
Contemporary Fertility-Sparing Management Options of Early Stage Endometrioid Endometrial Cancer in Young Nulliparous Patients

 ,
, 
 ,
, 
Abstract
:1. Endometrial cancer
1.1. Introduction
1.2. Diagnostic Tools and Molecular Markers for Detection of Endometrial Cancer
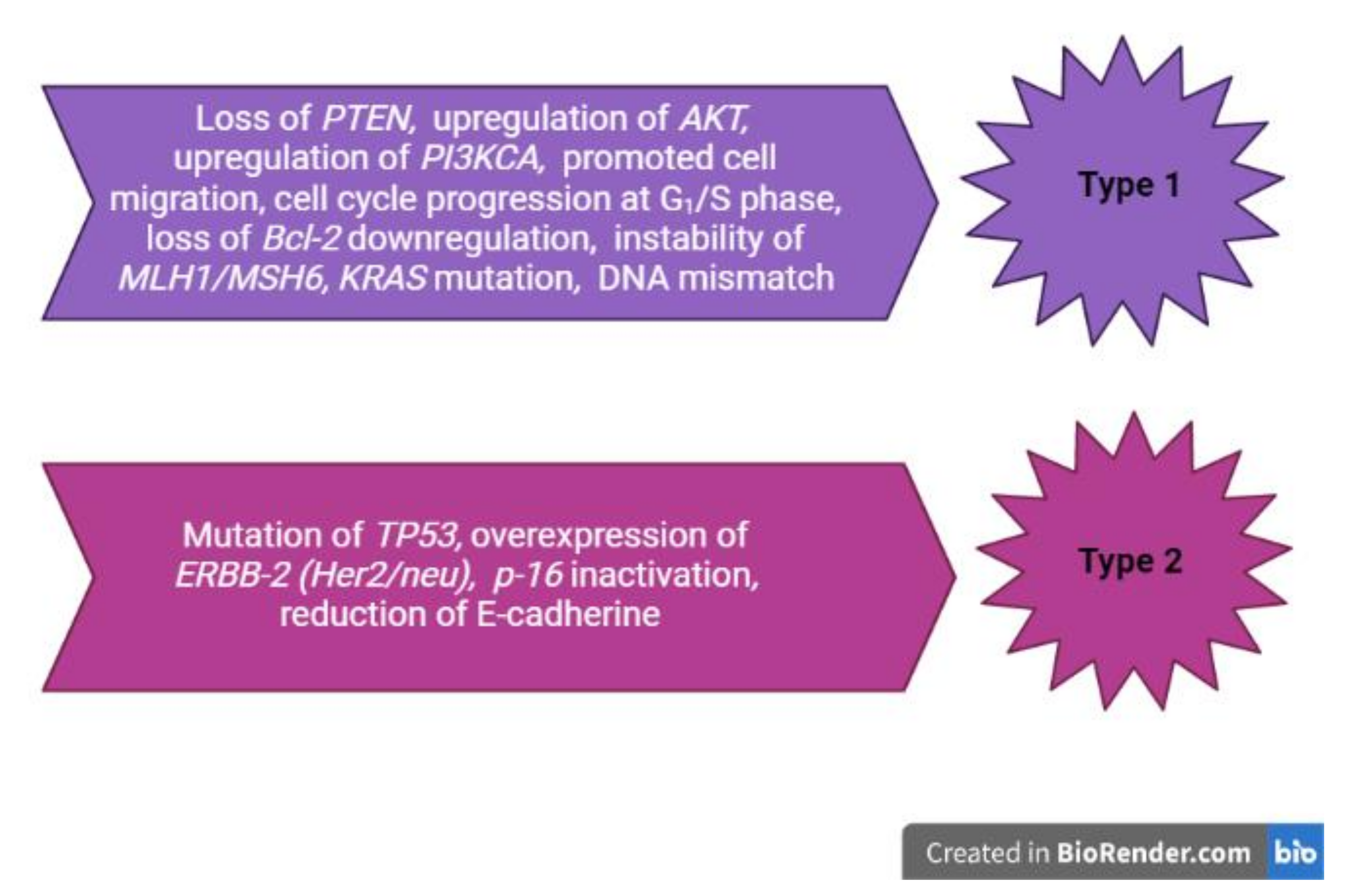
2. Molecular Mechanisms of Endometrial Pathology
3. Management of Endometrial Cancer
3.1. Guidelines for Endometrial Cancer Management
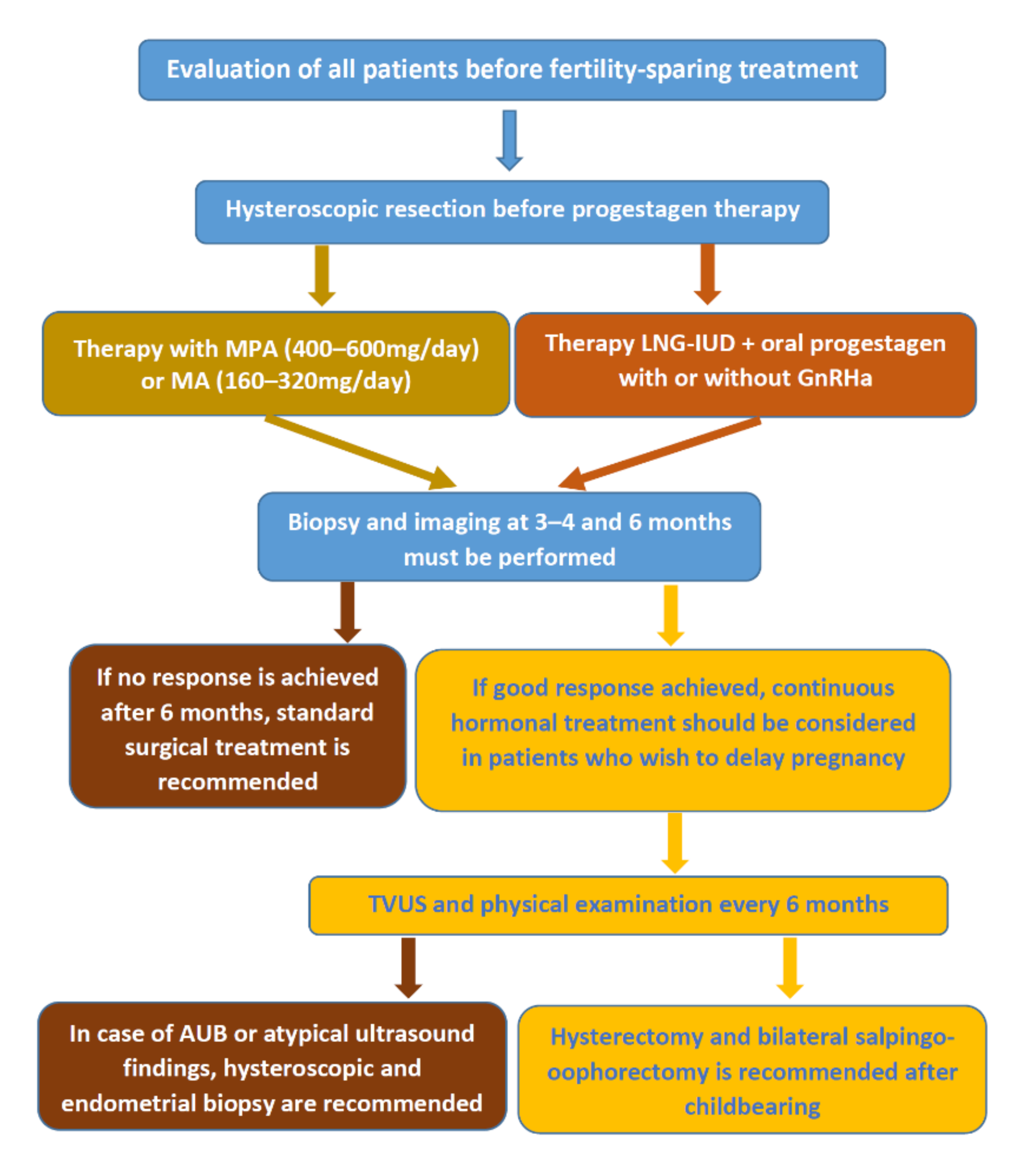
3.2. Fertility-Sparing Treatment for Endometrioid Endometrial Cancer
3.2.1. Conservative Management of Endometrioid Endometrial Cancer
Hormonal Treatment with Confirmed Beneficial Effects
- (a)
- Progestagens
- (b)
- Megestrol acetate and Medroxyprogesterone acetate
- (c)
- Gonadotropin-releasing hormone analogues
Future Treatment Options under Study—Metformin
Levonorgestrel Intrauterine Device
3.2.2. Surgical Treatment
Hysteroscopic Resection
3.3. Role of Adjuvant and Post-Surgical Treatment in Endometrial Cancer
3.4. Conservative Treatment for Persistent Early Endometrial Cancer in Young Women
3.5. IVF Impact on the Risk of Recurrence of Endometrial Cancer after Fertility-Sparing Treatments
4. Endometrial Cancer and Pregnancy
5. Innovative Follow-up Strategies for Endometrial Cancer
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Amant, F.; Moerman, P.; Neven, P.; Timmerman, D.; Van Limbergen, E.; Vergote, I. Endometrial cancer. Lancet 2005, 366, 491–505. [Google Scholar] [CrossRef]
- Dörk, T.; Hillemanns, P.; Tempfer, C.; Breu, J.; Fleisch, M.C. Genetic Susceptibility to Endometrial Cancer: Risk Factors and Clinical Management. Cancers 2020, 12, 2407. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/endometrial-cancer (accessed on 18 October 2021).
- Doherty, M.T.; Sanni, O.B.; Coleman, H.G.; Cardwell, C.R.; McCluggage, W.G.; Quinn, D.; Wylie, J.; McMenamin, Ú.C. Concurrent and future risk of endometrial cancer in women with endometrial hyperplasia: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0232231. [Google Scholar] [CrossRef]
