
Callosal Angle Sub-Score of the Radscale in Patients with Idiopathic Normal Pressure Hydrocephalus Is Associated with Positive Tap Test Response

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Issues
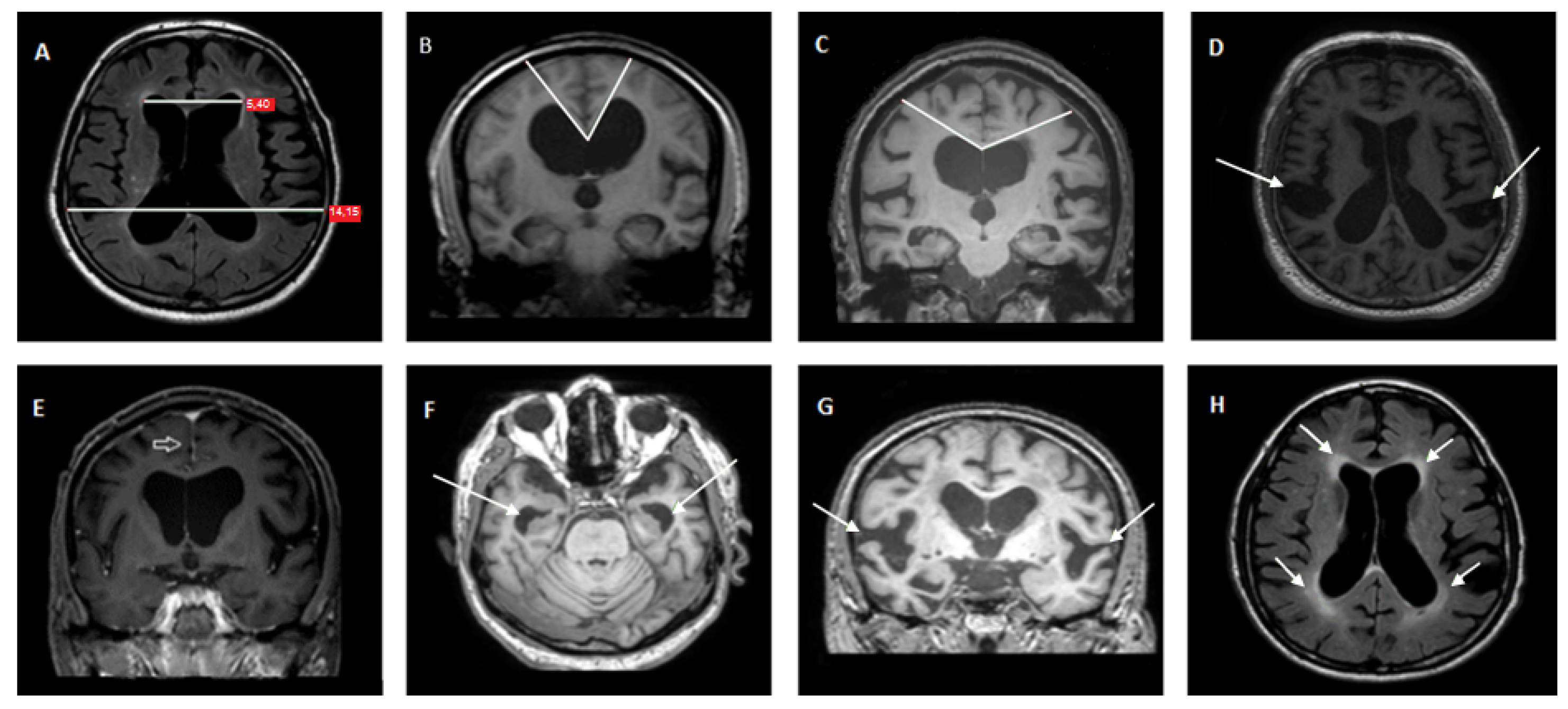
2.3. Magnetic Resonance Imaging
2.4. Clinical and Neuropsychological Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leinonen, V.; Vanninen, R.; Rauramaa, T. Cerebrospinal fluid circulation and hydrocephalus. Handb. Clin. Neurol. 2017, 145, 39–50. [Google Scholar] [PubMed]
- Oliveira, L.M.; Nitrini, R.; Roman, G.C. Normal-pressure hydrocephalus: A critical review. Dement. Neuropsychol. 2019, 13, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Skalicky, P.; Mladek, A.; Valsad, A.; De Lacy, P.; Benes, V.; Bradac, O. Normal pressure hydrocephalus-an overview of pathophysiological mechanisms and diagnostic procedures. Neurosurg. Rev. 2020, 43, 1451–1464. [Google Scholar] [CrossRef]
- Adams, R.D.; Fisher, C.M.; Hakim, S.; Ojemann, R.G.; Sweet, W.H. Symptomatic Occult Hydrocephalus with “Normal” Cerebrospinal-Fluid Pressure. A Treatable Syndrome. N. Engl. J. Med. 1965, 273, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Hakim, S.; Adams, R.D. The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure. Observations on cerebrospinal fluid hydrodynamics. J. Neurol. Sci. 1965, 2, 307–327. [Google Scholar] [CrossRef]
- Zaccaria, V.; Bacigalupo, I.; Gervasi, G.; Canevelli, M.; Corbo, M.; Vanacore, N.; Lacorte, E. A systematic review on the epidemiology of normal pressure hydrocephalus. Acta Neurol. Scand. 2020, 141, 101–114. [Google Scholar] [CrossRef]
- Toma, A.K.; Papadopoulos, M.C.; Stapleton, S.; Kitchen, N.D.; Watkins, L.D. Systematic review of the outcome of shunt surgery in idiopathic normal-pressure hydrocephalus. Acta Neurochir. 2013, 155, 1977–1980. [Google Scholar] [CrossRef]
- Shaw, R.; Mahant, N.; Jacobson, E.; Owler, B. A Review of Clinical Outcomes for Gait and Other Variables in the Surgical Treatment of Idiopathic Normal Pressure Hydrocephalus. Mov. Disord. Clin. Pract. 2016, 3, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Mihalj, M.; Dolic, K.; Kolic, K.; Ledenko, V. CSF tap test—Obsolete or appropriate test for predicting shunt responsiveness? A systemic review. J. Neurol. Sci. 2016, 362, 78–84. [Google Scholar] [CrossRef]
- Relkin, N.; Marmarou, A.; Klinge, P.; Bergsneider, M.; Black, P.M. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery 2005, 57, S4–S16, discussion ii–v. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, M.; Yamada, S.; Miyajima, M.; Ishii, K.; Kuriyama, N.; Kazui, H.; Kanemoto, H.; Suehiro, T.; Yoshiyama, K.; Kameda, M.; et al. Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (Third Edition): Endorsed by the Japanese Society of Normal Pressure Hydrocephalus. Neurol. Med. Chir. 2021, 61, 63–97. [Google Scholar] [CrossRef] [PubMed]
