
Association between Three Waist Circumference-Related Obesity Metrics and Estimated Glomerular Filtration Rates


Abstract
:1. Introduction
2. Materials and Methods
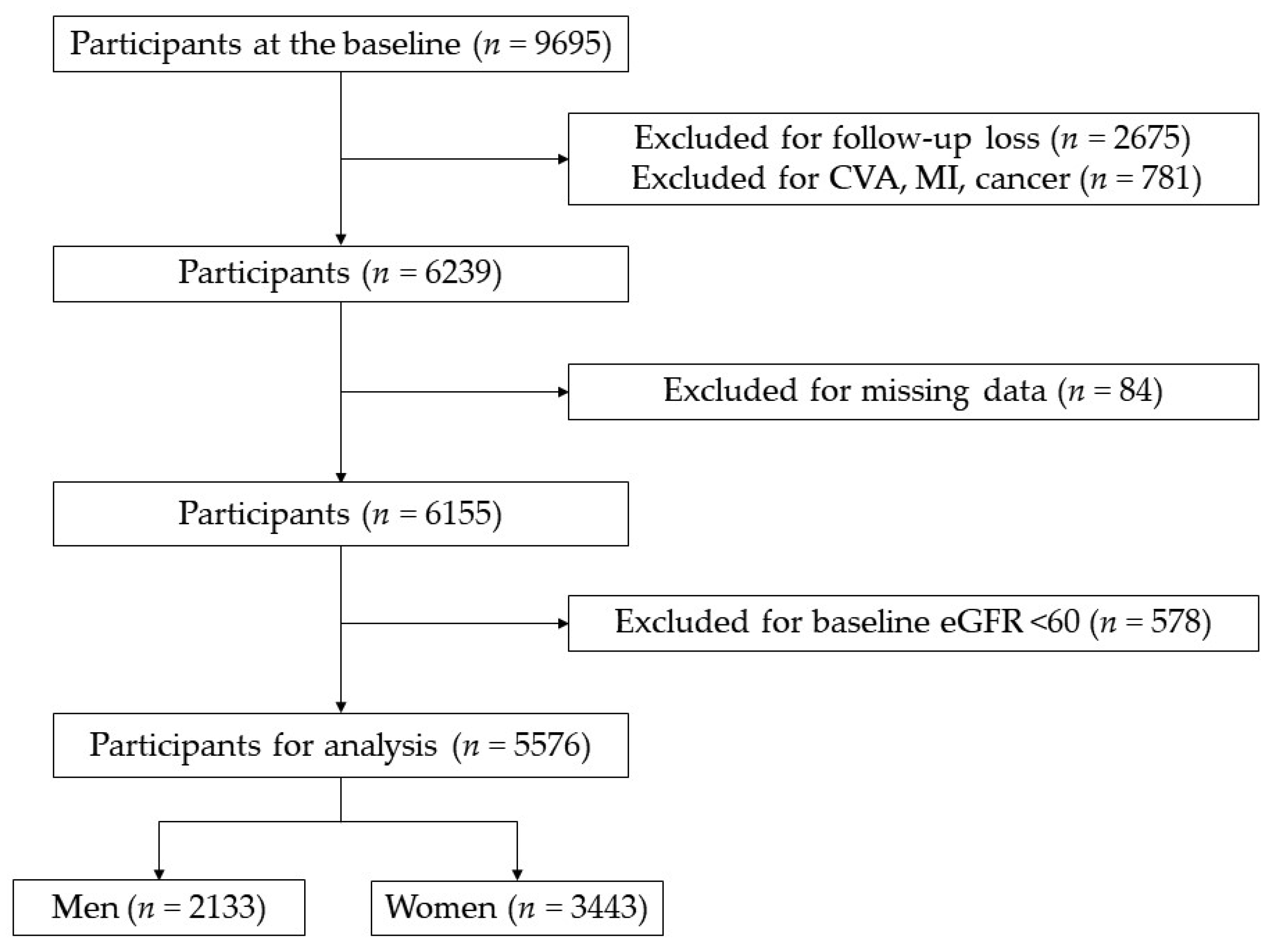
2.1. Study Population
2.2. Data Collection
2.3. Definition of Renal Functions
2.4. Definition of WC-Related Obesity Metrics
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Multi-Rural Communities Cohort
3.2. Multiple Linear Regression of eGFR and Three Obesity Metrics Ratios Compared with the BMI or Residual BMI
3.3. Multiple Linear Regression of eGFR and Quartiles of Three Obesity Metrics Ratios Compared with the BMI or Residual BMI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 16 February 2022).
