Individual-Level and Neighborhood-Level Factors Associated with Longitudinal Changes in Cardiometabolic Measures in Participants of a Clinic-Based Care Coordination Program: A Secondary Data Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
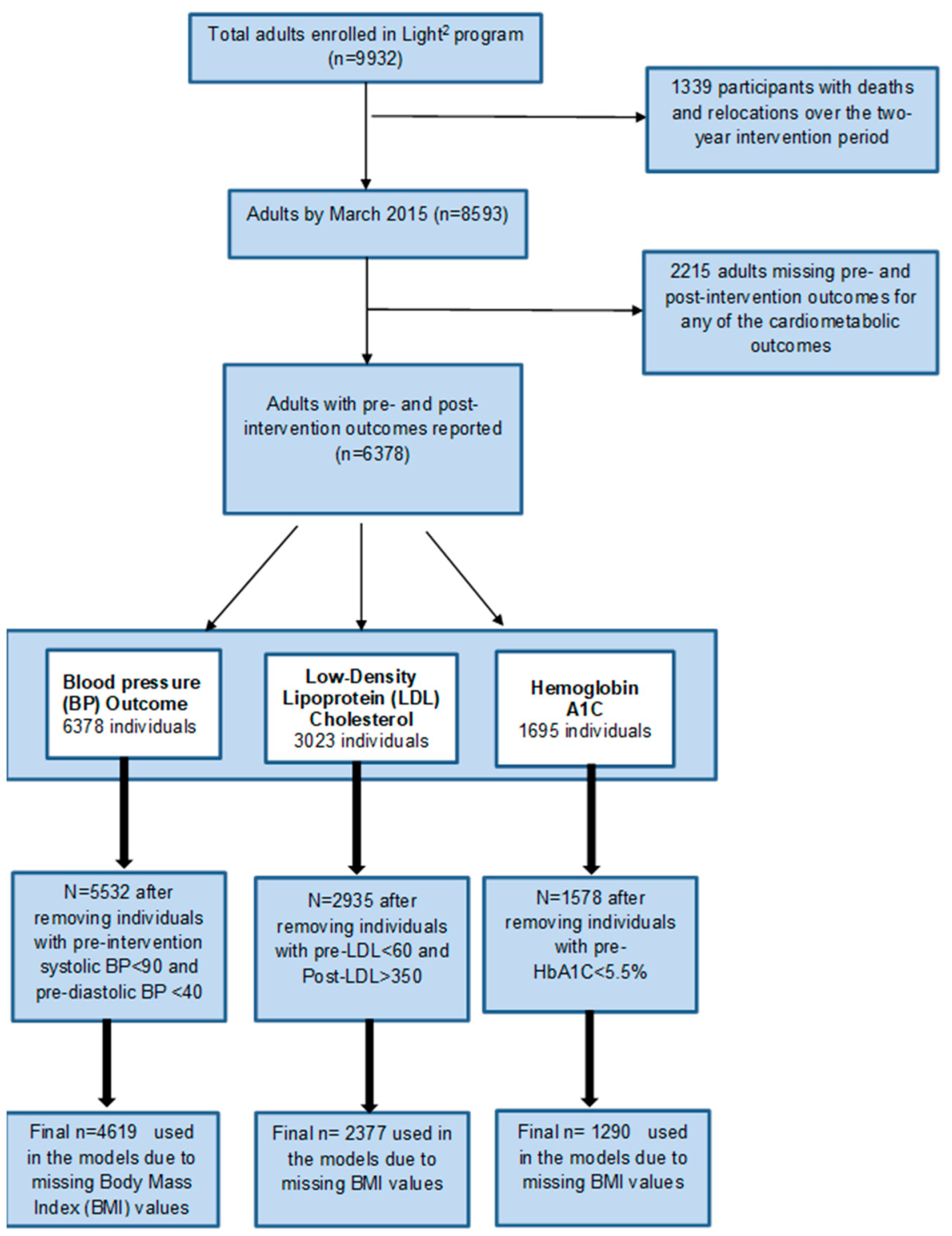
2.2. Participants
2.3. Outcomes
2.4. Variables
2.5. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Center for Health Statistics. With Special Feature on Racial and Ethnic Health Disparities. 2015. Available online: https://pubmed.ncbi.nlm.nih.gov/27308685 (accessed on 1 December 2020).
