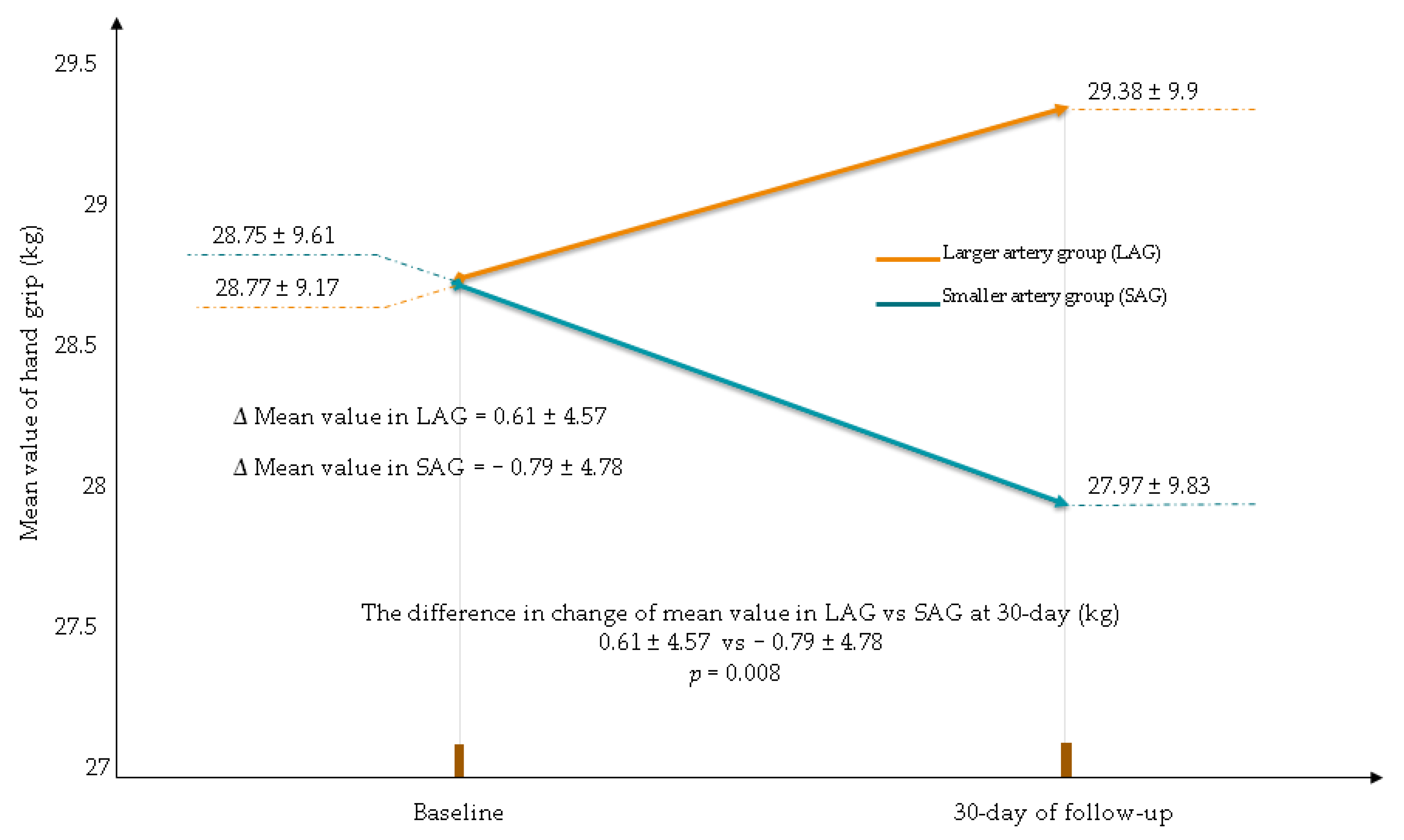
3.4. Changes in the Hand Grip Value
4. Discussion
4.1. Hand Strength Reduction
4.1.1. Potential Mechanisms of the Hand Disorder after CAG/PCI
4.1.2. Outcomes of Previous Studies
4.1.3. Pre-Procedural Selection of the Forearm Artery
4.2. Impact on Daily Practice
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agostoni, P.; Biondi-Zoccai, G.G.; de Benedictis, M.L.; Rigattieri, S.; Turri, M.; Anselmi, M.; Vassanelli, C.; Zardini, P.; Louvard, Y.; Hamon, M. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures; Systematic overview and meta-analysis of randomized trials. J. Am. Coll. Cardiol. 2004, 44, 349–356. [Google Scholar] [CrossRef] [Green Version]
- Jolly, S.S.; Yusuf, S.; Cairns, J.; Niemela, K.; Xavier, D.; Widimsky, P.; Budaj, A.; Niemela, M.; Valentin, V.; Lewis, B.S.; et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomized, parallel group, multicentre trial. Lancet 2011, 377, 1409–1420. [Google Scholar] [CrossRef]
- Pristipino, C.; Trani, C.; Nazzaro, M.; Berni, A.; Patti, G.; Patrizi, R.; Pironi, B.; Mazzarotto, P.; Gioffre, G.; Zoccai, G.B.; et al. Major improvement of percutaneous cardiovascular procedure outcomes with radial artery catheterisation: Results from the PREVAIL study. Heart 2008, 95, 476–482. [Google Scholar] [CrossRef]
- Li, Y.-Z.; Zhou, Y.-J.; Zhao, Y.-X.; Guo, Y.-H.; Liu, Y.-Y.; Shi, D.-M.; Wang, Z.-J.; Jia, D.-A.; Yang, S.-W.; Nie, B.; et al. Safety and efficacy of transulnar approach for coronary angiography and intervention. Chin. Med. J. 2010, 123, 1774–1779. [Google Scholar] [PubMed]
- De Andrade, P.B.; Tebet, M.A.; Nogueira, E.F.; Esteves, V.C.; de Andrade, M.V.; Labrunie, A.; Mattos, L.A. Transulnar approach as an alternative access site for coronary invasive procedures after transradial approach failure. Am. Heart J. 2012, 164, 462–467. [Google Scholar] [CrossRef]
- Aptecar, E.; Pernès, J.-M.; Chabane-Chaouch, M.; Bussy, N.; Catarino, G.; Shahmir, A.; Bougrini, K.; Dupouy, P. Transulnar versus transradial artery approach for coronary angioplasty: The PCVI-CUBA study. Catheter. Cardiovasc. Interv. 2006, 67, 711–720. [Google Scholar] [CrossRef]
- Hahalis, G.; Tsigkas, G.; Xanthopoulou, I.; Deftereos, S.; Ziakas, A.; Raisakis, K.; Pappas, C.; Sourgounis, A.; Grapsas, N.; Davlouros, P.; et al. Transulnar compared with transradial artery approach as a default strategy for coronary procedures: A randomized trial. The Transulnar or Transradial Instead of Coronary Transfemoral Angiographies Study (the AURA of ARTEMIS Study). Circ. Cardiovasc. Interv. 2013, 6, 252–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gokhroo, R.; Bisht, D.; Padmanabhan, D.; Gupta, S.; Kishor, K.; Ranwa, B. Feasibility of ulnar artery for cardiac catheterization: AJmer ULnar ARtery (AJULAR) catheterization study. Catheter. Cardiovasc. Interv. 2015, 86, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Geng, W.; Fu, X.; Gu, X.; Jiang, Y.; Fan, W.; Wang, Y.; Li, W.; Xing, K.; Liu, C. Safety and feasibility of transulnar versus transradial artery approach for coronary catheterization in non-selective patients. Chin. Med. J. 2014, 127, 1222–1228. [Google Scholar] [PubMed]