- Urick, M.E.; Bell, D.W. Clinical actionability of molecular targets in endometrial cancer. Nat. Rev. Cancer 2019, 19, 510–521. [Google Scholar] [CrossRef] [PubMed]
- Terzic, M.; Aimagambetova, G.; Kunz, J.; Bapayeva, G.; Aitbayeva, B.; Terzic, S.; Laganà, A.S. Molecular Basis of Endometriosis and Endometrial Cancer: Current Knowledge and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 9274. [Google Scholar] [CrossRef]
- Coll-de la Rubia, E.; Martinez-Garcia, E.; Dittmar, G.; Gil-Moreno, A.; Cabrera, S.; Colas, E. Prognostic Biomarkers in Endometrial Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1900. [Google Scholar] [CrossRef]
- Tung, H.J.; Huang, H.J.; Lai, C.H. Adjuvant and post-surgical treatment in endometrial cancer [published online ahead of print, 2021 Aug 5]. Best Pract. Res. Clin. Obstet. Gynaecol. 2021. [Google Scholar] [CrossRef]
- Terzic, M.; Norton, M.; Terzic, S.; Bapayeva, G.; Aimagambetova, G. Fertility preservation in endometrial cancer patients: Options, challenges and perspectives. Ecancermedicalscience 2020, 14, 1030. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.E.; Bender, D.P. Endometrial Cancer. Obstet. Gynecol. Clin. N. Am. 2019, 46, 89–105. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.H.; Broaddus, R.R. Endometrial Cancer. N. Engl. J. Med. 2020, 383, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.N.A.K.M.; Noone, A.M.; Krapcho, M.; Garshell, J.; Miller, D.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review, 1975–2015; National Cancer Institute: Bethesda, MD, USA, 2015. Available online: https://seer.cancer.gov/csr/1975_2015/ (accessed on 2 October 2021).
- National Cancer Institute. SEER Cancer Stat Facts: Uterine Cancer. Available online: https://seer.cancer.gov/statfacts/html/corp.html (accessed on 2 October 2021).