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart disease and stroke statistics-2018 update: A report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, T.J.; Croft, J.B.; Liu, Y.; Lu, H.; Eke, P.I.; Giles, W.H. Vital signs: Racial disparities in age-specific mortality among Blacks or African Americans—United States, 1999–2015. MMWR Morb. Mortal Wkly. Rep. 2017, 66, 444–456. [Google Scholar] [CrossRef] [PubMed]
- Sterling, M.R.; Echeverría, S.E.; Commodore-Mensah, Y.; Breland, J.Y.; Nunez-Smith, M. Health equity and implementation science in heart, lung, blood, and sleep-related research: Emerging themes from the 2018 Saunders-Watkins Leadership Workshop. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005586. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.S.; Molsberry, R.; Rana, J.S.; Sidney, S.; Capewell, S.; O’Flaherty, M.; Carnethon, M.; Lloyd-Jones, D.M.; Khan, S.S. Heterogeneous trends in burden of heart disease mortality by subtypes in the United States, 1999–2018: Observational analysis of vital statistics. BMJ 2020, 370, m2688. [Google Scholar] [CrossRef]
- Shen, X.; DiMario, S.; Philip, K. Gender disparities in health resource utilization in patients with atherosclerotic cardiovascular disease: A retrospective cross-sectional study. Adv. Ther. 2019, 36, 3424–3434. [Google Scholar] [CrossRef] [Green Version]
- Care Coordination. Available online: https://www.ahrq.gov/professionals/prevention-chronic-care/improve/coordination/index.html (accessed on 30 November 2020).
- Gunderson, J.M.; Wieland, M.L.; Quirindongo-Cedeno, O.; Asiedu, G.B.; Ridgeway, J.L.; O’Brien, M.W.; Nelson, T.M.; Buzard, R.; Campbell, C.; Njeru, J.W. Community health workers as an extension of care coordination in primary care: A community-based cosupervisory model. J. Ambul. Care Manag. 2018, 41, 333–340. [Google Scholar] [CrossRef]
- Engaging Community Health Workers Recommended to Prevent Cardiovascular Disease. Available online: https://www.thecommunityguide.org/content/engaging-community-health-workers-recommended-prevent-cardiovascular-disease (accessed on 10 December 2020).
- Clinical-Community Linkages. Available online: https://www.ahrq.gov/professionals/prevention-chronic-care/improve/community/index.html (accessed on 5 December 2020).
- Mensah, G.A.; Cooper, R.S.; Siega-Riz, A.M.; Cooper, L.A.; Smith, J.D.; Brown, C.H.; Westfall, J.M.; Ofili, E.O.; Price, L.N.; Arteaga, S.; et al. Reducing cardiovascular disparities through community-engaged implementation research: A national heart, lung, and blood institute workshop report. Circ. Res. 2018, 122, 213–230. [Google Scholar] [CrossRef]
- Patil, S.J. Task sharing chronic disease self-management training with lay health coaches to reduce health disparities. Ann. Fam. Med. 2020, 18, 2–3. [Google Scholar] [CrossRef] [Green Version]
- Prasad, K.; Poplau, S.; Brown, R.; Yale, S.; Grossman, E.; Varkey, A.B.; Williams, E.; Neprash, H.; Linzer, M. Time pressure during primary care office visits: A prospective evaluation of data from the Healthy Work Place Study. J. Gen. Intern. Med. 2020, 35, 465–472. [Google Scholar] [CrossRef]
- Kaufman, A.; Dickinson, W.P.; Fagnan, L.J.; Duffy, F.D.; Parchman, M.L.; Rhyne, R.L. The role of health extension in practice transformation and community health improvement: Lessons from 5 case studies. Ann. Fam. Med. 2019, 17 (Suppl. 1), S67–S72. [Google Scholar] [CrossRef]
- Schickedanz, A.; Hamity, C.; Rogers, A.; Sharp, A.L.; Jackson, A. Clinician experiences and attitudes regarding screening for social determinants of health in a large integrated health system. Med. Care 2019, 57 (Suppl. 62), S197–S201. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, E.K.; Dambrun, K.; Cowburn, S.; Mossman, N.; Bunce, A.E.; Marino, M.; Krancari, M.; Gold, R. Variation in Electronic Health Record Documentation of Social Determinants of Health Across a National Network of Community Health Centers. Am. J. Prev. Med. 2019, 57 (Suppl. 1), S65–S73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigmund, C.D.; Carey, R.M.; Appel, L.J.; Arnett, D.K.; Bosworth, H.B.; Cushman, W.C.; Galis, Z.S.; Green Parker, M.; Hall, J.E.; Harrison, D.G.; et al. Report of the National Heart, Lung, and Blood Institute Working Group on Hypertension: Barriers to Translation. Hypertension 2020, 75, 902–917. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.A.; Tan, A.X.; Coyle, C.E.; Ndumele, C.; Rogan, E.; Canavan, M.; Curry, L.A.; Bradley, E.H. Leveraging the social determinants of health: What works? PLoS ONE 2016, 11, e0160217. [Google Scholar] [CrossRef] [PubMed]
