
Impact of On-Clopidogrel Platelet Reactivity on Incidence of Peri-Interventional Bleeding in Patients Undergoing Transcatheter Aortic Valve Implantation

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Kumbhani, D.J.; Alexander, K.P.; Calhoon, J.H.; Desai, M.Y.; Kaul, S.; Lee, J.C.; Ruiz, C.E.; Vassileva, C.M. 2017 ACC Expert Consensus Decision Pathway for Transcatheter Aortic Valve Replacement in the Management of Adults with Aortic Stenosis: A Report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J. Am. Coll. Cardiol. 2017, 69, 1313–1346. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Fontana, G.; Jilaihawi, H.; Chakravarty, T.; Kofoed, K.; De Backer, O.; Asch, F.M.; Ruiz, C.E.; Olsen, N.T.; Trento, A.; et al. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N. Engl. J. Med. 2015, 373, 2015–2024. [Google Scholar] [CrossRef] [PubMed]
- Ruile, P.; Jander, N.; Blanke, P.; Schoechlin, S.; Reinöhl, J.; Gick, M.; Rothe, J.; Langer, M.; Leipsic, J.; Buettner, H.-J.; et al. Course of early subclinical leaflet thrombosis after transcatheter aortic valve implantation with or without oral anticoagulation. Clin. Res. Cardiol. 2017, 106, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Nijenhuis, V.J.; Brouwer, J.; Delewi, R.; Hermanides, R.S.; Holvoet, W.; Dubois, C.L.; Frambach, P.; De Bruyne, B.; Van Houwelingen, G.K.; Van Der Heyden, J.A.; et al. Anticoagulation with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N. Engl. J. Med. 2020, 382, 1696–1707. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients with Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar] [CrossRef]
- Gurbel, P.A.; Bliden, K.P.; Hiatt, B.L.; O’Connor, C.M. Clopidogrel for coronary stenting: Response variability, drug resistance, and the effect of pretreatment platelet reactivity. Circulation 2003, 107, 2908–2913. [Google Scholar] [CrossRef] [Green Version]
- Hochholzer, W.; Trenk, D.; Frundi, D.; Blanke, P.; Fischer, B.; Andris, K.; Bestehorn, H.P.; Büttner, H.J.; Neumann, F.J. Time dependence of platelet inhibition after a 600-mg loading dose of clopidogrel in a large, unselected cohort of candidates for percutaneous coronary intervention. Circulation 2005, 111, 2560–2564. [Google Scholar] [CrossRef]
- Hochholzer, W.; Trenk, D.; Fromm, M.F.; Valina, C.M.; Stratz, C.; Bestehorn, H.P.; Büttner, H.J.; Neumann, F.J. Impact of cytochrome P450 2C19 loss-of-function polymorphism and of major demographic characteristics on residual platelet function after loading and maintenance treatment with clopidogrel in patients undergoing elective coronary stent placement. J. Am. Coll. Cardiol. 2010, 55, 2427–2434. [Google Scholar] [CrossRef] [Green Version]