- Fox, C.S.; Larson, M.G.; Leip, E.P.; Culleton, B.; Wilson, P.W.; Levy, D. Predictors of new-onset kidney disease in a community-based population. J. Am. Med. Assoc. 2004, 291, 844–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Chen, X.; Song, Y.; Caballero, B.; Cheskin, L.J. Association between obesity and kidney disease: A systematic review and meta-analysis. Kidney Int. 2008, 73, 19–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashwell, M.; Gibson, S. Waist-to-height ratio as an indicator of ‘early health risk’: Simpler and more predictive than using a ‘matrix’ based on BMI and waist circumference. BMJ Open 2016, 6, e010159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swainson, M.G.; Batterham, A.M.; Tsakirides, C.; Rutherford, Z.H.; Hind, K. Prediction of whole-body fat percentage and visceral adipose tissue mass from five anthropometric variables. PLoS ONE 2017, 12, e0177175. [Google Scholar] [CrossRef]
- Nevill, A.M.; Duncan, M.J.; Lahart, I.M.; Sandercock, G.R. Scaling waist girth for differences in body size reveals a new improved index associated with cardiometabolic risk. Scand. J. Med. Sci. Sports 2017, 27, 1470–1476. [Google Scholar] [CrossRef]
- Ashwell, M.; Gibson, S. Waist to height ratio is a simple and effective obesity screening tool for cardiovascular risk factors: Analysis of data from the British National Diet and Nutrition Survey of adults aged 19-64 years. Obes. Facts 2009, 2, 97–103. [Google Scholar] [CrossRef]
- Bae, E.H.; Lim, S.Y.; Jung, J.H.; Oh, T.R.; Choi, H.S.; Kim, C.S.; Ma, S.K.; Han, K.D.; Kim, S.W. Obesity, Abdominal Obesity and Chronic Kidney Disease in Young Adults: A Nationwide Population-Based Cohort Study. J. Clin. Med. 2021, 10, 1065. [Google Scholar] [CrossRef]
- Oh, H.; Quan, S.A.; Jeong, J.Y.; Jang, S.N.; Lee, J.E.; Kim, D.H. Waist circumference, not body mass index, is associated with renal function decline in korean population: Hallym aging study. PLoS ONE 2013, 8, e59071. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Wang, Y.; Zhang, W.; Chang, W.; Jin, Y.; Yao, Y. Waist height ratio predicts chronic kidney disease: A systematic review and meta-analysis, 1998-2019. Arch. Public Health 2019, 77, 55. [Google Scholar] [CrossRef] [Green Version]
- Elsayed, E.F.; Tighiouart, H.; Weiner, D.E.; Griffith, J.; Salem, D.; Levey, A.S.; Sarnak, M.J. Waist-to-hip ratio and body mass index as risk factors for cardiovascular events in CKD. Am. J. Kidney Dis. 2008, 52, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Yu, Z.; Grams, M.E.; Ndumele, C.E.; Wagenknecht, L.; Boerwinkle, E.; North, K.E.; Rebholz, C.M.; Giovannucci, E.L.; Coresh, J. Association Between Midlife Obesity and Kidney Function Trajectories: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Kidney Dis. 2021, 77, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Odagiri, K.; Mizuta, I.; Yamamoto, M.; Miyazaki, Y.; Watanabe, H.; Uehara, A. Waist to height ratio is an independent predictor for the incidence of chronic kidney disease. PLoS ONE 2014, 9, e88873. