
Accuracy, Labor-Time and Patient-Reported Outcomes with Partially versus Fully Digital Workflow for Flapless Guided Dental Implants Insertion—A Randomized Clinical Trial with One-Year Follow-Up

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Age over 18 years old, with good mental health and ability to fully understand and sign the consent form,
- Kennedy Class III partially edentulism with 4 or fewer missing teeth in a row,
- Good general health (healthy or with well-controlled chronical disease) with no contraindications for implant surgery,
- Acceptance of dental implant treatment and willing to comply with follow-up recalls,
- Acceptance of CBCT investigation.
- Parkinson’s disease (impossible to perform an accurate CBCT),
- Limited bone volume with stadial bone graft requirement,
- Limited mouth opening (impossible to use the surgical template),
- Untreated or uncontrolled periodontal disease,
- History of radiotherapy of the head and neck region,
- Poor oral hygiene and lack of compliance,
- Pregnancy or nursing.
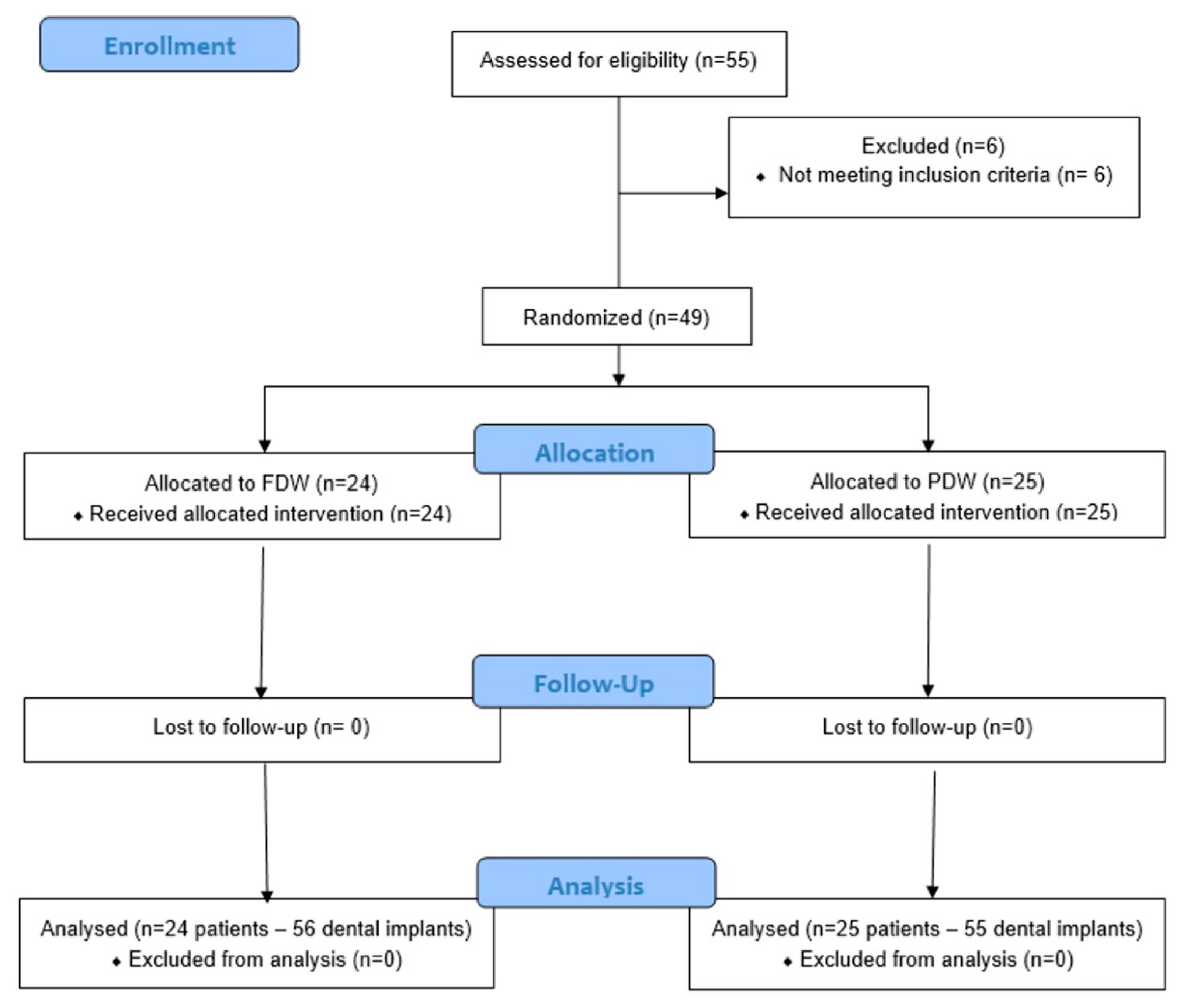
2.1. Sample Size Calculation and Randomisation
2.2. Data Collection
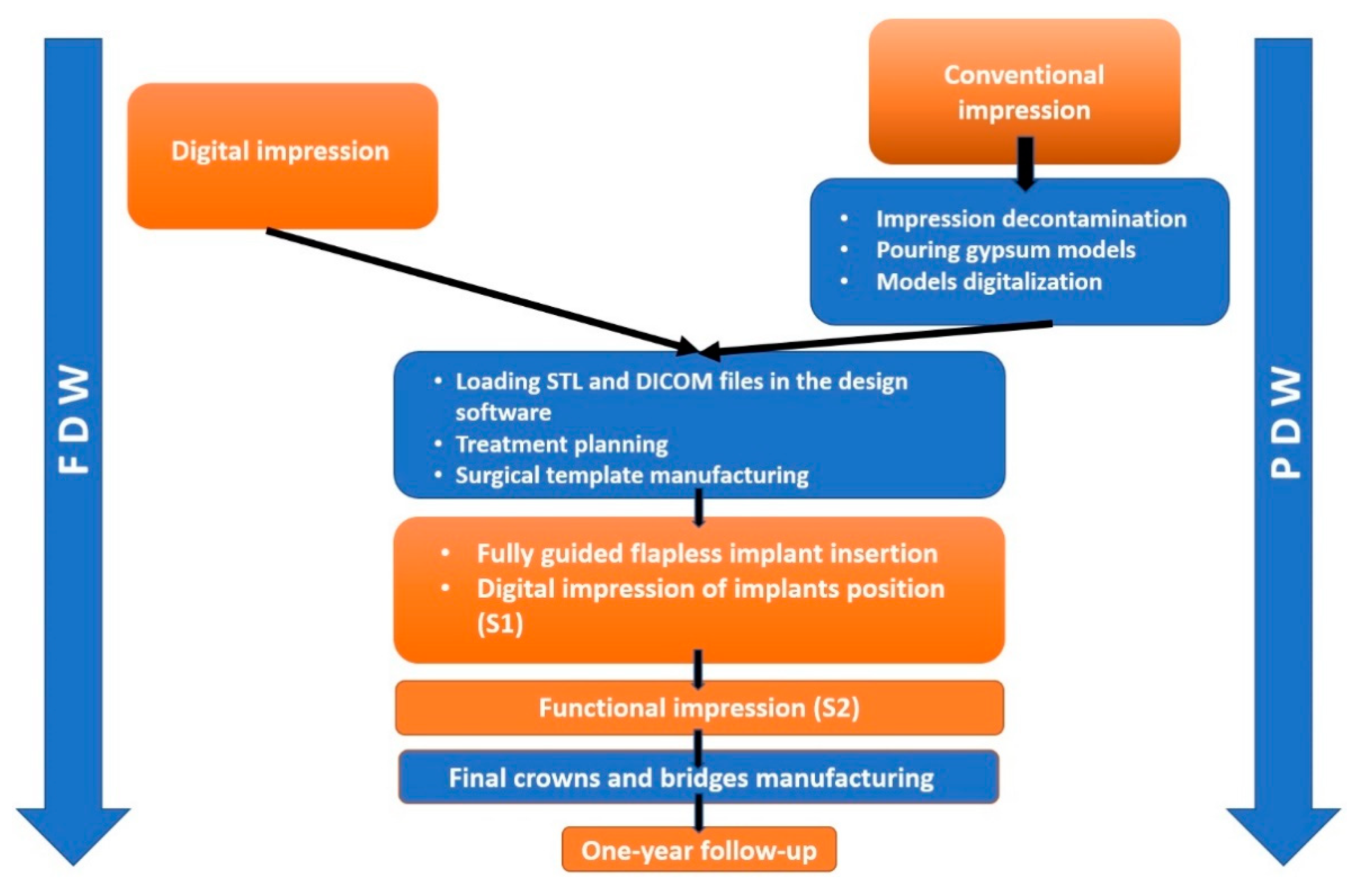
- -
- Digitally (FDW)—using Carestream 3600 (Carestream Dental LLC, Atlanta, GA, USA) intraoral surface scanner,
- -