- Stratz, C.; Bömicke, T.; Younas, I.; Kittel, A.; Amann, M.; Valina, C.M.; Nührenberg, T.; Trenk, D.; Neumann, F.-J.; Hochholzer, W. Comparison of Immature Platelet Count to Established Predictors of Platelet Reactivity During Thienopyridine Therapy. J. Am. Coll. Cardiol. 2016, 68, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Nührenberg, T.G.; Hromek, J.; Kille, A.; Hochholzer, W.; Hein, M.; Trenk, D.; Neumann, F.J.; Stratz, C.; Ruile, P. Impact of On-Clopidogrel Platelet Reactivity on Incidence of Hypoattenuated Leaflet Thickening After Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Gross, L.; Jochheim, D.; Nitschke, T.; Baquet, M.; Orban, M.; Holdt, L.; Zadrozny, M.; Hagl, C.; Teupser, D.; Bauer, A.; et al. Platelet Reactivity and Early Outcomes after Transfemoral Aortic Valve Implantation. Thromb. Haemost. 2018, 118, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Hochholzer, W.; Amann, M.; Titov, A.; Younas, I.; Löffelhardt, N.; Riede, F.; Potocnik, C.; Stratz, C.; Hauschke, D.; Trenk, D.; et al. Randomized Comparison of Different Thienopyridine Loading Strategies in Patients Undergoing Elective Coronary Intervention: The ExcelsiorLOAD Trial. JACC Cardiovasc. Interv. 2016, 9, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized Bleeding Definitions for Cardiovascular Clinical Trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 123, 2736–2747. [Google Scholar] [CrossRef] [Green Version]
- Sibbing, D.; Braun, S.; Morath, T.; Mehilli, J.; Vogt, W.; Schömig, A.; Kastrati, A.; von Beckerath, N. Platelet reactivity after clopidogrel treatment assessed with point-of-care analysis and early drug-eluting stent thrombosis. J. Am. Coll. Cardiol. 2009, 53, 849–856. [Google Scholar] [CrossRef] [Green Version]
- Sibbing, D.; Schulz, S.; Braun, S.; Morath, T.; Stegherr, J.; Mehilli, J.; Schömig, A.; von Beckerath, N.; Kastrati, A. Antiplatelet effects of clopidogrel and bleeding in patients undergoing coronary stent placement. J. Thromb. Haemost. 2010, 8, 250–256. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; Unverdorben, M.; Hengstenberg, C.; Möllmann, H.; Mehran, R.; López-Otero, D.; Nombela-Franco, L.; Moreno, R.; Nordbeck, P.; Thiele, H.; et al. Edoxaban versus Vitamin K Antagonist for Atrial Fibrillation after TAVR. N. Engl. J. Med. 2021, 385, 2150–2160. [Google Scholar] [CrossRef]
- Dangas, G.D.; Tijssen, J.G.; Wöhrle, J.; Sondergaard, L.; Gilard, M.; Möllmann, H.; Makkar, R.R.; Herrmann, H.C.; Giustino, G.; Baldus, S.; et al. A Controlled Trial of Rivaroxaban after Transcatheter Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 120–129. [Google Scholar] [CrossRef]
- Brouwer, J.; Nijenhuis, V.J.; Delewi, R.; Hermanides, R.S.; Holvoet, W.; Dubois, C.L.; Frambach, P.; De Bruyne, B.; Van Houwelingen, G.K.; Van Der Heyden, J.A.; et al. Aspirin with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N. Engl. J. Med. 2020, 383, 1447–1457. [Google Scholar] [CrossRef]