- Cantor, M.N.; Chandras, R.; Pulgarin, C. FACETS: Using open data to measure community social determinants of health. J. Am. Med. Inform. Assoc. JAMIA 2018, 25, 419–422. [Google Scholar] [CrossRef]
- Sequist, T.D.; Taveras, E.M. Clinic-community linkages for high-value care. N. Engl. J. Med. 2014, 371, 2148–2150. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, Y.; Sholle, E.; Abedian, S.; Sharko, M.; Turchioe, M.R.; Wu, Y.; Ancker, J.S. Assessing the impact of social determinants of health on predictive models for potentially avoidable 30-day readmission or death. PLoS ONE 2020, 15, e0235064. [Google Scholar] [CrossRef]
- Evaluation of the Health Care Innovation Awards: Community Resource Planning, Prevention, and Monitoring. pp. 231–292. Available online: https://downloads.cms.gov/files/cmmi/hcia-crppm-thirdannrptaddendum.pdf (accessed on 10 May 2022).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Popejoy, L.L.; Jaddoo, J.; Sherman, J.; Howk, C.; Nguyen, R.; Parker, J.C. Monitoring resource utilization in a health care coordination program. Prof. Case Manag. 2015, 20, 310–320. [Google Scholar] [CrossRef]
- Sheets, L.; Popejoy, L.; Aprn, G.B.; Khalilia, M.; Petroski, G.; Parker, J.C. Identifying patients at risk of high healthcare utilization. AMIA Annu. Symp. Proc. 2016, 2016, 1129–1138. [Google Scholar]
- Care Coordination Measures Atlas Update. Available online: https://www.ahrq.gov/professionals/prevention-chronic-care/improve/coordination/atlas2014/index.html (accessed on 30 November 2020).
- Adler, N.E.; Stead, W.W. Patients in Context—EHR Capture of Social and Behavioral Determinants of Health. N. Engl. J. Med. 2015, 372, 698–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuse, N.B.; Koonce, T.Y.; Kusnoor, S.V.; Prather, A.A.; Gottlieb, L.M.; Huang, L.-C.; Phillips, S.E.; Shyr, Y.; Adler, N.E.; Stead, W.W. Institute of Medicine Measures of Social and Behavioral Determinants of Health: A Feasibility Study. Am. J. Prev. Med. 2017, 52, 199–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ESRI. ArcGIS Online World Geocoding Service; Environmental Systems Research Institute: Redlands, CA, USA, 2019. [Google Scholar]
- Infogroup Inc. ReferenceUSA [Dataset]. Available online: http://www.referenceusa.com (accessed on 5 November 2020).
- Low-Income and Low-Supermarket-Access Census Tracts, 2010–2015. Available online: https://www.ers.usda.gov/publications/pub-details/?pubid=82100 (accessed on 8 November 2020).
- 2014 TIGER/Line Shapefiles (Machine-Readable Data Files). Available online: https://www.census.gov/geographies/mapping-files/time-series/geo/tiger-line-file.2014.html (accessed on 2 November 2020).
- Rupasingha, A.; Goetz, S.J.; Freshwater, D. The production of social capital in US counties. J. Socio. Econ. 2006, 35, 83–101. [Google Scholar] [CrossRef]
- Walk Score API Sign Up. Available online: https://www.walkscore.com/professional/api-sign-up.php (accessed on 5 November 2020).
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Maroko, A.R.; Doan, T.M.; Arno, P.S.; Hubel, M.; Yi, S.; Viola, D. Integrating Social Determinants of Health with Treatment and Prevention: A New Tool to Assess Local Area Deprivation. Prev. Chronic Dis. 2016, 13, E128. [Google Scholar] [CrossRef] [Green Version]
- Shortage Designation Application and Review Process. Available online: https://bhw.hrsa.gov/shortage-designation/application-review-process (accessed on 5 December 2020).