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, H.; Tao, X.; Fan, Y.; Gao, Q.; Yang, J. Optimised anthropometric indices as predictive screening tools for metabolic syndrome in adults: A cross-sectional study. BMJ Open 2021, 11, e043952. [Google Scholar] [CrossRef] [PubMed]
- Kaluzna, M.; Czlapka-Matyasik, M.; Bykowska-Derda, A.; Moczko, J.; Ruchala, M.; Ziemnicka, K. Indirect Predictors of Visceral Adipose Tissue in Women with Polycystic Ovary Syndrome: A Comparison of Methods. Nutrients 2021, 13, 2494. [Google Scholar] [CrossRef]
- Lu, Y.; Liu, S.; Qiao, Y.; Li, G.; Wu, Y.; Ke, C. Waist-to-height ratio, waist circumference, body mass index, waist divided by height(0.5) and the risk of cardiometabolic multimorbidity: A national longitudinal cohort study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2644–2651. [Google Scholar] [CrossRef]
- Vatcheva, K.P.; Lee, M.; McCormick, J.B.; Rahbar, M.H. Multicollinearity in Regression Analyses Conducted in Epidemiologic Studies. Epidemiology 2016, 6, 227. [Google Scholar] [CrossRef] [Green Version]
- Ngueta, G.; Laouan-Sidi, E.A.; Lucas, M. Does waist circumference uncorrelated with BMI add valuable information? J. Epidemiol. Community Health 2014, 68, 849–855. [Google Scholar] [CrossRef]
- Zheng, R.; Li, M.; Xu, M.; Lu, J.; Wang, T.; Dai, M.; Zhang, D.; Chen, Y.; Zhao, Z.; Wang, S.; et al. Chinese Adults Are More Susceptible to Effects of Overall Obesity and Fat Distribution on Cardiometabolic Risk Factors. J. Clin. Endocrinol. Metab. 2021, 106, e2775–e2788. [Google Scholar] [CrossRef]
- Noria, S.F.; Grantcharov, T. Biological effects of bariatric surgery on obesity-related comorbidities. Can. J. Surg. 2013, 56, 47–57. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Han, B.G.; KoGES Group. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Lente, F.V.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.J.; Kim, T.H.; Yoon, S.Y.; Chung, J.H.; Hwang, H.J. Relationship between Stage of Chronic Kidney Disease and Sarcopenia in Korean Aged 40 Years and Older Using the Korea National Health and Nutrition Examination Surveys (KNHANES IV-2, 3, and V-1, 2), 2008-2011. PLoS ONE 2015, 10, e0130740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, C.; Borrelli, S.; Minutolo, R.; Chiodini, P.; De Nicola, L.; Conte, G. A systematic review and meta-analysis suggests obesity predicts onset of chronic kidney disease in the general population. Kidney Int. 2017, 91, 1224–1235. [Google Scholar] [CrossRef]
- Yun, H.R.; Kim, H.W.; Chang, T.I.; Kang, E.W.; Joo, Y.S.; Nam, K.H.; Kim, H.; Park, J.T.; Yoo, T.H.; Kang, S.W.; et al. Increased Risk of Chronic Kidney Disease Associated with Weight Gain in Healthy Adults: Insight From Metabolic Profiles and Body Composition. Front. Med. 2021, 8, 705881. [Google Scholar] [CrossRef]