- Stähli, B.; Kasel, M. Optimal Timing of Transcatheter Aortic Valve Implantation and Percutaneous Coronary Intervention—The TAVI PCI Trial; National Library of Medicine: Bethesda, MD, USA, 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04310046 (accessed on 16 May 2022).
- Kobari, Y.; Inohara, T.; Saito, T.; Yoshijima, N.; Tanaka, M.; Tsuruta, H.; Yashima, F.; Shimizu, H.; Fukuda, K.; Naganuma, T.; et al. Aspirin Versus Clopidogrel as Single Antithrombotic Therapy After Transcatheter Aortic Valve Replacement: Insight From the OCEAN-TAVI Registry. Circ. Cardiovasc. Interv. 2021, 14, e010097. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total = 484 | No Bleeding = 285 | Bleeding = 199 | p-Value | ||
|---|---|---|---|---|---|
| Age (years) | 83 [79–86] | 83 [79–86] | 83 [80–86] | 0.938 | |
| Female | 264 (54.5%) | 164 (57.5%) | 100 (50.3%) | 0.113 | |
| Body mass index (kg/m2) | 25.8 [23.5–28.8] | 25.7 [23.1–29.2] | 26.1 [23.6–28.4] | 0.760 | |
| Body mass index (kg/m2) > 30 | 96 (19.8%) | 61 (21.4%) | 35 (17.6%) | 0.300 | |
| Hypertension | 438 (90.5%) | 258 (90.5%) | 180 (90.5%) | 0.978 | |
| Diabetes mellitus type II | 136 (28.1%) | 79 (27.7%) | 57 (28.6%) | 0.079 | |
| History of smoking | 91 (18.8%) | 49 (17.2%) | 42 (21.1%) | 0.717 | |
| History of coronary disease | 345 (71.3%) | 196 (68.8%) | 149 (74.9%) | 0.144 | |
| Previous CABG | 46 (9.5%) | 26 (9.1%) | 20 (10.1%) | 0.705 | |
| Positive family history for CAD | 69 (14.3%) | 42 (14.7%) | 27 (13.6%) | 0.717 | |
| History of pAOD | 56 (11.6%) | 36 (12.6%) | 20 (10.1%) | 0.382 | |
| Creatinine clearance (CKD-EPI; mL/min) | 52.0 [38.0–69.0] | 52.0 [39.0–69.0] | 52.0 [37.1–68.7] | 0.812 | |
| Platelets (103/µL) | 208 [164–255] | 215 [170–256] | 202 [159–251] | 0.104 | |
| STS mortality score | 4.0 [2.7–5.6] | 4.0 [2.7–5.6] | 3.9 [2.7–5.9] | 0.985 | |
| Transapical access route | 2 (0.4%) | 0 (0%) | 2 (1.0%) | 0.169 | |
| Valve type | Balloon-expandable | 318 (65.7%) | 193 (67.7%) | 125 (62.8%) | 0.263 |
| Self-expandable | 166 (34.3%) | 92 (32.3%) | 74 (37.3%) | ||
| Pacemaker after TAVI | 71 (14.7%) | 42 (14.75%) | 29 (14.7%) | 0.665 | |
| On long term ASA | 245 (50.6%) | 146 (51.2%) | 99 (49.7%) | 0.749 | |
| On long term clopidogrel | 120 (24.8%) | 70 (24.6%) | 50 (25.1%) | 0.737 | |
| Indication for oral anticoagulation | 188 (36.8%) | 94 (33.0%) | 94 (47.2%) | 0.001 | |
| BARC 1 | BARC 2 | BARC 3a | BARC 3b | BARC 3c | BARC 5a + b | All | |
|---|---|---|---|---|---|---|---|
| Hematoma (any location) | 20 (69.0%) | 8 (6.8%) | 3 (13.6%) | 1 (4.0%) | - | - | 32 (16.1%) |
| Central/peripheral venosus access | 2 (6.9%) | 25 (21.4%) | - | - | - | - | 27 (13.6%) |
| Puncture site inguinal (surface) | 1 (3.4%) | 43 (36.8%) | 1 (4.5%) | 2 (8.0%) | - | - | 47 (23.6%) |
| Puncture site inguinal (vessel) | - | 12 (10.3%) | 9 (40.9%) | 20 (80.0%) | - | - | 41 (20.6%) |
| Gastrointestinal | - | 2 (1.7%) | 7 (31.8%) | - | - | - | 9 (4.5%) |