- Conventionally (PDW)—with condensation-cured polymethyl siloxane impression material (Speedex, Coltene, Switzerland), in two consistencies (two phase): putty and light body with Universal Activator and Coltene Adhesive in a stock tray. In the dental laboratory, a Type IV (Elite rock, Zhermack SpA, Polesine, Italy) dental stone was used for pouring all the models. To obtain the STL files, the models were digitalized with a D 700 3D scanner (3Shape, Copenhagen, Denmark).
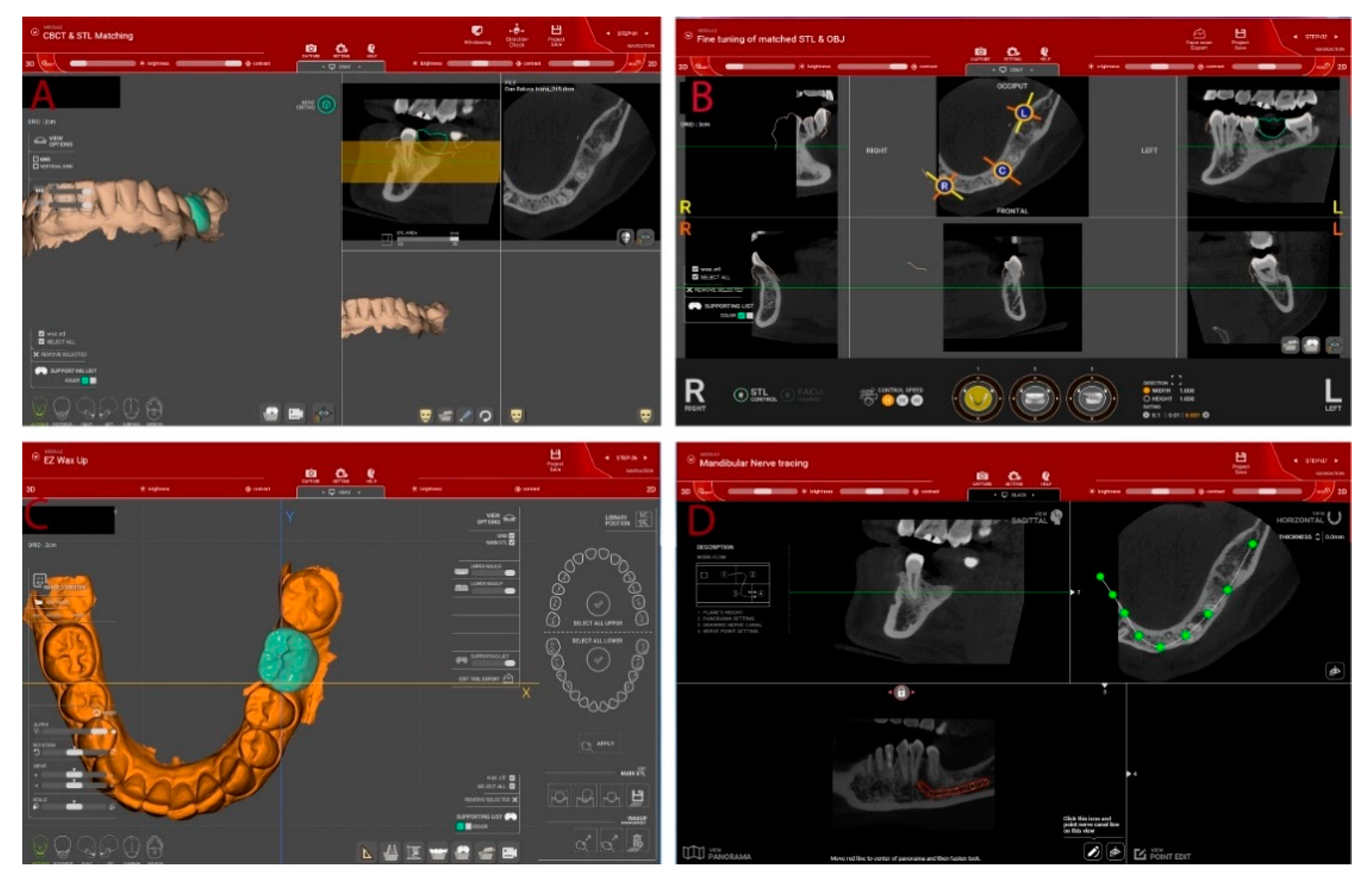
2.3. Design and Manufacturing of the Surgical Template
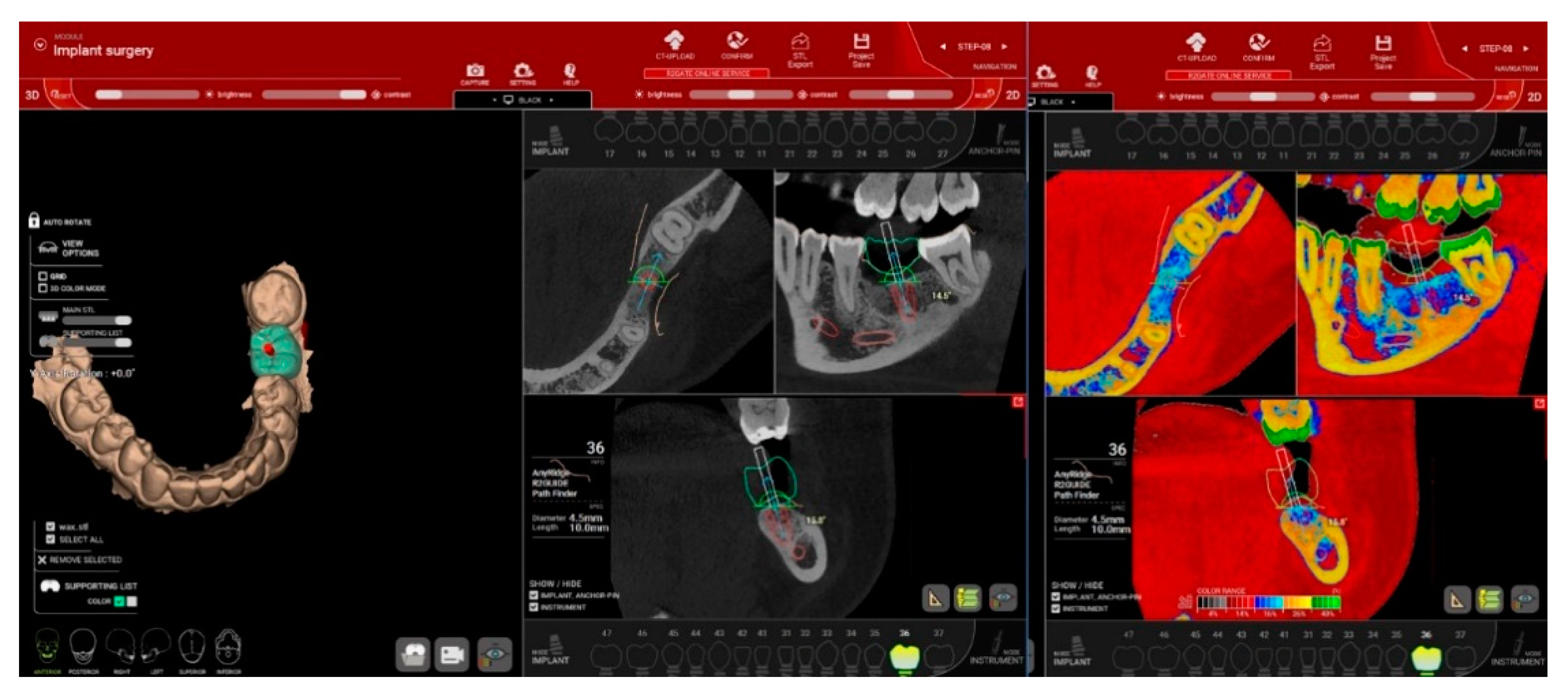
2.4. Dental Implants Surgery
2.5. Prosthetic Procedures