- Chandramouli, C.; Tay, W.T.; Bamadhaj, N.S.; Tromp, J.; Teng, T.K.; Yap, J.J.L.; MacDonald, M.R.; Hung, C.L.; Streng, K.; Naik, A.; et al. Association of obesity with heart failure outcomes in 11 Asian regions: A cohort study. PLoS Med. 2019, 16, e1002916. [Google Scholar] [CrossRef] [Green Version]
- Tian, L.; Zheng, H.; Li, Y.; Jia, C. Association of waist-to-height ratio with estimated glomerular filtration rate in middle-aged and elderly Chinese. Menopause 2020, 28, 407–412. [Google Scholar] [CrossRef]
- Hwaung, P.; Heo, M.; Kennedy, S.; Hong, S.; Thomas, D.M.; Shepherd, J.; Heymsfield, S.B. Optimum waist circumference-height indices for evaluating adult adiposity: An analytic review. Obes. Rev. 2020, 21, e12947. [Google Scholar] [CrossRef]
- Nevill, A.M.; Stewart, A.D.; Olds, T.; Duncan, M.J. A new waist-to-height ratio predicts abdominal adiposity in adults. Res. Sports Med. 2020, 28, 15–26. [Google Scholar] [CrossRef]
- Manyara, A.M. Optimal cut-offs of five anthropometric indices and their predictive ability of type 2 diabetes in a nationally representative Kenyan study. AIMS Public Health 2021, 8, 507–518. [Google Scholar] [CrossRef]
- Evans, P.D.; McIntyre, N.J.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. Anthropomorphic measurements that include WC-related fat distribution are more closely related with key risk factors than BMI in CKD stage 3. PLoS ONE 2012, 7, e34699. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Wu, B.; Liu, X.; Chen, Y.; Li, Y.; Li, M.; Liang, Y.; Shao, X.; Holthofer, H.; Zou, H. Association of Anthropometric indexes with chronic kidney disease in a Chinese population. Clin. Nephrol. 2013, 80, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.I.; Gao, Y.; Anugu, P.; Anugu, A.; Correa, A. Obesity and overall mortality: Findings from the Jackson Heart Study. BMC Public Health 2021, 21, 50. [Google Scholar] [CrossRef] [PubMed]
- Darko, S.N.; Meeks, K.A.C.; Owiredu, W.; Laing, E.F.; Boateng, D.; Beune, E.; Addo, J.; de-Graft Aikins, A.; Bahendeka, S.; Mockenhaupt, F.; et al. Anthropometric indices and their cut-off points in relation to type 2 diabetes among Ghanaian migrants and non-migrants: The RODAM study. Diabetes Res. Clin. Pract. 2021, 173, 108687. [Google Scholar] [CrossRef]
- O’brien, R.M. A Caution Regarding Rules of Thumb for Variance Inflation Factors. Qual. Quant. 2007, 41, 673–690. [Google Scholar] [CrossRef]
- Ashwell, M.; Gibson, S. A proposal for a primary screening tool: ‘Keep your waist circumference to less than half your height’. BMC Med. 2014, 12, 207. [Google Scholar] [CrossRef] [Green Version]
- Chu, F.L.; Hsu, C.H.; Jeng, C. Low predictability of anthropometric indicators of obesity in metabolic syndrome (MS) risks among elderly women. Arch. Gerontol. Geriatr. 2012, 55, 718–723. [Google Scholar] [CrossRef]