- Vitale, S.G.; Capriglione, S.; Zito, G.; Lopez, S.; Gulino, F.A.; Di Guardo, F.; Vitagliano, A.; Noventa, M.; La Rosa, V.L.; Sapia, F.; et al. Management of endometrial, ovarian and cervical cancer in the elderly: Current approach to a challenging condition. Arch. Gynecol. Obstet. 2019, 299, 299–315. [Google Scholar] [CrossRef]
- Shiomi, M.; Matsuzaki, S.; Kobayashi, E.; Hara, T.; Nakagawa, S.; Takiuchi, T.; Mimura, K.; Ueda, Y.; Tomimatsu, T.; Kimura, T. Endometrial carcinoma in a gravid uterus: A case report and literature review. BMC Pregnancy Childbirth 2019, 19, 425. [Google Scholar] [CrossRef] [PubMed]
- Ngu, S.F.; Ngan, H.Y.; Chan, K.K. Role of adjuvant and post-surgical treatment in gynaecological cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2021. [published online ahead of print, 2021 Sep 15]. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, 16–41, [published correction appears in Ann Oncol. 2017 Jul 1;28(suppl_4):iv167-iv168]. [Google Scholar] [CrossRef] [PubMed]
- Paleari, L.; Pesce, S.; Rutigliani, M.; Greppi, M.; Obino, V.; Gorlero, F.; Vellone, V.G.; Marcenaro, E. New Insights into Endometrial Cancer. Cancers 2021, 13, 1496. [Google Scholar] [CrossRef] [PubMed]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.; Karnezis, A.N.; et al. A clinically applicable molecular-based classification for endometrial cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef] [Green Version]
- Corzo, C.; Barrientos Santillan, N.; Westin, S.N.; Ramirez, P.T. Updates on Conservative Management of Endometrial Cancer. J. Min. Invasive Gynecol. 2018, 25, 308–313. [Google Scholar] [CrossRef]
- Passarello, K.; Kurian, S.; Villanueva, V. Endometrial Cancer: An Overview of Pathophysiology, Management, and Care. Semin. Oncol. Nurs. 2019, 35, 157–165. [Google Scholar] [CrossRef]
- Njoku, K.; Sutton, C.J.; Whetton, A.D.; Crosbie, E.J. Metabolomic Biomarkers for Detection, Prognosis and Identifying Recurrence in Endometrial Cancer. Metabolites 2020, 10, 314. [Google Scholar] [CrossRef]
- Terzic, M.; Aimagambetova, G.; Terzic, S.; Norton, M.; Bapayeva, G.; Garzon, S. Current role of Pipelle endometrial sampling in early diagnosis of endometrial cancer. Transl. Cancer Res. 2020, 9, 7716–7724. [Google Scholar] [CrossRef]
- Braun, M.M.; Overbeek-Wager, E.A.; Grumbo, R.J. Diagnosis and Management of Endometrial Cancer. Am. Fam. Phys. 2016, 93, 468–474. [Google Scholar]
- Andrijasevic, S.; Dotlic, J.; Arsenovic, N.; Terzic, M. Differences in endometrial carcinoma presentations and characteristics in pre- and postmenopausal women. Srp. Arh. Celok. Lek. 2019, 147, 692–698. [Google Scholar] [CrossRef]
- Terzic, M.M.; Dotlic, J.; Likic, I.; Ladjevic, N.; Brndusic, N.; Arsenovic, N.; Maricic, S.; Mihailovic, T.; Andrijasevic, S. Current diagnostic approach to patients with adnexal masses: Which tools are relevant in routine praxis? Chin. J. Cancer Res. 2013, 25, 55–62. [Google Scholar] [CrossRef]
- Terzic, M.; Dotlic, J.; Likic, I.; Ladjevic, N.; Brndusic, N.; Mihailovic, T.; Andrijasevic, S.; Pilic, I.; Bila, J. Predictive factors of malignancy in patients with adnexal masses. Eur. J. Gynaec. Oncol. 2013, 34, 65–69. [Google Scholar] [PubMed]
- Terzic, M.; Aimagambetova, G.; Norton, M.; Della Corte, L.; Marín-Buck, A.; Lisón, J.F.; Amer-Cuenca, J.J.; Zito, G.; Garzon, S.; Caruso, S.; et al. Scoring systems for the evaluation of adnexal masses nature: Current knowledge and clinical applications. J. Obstet. Gynaecol. 2021, 41, 340–347. [Google Scholar] [CrossRef]
- Jones, E.R.; O’Flynn, H.; Njoku, K.; Crosbie, E.J. Detecting endometrial cancer. Obstet. Gynaecol. 2021, 23, 103–112. [Google Scholar] [CrossRef]
- Costas, T.; Belda, R.; Alcazar, J.L. Transvaginal three-dimensional ultrasound for preoperative assessment of myometrial invasion in patients with endometrial cancer: A systematic review and meta-analysis. Med. Ultrason. 2021. [published online ahead of print, 2021 Mar 14]. [Google Scholar] [CrossRef]
- Faria, S.C.; Devine, C.E.; Rao, B.; Sagebiel, T.; Bhosale, P. Imaging and Staging of Endometrial Cancer. Semin. Ultrasound CT MRI 2019, 40, 287–294. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Survival Rates for Endometrial Cancer. Available online: https://www.cancer.org/cancer/endometrial-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 15 October 2021).
- Scioscia, M.; Noventa, M.; Laganà, A.S. Abnormal uterine bleeding and the risk of endometrial cancer: Can subendometrial vascular ultrasound be of help to discriminate cancer from adenomyosis? Am. J. Obstet. Gynecol. 2020, 223, 605–606. [Google Scholar] [CrossRef]
- Rizzo, S.; Femia, M.; Buscarino, V.; Franchi, D.; Garbi, A.; Zanagnolo, V.; Del Grande, M.; Manganaro, L.; Alessi, S.; Giannitto, C.; et al. Endometrial cancer: An overview of novelties in treatment and related imaging keypoints for local staging. Cancer Imaging 2018, 18, 45. [Google Scholar] [CrossRef]
- Gentry-Maharaj, A.; Karpinskyj, C. Current and future approaches to screening for endometrial cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2020, 65, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Long, B.; Clarke, M.A.; Morillo, A.D.M.; Wentzensen, N.; Bakkum-Gamez, J.N. Ultrasound detection of endometrial cancer in women with postmenopausal bleeding: Systematic review and meta-analysis. Gynecol. Oncol. 2020, 157, 624–633. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Scioscia, M. Endometrial Cancer in Women with Adenomyosis: An Underestimated Risk? Int. J. Fertil. Steril. 2020, 14, 260–261. [Google Scholar] [CrossRef]
- Nougaret, S.; Horta, M.; Sala, E.; Lakhman, Y.; Thomassin-Naggara, I.; Kido, A.; Masselli, G.; Bharwani, N.; Sadowski, E.; Ertmer, A.; et al. Endometrial Cancer MRI staging: Updated Guidelines of the European Society of Urogenital Radiology. Eur. Radiol. 2019, 29, 792–805. [Google Scholar] [CrossRef]
- Yan, B.C.; Li, Y.; Ma, F.H.; Feng, F.; Sun, M.H.; Lin, G.W.; Zhang, G.F.; Qiang, J.W. Preoperative Assessment for High-Risk Endometrial Cancer by Developing an MRI- and Clinical-Based Radiomics Nomogram: A Multicenter Study. J. Magn. Reson. Imaging 2020, 52, 1872–1882. [Google Scholar] [CrossRef]