- Shah, B.; Bangalore, S.; Feit, F.; Fernandez, G.; Coppola, J.; Attubato, M.J.; Slater, J. Radiation exposure during coronary angiography via transradial or transfemoral approaches when performed by experienced operators. Am. Heart J. 2013, 165, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Rashid, M.; Sperrin, M.; Ludman, P.F.; O’Neill, D.; Nicholas, O.; De Belder, M.A.; Mamas, M.A. Impact of operator volume for percutaneous coronary intervention on clinical outcomes: What do the numbers say? Eur. Heart J. Qual. Care Clin. Outcomes 2016, 2, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, T.S.; Nolan, J.; Fountzopoulos, E.; Behan, M.; Butler, R.; Hetherington, S.L.; Vijayalakshmi, K.; Rajagopal, R.; Fraser, D.; Zaman, A.; et al. Radial artery anomaly and its influence on transradial coronary procedural outcome. Heart 2008, 95, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Kwok, C.S.; Rashid, M.; Fraser, D.; Nolan, J.; Mamas, M. Intra-arterial vasodilators to prevent radial artery spasm: A systematic review and pooled analysis of clinical studies. Cardiovasc. Revascularization Med. 2015, 16, 484–490. [Google Scholar] [CrossRef]
- Rashid, M.; Kwok, C.S.; Pancholy, S.; Chugh, S.; Kedev, S.A.; Bernat, I.; Ratib, K.; Large, A.; Fraser, D.; Nolan, J.; et al. Radial Artery Occlusion After Transradial Interventions: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e002686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Leeuwen, M.A.; van Mieghem, N.M.; Lenzen, M.J.; Selles, R.W.; Hoefkens, M.F.; Zijlstra, F.; van Royen, N. The effect of transradial coronary catheterization on upper limb function. JACC Cardiovasc. Interv. 2015, 8, 515–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Leeuwen, M.A.; van der Heijden, D.J.; Hermie, J.; Lenzen, M.J.; Selles, R.W.; Ritt, M.J.; Kiemeneij, F.; Zijlstra, F.; Van Mieghem, N.M.; van Royen, N. The long-term effect of transradial coronary catheterisation on upper limb function. EuroIntervention 2017, 12, 1766–1772. [Google Scholar] [CrossRef] [PubMed]
- Zwaan, E.; Koopman, A.; Holtzer, C.; Zijlstra, F.; Ritt, M.; Amoroso, G.; Moerman, E.; Kofflard, M.; Ijsselmuiden, A. Revealing the impact of local access-site complications and upper extremity dysfunction post transradial percutaneous coronary procedures. Neth. Heart J. 2015, 23, 514–524. [Google Scholar] [CrossRef] [Green Version]