- Kabat, G.C.; Heo, M.; Allison, M.A.; Hou, L.; Nassir, R.; Zaslavsky, O.; Rohan, T.E. Association of anthropometric measures and hemostatic factors in postmenopausal women: A longitudinal study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1120–1127. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Men (n = 2133) | Women (n = 3443) | p-Value |
|---|---|---|---|
| Age (years) | |||
| Mean ± SD | 61.41 ± 8.98 | 59.65 ± 9.14 | <0.001 |
| Age groups, n (%) | <0.001 | ||
| 40–49 | 256 (12.0) | 556 (16.2) | |
| 50–59 | 588 (27.6) | 1082 (31.4) | |
| 60–69 | 869 (40.7) | 1281 (37.2) | |
| 70+ | 420 (19.7) | 524 (15.2) | |
| Educational attainment, n (%) | <0.001 | ||
| Uneducated | 145 (6.8) | 810 (23.5) | |
| Elementary school | 910 (42.7) | 1691 (49.1) | |
| Middle school | 440 (20.6) | 447 (13.0) | |
| High school | 439 (20.6) | 373 (10.8) | |
| College or higher | 199 (9.3) | 122 (3.6) | |
| Tobacco use, n (%) | <0.001 | ||
| Non-smoker | 663 (31.1) | 3314 (96.3) | |
| Ex-smoker | 796 (37.3) | 46 (1.3) | |
| Current smoker | 674 (31.6) | 83 (2.4) | |
| Alcohol consumption, n (%) | <0.001 | ||
| Non-drinker | 482 (22.6) | 2276 (66.1) | |
| Ex-drinker | 216 (10.1) | 93 (2.7) | |
| Current drinker | 1435 (67.3) | 1074 (31.2) | |
| Regular exercise, n (%) | 0.741 | ||
| No | 1481 (69.4) | 2405 (69.9) | |
| Yes | 652 (30.6) | 1038 (30.1) | |
| Obesity metrics | |||
| BMI (kg/m²) | 24.04 ± 2.95 | 24.57 ± 3.16 | <0.001 |
| −22.9 | 803 (37.7) | 1115 (32.4) | <0.001 |
| 23.0–24.9 | 538 (25.2) | 883 (25.7) | |
| 25.0–29.9 | 751 (35.2) | 1261 (36.6) | |
| 30.0+ | 41 (1.9) | 184 (5.3) | |
| Waist circumference (cm) | 85.77 ± 8.28 | 83.46 ± 8.94 | <0.001 |
| Male: ≥90 Female: ≥85 | 673 (31.6) | 1500 (43.6) | |
| Male: ≥95 Female: ≥90 | 290 (13.6) | 807 (23.4) | |
| WHR | 0.92 ± 0.06 | 0.89 ± 0.07 | <0.001 |
| WHtR | 0.52 ± 0.05 | 0.55 ± 0.06 | <0.001 |
| WHt.5R | 0.67 ± 0.06 | 0.68 ± 0.07 | <0.001 |
| eGFR (mL/min/1.73 m²) | 77.98 ± 9.59 | 76.40 ± 9.45 | <0.001 |
| Hypertension | 767 (36.0) | 1235 (35.9) | 0.946 |
| Diabetes mellitus | 288 (13.5) | 311 (9.0) | <0.001 |
| Total cholesterol (mg/dL) | 191.89 ± 34.61 | 204.43 ± 35.86 | <0.001 |
| LDL-C (mg/dL) | 116.02 ± 33.44 | 130.16 ± 32.66 | <0.001 |
| TG (mg/dL) | 160.90 ± 110.43 | 144.03 ± 85.93 | <0.001 |
| HDL-C (mg/dL) | 43.69 ± 11.10 | 45.47 ± 10.03 | <0.001 |
| HS-CRP (mg/L) | 2.11 ± 5.09 | 1.54 ± 3.76 | <0.001 |
| Glucose (mg/dL) | 104.27 ± 28.63 | 97.77 ± 18.76 | <0.001 |
| Creatinine (mg/dL) | 1.04 ± 0.11 | 0.84 ± 0.08 | <0.001 |
| Albumin (g/dL) | 4.46 ± 0.25 | 4.45 ± 0.23 | 0.058 |
| Uric acid (mg/dL) | 5.67 ± 1.41 | 4.27 ± 1.00 | <0.001 |
| Model * | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Coefficient (S.E.) | β | p-Value | VIF | Coefficient (S.E.) | β | p-Value | VIF | |