- Lin, M.Y.; Dobrotwir, A.; McNally, O.; Abu-Rustum, N.R.; Narayan, K. Role of imaging in the routine management of endometrial cancer. Int. J. Gynaecol. Obstet. 2018, 143 (Supplement S2), 109–117. [Google Scholar] [CrossRef]
- Franchi, M.; Garzon, S.; Zorzato, P.C.; Laganà, A.S.; Casarin, J.; Locantore, L.; Raffaelli, R.; Ghezzi, F. PET-CT scan in the preoperative workup of early stage intermediate- and high-risk endometrial cancer. Minim. Invasive Ther. Allied Technol. 2020, 29, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Rockall, A.G.; Barwick, T.D.; Wilson, W.; Singh, N.; Bharwani, N.; Sohaib, A.; Nobbenhuis, M.; Warbey, V.; Miquel, M.; Koh, D.M.; et al. Diagnostic Accuracy of FEC-PET/CT, FDG-PET/CT, and Diffusion-Weighted MRI in Detection of Nodal Metastases in Surgically Treated Endometrial and Cervical Carcinoma. Clin. Cancer Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Chiofalo, B.; Mazzon, I.; Di Angelo Antonio, S.; Amadore, D.; Vizza, E.; Laganà, A.S.; Vocaturo, G.; Calagna, G.; Favilli, A.; Palmara, V.; et al. Hysteroscopic Evaluation of Endometrial Changes in Breast Cancer Women with or without Hormone Therapies: Results from a Large Multicenter Cohort Study. J. Minim. Invasive Gynecol. 2020, 27, 832–839. [Google Scholar] [CrossRef]
- Cignini, P.; Vitale, S.G.; Laganà, A.S.; Biondi, A.; La Rosa, V.L.; Cutillo, G. Preoperative work-up for definition of lymph node risk involvement in early stage endometrial cancer: 5-year follow-up. Updates Surg. 2017, 69, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Aimagambetova, G.; Kaiyrlykyzy, A.; Bapayeva, G.; Ukybassova, T.; Kenbayeva, K.; Ibrayimov, B.; Lyasova, A.; Bonaldo, G.; Buzzaccarini, G.; Noventa, M.; et al. Validation of Pipelle endometrial biopsy in patients with abnormal uterine bleeding in Kazakhstani healthcare setting. Clin. Exper. Obstet. Gynecol. 2021, 48, 706–711. [Google Scholar]
- Tanko, N.M.; Linkov, F.; Bapayeva, G.; Ukybassova, T.; Kaiyrlykyzy, A.; Aimagambetova, G.; Kenbayeva, K.; Ibrayimov, B.; Lyasova, A.; Terzic, M. Pipelle Endometrial Biopsy for Abnormal Uterine Bleeding in Daily Clinical Practice: Why the Approach to Patients Should Be Personalized? J. Pers. Med. 2021, 11, 970. [Google Scholar] [CrossRef] [PubMed]
- Piatek, S.; Warzecha, D.; Kisielewski, F.; Szymusik, I.; Panek, G.; Wielgos, M. Pipelle biopsy and dilatation and curettage in clinical practice: Are factors affecting their effectiveness the same? J. Obstet. Gynaecol. Res. 2019, 45, 645–651. [Google Scholar] [CrossRef]
- Terzic, M.; Aimagambetova, G.; Bapayeva, G.; Ukybassova, T.; Kenbayeva, K.; Kaiyrlykyzy, A.; Ibrayimov, B.; Lyasova, A.; Terzic, S.; Alkatout, I.; et al. Pipelle endometrial sampling success rates in Kazakhstani settings: Results from a prospective cohort analysis. J. Obstet. Gynaecol. 2021, 1–6. [Google Scholar] [CrossRef]
- Terzic, M.; Dotlic, J.; Vasiljevic, M.; Andrijasevic, S.; Norton, M.; Terzic, S.; Laganà, A.S.; Vereczkey, A.; Arsenovic, N. Endometrial polyps in infertility patients: The first study of their clinical characteristics. Clin. Exp. Obstet. Gynecol. 2018, 45, 692–698. [Google Scholar] [CrossRef]
- Arend, R.C.; Jones, B.A.; Martinez, A.; Goodfellow, P. Endometrial cancer: Molecular markers and management of advanced stage disease. Gynecol. Oncol. 2018, 150, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Terzic, M.; Dotlic, J.; Likic, I.; Nikolic, B.; Brndusic, N.; Pilic, I.; Bila, J.; Maricic, S.; Arsenovic, N. Diagnostic value of serum tumor markers evaluation for adnexal masses. Open Med. 2014, 9, 210–216. [Google Scholar] [CrossRef]
- Terzic, M.; Aimagambetova, G. Clinical importance of serum tumor markers assessment in patients with adnexal masses. In Advances in Health and Disease; Duncan, L.T., Ed.; Nova Science Publishers, Inc.: New York, NY, USA, 2019; Volume 15, pp. 67–111. ISBN 978153616497. [Google Scholar]
- Screening Tool for Gynecologic Cancers Assessed. Cancer Discov. 2018, 8, 525–526. [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Li, L.; Douville, C.; Yen, T.T.; Kinde, I.; Sundfelt, K.; Kjær, S.K.; Hruban, R.H.; Shih, I.M.; Wang, T.L.; et al. Evaluation of liquid from the Papanicolaou test and other liquid biopsies for the detection of endometrial and ovarian cancers. Sci. Transl. Med. 2018, 10, eaap8793. [Google Scholar] [CrossRef] [Green Version]
- Casarin, J.; Bogani, G.; Serati, M.; Pinelli, C.; Laganà, A.S.; Garzon, S.; Raspagliesi, F.; Ghezzi, F. Presence of Glandular Cells at the Preoperative Cervical Cytology and Local Recurrence in Endometrial Cancer. Int. J. Gynecol. Pathol. 2020, 39, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Hutt, S.; Tailor, A.; Ellis, P.; Michael, A.; Butler-Manuel, S.; Chatterjee, J. The role of biomarkers in endometrial cancer and hyperplasia: A literature review. Acta Oncol. 2019, 58, 342–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiegand, K.C.; Lee, A.F.; Al-Agha, O.M.; Chow, C.; Kalloger, S.E.; Scott, D.W.; Steidl, C.; Wiseman, S.M.; Gascoyne, R.D.; Gilks, B.; et al. Loss of BAF250a (ARID1A) is frequent in high-grade endometrial carcinomas. J. Pathol. 2011, 224, 328–333. [Google Scholar] [CrossRef]
- Wang, L.; Li, L.; Wu, M.; Lang, J. The prognostic role of peritoneal cytology in stage IA endometrial endometrioid carcinomas. Curr. Probl. Cancer 2020, 44, 100514. [Google Scholar] [CrossRef] [PubMed]
- Boretto, M.; Maenhoudt, N.; Luo, X.; Hennes, A.; Boeckx, B.; Bui, B.; Heremans, R.; Perneel, L.; Kobayashi, H.; Van Zundert, I.; et al. Patient-derived organoids from endometrial disease capture clinical heterogeneity and are amenable to drug screening. Nat. Cell Biol. 2019, 21, 1041–1051. [Google Scholar] [CrossRef] [PubMed]