2.6. Outcome Measurements
2.6.1. One-Year Implants Survival and Complications
2.6.2. Accuracy of Implants Insertion
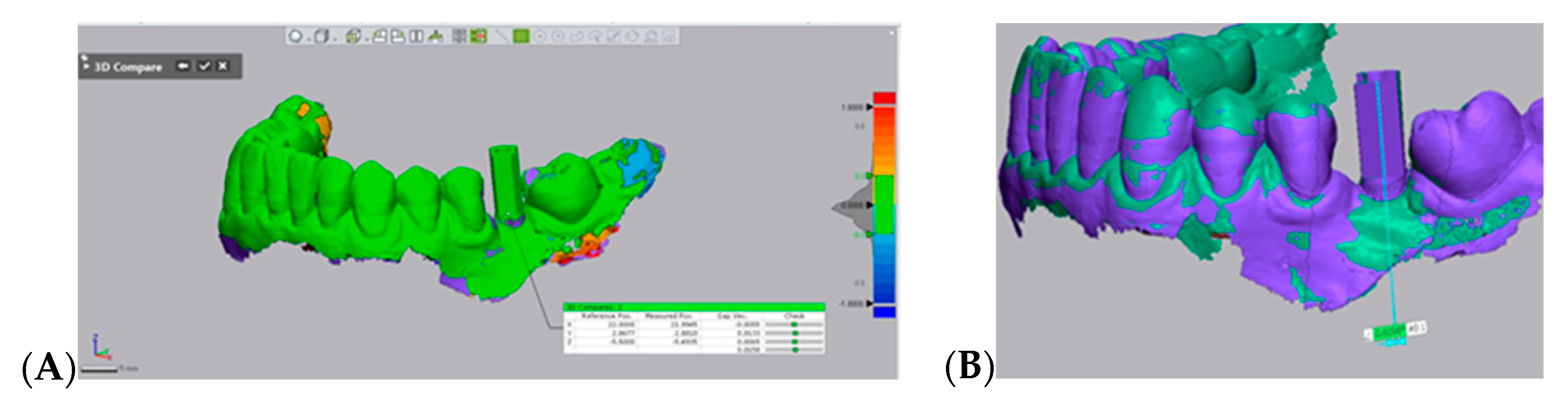
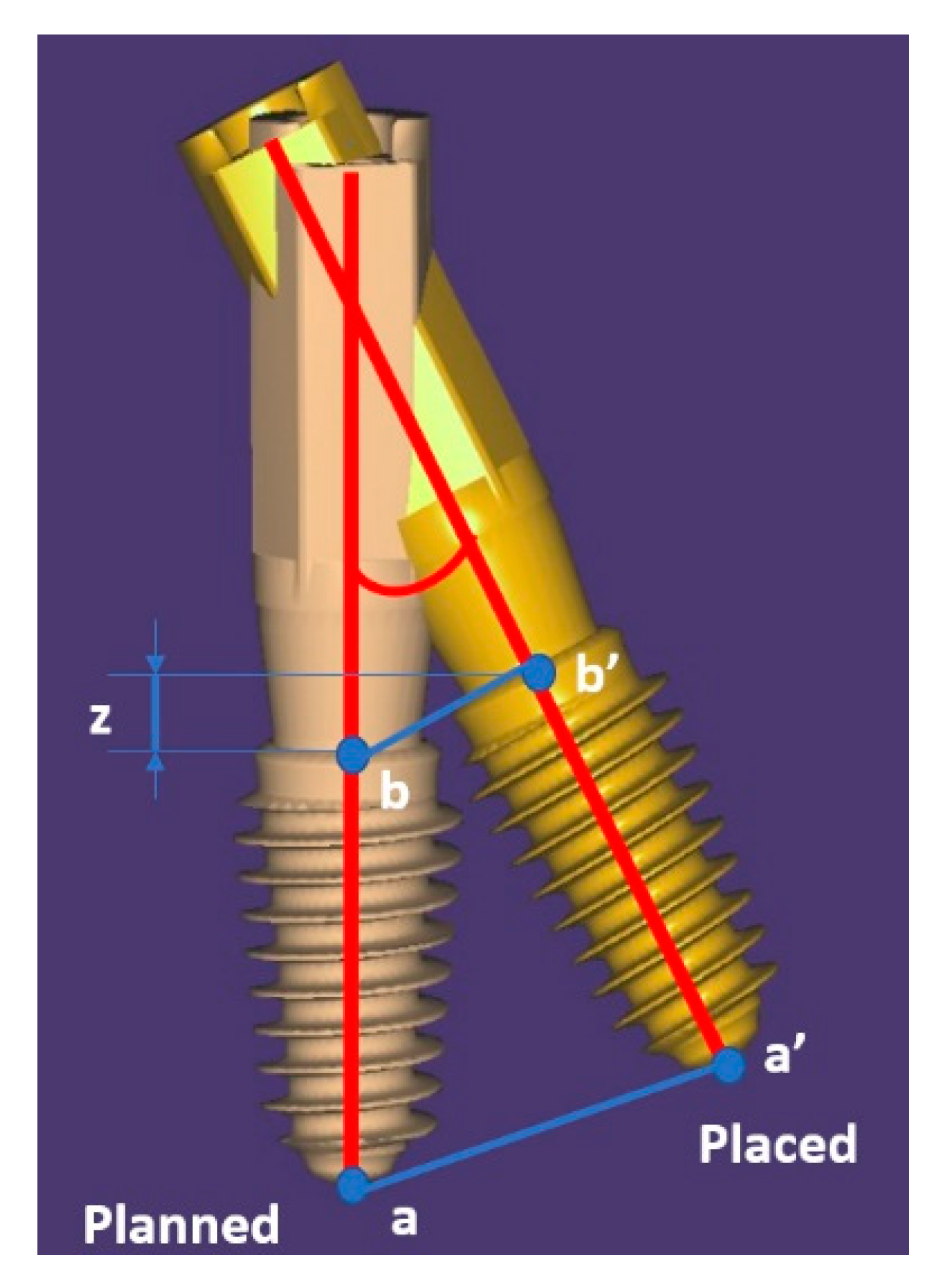
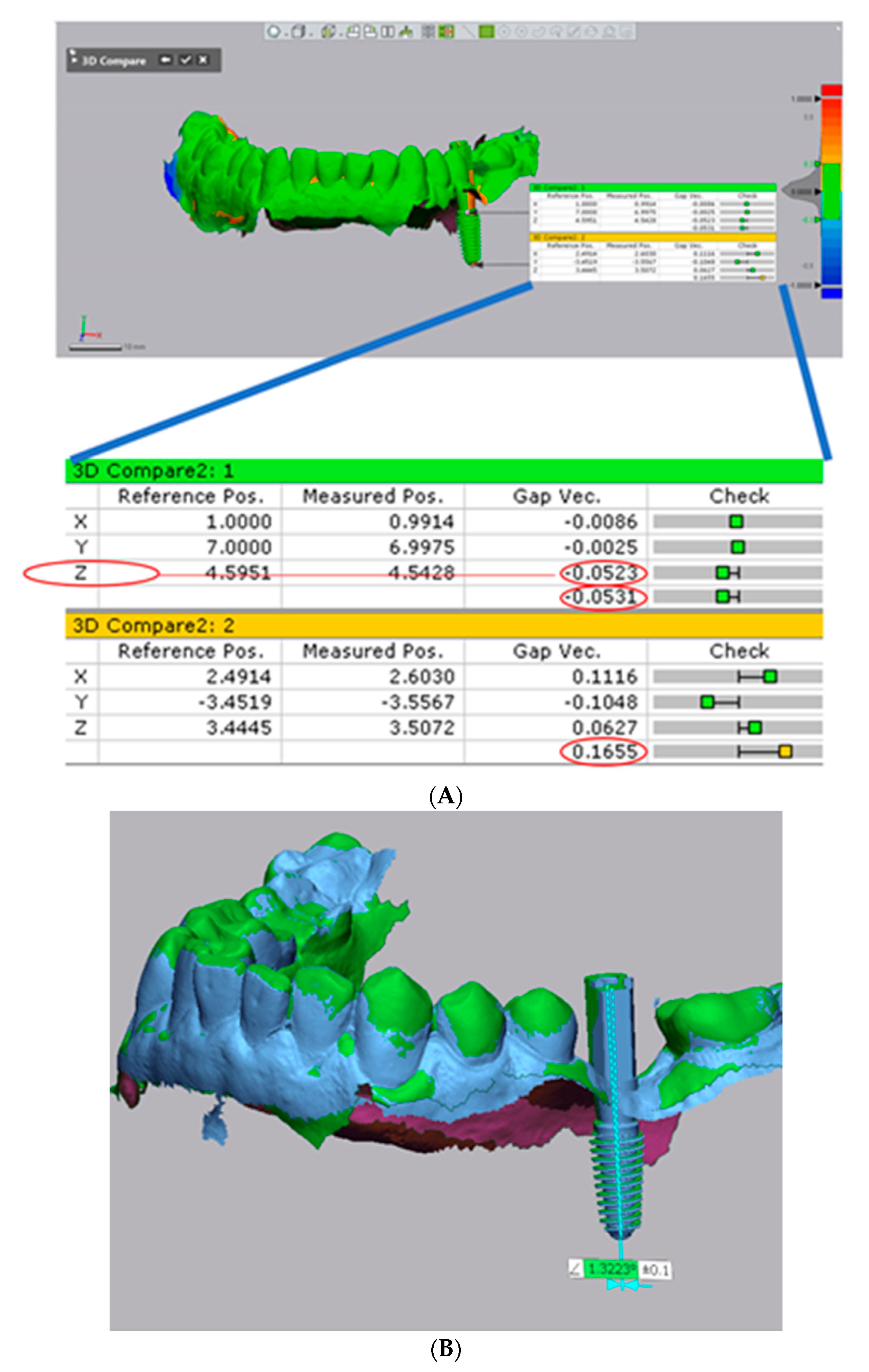
- For precision evaluation S1 and S2 for each implant were compared at the level of the marginal border of the scan abutment (Figure 5A). S2 was set as reference and the 3D coordinate axes were defined (x: bucco-lingual, y: mesio-distal, and z: apico-coronally), and S1 was aligned to the reference based on best fit of the neighboring remaining teeth. Angular deviation was also evaluated (Figure 5B).