| Macrohematuria | - | 10 (8.5%) | 1 (4.5%) | - | - | - | 11 (5.5%) |
| Pericardial tamponade | - | - | - | 1 (4.0%) | - | 3 (75.0%) | 4 (2.0%) |
| Cerebral | - | - | - | - | 2 (100.0%) | - | 2 (1.0%) |
| Epistaxis | 4 (13.8%) | 6 (5.1%) | 1 (4.5%) | - | - | - | 11 (5.5%) |
| PM-pocket | 2 (6.9%) | 6 (5.1) | - | - | - | - | 8 (4.0%) |
| Pulmonary | - | 1 (0.9%) | - | 1 (4.0%) | - | 1 (25.0%) | 3 (1.5%) |
| Others | - | 2 (1.7%) | - | - | - | - | 2 (1.0%) |
| Multiple | - | 2 (1.7%) | - | - | - | - | 2 (1.0%) |
| All | 29 (14.6%) | 117 (58.8%) | 22 (11.1%) | 25 (12.5%) | 2 (1.0%) | 4 (2.0%) | 199 (100%) |
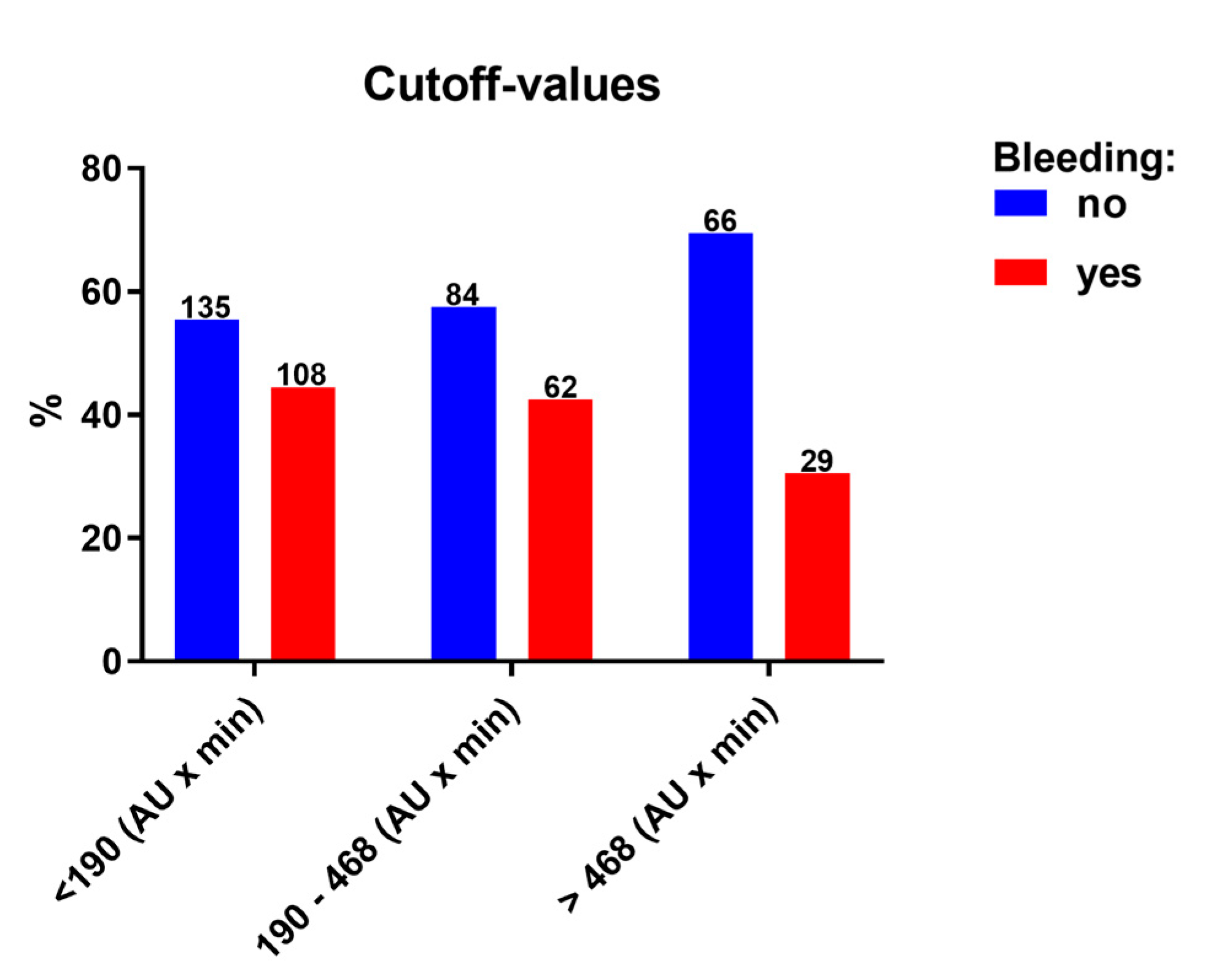
| <190 AU x min | 191–468 AU x min | >468 AU x min | |
|---|---|---|---|
| No bleeding | 135 (55.6%) | 84 (57.5%) | 66 (69.5%) |
| BARC 1 | 17 (7.0%) | 7 (4.8%) | 5 (5.3%) |
| BARC 2 | 64 (26.3%) | 41 (28.1%) | 12 (12.6%) |
| BARC 3a | 10 (4.1%) | 6 (4.1%) | 6 (6.3%) |
| BARC 3b | 13 (5.3%) | 6 (4.1%) | 6 (6.3%) |
| BARC 3c | 1 (0.4%) | 1 (0.7%) | - |
| BARC 5a + b | 3 (1.2%) | 1 (0.7%) | - |
| All | 243 (100%) | 146 (100%) | 95 (100%) |
| Univariate Model | Multivariate Model | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| On ASA platelet reactivity (AU x min) | 1.0 | 0.999–1.001 | 0.806 | |||
| Low/normal/high on—Clopidogrel platelet reactivity | 0.549 | 0.322–0.910 | 0.020 | 0.533 | 0.309–0.917 | 0.023 |
| Oral anticoagulation | 1.837 | 1.265–2.666 | 0.001 | 1.766 | 1.209–2.581 | 0.003 |
| Age (years) | 0.994 | 0.961–1.029 | 0.751 | |||
| Platelet count (103/µL) | 0.998 | 0.995–1.000 | 0.087 | 0.999 | 0.996–1.001 | 0.341 |
| Hemoglobin (g/dL) | 1.038 | 0.933–1.115 | 0.493 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kille, A.; Franke, K.; Corpataux, N.; Hromek, J.; Valina, C.M.; Neumann, F.-J.; Trenk, D.; Nührenberg, T.G.; Hochholzer, W. Impact of On-Clopidogrel Platelet Reactivity on Incidence of Peri-Interventional Bleeding in Patients Undergoing Transcatheter Aortic Valve Implantation. J. Clin. Med. 2022, 11, 2871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102871
Kille A, Franke K, Corpataux N, Hromek J, Valina CM, Neumann F-J, Trenk D, Nührenberg TG, Hochholzer W. Impact of On-Clopidogrel Platelet Reactivity on Incidence of Peri-Interventional Bleeding in Patients Undergoing Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine. 2022; 11(10):2871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102871
Chicago/Turabian StyleKille, Alexander, Kilian Franke, Noé Corpataux, Julia Hromek, Christian M. Valina, Franz-Josef Neumann, Dietmar Trenk, Thomas G. Nührenberg, and Willibald Hochholzer. 2022. "Impact of On-Clopidogrel Platelet Reactivity on Incidence of Peri-Interventional Bleeding in Patients Undergoing Transcatheter Aortic Valve Implantation" Journal of Clinical Medicine 11, no. 10: 2871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102871