- Hapangama, D.K.; Kamal, A.; Saretzki, G. Implications of telomeres and telomerase in endometrial pathology. Hum. Reprod. Update 2017, 23, 166–187. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.; Kim, S.E.; Lee, D.-Y.; Choi, D. Factors associated with endometrial pathology during tamoxifen therapy in women with breast cancer: A retrospective analysis of 821 biopsies. Breast Cancer Res. Treat. 2019. [Google Scholar] [CrossRef]
- Wiwatpanit, T.; Murphy, A.R.; Lu, Z.; Urbanek, M.; Burdette, J.E.; Woodruff, T.K.; Kim, J.J. Scaffold-Free Endometrial Organoids Respond to Excess Androgens Associated With Polycystic Ovarian Syndrome. J. Clin. Endocrinol. Metab. 2020, 105, 769–780. [Google Scholar] [CrossRef]
- Drizi, A.; Djokovic, D.; Laganà, A.S.; van Herendael, B. Impaired inflammatory state of the endometrium: A multifaceted approach to endometrial inflammation. Current insights and future directions. Prz. Menopauzalny 2020, 19, 90–100. [Google Scholar] [CrossRef]
- Puente, E.; Alonso, L.; Laganà, A.S.; Ghezzi, F.; Casarin, J.; Carugno, J. Chronic Endometritis: Old Problem, Novel Insights and Future Challenges. Int. J. Fertil. Steril. 2020, 13, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Benati, M.; Montagnana, M.; Danese, E.; Mazzon, M.; Paviati, E.; Garzon, S.; Laganà, A.S.; Casarin, J.; Giudici, S.; Raffaelli, R.; et al. Aberrant Telomere Length in Circulating Cell-Free DNA as Possible Blood Biomarker with High Diagnostic Performance in Endometrial Cancer. Pathol. Oncol. Res. 2020, 26, 2281–2289. [Google Scholar] [CrossRef]
- Chen, J.; Cao, D.; Yang, J.; Yu, M.; Zhou, H.; Cheng, N.; Wang, J.; Zhang, Y.; Peng, P.; Shen, K. Management of Recurrent Endometrial Cancer or Atypical Endometrial Hyperplasia Patients After Primary Fertility-Sparing Therapy. Front. Oncol. 2021, 11, 738370. [Google Scholar] [CrossRef] [PubMed]
- Sundar, S.; Balega, J.; Crosbie, E.; Drake, A.; Edmondson, R.; Fotopoulou, C.; Gallos, I.; Ganesan, R.; Gupta, J.; Johnson, N.; et al. BGCS uterine cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 71–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, A.; Taylor, A.; Guttery, D.S.; Moss, E.L. Innovative Follow-up Strategies for Endometrial Cancer. Clin. Oncol. 2021, 33, e383–e392. [Google Scholar] [CrossRef] [PubMed]
- Schuurman, T.; Zilver, S.; Samuels, S.; Schats, W.; Amant, F.; van Trommel, N.; Lok, C. Fertility-Sparing Surgery in Gynecologic Cancer: A Systematic Review. Cancers 2021, 13, 1008. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, S.M.; Esteban, A.; Nigra, M.A.; Palacios, A.T.; Alzate-Granados, J.P.; Borla, H.F. Updates on conservative management of endometrial cancer in patients younger than 45 years. Gynecol. Oncol. 2021, 161, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Falcone, F.; Laurelli, G.; Losito, S.; Di Napoli, M.; Granata, V.; Greggi, S. Fertility preserving treatment with hysteroscopic resection followed by progestin therapy in young women with early endometrial cancer. J. Gynecol. Oncol. 2017, 28, e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, D.; Behrens, G.; Keimling, M.; Jochem, C.; Ricci, C.; Leitzmann, M. A systematic review and meta-analysis of physical activity and endometrial cancer risk. Eur. J. Epidemiol. 2015, 30, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Freytag, D.; Pape, J.; Dhanawat, J.; Günther, V.; Maass, N.; Gitas, G.; Laganà, A.S.; Allahqoli, L.; Meinhold-Heerlein, I.; Moawad, G.N.; et al. Challenges Posed by Embryonic and Anatomical Factors in Systematic Lymphadenectomy for Endometrial Cancer. J. Clin. Med. 2020, 9, 4107. [Google Scholar] [CrossRef] [PubMed]
- Gitas, G.; Freytag, D.; Allahqoli, L.; Baum, S.; Rody, A.; Maass, N.; Dinas, K.; Laganà, A.S.; Moawad, G.; Sotiriadis, A.; et al. Lymphadenectomy in endometrial cancer—Achieving more with less? Minim. Invasive Ther. Allied Technol. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Casarin, J.; Bogani, G.; Piovano, E.; Falcone, F.; Ferrari, F.; Odicino, F.; Puppo, A.; Bonfiglio, F.; Donadello, N.; Pinelli, C.; et al. Survival implication of lymphadenectomy in patients surgically treated for apparent early-stage uterine serous carcinoma. J. Gynecol. Oncol. 2020, 31, e64. [Google Scholar] [CrossRef]
- Hamilton, C.A.; Pothuri, B.; Arend, R.C.; Backes, F.J.; Gehrig, P.A.; Soliman, P.T.; Thompson, J.S.; Urban, R.R.; Burke, W.M. Endometrial cancer: A society of gynecologic oncology evidence-based review and recommendations, part II. Gynecol. Oncol. 2021, 160, 827–834. [Google Scholar] [CrossRef]
- Emons, G.; Steiner, E.; Vordermark, D.; Uleer, C.; Bock, N.; Paradies, K.; Ortmann, O.; Aretz, S.; Mallmann, P.; Kurzeder, C.; et al. Interdisciplinary Diagnosis, Therapy and Follow-up of Patients with Endometrial Cancer. Guideline (S3-Level, AWMF Registry Nummer 032/034-OL, April 2018)—Part 1 with Recommendations on the Epidemiology, Screening, Diagnosis and Hereditary Factors of Endometrial Cancer. Geburtshilfe Und Frauenheilkd. 2018, 78, 949–971. [Google Scholar] [CrossRef] [Green Version]
- Emons, G.; Steiner, E.; Vordermark, D.; Uleer, C.; Bock, N.; Paradies, K.; Ortmann, O.; Aretz, S.; Mallmann, P.; Kurzeder, C.; et al. Interdisciplinary Diagnosis, Therapy and Follow-up of Patients with Endometrial Cancer. Guideline (S3-Level, AWMF Registry Number 032/034-OL, April 2018)—Part 2 with Recommendations on the Therapy and Follow-up of Endometrial Cancer, Palliative Care, Psycho-oncological/Psychosocial Care/Rehabilitation/Patient Information and Healthcare Facilities. Geburtshilfe Frauenheilkunde 2018, 78, 1089–1109. [Google Scholar] [CrossRef] [Green Version]
- Shigeta, S.; Nagase, S.; Mikami, M.; Ikeda, M.; Shida, M.; Sakaguchi, I.; Ushioda, N.; Takahashi, F.; Yamagami, W.; Yaegashi, N.; et al. Assessing the effect of guideline introduction on clinical practice and outcome in patients with endometrial cancer in Japan: A project of the Japan Society of Gynecologic Oncology (JSGO) guideline evaluation committee. J. Gynecol. Oncol. 2017, 28, e76. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y. Tailored Therapy Based on Molecular Characteristics in Endometrial Cancer. BioMed Res. Int. 2021, 2068023. [Google Scholar] [CrossRef]