- For trueness evaluation S1 for each implant was 3D compared with the STL file of treatment plan. Treatment plan was set as reference and S1 was aligned based on the best fit of the neighboring teeth using the best fit algorithm of the software. To facilitate an accurate evaluation, irrelevant areas, beyond the field of interest, were removed [4].
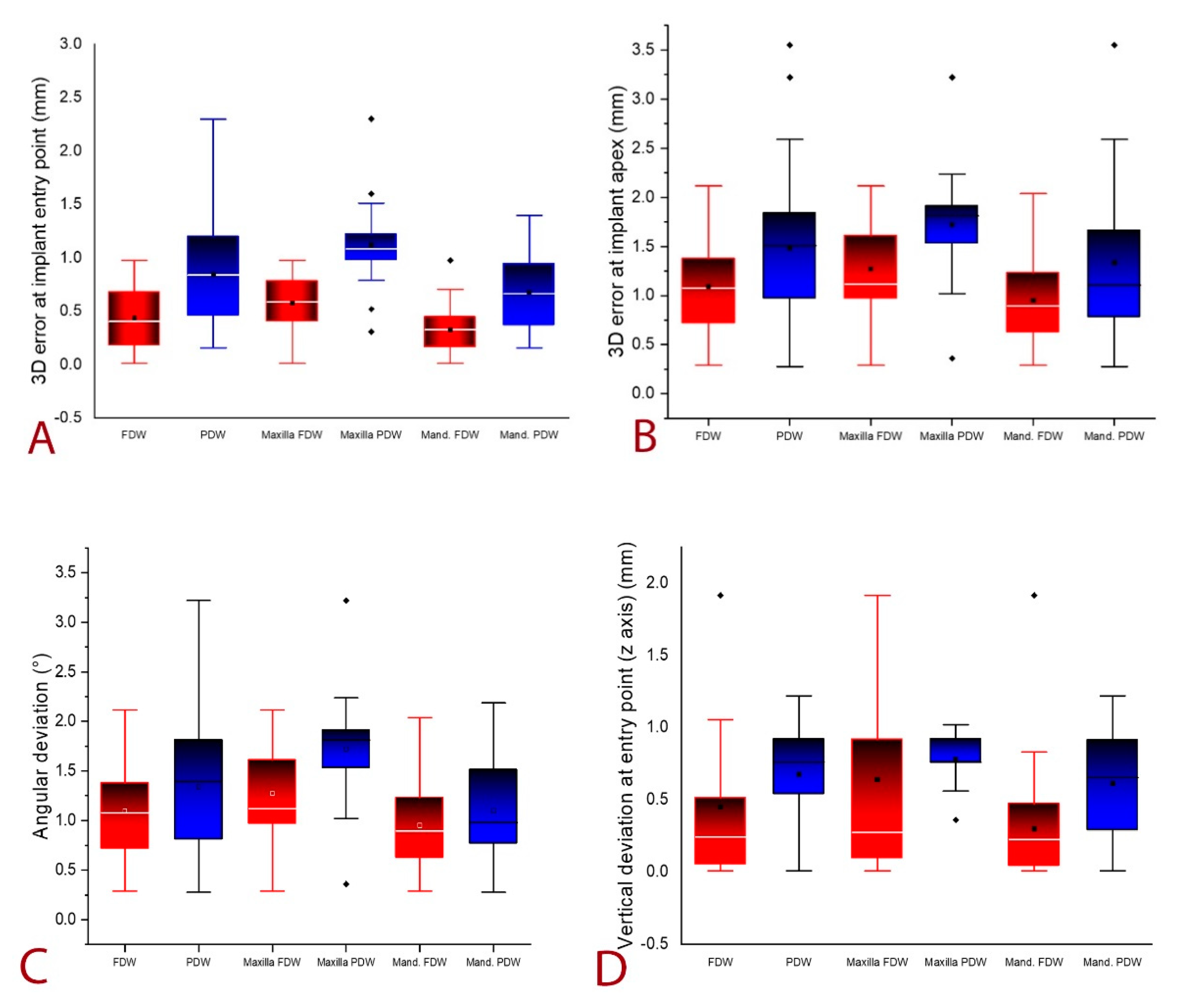
- 3D error at the entry point measured at the center of the implant (in mm),
- 3D error at the apex measured at the center of the implant apex (in mm),
- Angular deviation,
- Vertical deviation at entry point measured at the center of the implant (on z-axis).