- Ul Haq, M.A.; Rashid, M.; Kwok, C.S.; Wong, C.W.; Nolan, J.; Mamas, M.A. Hand dysfunction after transradial artery catheterization for coronary procedures. World J. Cardiol. 2017, 9, 609–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayyaz, U.l.; Haq, M.; Rashid, M.; Gilchrist, I.C.; Bertrand, O.; Kwok, C.S.; Wong, C.W.; Mansour, H.M.; Baghdaddy, Y.; Nolan, J.; et al. Incidence and Clinical Course of Limb Dysfunction Post Cardiac Catheterization: A systematic review. Circ. J. 2018, 82, 2736–2744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Sciahbasi, A.; Rigattieri, S.; Sarandrea, A.; Cera, M.; Di Russo, C.; Fedele, S.; Romano, S.; Penco, M.; Pugliese, F.R. Radial artery occlusion and hand strength after percutaneous coronary procedures: Results of the HANGAR study. Catheter. Cardiovasc. Interv. 2016, 87, 868–874. [Google Scholar] [CrossRef]
- Greenwood, M.J.; Della-Siega, A.J.; Fretz, E.B.; Kinloch, D.; Klinke, P.; Mildenberger, R.; Williams, M.B.; Hilton, D. Vascular communications of the hand in patients being considered for transradial coronary angiography: Is the Allen’s test accurate? J. Am. Coll. Cardiol. 2005, 46, 2013–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M.R. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF). Arthritis Rheum. 2011, 63, S240–S252. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, P.; Zuk, A.; Slomski, T.; Maciejewski, P.; Ramotowski, B.; Budaj, A. Impact of the Use of a Larger Forearm Artery on the Efficacy and Safety of Transradial and Transulnar Access: A Randomized Trial with Preprocedural Ultrasonography. J. Clin. Med. 2020, 9, 3607. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Rao, S.V.; Juni, P.; Da Costa, B.R.; Reimers, B.; Condorelli, G.; Anzuini, A.; Jolly, S.S.; Bertrand, O.F.; Krucoff, M.W.; et al. Radial Versus Femoral Access for Coronary Interventions Across the Entire Spectrum of Patients with Coronary Artery Disease: A Meta-Analysis of Randomized Trials. JACC Cardiovasc. Interv. 2016, 9, 1419–1434. [Google Scholar] [CrossRef] [PubMed]
- Campeau, L. Percutaneous radial artery approach for coronary angiography. Catheter. Cardiovasc. Diagn. 1989, 16, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Zankl, A.R.; Andrassy, M.; Volz, C.; Ivandic, B.; Krumsdorf, U.; Katus, H.A.; Blessing, E. Radial artery thrombosis following transradial coronary angiography: Incidence and rationale for treatment of symptomatic patients with low-molecular-weight heparins. Clin. Res. Cardiol. 2010, 99, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Tharmaratnam, D.; Webber, S.; Owens, P. Adverse local reactions to the use of hydrophilic sheaths for radial artery canulation. Int. J. Cardiol. 2010, 142, 296–298. [Google Scholar] [CrossRef] [PubMed]
- Kent, K.; Moscucci, M.; Gallagher, S.G.; DiMattia, S.T.; Skillman, J.J. Neuropathy after cardiac catheterization: Incidence, clinical patterns, and long-term outcome. J. Vasc. Surg. 1994, 19, 1008–1014. [Google Scholar] [CrossRef] [Green Version]