- Vermij, L.; Smit, V.; Nout, R.; Bosse, T. Incorporation of molecular characteristics into endometrial cancer management. Histopathology 2020, 76, 52–63. [Google Scholar] [CrossRef] [PubMed]
- León-Castillo, A.; Gilvazquez, E.; Nout, R.; Smit, V.T.; McAlpine, J.N.; McConechy, M.; Kommoss, S.; Brucker, S.Y.; Carlson, J.W.; Epstein, E.; et al. Clinicopathological and molecular haracterization of ‘multiple-classifier’ endometrial carcinomas. J. Pathol. 2020, 250, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Van den Heerik, A.; Horeweg, N.; de Boer, S.M.; Bosse, T.; Creutzberg, C.L. Adjuvant therapy for endometrial cancer in the era of molecular classification: Radiotherapy, chemoradiation and novel targets for therapy. Int. J. Gyneccol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 594–604. [Google Scholar] [CrossRef]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Cancer Genome Atlas Research Network; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.; Ronn, R.; Tallon, N.; Holzer, H. Fertility preservation in reproductive-age women facing gonadotoxic treatments. Curr. Oncol. 2015, 22, e294–e304. [Google Scholar] [CrossRef] [Green Version]
- Won, S.; Kim, M.K.; Seong, S.J. Fertility-sparing treatment in women with endometrial cancer. Clin. Exp. Reprod. Med. 2020, 47, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Garzon, S.; Uccella, S.; Zorzato, P.C.; Bosco, M.; Franchi, M.P.; Student, V.; Mariani, A. Fertility-sparing management for endometrial cancer: Review of the literature. Minerva Med. 2021, 112, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Cho, A.; Lee, S.W.; Park, J.Y.; Kim, D.Y.; Suh, D.S.; Kim, J.H.; Kim, Y.M.; Kim, Y.T. Continued medical treatment for persistent early endometrial cancer in young women. Gynecol. Oncol. 2021, 160, 413–417. [Google Scholar] [CrossRef]
- Rodolakis, A.; Biliatis, I.; Morice, P.; Reed, N.; Mangler, M.; Kesic, V.; Denschlag, D. European Society of Gynecological Oncology Task Force for Fertility Preservation: Clinical recommendations for fertility-sparing management in young endometrial cancer patients. Int. J. Gynecol. Cancer 2015, 25, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.R.; Lu, Q.; Zhou, R.; Wang, Y.Q.; Liang, W.Y.; Liu, H.X.; Tang, H.R.; Wu, G.Z.; Liu, X.S.; Zhang, H.; et al. Analysis of pregnancy outcome after fertility-preserving treatment among women with atypical endometrial hyperplasia or endometrial carcinoma. Zhonghua Fu Chan Ke Za Zhi 2020, 55, 857–864. [Google Scholar] [CrossRef]
- Varga, A.; Henriksen, E. Histologic observations on the effect of 17-alpha-hydroxyprogesterone-17-n-caproate on endometrial carcinoma. Obstet. Gynecol. 1965, 26, 656–664. [Google Scholar]
- Onsrud, M. Adjuvant hydroxyprogesterone caproate in stage I endometrial carcinoma: Changes in numbers and reactivities of some blood lymphocyte subpopulations. Gynecol. Oncol. 1982, 14, 355–364. [Google Scholar] [CrossRef]
- Martin-Hirsch, P.L.; Jarvis, G.; Kitchener, H.; Lilford, R. Progestagens for endometrial cancer. Cochrane Database Syst. Rev. 2000, CD001040. [Google Scholar] [CrossRef]
- Vitale, S.G.; Rossetti, D.; Tropea, A.; Biondi, A.; Laganà, A.S. Fertility sparing surgery for stage IA type I and G2 endometrial cancer in reproductive-aged patients: Evidence-based approach and future perspectives. Updates Surg. 2017, 69, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Yamout, W.; Yazbeck, J.; Moufawad, G.; Abboud, K.; Sleiman, Z. Fertility Preservation Management for Endometrial Cancer in Fertility Preservation in Gynecological Cancer: Current Management and Novel Insights; Simone, G., Antonio, S.L., Eds.; Nova Science Publisher, Inc.: New York, NY, USA, 2021; Chapter 8; p. 224. [Google Scholar]
- Lee, M.; Piao, J.; Jeon, M.J. Risk Factors Associated with Endometrial Pathology in Premenopausal Breast Cancer Patients Treated with Tamoxifen. Yonsei Med. J. 2020, 61, 317–322. [Google Scholar] [CrossRef]
- Jerzak, K.J.; Duska, L.; MacKay, H.J. Endocrine therapy in endometrial cancer: An old dog with new tricks. Gynecol. Oncol. 2019, 153, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Tamauchi, S.; Kajiyama, H.; Utsumi, F.; Suzuki, S.; Niimi, K.; Sakata, J.; Mizuno, M.; Shibata, K.; Kikkawa, F. Efficacy of medroxyprogesterone acetate treatment and retreatment for atypical endometrial hyperplasia and endometrial cancer. J. Obstet. Gynaecol. Res. 2018, 44, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Gompel, A. Progesterone and endometrial cancer. Best practice & research. Clin. Obstet. Gynaecol. 2020, 69, 95–107. [Google Scholar] [CrossRef]
- Martin-Hirsch, P.P.; Bryant, A.; Keep, S.L.; Kitchener, H.C.; Lilford, R. Adjuvant progestagens for endometrial cancer. Cochrane Database Syst. Rev. 2011, 6, CD001040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, N.; Broaddus, R.R.; Urbauer, D.L.; Balakrishnan, N.; Milbourne, A.; Schmeler, K.M.; Meyer, L.A.; Soliman, P.T.; Lu, K.H.; Ramirez, P.T.; et al. Treatment of Low-Risk Endometrial Cancer and Complex Atypical Hyperplasia With the Levonorgestrel-Releasing Intrauterine Device. Obstet. Gynecol. 2018, 131, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, Z.R.; Huang, L.N.; Wissing, M.D.; Franco, E.L.; Gotlieb, W.H. Does hormonal therapy for fertility preservation affect the survival of young women with early stage endometrial cancer? Cancer 2017, 123, 1545–1554. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Gao, W.; Zheng, P.; Sun, X.; Wang, L. Medroxyprogesterone acetate causes the alterations of endoplasmic reticulum related mRNAs and lncRNAs in endometrial cancer cells. BMC Med. Genom. 2019, 12, 163. [Google Scholar] [CrossRef] [PubMed]
- Mu, N.; Dong, M.; Li, L.; Xia, M.; Qv, L.; Wang, Y.; Dong, C.; Chen, Y.; Zuo, Y.; Hou, J.; et al. Synergistic effect of metformin and medroxyprogesterone 17-acetate on the development of endometrial cancer. Oncol. Rep. 2018, 39, 2015–2021. [Google Scholar] [CrossRef]