| Model 1 | ||||||||
| WHR | −8.167 (4.248) | −0.048 | 0.055 | 1.35 | −14.609 (2.527) | −0.106 | 0.000 | 1.17 |
| BMI | −0.157 (0.082) | −0.048 | 0.054 | 1.35 | 0.129 (0.055) | 0.043 | 0.018 | 1.17 |
| Model 2 | ||||||||
| WHtR | −28.155 (6.967) | −0.142 | 0.000 | 2.68 | −30.737 (3.885) | −0.197 | 0.000 | 2.17 |
| BMI | 0.130 (0.115) | 0.040 | 0.259 | 2.68 | 0.440 (0.074) | 0.147 | 0.000 | 2.17 |
| Model 3 | ||||||||
| WHt.5R | −22.238 (5.809) | −0.144 | 0.000 | 3.06 | −23.143 (3.415) | −0.177 | 0.000 | 2.39 |
| BMI | 0.147 (0.123) | 0.045 | 0.229 | 3.06 | 0.412 (0.078) | 0.138 | 0.000 | 2.39 |
| Model 4 | ||||||||
| WHR | 7.809 (4.051) | 0.046 | 0.054 | 1.50 | 6.267 (2.439) | 0.046 | 0.010 | 1.35 |
| BMI | −0.519 (0.082) | −0.160 | 0.000 | 1.66 | −0.118 (0.052) | −0.039 | 0.023 | 1.30 |
| Model 5 | ||||||||
| WHtR | 15.509 (6.923) | 0.078 | 0.025 | 3.21 | 16.528 (4.033) | 0.106 | 0.000 | 2.87 |
| BMI | −0.656 (0.120) | −0.202 | 0.000 | 3.54 | −0.302 (0.075) | −0.101 | 0.000 | 2.69 |
| Model 6 | ||||||||
| WHt.5R | 5.194 (5.604) | 0.034 | 0.354 | 3.45 | 9.941 (3.378) | 0.076 | 0.003 | 2.87 |
| BMI | −0.534 (0.123) | −0.164 | 0.000 | 3.74 | −0.242 (0.076) | −0.081 | 0.002 | 2.79 |
| Model * | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Coefficient (S.E.) | β | p-Value | VIF | Coefficient (S.E.) | β | p-Value | VIF | |
| Model 1 | ||||||||
| WHR | −12.334 (3.658) | −0.073 | 0.001 | 1.00 | −12.328 (2.334) | −0.090 | 0.000 | 1.00 |
| Residual BMI | −0.157 (0.082) | −0.042 | 0.054 | 1.00 | 0.129 (0.055) | 0.040 | 0.018 | 1.00 |
| Model 2 | ||||||||
| WHtR | −21.924 (4.257) | −0.111 | 0.000 | 1.00 | −13.819 (2.638) | −0.089 | 0.000 | 1.00 |
| Residual BMI | 0.130 (0.115) | 0.024 | 0.259 | 1.00 | 0.440 (0.074) | 0.100 | 0.000 | 1.00 |
| Model 3 | ||||||||
| WHt.5R | −16.505 (3.324) | −0.107 | 0.000 | 1.00 | −9.394 (2.211) | −0.072 | 0.000 | 1.00 |
| Residual BMI | 0.147 (0.123) | 0.026 | 0.229 | 1.00 | 0.412 (0.078) | 0.089 | 0.000 | 1.00 |
| Model 4 * | ||||||||
| WHR | −5.933 (3.508) | −0.035 | 0.091 | 1.12 | 4.188 (2.257) | 0.030 | 0.064 | 1.15 |
| Residual BMI | −0.519 (0.082) | −0.137 | 0.000 | 1.23 | −0.118 (0.052) | −0.036 | 0.023 | 1.11 |
| Model 5 * | ||||||||
| WHtR | −16.040 (4.103) | −0.081 | 0.000 | 1.13 | 4.904 (2.600) | 0.031 | 0.059 | 1.19 |
| Residual BMI | −0.656 (0.120) | −0.123 | 0.000 | 1.32 | −0.302 (0.075) | −0.069 | 0.000 | 1.24 |
| Model 6 * | ||||||||
| WHt.5R | −15.554 (3.231) | −0.101 | 0.000 | 1.15 | 1.872 (2.130) | 0.014 | 0.380 | 1.14 |
| Residual BMI | −0.534 (0.123) | −0.094 | 0.000 | 1.23 | −0.242 (0.076) | −0.052 | 0.002 | 1.17 |
| Model * | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Coefficient (S.E.) | β | p-Value | VIF | Coefficient (S.E.) | β | p-Value | VIF | |
| Model 1 | ||||||||
| WHR | ||||||||