- Valgimigli, M.; Campo, G.; Penzo, C.; Tebaldi, M.; Biscaglia, S.; Ferrari, R. Transradial Coronary Catheterization and Intervention Across the Whole Spectrum of Allen Test Results. J. Am. Coll. Cardiol. 2014, 63, 1833–1841. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Larger UA/RA (n = 115) | Smaller UA/RA (n = 85) | p-Value | |
|---|---|---|---|
| Age, years (mean ± SD) | 68 ± 8 | 68.5 ± 7 | 0.45 |
| Male, n (%) | 64 (56) | 43 (51) | 0.5 |
| BMI, kg/m2 (mean ± SD) | 28.5 ± 4.6 | 28.5 ± 5.5 | 0.73 |
| BSA, m2 (mean ± SD) | 1.95 ± 0.25 | 1.94 ± 0.2 | 0.95 |
| Medical history | |||
| Smoking, n (%) | 28 (24) | 24 (28) | 0.53 |
| Hypertension, n (%) | 113 (98) | 82 (96) | 0.65 |
| Hypercholesterolemia, n (%) | 112 (97) | 79 (92) | 0.17 |
| Peripheral artery disease, n (%) | 23 (20) | 11 (13) | 0.19 |
| Diabetes, n (%) | 38 (33) | 24 (28) | 0.46 |
| Stroke, n (%) | 4 (3) | 4 (5) | 0.72 |
| Renal insufficiency, n (%) | 20 (17) | 10 (12) | 0.27 |
| Myocardial Infarction, n (%) | 22 (19) | 14 (16) | 0.62 |
| CABG, n (%) | 4 (3) | 3 (4) | 1.0 |
| Prior CAG or PCI, n (%) | 28 (29) | 21 (25) | 0.53 |
| Diagnosis upon admission | |||
| Suspected CAD, n (%) | 106 (92) | 78 (92) | 0.9 |
| CHF, n (%) | 3 (3) | 2 (2) | 1.0 |
| Ventricular arrythmia, n (%) | 6 (5) | 5 (6) | 0.83 |
| Pre-procedural medications | |||
| Aspirin, n (%) | 112 (97) | 84 (99) | 0.63 |
| Clopidogrel, n (%) | 110 (96) | 82 (96) | 1.0 |
| Warfarin, n (%) | 9 (8) | 4 (5) | 0.56 |
| NOAC, n (%) | 6 (5) | 6 (7) | 0.58 |
| Statin, n (%) | 107 (93) | 80 (94) | 0.76 |
| β-Blocker, n (%) | 107 (93) | 77 (91) | 0.52 |
| Angiography alone, n (%) | 68 (59) | 57 (67) | 0.25 |
| Angiography and FFR, n (%) | 5 (4) | 1 (1) | 0.19 |
| PCI ad hoc, n (%) | 31 (27) | 24 (28) | 0.84 |
| Elective PCI, n (%) | 11 (10) | 3 (4) | 0.98 |
| TRA, n (%) | 58 (50.4) | 43 (50.6) | 0.91 |
| TUA, n (%) | 57 (49.6) | 42 (50.4) | 0.98 |
| Right radial or ulnar access, n (%) | 101 (88) | 70 (82) | 0.27 |
| Left radial or ulnar access, n (%) | 14 (12) | 15 (18) | 0.27 |
| Fluoroscopy time (min) (mean ± SD) | 5.4 ± 5.2 | 4.9 ± 4.2 | 0.49 |
| Contrast medium (mL) (mean ± SD) | 149 ± 94 | 143 ± 41 | 0.63 |
| Radiation dose of X-ray (mSv) (mean ± SD) | 281 ± 281 | 246 ± 197 | 0.64 |
| Time of compression, (min) (mean ± SD) | 147 ± 31 | 149 ± 33 | 0.49 |
| Nitroglycerin (dose 200 ug) ia, n (%) | 115 (100) | 82 (96) | 1.0 |
| Dose of heparin (IU) (mean ± SD) | 6008 ± 1600 | 5900 ± 1544 | 0.6 |
| Arterial sheath size | |||
| 6-Fr, n (%) | 115 (100) | 85 (100) | 1.0 |
| Diagnostic catheter size | |||
| 6-Fr, n (%) | 105 (91) | 80 (94) | 0.45 |
| 5-Fr, n (%) | 2 (1.8) | 2 (2) | |
| Catheter used for PCI, n (%) | 47 (40) | 32 (37) | |
| 6-Fr, n (%) | 47 (100) | 32 (100) | 1.0 |
| Larger RA/UA (n = 115) | Smaller RA/UA (n = 85) | p-Value | |
|---|---|---|---|
| Strength reduction in used hand, n (%) † | 33 (29) | 40 (47) | 0.008 |