- Mitsuhashi, A.; Kawasaki, Y.; Hori, M.; Fujiwara, T.; Hanaoka, H.; Shozu, M. Medroxyprogesterone acetate plus metformin for fertility-sparing treatment of atypical endometrial hyperplasia and endometrial carcinoma: Trial protocol for a prospective, randomized, open, blinded-endpoint design, dose-response trial (FELICIA trial). BMJ Open 2020, 10, e035416. [Google Scholar] [CrossRef] [Green Version]
- Dore, M.; Filoche, S.; Danielson, K.; Henry, C. Efficacy of the LNG-IUS for treatment of endometrial hyperplasia and early stage endometrial cancer: Can biomarkers predict response? Gynecol. Oncol. Rep. 2021, 36, 100732. [Google Scholar] [CrossRef]
- Limonta, P.; Montagnani Marelli, M.; Mai, S.; Motta, M.; Martini, L.; Moretti, R.M. GnRH receptors in cancer: From cell biology to novel targeted therapeutic strategies. Endocr. Rev. 2012, 33, 784–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ethier, J.L.; Desautels, D.N.; Amir, E.; MacKay, H. Is hormonal therapy effective in advanced endometrial cancer? A systematic review and meta-analysis. Gynecol. Oncol. 2017, 147, 158–166. [Google Scholar] [CrossRef]
- Emons, G.; Gründker, C. The Role of Gonadotropin-Releasing Hormone (GnRH) in Endometrial Cancer. Cells 2021, 10, 292. [Google Scholar] [CrossRef] [PubMed]
- Mitsuhashi, A.; Sato, Y.; Kiyokawa, T.; Koshizaka, M.; Hanaoka, H.; Shozu, M. Phase II study of medroxyprogesterone acetate plus metformin as a fertility-sparing treatment for atypical endometrial hyperplasia and endometrial cancer. Ann Oncol. 2016, 27, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Aljofan, M.; Riethmacher, D. Anticancer activity of metformin: A systematic review of the literature. Future Sci. OA 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Takhwifa, F.; Aninditha, T.; Setiawan, H.; Sauriasari, R. The potential of metformin as an antineoplastic in brain tumors: A systematic review. Heliyon 2021, 7, e06558. [Google Scholar] [CrossRef] [PubMed]
- Farkhondeh, T.; Amirabadizadeh, A.; Aramjoo, H.; Llorens, S.; Roshanravan, B.; Saeedi, F.; Talebi, M.; Shakibaei, M.; Samarghandian, S. Impact of Metformin on Cancer Biomarkers in Non-Diabetic Cancer Patients: A Systematic Review and Meta-Analysis of Clinical Trials. Curr. Oncol. 2021, 28, 1412–1423. [Google Scholar] [CrossRef]
- Soliman, P.T.; Westin, S.N.; Iglesias, D.A.; Fellman, B.M.; Yuan, Y.; Zhang, Q.; Yates, M.S.; Broaddus, R.R.; Slomovitz, B.M.; Lu, K.H.; et al. Everolimus, Letrozole, and Metformin in Women with Advanced or Recurrent Endometrioid Endometrial Cancer: A Multi-Center, Single Arm, Phase II Study. Clin Cancer Res. 2020, 26, 581–587. [Google Scholar] [CrossRef] [Green Version]
- Meireles, C.G.; Pereira, S.A.; Valadares, L.P.; Rego, D.F.; Simeoni, L.A.; Guerra, E.N.; Lofrano-Porto, A. Effects of metformin on endometrial cancer: Systematic review and meta-analysis. Gynecol. Oncol. 2017, 147, 167–180. [Google Scholar] [CrossRef]
- Leone Roberti Maggiore, U.; Martinelli, F.; Dondi, G.; Bogani, G.; Chiappa, V.; Evangelista, M.T.; Liberale, V.; Ditto, A.; Ferrero, S.; Raspagliesi, F. Efficacy and fertility outcomes of levonorgestrel-releasing intra-uterine system treatment for patients with atypical complex hyperplasia or endometrial cancer: A retrospective study. J. Gynecol. Oncol. 2019, 30, e57. [Google Scholar] [CrossRef] [PubMed]
- Novikova, O.V.; Nosov, V.B.; Panov, V.A.; Novikova, E.G.; Krasnopolskaya, K.V.; Andreeva, Y.Y.; Shevchuk, A.S. Live births and maintenance with levonorgestrel IUD improve disease-free survival after fertility-sparing treatment of atypical hyperplasia and early endometrial cancer. Gynecol. Oncol. 2021, 161, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Luo, B.; Zheng, Y.; Zhang, H.; Li, J.; Sidell, N. Oral and intrauterine progestagens for atypical endometrial hyperplasia. Cochrane Database Syst. Rev. 2018, 12, CD009458. [Google Scholar] [CrossRef] [PubMed]
- Chen, X. The current situation of the levonorgestrel intrauterine system (LNG-IUS) in conservative treatment for patients with early-stage endometrial cancer and atypical hyperplasia. J. Gynecol. Oncol. 2019, 30, e79. [Google Scholar] [CrossRef]
- Gallos, I.D.; Yap, J.; Rajkhowa, M.; Luesley, D.M.; Coomarasamy, A.; Gupta, J.K. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2012, 207. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Xu, Y.; Xu, Y.; Zhu, Q.; Xie, L.; Shan, W.; Ning, C.; Xie, B.; Shi, Y.; Luo, X.; et al. Treatment efficiency of comprehensive hysteroscopic evaluation and lesion resection combined with progestin therapy in young women with endometrial atypical hyperplasia and endometrial cancer. Gynecol. Oncol. 2019, 153, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparac, V.; Ujevic, B.; Ujevic, M.; Pagon-Belina, Z.; Marton, U. Successful pregnancy after hysteroscopic removal of grade I endometrial carcinoma in a young woman with Lynch syndrome. Int. J. Gynecol. Cancer 2006, 16 (Supplement S1), 442–445. [Google Scholar] [CrossRef] [PubMed]
- Vilos, G.A.; Ettler, H.C.; Edris, F.; Hollett-Caines, J.; Abu-Rafea, B. Endometrioid adenocarcinoma treated by hysteroscopic endomyometrial resection. J. Minim. Invasive Gynecol. 2007, 14, 119–122. [Google Scholar] [CrossRef]
- Mazzon, I.; Corrado, G.; Masciullo, V.; Morricone, D.; Ferrandina, G.; Scambia, G. Conservative surgical management of stage IA endometrial carcinoma for fertility preservation. Fertil. Steril. 2010, 93, 1286–1289. [Google Scholar] [CrossRef]