| Q2 | −0.205 (0.600) | −0.009 | 0.732 | 1.57 | −0.832 (0.462) | −0.038 | 0.071 | 1.55 |
| Q3 | −1.539 (0.628) | −0.069 | 0.014 | 1.73 | −2.190 (0.475) | −0.100 | 0.000 | 1.65 |
| Q4 | −1.543 (0.665) | −0.070 | 0.021 | 1.94 | −2.370 (0.487) | −0.109 | 0.000 | 1.73 |
| BMI | −0.126 (0.081) | −0.039 | 0.119 | 1.32 | 0.124 (0.055) | 0.041 | 0.024 | 1.17 |
| Model 2 | ||||||||
| WHtR | ||||||||
| Q2 | −1.512 (0.626) | −0.068 | 0.016 | 1.73 | −1.050 (0.475) | −0.048 | 0.027 | 1.65 |
| Q3 | −2.586 (0.706) | −0.117 | 0.000 | 2.20 | −2.671 (0.509) | −0.122 | 0.000 | 1.90 |
| Q4 | −4.311 (0.853) | −0.195 | 0.000 | 3.21 | −4.059 (0.607) | −0.186 | 0.000 | 2.70 |
| BMI | 0.158 (0.104) | 0.049 | 0.129 | 2.23 | 0.334 (0.069) | 0.112 | 0.000 | 1.84 |
| Model 3 | ||||||||
| WHt.5R | ||||||||
| Q2 | −1.765 (0.637) | −0.080 | 0.006 | 1.79 | −0.458 (0.476) | −0.021 | 0.336 | 1.66 |
| Q3 | −2.415 (0.724) | −0.109 | 0.001 | 2.31 | −2.832 (0.518) | −0.130 | 0.000 | 1.97 |
| Q4 | −4.381 (0.907) | −0.198 | 0.000 | 3.62 | −3.454 (0.629) | −0.158 | 0.000 | 2.90 |
| BMI | 0.173 (0.111) | 0.053 | 0.119 | 2.51 | 0.317 (0.071) | 0.106 | 0.000 | 1.99 |
| Model 4 | ||||||||
| WHR | ||||||||
| Q2 | 0.313 (0.547) | 0.014 | 0.567 | 1.59 | 0.508 (0.421) | 0.023 | 0.227 | 1.59 |
| Q3 | −0.213 (0.579) | −0.010 | 0.713 | 1.79 | 0.376 (0.443) | 0.017 | 0.397 | 1.77 |
| Q4 | 0.783 (0.630) | 0.035 | 0.214 | 2.12 | 1.113 (0.464) | 0.051 | 0.016 | 1.93 |
| BMI | −0.475 (0.081) | −0.146 | 0.000 | 1.62 | −0.108 (0.052) | −0.036 | 0.038 | 1.29 |
| Model 5 | ||||||||
| WHtR | ||||||||
| Q2 | 0.291 (0.583) | 0.013 | 0.617 | 1.81 | 0.683 (0.438) | 0.031 | 0.119 | 1.73 |
| Q3 | 0.230 (0.666) | 0.010 | 0.730 | 2.36 | 1.091 (0.488) | 0.050 | 0.025 | 2.14 |
| Q4 | 0.414 (0.831) | 0.019 | 0.618 | 3.68 | 2.033 (0.606) | 0.093 | 0.001 | 3.31 |
| BMI | −0.477 (0.107) | −0.146 | 0.000 | 2.84 | −0.226 (0.067) | −0.076 | 0.001 | 2.17 |
| Model 6 | ||||||||
| WHt.5R | ||||||||
| Q2 | −0.257 (0.591) | −0.012 | 0.664 | 1.86 | 1.110 (0.435) | 0.051 | 0.011 | 1.70 |
| Q3 | −0.056 (0.678) | −0.003 | 0.934 | 2.45 | 0.333 (0.486) | 0.015 | 0.494 | 2.13 |
| Q4 | −0.463 (0.866) | −0.021 | 0.593 | 4.00 | 1.823 (0.609) | 0.084 | 0.003 | 3.35 |
| BMI | −0.401 (0.111) | −0.123 | 0.000 | 3.04 | −0.195 (0.069) | −0.065 | 0.005 | 2.27 |
| Model * | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Coefficient (S.E.) | β | p-Value | VIF | Coefficient (S.E.) | β | p-Value | VIF | |
| Model 1 | ||||||||
| WHR | ||||||||
| Q2 | −0.381 (0.585) | −0.017 | 0.515 | 1.50 | −0.712 (0.454) | −0.033 | 0.117 | 1.51 |
| Q3 | −1.832 (0.586) | −0.083 | 0.002 | 1.50 | −1.979 (0.455) | −0.091 | 0.000 | 1.51 |
| Q4 | −2.009 (0.585) | −0.091 | 0.001 | 1.50 | −1.999 (0.453) | −0.092 | 0.000 | 1.50 |
| Residual BMI | −0.142 (0.082) | −0.038 | 0.082 | 1.00 | 0.145 (0.055) | 0.045 | 0.009 | 1.01 |
| Model 2 | ||||||||
| WHtR | ||||||||