2.6.3. Patients’ Feedback Regarding Dental Implant Insertion
2.6.4. Labor Time from Data Collection to Dental Implants Surgery for FDW and PDW
2.7. Statistical Analysis
3. Results
3.1. One Year Implant Survival and Complications
3.2. Accuracy of Implant Insertion
3.2.1. Assessment of Precision
3.2.2. Assessment of Trueness
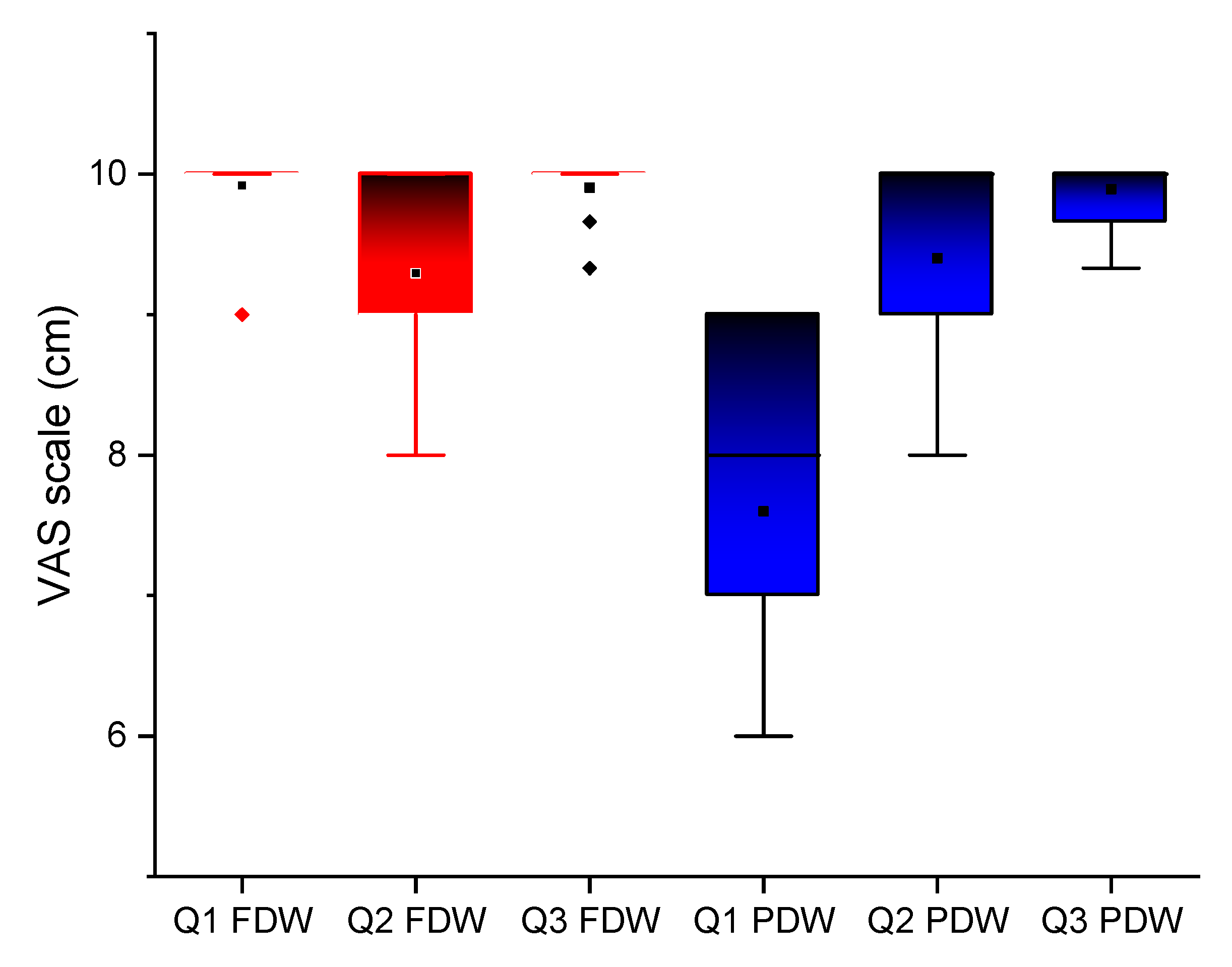
3.3. Patients’ Feedback Regarding Dental Implant Insertion
3.4. Labor Time from Data Collection to Dental Implants Surgery for FDW and PDW
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Siqueira, R.; Chen, Z.; Galli, M.; Saleh, I.; Wang, H.L.; Chan, H.L. Does a fully digital workflow improve the accuracy of computer-assisted implant surgery in partially edentulous patients? A systematic review of clinical trials. Clin. Implant. Dent. Relat. Res. 2020, 22, 660–671. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hammerle, C.H.; Tahmaseb, A. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2009, 24 (Suppl. S), 92–109. [Google Scholar]
- Pellegrino, G.; Bellini, P.; Cavallini, P.F.; Ferri, A.; Zacchino, A.; Taraschi, V.; Marchetti, C.; Consolo, U. Dynamic navigation in dental implantology: The influence of surgical experience on implant placement accuracy and operating time. An in vitro study. Int. J. Environ. Res. Public Health 2020, 17, 2153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristache, C.M.; Gurbanescu, S. Accuracy Evaluation of a Stereolithographic Surgical Template for Dental Implant Insertion Using 3D Superimposition Protocol. Int. J. Dent. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorba-García, A.; Figueiredo, R.; González-Barnadas, A.; Camps-Font, O.; Valmaseda-Castellón, E. Accuracy and the role of experience in dynamic computer guided dental implant surgery: An in-vitro study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e76. [Google Scholar] [CrossRef] [PubMed]
- Younes, F.; Eghbali, A.; De Bruyckere, T.; Cleymaet, R.; Cosyn, J. A randomized controlled trial on the efficiency of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients. Clin. Oral Implants Res. 2019, 30, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Meloni, S.M.; De Riu, G.; Lolli, F.M.; Pisano, M.; Deledda, A.; Frisardi, G.; Tullio, A. Computer-guided implant surgery: A critical review of treatment concepts. J. Oral Maxillofac. Surg. Med. Pathol. 2014, 26, 1–6. [Google Scholar] [CrossRef]
- Tallarico, M.; Xhanari, E.; Kim, Y.J.; Cocchi, F.; Martinolli, M.; Alushi, A.; Meloni, S.M. Accuracy of computer-assisted template-based implant placement using conventional impression and scan model or intraoral digital impression: A randomised controlled trial with 1 year of follow-up. Eur. J. Oral Implantol. 2019, 12, 197–206. [Google Scholar]
- Kiatkroekkrai, P.; Takolpuckdee, C.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. Accuracy of implant position when placed using static computer-assisted implant surgical guides manufactured with two different optical scanning techniques: A randomized clinical trial. Int. J. Oral Maxillofac. Surg. 2020, 49, 377–383. [Google Scholar] [CrossRef]
- Varga, E.; Antal, M.; Major, L.; Kiscsatári, R.; Braunitzer, G.; Piffkó, J. Guidance means accuracy: A randomized clinical trial on freehand versus guided dental implantation. Clin. Oral Implants Res. 2020, 31, 417–430. [Google Scholar] [CrossRef] [Green Version]
- Putra, R.H.; Yoda, N.; Astuti, E.R.; Sasaki, K. The accuracy of implant placement with computer-guided surgery in partially edentulous patients and possible influencing factors: A systematic review and meta-analysis. J. Prosthodont. Res. 2021, Online ahead of print. [CrossRef]
- Vercruyssen, M.; Laleman, I.; Jacobs, R.; Quirynen, M. Computer-supported implant planning and guided surgery: A narrative review. Clin. Oral Implant. Res. 2015, 26 (Suppl. S1), 69–76. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 10, 28–55. [Google Scholar]
- Tallarico, M.; Kim, Y.J.; Cocchi, F.; Martinolli, M.; Meloni, S.M. Accuracy of newly developed sleeve-designed templates for insertion of dental implants: A prospective multicenters clinical trial. Clin. Implant. Dent. Relat. Res. 2019, 21, 108–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristache, C.M. Presurgical Cone Beam Computed Tomography Bone Quality Evaluation for Predictable Immediate Implant Placement and Restoration in Esthetic Zone. Case Rep. Dent. 2017. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar]
- Ender, A.; Mehl, A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 2015, 46, 9–17. [Google Scholar] [CrossRef]
- ISO Standard 5725-2:2019. 2019. Available online: https://www.iso.org/obp/ui/#iso:std:iso:5725:-2:ed-2:v1:en (accessed on 4 January 2021).