- Alonso, S.; Castellanos, T.; Lapuente, F.; Chiva, L. Hysteroscopic surgery for conservative management in endometrial cancer: A review of the literature. Ecancermedicalscience 2015, 9, 505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, W., Jr.; Bosch, W.R.; Harkenrider, M.M.; Strauss, J.B.; Abu-Rustum, N.; Albuquerque, K.V.; Beriwal, S.; Creutzberg, C.L.; Eifel, P.J.; Erickson, B.A.; et al. NRG Oncology/RTOG Consensus Guidelines for Delineation of Clinical Target Volume for Intensity Modulated Pelvic Radiation Therapy in Postoperative Treatment of Endometrial and Cervical Cancer: An Update. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.F.; He, W.; Fu, S.; Zhao, H.; Sun, C.C.; Suidan, R.S.; Woodard, T.L.; Rauh-Hain, J.A.; Westin, S.N.; Giordano, S.H.; et al. National patterns of care and fertility outcomes for reproductive-aged women with endometrial cancer or atypical hyperplasia. Am. J. Obstet. Gynecol. 2019, 221, e1–e474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elizur, S.E.; Beiner, M.E.; Korach, J.; Weiser, A.; Ben-Baruch, G.; Dor, J. Outcome of in vitro fertilization treatment in infertile women conservatively treated for endometrial adenocarcinoma. Fertil. Steril. 2007, 88, 1562–1567. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Choe, S.A.; Kim, M.K.; Yun, B.S.; Seong, S.J.; Kim, Y.S. Outcomes of in vitro fertilization cycles following fertility-sparing treatment in stage IA endometrial cancer. Arch. Gynecol. Obstet. 2019, 300, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.M.; Lai, C.H.; Huang, H.Y.; Wang, H.S.; Soong, Y.K. A successful live twin birth by in vitro fertilization after conservative treatment of recurrent endometrial cancer. Chang. Gung Med. J. 2008, 31, 102–106. [Google Scholar]
- Vaugon, M.; Peigné, M.; Phelippeau, J.; Gonthier, C.; Koskas, M. IVF impact on the risk of recurrence of endometrial adenocarcinoma after fertility-sparing management. Reprod. Biomed. Online 2021, 43, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Skalkidou, A.; Sergentanis, T.N.; Gialamas, S.P.; Georgakis, M.K.; Psaltopoulou, T.; Trivella, M.; Siristatidis, C.S.; Evangelou, E.; Petridou, E. Risk of endometrial cancer in women treated with ovary-stimulating drugs for subfertility. Cochrane Database Syst. Rev. 2017, 3, CD010931. [Google Scholar] [CrossRef] [PubMed]
- Salani, R.; Billingsley, C.C.; Crafton, S.M. Cancer and pregnancy: An overview for obstetricians and gynecologists. Am. J. Obstet. Gynecol. 2014, 211, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.M.; Tanner, E.J.; Pavone, M.E. Management and Recommendations for Future Pregnancy in Patients with Early-Stage Endometrial Cancer: A Survey of Gynecologic Oncologists and Reproductive Endocrinology and Infertility Specialists. J. Adolesc. Young Adult Oncol. 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Seong, S.J.; Kim, T.J.; Kim, J.W.; Kim, S.M.; Bae, D.S.; Nam, J.H. Pregnancy outcomes after fertility-sparing management in young women with early endometrial cancer. Obstet. Gynecol. 2013, 121, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, A.G.; Fallaas Dahl, G.; Nesbakken, A.J.; Lund, K.V.; Amant, F. Endometrial cancer during pregnancy: Management strategies. Int. J. Gynecol. Cancer 2019, 29, 1221–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, S.H.; Shim, S.H.; Lee, S.J.; Lee, J.Y.; Kim, S.N.; Kang, S.B. Pregnancy and oncologic outcomes after fertility-sparing management for early stage endometrioid endometrial cancer. Int. J. Gynecol. Cancer 2019, 29, 77–85. [Google Scholar] [CrossRef]
- Piergentili, R.; Zaami, S.; Cavaliere, A.F.; Signore, F.; Scambia, G.; Mattei, A.; Marinelli, E.; Gulia, C.; Perelli, F. Non-Coding RNAs as Prognostic Markers for Endometrial Cancer. Int. J. Mol. Sci. 2021, 22, 3151. [Google Scholar] [CrossRef]
- Laganà, A.S.; Garzon, S.; Unfer, V. New clinical targets of d-chiro-inositol: Rationale and potential applications. Expert Opin. Drug Metab. Toxicol. 2020, 16, 703–710. [Google Scholar] [CrossRef]
- Laganà, A.S.; Unfer, V. D-Chiro-Inositol’s action as aromatase inhibitor: Rationale and potential clinical targets. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 10575–10576. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Class | Name | Molecular characterization | Prognosis | |
|---|---|---|---|---|
| 1 | Ultra-Mutated POLE | Increased mutations and hot spots mutations in esonucleasic POLE domain; increased frequency of C-A transversions; PTEN, PIK3R1, PIK3CA, KRAS, and FBXW7 gene mutations. | Favorable |  |
| 2 | Copy-Number Low (CNL) | EEC of grade 1 and 2 with microsatellite stability; low frequency of mutations; β catenin gene (CTNNB1) alteration. | ||
| 3 | Microsatellite instability (MSI) | Microsatellite instability caused by MLH1 promoter methylation; high frequency of mutations—KRAS and PTEN; RPL22 frameshift mutations. | ||
| 4 | Copy-Number High (CNH) | High number of aberrations in copy numbers and a low frequency of mutations; frequent mutations of P53, FBXW7, and PPP2R1A gene; rare mutations of PTEN and KRAS mutations. | Unfavorable | |
| Fertility-Sparing Therapy Options for Endometrioid Endometrial Carcinoma | |||
|---|---|---|---|
| Conservative | Surgical | ||
| Hormonal therapy (single agent or medications combined) | LNG-IUD (alone or combined with hormones) | Hysteroscopic resection followed by progestagens | |
| With confirmed beneficial effect | Used earlier, but not currently advised | ||
| Progestagens | 17-hydroxyprogesterone caproate | ||
| MA and MPA | Selective estrogen receptors modulators | ||
| GnRHa | Aromatase Inhibitors | ||
| Metformin | Selective progesterone receptors modulators | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aimagambetova, G.; Terzic, S.; Laganà, A.S.; Bapayeva, G.; la Fleur, P.; Terzic, M. Contemporary Fertility-Sparing Management Options of Early Stage Endometrioid Endometrial Cancer in Young Nulliparous Patients. J. Clin. Med. 2022, 11, 196. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010196
Aimagambetova G, Terzic S, Laganà AS, Bapayeva G, la Fleur P, Terzic M. Contemporary Fertility-Sparing Management Options of Early Stage Endometrioid Endometrial Cancer in Young Nulliparous Patients. Journal of Clinical Medicine. 2022; 11(1):196. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010196
Chicago/Turabian StyleAimagambetova, Gulzhanat, Sanja Terzic, Antonio Simone Laganà, Gauri Bapayeva, Philip la Fleur, and Milan Terzic. 2022. "Contemporary Fertility-Sparing Management Options of Early Stage Endometrioid Endometrial Cancer in Young Nulliparous Patients" Journal of Clinical Medicine 11, no. 1: 196. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11010196