- Chen, M.; Tan, X.; Padman, R. Social determinants of health in electronic health records and their impact on analysis and risk prediction: A systematic review. J. Am. Med. Inform. Assoc. 2020, 27, 1764–1773. [Google Scholar] [CrossRef]
- Holcomb, J.; Oliveira, L.C.; Highfield, L.; Hwang, K.O.; Giancardo, L.; Bernstam, E.V. Predicting health-related social needs in Medicaid and Medicare populations using machine learning. Sci. Rep. 2022, 12, 4554. [Google Scholar] [CrossRef]
- Norris, S.L.; Nichols, P.J.; Caspersen, C.J.; Glasgow, R.E.; Engelgau, M.M.; Jack, L.; Isham, G.; Snyder, S.R.; Carande-Kulis, V.G.; Garfield, S.; et al. The effectiveness of disease and case management for people with diabetes. A systematic review. Am. J. Prev. Med. 2002, 22 (Suppl. 4), 15–38. [Google Scholar] [CrossRef]
- Proia, K.K.; Thota, A.B.; Njie, G.J.; Finnie, R.K.; Hopkins, D.P.; Mukhtar, Q.; Pronk, N.P.; Zeigler, D.; Kottke, T.E.; Rask, K.J.; et al. Team-based care and improved blood pressure control: A community guide systematic review. Am. J. Prev. Med. 2014, 47, 86–99. [Google Scholar] [CrossRef] [Green Version]
- Kastner, M.; Cardoso, R.; Lai, Y.; Treister, V.; Hamid, J.S.; Hayden, L.; Wong, G.; Ivers, N.M.; Liu, B.; Marr, S.; et al. Effectiveness of interventions for managing multiple high-burden chronic diseases in older adults: A systematic review and meta-analysis. CMAJ 2018, 190, E1004–E1012. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, J.; Tabish, H.; Welch, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo Pardo, J.; Waters, E.; White, H.; et al. Applying an equity lens to interventions: Using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J. Clin. Epidemiol. 2014, 67, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Iso, H.; Kawachi, I.; Yamagishi, K.; Inoue, M.; Tsugane, S. Living arrangement and coronary heart disease: The JPHC study. Heart 2009, 95, 577–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, A.L.; Magnani, J.W.; Barinas-Mitchell, E.; Matthews, K.A.; Khoudary, S.R.E.; Jackson, E.A.; Brooks, M.M. Social role stress, reward, and the American Heart Association Life 2019 Simple 7 in midlife women: The study of women 2019 health across the nation. J. Am. Heart Assoc. 2020, 9, e017489. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Jou, J.; Upchurch, D.M. Health Care Disparities Among U.S. Women of Reproductive Age by Level of Psychological Distress. J. Womens Health 2019, 28, 1286–1294. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Jou, J.; Upchurch, D.M. Psychological distress and access to care among midlife women. J. Aging Health 2020, 32, 317–327. [Google Scholar] [CrossRef]
- Committee on the Recommended Social and Behavioral Domains and Measures for Electronic Health Records; Board on Population Health and Public Health Practice; Institute of Medicine. Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Healthy People 2030: Social Determinants of Health. Available online: https://health.gov/healthypeople/objectives-and-data/social-determinants-health (accessed on 10 December 2020).
- Tamura, K.; Langerman, S.D.; Ceasar, J.N.; Andrews, M.R.; Agrawal, M.; Powell-Wiley, T.M. Neighborhood Social Environment and Cardiovascular Disease Risk. Curr. Cardiovasc. Risk Rep. 2019, 13, 7. [Google Scholar] [CrossRef]
- Hansen, A.Y.; Umstattd Meyer, M.R.; Lenardson, J.D.; Hartley, D. Built Environments and Active Living in Rural and Remote Areas: A Review of the Literature. Curr. Obes. Rep. 2015, 4, 484–493. [Google Scholar] [CrossRef]
- Cottrell, E.K.; Hendricks, M.; Dambrun, K.; Cowburn, S.; Pantell, M.; Gold, R.; Gottlieb, L.M. Comparison of community-level and patient-level social risk data in a network of community health centers. JAMA Netw. Open. 2020, 3, e2016852. [Google Scholar] [CrossRef]
- Zulman, D.M.; Maciejewski, M.L.; Grubber, J.M.; Weidenbacher, H.J.; Blalock, D.V.; Zullig, L.L.; Greene, L.; Whitson, H.E.; Hastings, S.N.; Smith, V.A. Patient-Reported Social and Behavioral Determinants of Health and Estimated Risk of Hospitalization in High-Risk Veterans Affairs Patients. JAMA Netw. Open 2020, 3, e2021457. [Google Scholar] [CrossRef]
- 2010–2014 American Community Survey 5-year Estimates [Data File]. Available online: https://www2.census.gov/programs-surveys/acs/summary_file/2014/data/5_year_entire_sf/ (accessed on 2 November 2020).