- Ender, A.; Mehl, A. Accuracy of complete-Arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Bootvong, K.; Liu, Z.; McGrath, C.; Hägg, U.; Wong, R.W.K.; Bendeus, M.; Yeung, S. Virtual model analysis as an alternative approach to plaster model analysis: Reliability and validity. Eur. J. Orthod. 2010, 32, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29 (Suppl. S), 25–42. [Google Scholar] [CrossRef] [Green Version]
- Cristache, C.M.; Totu, E.E.; Iorgulescu, G.; Pantazi, A.; Dorobantu, D.; Nechifor, A.C.; Isildak, I.; Burlibasa, M.; Nechifor, G.; Enachescu, M. Eighteen Months Follow-Up with Patient-Centered Outcomes Assessment of Complete Dentures Manufactured Using a Hybrid Nanocomposite and Additive CAD/CAM Protocol. J. Clin. Med. 2020, 9, 324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- di Torresanto, V.M.; Milinkovic, I.; Torsello, F.; Cordaro, L. Computer-assisted flapless implant surgery in edentulous elderly patients: A 2-year follow up. Quintessence Int. 2014, 45, 419–429. [Google Scholar] [CrossRef]
- Vinhas, A.S.; Aroso, C.; Salazar, F.; López-Jarana, P.; Ríos-Santos, J.V.; Herrero-Climent, M. Review of the mechanical behavior of different implant–abutment connections. Int. J. Environ. Res. Public Health 2020, 17, 8685. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.M.; Nogueira-Filho, G.; Tenenbaum, H.C.; Lai, J.Y.; Brito, C.; Döring, H.; Nonhoff, J. Performance of conical abutment (Morse Taper) connection implants: A systematic review. J. Biomed. Mater. Res. Part. A 2014, 102, 552–574. [Google Scholar] [CrossRef]
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodontics Restor. Dent. 2006, 26, 9–17. [Google Scholar]
- Rocha, S.; Wagner, W.; Wiltfang, J.; Nicolau, P.; Moergel, M.; Messias, A.; Behrens, E.; Guerra, F. Effect of platform switching on crestal bone levels around implants in the posterior mandible: 3 years results from a multicentre randomized clinical trial. J. Clin. Periodontol. 2016, 43, 374–382. [Google Scholar] [CrossRef]
- Yadav, M.; Verma, U.; Parikh, H.; Dixit, M. Minimally invasive transgingival implant therapy: A literature review. Natl. J. Maxillofac. Surg. 2018, 9, 117. [Google Scholar] [PubMed]
- Bocklet, C.; Renne, W.; Mennito, A.; Bacro, T.; Latham, J.; Evans, Z.; Ludlow, M.; Kelly, A.; Nash, J. Effect of scan substrates on accuracy of 7 intraoral digital impression systems using human maxilla model. Orthod. Craniofac. Res. 2019, 22, 168–174. [Google Scholar] [CrossRef]
- Tang, T.; Liao, L.; Huang, Z.; Gu, X.; Zhang, X. Accuracy of the evaluation of implant position using a completely digital registration method compared with a radiographic method. J. Prosthet. Dent. 2019, 122, 537–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercruyssen, M.; Hultin, M.; Van Assche, N.; Svensson, K.; Naert, I.; Quirynen, M. Guided surgery: Accuracy and efficacy. Periodontology 2000 2014, 66, 228–246. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 416–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, W.; Liu, Z.; Song, L.; Kuo, C.L.; Shafer, D.M. Clinical Factors Affecting the Accuracy of Guided Implant Surgery—A Systematic Review and Meta-analysis. J. Evid. Based. Dent. Pract. 2018, 18, 28–40. [Google Scholar] [CrossRef]
- Lin, C.-C.; Wu, C.-Z.; Huang, M.-S.; Huang, C.-F.; Cheng, H.-C.; Wang, D.P. Fully Digital Workflow for Planning Static Guided Implant Surgery: A Prospective Accuracy Study. J. Clin. Med. 2020, 9, 980. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; An, S.Y.; Hong, M.H.; Jeon, K.B.; Lee, K.B. Accuracy of a direct drill-guiding system with minimal tolerance of surgical instruments used for implant surgery: A prospective clinical study. J. Adv. Prosthodont. 2016, 8, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Son, K.; Lee, K.B. A novel method for precise guided hole fabrication of dental implant surgical guide fabricated with 3d printing technology. Appl. Sci. 2021, 11, 49. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149 . [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | FDW | PDW |
|---|---|---|
| Number of patients | 24 | 25 |
| Mean age at implant insertion (SD) | 54.45 (±11.11) | 54.58 (±9.41) |
| Gender (F/M) | 14/10 | 18/7 |
| Number of restored sites | 33 | 33 |
| Number of implants 111 (maxilla/mandible) | 56 (25/31) | 55 (21/34) |
| Single/multiple gap | 12/21 | 14/19 |