| Q2 | −1.150 (0.583) | −0.052 | 0.049 | 1.50 | −0.334 (0.451) | −0.015 | 0.460 | 1.50 |
| Q3 | −1.980 (0.583) | −0.089 | 0.001 | 1.50 | −1.436 (0.452) | −0.066 | 0.001 | 1.50 |
| Q4 | −3.372 (0.583) | −0.152 | 0.000 | 1.50 | −2.083 (0.452) | −0.095 | 0.000 | 1.50 |
| Residual BMI | 0.138 (0.115) | 0.026 | 0.228 | 1.00 | 0.435 (0.074) | 0.099 | 0.000 | 1.00 |
| Model 3 | ||||||||
| WHt.5R | ||||||||
| Q2 | −1.348 (0.583) | −0.061 | 0.021 | 1.50 | 0.280 (0.452) | 0.013 | 0.536 | 1.50 |
| Q3 | −1.725 (0.583) | −0.078 | 0.003 | 1.50 | −1.607 (0.452) | −0.074 | 0.000 | 1.50 |
| Q4 | −3.315 (0.583) | −0.150 | 0.000 | 1.50 | −1.503 (0.452) | −0.069 | 0.001 | 1.50 |
| Residual BMI | 0.165 (0.123) | 0.029 | 0.179 | 1.00 | 0.411 (0.078) | 0.089 | 0.000 | 1.00 |
| Model 4 | ||||||||
| WHR | ||||||||
| Q2 | −0.352 (0.535) | −0.016 | 0.511 | 1.53 | 0.401 (0.414) | 0.018 | 0.333 | 1.55 |
| Q3 | −1.318 (0.541) | −0.060 | 0.015 | 1.57 | 0.191 (0.426) | 0.009 | 0.654 | 1.63 |
| Q4 | −0.958 (0.556) | −0.043 | 0.085 | 1.65 | 0.796 (0.434) | 0.037 | 0.066 | 1.69 |
| Residual BMI | −0.508 (0.082) | −0.134 | 0.000 | 1.23 | −0.117 (0.052) | −0.036 | 0.025 | 1.11 |
| Model 5 | ||||||||
| WHtR | ||||||||
| Q2 | −0.813 (0.537) | −0.037 | 0.130 | 1.54 | 0.214 (0.413) | 0.010 | 0.605 | 1.54 |
| Q3 | −1.605 (0.544) | −0.072 | 0.003 | 1.58 | 0.294 (0.423) | 0.013 | 0.487 | 1.62 |
| Q4 | −2.389 (0.558) | −0.108 | 0.000 | 1.66 | 0.756 (0.440) | 0.035 | 0.085 | 1.74 |
| Residual BMI | −0.649 (0.119) | −0.122 | 0.000 | 1.32 | −0.301 (0.075) | −0.068 | 0.000 | 1.24 |
| Model 6 | ||||||||
| WHt.5R | ||||||||
| Q2 | −1.224 (0.539) | −0.055 | 0.023 | 1.55 | 0.665 (0.411) | 0.030 | 0.106 | 1.52 |
| Q3 | −1.665 (0.547) | −0.075 | 0.002 | 1.60 | −0.403 (0.419) | −0.018 | 0.336 | 1.58 |
| Q4 | −2.903 (0.561) | −0.131 | 0.000 | 1.68 | 0.650 (0.432) | 0.030 | 0.132 | 1.68 |
| Residual BMI | −0.514 (0.123) | −0.090 | 0.000 | 1.23 | −0.246 (0.076) | −0.053 | 0.001 | 1.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.Y.; Yu, G.I.; Kim, Y.-M.; Kim, M.K.; Shin, M.-H.; Lee, M.-Y. Association between Three Waist Circumference-Related Obesity Metrics and Estimated Glomerular Filtration Rates. J. Clin. Med. 2022, 11, 2876. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102876
Lee DY, Yu GI, Kim Y-M, Kim MK, Shin M-H, Lee M-Y. Association between Three Waist Circumference-Related Obesity Metrics and Estimated Glomerular Filtration Rates. Journal of Clinical Medicine. 2022; 11(10):2876. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102876
Chicago/Turabian StyleLee, Dong Yoon, Gyeong Im Yu, Yu-Mi Kim, Mi Kyung Kim, Min-Ho Shin, and Mi-Young Lee. 2022. "Association between Three Waist Circumference-Related Obesity Metrics and Estimated Glomerular Filtration Rates" Journal of Clinical Medicine 11, no. 10: 2876. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102876