| Paresthesia of the upper limb, n (%) | 8 (7) | 15 (22) | 0.002 |
| Strength reduction—subjective change, n (%) | 12 (10) | 18 (21) | 0.03 |
| Any pain of the upper limb, n (%) | 14 (12) | 17 (20) | 0.1 |
| 24 h of Follow-Up | Larger RA/UA (n = 115) | Smaller RA/UA (n = 85) | p-Value |
|---|---|---|---|
| VAS at the procedure | |||
| (points 0–10) (mean ± SD) | 2.63 ± 1.6 | 3.08 ± 1.8 | <0.048 |
| VAS at 24 h after CAG/PCI | |||
| (points 0–10) (mean ± SD) | 1.9 ± 2 | 2.5 ± 2.5 | 0.08 |
| Larger RA/UA (n = 115) | Smaller RA/UA (n = 85) | p-Value | |
|---|---|---|---|
| Hand grip of used hand | |||
| Maximum value at the baseline (kg) (mean ± SD) | 32.87 ± 9.79 | 33.09 ± 11.06 | 0.87 |
| Maximum value at 30-day (kg) (mean ± SD) | 33.33 ± 10.23 | 31.53 ± 10.35 | 0.22 |
| The difference in change in maximum value at 30-day (kg) (mean ± SD) | 0.46 ± 4.5 | −1.56 ± 6.21 | 0.001 |
| Mean value at the baseline (kg) (mean ± SD) | 28.77 ± 9.17 | 28.75 ± 9.61 | 0.99 |
| Mean value at the 30-day (kg) (mean ± SD) | 29.38 ± 9.9 | 27.97 ± 9.83 | 0.31 |
| The difference in change in mean value at 30-day (kg) (mean ± SD) | 0.61 ± 4.57 | −0.79 ± 4.78 | 0.008 |
| Hand grip of unused hand | |||
| Maximum value at the baseline (kg) (mean ± SD) | 30.01 ± 10.01 | 29.82 ± 9.92 | 0.74 |
| Maximum value at 30-day (kg) (mean ± SD) | 30.31 ± 9.70 | 30.15 ± 10.22 | 0.9 |
| The difference in change in maximum value at 30-day (kg) (mean ± SD) | 0.3 ± 3.08 | 0.33 ± 1.95 | 0.87 |
| Mean value at the baseline (kg) (mean ± SD) | 26.38 ± 9.29 | 26.41 ± 9.19 | 0.98 |
| Mean value at the 30-day (kg) (mean ± SD) | 26.4 ± 9.18 | 26.73 ± 9.22 | 0.8 |
| The difference in change in mean value at 30-day (kg) (mean ± SD) | 0.01 ± 3.37 | 0.32 ± 1.94 | 0.59 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Larger RA/UA | 0.45 (0.24–0.82) | 0.01 |
| Use of TRA | 1.87 (1.01–3.4) | 0.045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewandowski, P.; Zuk, A.; Slomski, T.; Maciejewski, P.; Ramotowski, B.; Budaj, A. The Impact of Using a Larger Forearm Artery for Percutaneous Coronary Interventions on Hand Strength: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 1099. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051099
Lewandowski P, Zuk A, Slomski T, Maciejewski P, Ramotowski B, Budaj A. The Impact of Using a Larger Forearm Artery for Percutaneous Coronary Interventions on Hand Strength: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(5):1099. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051099
Chicago/Turabian StyleLewandowski, Pawel, Anna Zuk, Tomasz Slomski, Pawel Maciejewski, Bogumil Ramotowski, and Andrzej Budaj. 2021. "The Impact of Using a Larger Forearm Artery for Percutaneous Coronary Interventions on Hand Strength: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 5: 1099. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051099