| Implants length (mean, SD) min/max (mm) | 10.05 (±1.40) 7/13 | 9.80 (±1.29) 8.5/13 |
| Implants diameter (mean, SD) min/max (mm) | 3.91 (±0.43) 3.5/4.5 | 4.06 (±0.39) 3.5/4.5 |
| Bone Loss (mm) Mean [SD ± (95% CI)] | Loading | p Value | 1 Year Follow-Up | p Value | ||
|---|---|---|---|---|---|---|
| FDW | PDW | FDW | PDW | |||
| Maxilla | 0.04 [±0.15 (−0.02–0.10)] | 0.10 [±0.13 (−0.05–0.07)] | 0.13 | 0.05 [±0.12 (−0.00–0.10)] | 0.11 [±0.12 (0.05–0.17)] | 0.08 |
| Mandible | 0.07 [±0.11 (0.03–0.11)] | 0.04 [±0.12 (0.00–0.08)] | 0.22 | 0.03 [±0.13 (−0.01–0.08)] | 0.01 [±0.14 (−0.04–0.06)] | 0.59 |
| Overall | 0.06 [±0.13 (0.03–0.09)] | 0.07 [±0.13 (0.04–0.10)] | 0.93 | 0.04 [±0.12 (0.01–0.07)] | 0.05 [±0.14 (0.01–0.09)] | 0.55 |
| S1 vs. S2 | FDW Mean (SD) | PDW Mean (SD) | p Value |
|---|---|---|---|
| 3D errors at vestibular border (abutment) (mm) | 0.042 (±0.013) | 0.044 (±0.016) | 0.23 |
| Angular error (°) | 0.264 (±0.085) | 0.270 (±0.100) | 0.95 |
| FDW (mm) Mean [SD± (95% CI)] min/max | PDW (mm) Mean [SD± (95% CI)] min/max | p Value | |
|---|---|---|---|
| 3D error entry point (mm)—overall | 0.44 [±0.28 (0.36–0.51)] 0.01/0.98 | 0.85 [±0.43 (0.73–0.96)] 0.16/2.30 | p ≤ 0.00 |
| 3D error entry point (mm)—maxilla | 0.58 [±0.30 (0.46–0.70)] 0.01/0.98 | 1.12 [±0.40 (0.94–1.30)] 0.31/2.30 | p ≤ 0.00 |
| 3D error entry point (mm)—mandible | 0.33 [±0.22 (0.25–0.41)] 0.01/0.98 | 0.68 [±0.35 (0.55–0.80) 0.16/1.40 | p ≤ 0.00 |
| 3D error apex (mm)—overall | 1.03 [±0.48 (0.97–1.22)] 0.29/2.12 | 1.48 [±0.72 (1.29–1.68)] 0.28/3.55 | p ≤ 0.00 |
| 3D error apex (mm)—maxilla | 1.27 [±0.47 (1.08–1.47)] 0.29/2.12 | 1.72 [±0.53 (1.48–1.97)] 0.36/3.22 | p ≤ 0.00 |
| 3D error apex (mm)—mandible | 0.95 [±0.43 (0.79–1.10)] 0.29–2.04 | 1.33 [±0.78 (1.06–1.60)] 0.28/3.55 | 0.04 * |
| Angular deviation (°)—overall | 2.12 [±0.85 (1.90–2.35)] 0.39/3.86 | 2.48 [±0.75 (2.27–2.68)] 1.15/3.95 | 0.03 * |
| Angular deviation (°)—maxilla | 2.5 [±0.73 (2.20–2.80)] 0.39/3.50 | 2.92 [±0.57 (2.66–3.18)] 1.28/3.95 | 0.04 * |
| Angular deviation (°)—mandible | 1.82 [±0.83 (1.52–2.12)] 0.71/3.86 | 2.20 [±0.72 (1.95–2.45)] 1.15/3.91 | p ≤ 0.00 |
| Vertical deviation at entry point (z axis) (mm)—overall | 0.45 [±0.57 (0.30–0.60)] 0.01/1.92 | 0.68 [±0.28 (0.60–0.75)] 0.01/1.22 | p ≤ 0.00 |
| Vertical deviation at entry point (z axis) (mm)—maxilla | 0.64 [±0.70 (0.36–0.93)] 0.01/1.92 | 0.78 [±0.17 (0.80–0.86)] 0.36/1.02 | 0.01 * |
| Vertical deviation at entry point (z axis) (mm)—mandible | 0.30 [±0.38 (0.16–0.44)] 0.01/1.92 | 0.61 [±0.32 (0.50–0.72) 0.01/1.22 | p ≤ 0.00 |
| FDW (in min.) | PDW (in min.) | |
|---|---|---|
| Impression two arches and occlusion registration (clinic) | 8–12 5 (R2tray digitalization) | 9–12 |
| Data sent to the lab | 2 (data transfer) | 5 (cleaning & decontamination) 2 (packing) 60 (sending package) |
| Laboratory impression decontamination and check | - | 5 |
| Pouring gypsum models | - | 45 |
| Casts digitalization | - | 15 (arch model scanning) 5 (R2tray scanning) |
| Loading STL files in the design software | 2 | 2 |
| TOTAL | 17–21 | 148–151 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristache, C.M.; Burlibasa, M.; Tudor, I.; Totu, E.E.; Di Francesco, F.; Moraru, L. Accuracy, Labor-Time and Patient-Reported Outcomes with Partially versus Fully Digital Workflow for Flapless Guided Dental Implants Insertion—A Randomized Clinical Trial with One-Year Follow-Up. J. Clin. Med. 2021, 10, 1102. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051102
Cristache CM, Burlibasa M, Tudor I, Totu EE, Di Francesco F, Moraru L. Accuracy, Labor-Time and Patient-Reported Outcomes with Partially versus Fully Digital Workflow for Flapless Guided Dental Implants Insertion—A Randomized Clinical Trial with One-Year Follow-Up. Journal of Clinical Medicine. 2021; 10(5):1102. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051102
Chicago/Turabian StyleCristache, Corina Marilena, Mihai Burlibasa, Ioana Tudor, Eugenia Eftimie Totu, Fabrizio Di Francesco, and Liliana Moraru. 2021. "Accuracy, Labor-Time and Patient-Reported Outcomes with Partially versus Fully Digital Workflow for Flapless Guided Dental Implants Insertion—A Randomized Clinical Trial with One-Year Follow-Up" Journal of Clinical Medicine 10, no. 5: 1102. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10051102