- ESRI. ArcGIS Desktop: Release 10; Environmental Systems Research Institute: Redlands, CA, USA, 2018. [Google Scholar]


{kind=link}
| Variable | Total |
|---|---|
| Demographics | |
| Age (mean, SD) | 62.67 (18.5) |
| Sex (frequency [%]) | |
| Female | 3928 (61.59) |
| Male | 2450 (38.41) |
| Race (frequency [%]) | |
| White non-Hispanic | 5507 (86.34) |
| Other | 871 (13.66) |
| Marital status (frequency [%]) | |
| Married | 2746 (43.05) |
| Other | 892 (13.99) |
| Single | 1622 (25.43) |
| Widowed | 1118 (17.53) |
| Cardiometabolic measures (mean, S.D.) | |
| Pre-intervention LDL (mg/dL) | 106.26 (31.55) |
| Post-intervention LDL (mg/dL) | 99.41 (36.22) |
| Pre-intervention HbA1c (%) | 6.94 (1.43) |
| Post-intervention HbA1c (%) | 7.09 (1.53) |
| Pre-intervention systolic BP (mm of Hg) | 132.74 (14.17) |
| Post-intervention systolic BP (mm of Hg) | 131.14 (17.61) |
| Pre-intervention diastolic BP (mm of Hg) | 75.83 (7.64) |
| Post-intervention diastolic BP (mm of Hg) | 75.05 (9.69) |
| Neighborhood characteristics | |
| Percentage of population below 200% of the FPL (mean, SD) for patient’s census-tract | 36.14 (14.30) |
| Percentage of population that did not graduate from high school for patient’s census-block group (frequency [%]) | |
| Quartile 1: <3.17% | 2049 (32.13) |
| Quartile 2: 3.17–8.79% | 1519 (23.82) |
| Quartile 3: 8.79–14.06% | 1325 (20.77) |
| Quartile 4: >14.06% | 1485 (23.28) |
| Domestic violence injury rates (per 1000) for patient zip codes, 2011–2015 (mean, SD) | 0.39 (0.37) |
| Distance to nearest grocery store from patient’s geocoded address (miles) | 3.42 (3.69) |
| Number of civic or social organizations per capita for patient zip codes (mean, SD) | 13.10 (4.9) |
| Health characteristics | |
| Number of comorbidities | 4.89 (4.23) |
| Pre-intervention body mass index (kg/m2) | 30.35 (7.71) |
| Current smoking (frequency [%]) | |
| Yes | 1455 (22.81) |
| No | 4810 (75.42) |
| Missing | 113 (1.77) |
| High-risk alcohol use (frequency [%]) | |
| Yes | 110 (1.72) |
| Unknown | 6368 (98.28) |
| Presence of mood disorder (frequency [%]) | |
| Yes | 1475 (23.13) |
| Unknown | 4903 (76.87) |
| Total number of nurse care manager contacts during the study period (frequency [%]) | |
| Quartile 1: <5 | 1504 (23.58) |
| Quartile 2: 5–10 | 1489 (23.35) |
| Quartile 3: 11–21 | 1745 (27.36) |
| Quartile 4: >22 | 1640 (25.71) |
| High versus low healthcare resource utilizer (frequency [%]) | |
| High utilizer | 778 (12.2) |
| Low utilizer | 5600 (87.8) |
| Travel time to PCP office from geocoded addresses (frequency [%]) | |
| <=30 min | 4004 (62.78) |
| >30 min | 1331 (20.87) |
| Unknown | 1043 (16.35) |
| Parameter | Adjusted β (95% Confidence Limits) | p-Value |
|---|---|---|
| Intercept | 68.66 (57.87, 79.44) | <0.001 |
| Pre-intervention BMI | −0.19 (−0.35, −0.02) | 0.02 |
| Pre-intervention LDL | 0.56 (0.52, 0.60) | <0.001 |
| Female (ref = male) | 7.76 (5.21, 10.32) | <0.001 |
| Non-White race (ref = White) | −3.43 (−7.24, 0.38) | 0.077 |
| Age | −0.26 (−0.36, −0.17) | <0.001 |
| Number of comorbidities | −0.47 (−0.79, −0.15) | 0.004 |
| Percentage of area population below 200% of the FPL | −0.14 (-0.23, −0.05) | 0.002 |
| Domestic violence injury hospitalization rate (per 1000 population) | −5.78 (−9.24, −2.33) | 0.001 |
| Parameter | Adjusted β (95% Confidence Limits) | p-Value |
|---|---|---|
| Intercept | 3.73 (2.93, 4.53) | <0.001 |
| Pre-intervention HbA1C | 0.51 (0.43, 0.59) | <0.001 |
| Female (ref = male) | −1.29 (−1.95, −0.62) | <0.001 |
| Pre-intervention HbA1C × female sex | 0.19 (0.09, 0.28) | <0.001 |
| Non-White race (ref = White) | −1.16 (−1.94, −0.37) | 0.004 |
| Pre-intervention HbA1C × non-White race | 0.14 (0.03, 0.25) | 0.01 |
| Age | −0.006 (−0.012, −0.00001) | 0.05 |
| Current smoker (ref = No) | ||
| Yes | −0.20 (−0.38, −0.017) | 0.03 |
| Unknown | −0.58 (−1.16, −0003) | 0.05 |
| Civic and social associations rate (per 100,000 population) | 0.01 (−0.0008, 0.026) | 0.06 |
| Distance to nearest grocery store from patient’s geocoded address in miles | 0.01 (−0.007, 0.03) | 0.25 |
| Parameter | Adjusted β (95% Confidence Limits) | p-Value |
|---|---|---|
| Intercept | −3.68 (−19.70, 12.34) | 0.65 |
| Pre-intervention BMI | 0.096 (0.04, 0.15) | <0.001 |
| Pre-intervention SBP | 0.95 (0.83, 1.08) | <0.001 |
| Female (ref = Male) | −7.86 (−15.55, −0.17) | 0.045 |
| Pre-intervention SBP × female sex | 0.06 (0.002, 0.12) | 0.043 |
| Age | 0.38 (0.17, 0.60) | <0.001 |
| Pre-intervention SBP × age | −0.003 (−0.004, −0.0008) | 0.003 |
| Number of comorbidities | 0.10 (0.009, 0.19) | 0.03 |
| Female sex × mood disorder | 1.81 (0.96, 1.9) | 0.058 |
| Percentage of area population below 200% of the FPL | 0.30 (0.18, 0.43) | <0.001 |
| Pre-intervention DBP × Percentage of area population below 200% of the FPL | −0.004 (−005, −0.002) | <0.001 |
| Domestic violence injury hospitalization rate (per 1000) | 2.21 (1.16, 3.26) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patil, S.J.; Golzy, M.; Johnson, A.; Wang, Y.; Parker, J.C.; Saper, R.B.; Haire-Joshu, D.; Mehr, D.R.; Foraker, R.E.; Kruse, R.L. Individual-Level and Neighborhood-Level Factors Associated with Longitudinal Changes in Cardiometabolic Measures in Participants of a Clinic-Based Care Coordination Program: A Secondary Data Analysis. J. Clin. Med. 2022, 11, 2897. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102897
Patil SJ, Golzy M, Johnson A, Wang Y, Parker JC, Saper RB, Haire-Joshu D, Mehr DR, Foraker RE, Kruse RL. Individual-Level and Neighborhood-Level Factors Associated with Longitudinal Changes in Cardiometabolic Measures in Participants of a Clinic-Based Care Coordination Program: A Secondary Data Analysis. Journal of Clinical Medicine. 2022; 11(10):2897. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102897
Chicago/Turabian StylePatil, Sonal J., Mojgan Golzy, Angela Johnson, Yan Wang, Jerry C. Parker, Robert B. Saper, Debra Haire-Joshu, David R. Mehr, Randi E. Foraker, and Robin L. Kruse. 2022. "Individual-Level and Neighborhood-Level Factors Associated with Longitudinal Changes in Cardiometabolic Measures in Participants of a Clinic-Based Care Coordination Program: A Secondary Data Analysis" Journal of Clinical Medicine 11, no. 10: 2897. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102897