- Onder, H.; Goksungur, G. The Utility of Neuroimaging Parameters in Discriminating Patients of Normal-Pressure Hydrocephalus with Positive Cerebrospinal Fluid Tap Test Response from Healthy Controls. Ann. Indian Acad. Neurol. 2020, 23, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Kockum, K.; Larsson, E.-M.; Lilja-Lund, O.; Rosell, M.; Söderström, L.; Virhammar, J.; Laurell, K. The NPH radscale; a new radiological scale for evaluation of suspected normal pressure hydrocephalus. Fluids Barriers CNS 2015, 12, P27. [Google Scholar] [CrossRef] [Green Version]
- Kockum, K.; Lilja-Lund, O.; Larsson, E.M.; Rosell, M.; Soderstrom, L.; Virhammar, J.; Laurell, K. The idiopathic normal-pressure hydrocephalus Radscale: A radiological scale for structured evaluation. Eur. J. Neurol. 2018, 25, 569–576. [Google Scholar] [CrossRef]
- Kockum, K.; Virhammar, J.; Riklund, K.; Soderstrom, L.; Larsson, E.M.; Laurell, K. Standardized image evaluation in patients with idiopathic normal pressure hydrocephalus: Consistency and reproducibility. Neuroradiology 2019, 61, 1397–1406. [Google Scholar] [CrossRef] [Green Version]
- Bradley, W.G., Jr. CSF Flow in the Brain in the Context of Normal Pressure Hydrocephalus. Am. J. Neuroradiol. 2015, 36, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Kubo, Y.; Kazui, H.; Yoshida, T.; Kito, Y.; Kimura, N.; Tokunaga, H.; Ogino, A.; Miyake, H.; Ishikawa, M.; Takeda, M. Validation of grading scale for evaluating symptoms of idiopathic normal-pressure hydrocephalus. Dement. Geriatr. Cogn. Disord. 2008, 25, 37–45. [Google Scholar] [CrossRef]
- Schniepp, R.; Trabold, R.; Romagna, A.; Akrami, F.; Hesselbarth, K.; Wuehr, M.; Peraud, A.; Brandt, T.; Dieterich, M.; Jahn, K. Walking assessment after lumbar puncture in normal-pressure hydrocephalus: A delayed improvement over 3 days. J. Neurosurg. 2017, 126, 148–157. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal Assessment Battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Dubois, B.; Touchon, J.; Portet, F.; Ousset, P.J.; Vellas, B.; Michel, B. “The 5 words”: A simple and sensitive test for the diagnosis of Alzheimer’s disease. Presse Med. 2002, 31, 1696–1699. [Google Scholar] [PubMed]
- Royall, D.R.; Cordes, J.A.; Polk, M. CLOX: An executive clock drawing task. J. Neurol. Neurosurg. Psychiatry 1998, 64, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Mori, E.; Ishikawa, M.; Kato, T.; Kazui, H.; Miyake, H.; Miyajima, M.; Nakajima, M.; Hashimoto, M.; Kuriyama, N.; Tokuda, T.; et al. Guidelines for management of idiopathic normal pressure hydrocephalus: Second edition. Neurol. Med. Chir. 2012, 52, 775–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damasceno, B.P. Neuroimaging in normal pressure hydrocephalus. Dement. Neuropsychol. 2015, 9, 350–355. [Google Scholar] [CrossRef]
- Zhou, X.; Xia, J. Application of Evans Index in Normal Pressure Hydrocephalus Patients: A Mini Review. Front. Aging Neurosci. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Ju, H.; Im, K.; Kwon, K.Y. Revisiting the diagnostic value of Evans’ index: Lessons from an unusual case of normal pressure hydrocephalus with Evans’ index less than 0.3. Neurol. Sci. 2019, 40, 2637–2639. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Andrews, A.W.; Thomas, M.W. Walking speed: Reference values and correlates for older adults. J. Orthop. Sports Phys. Ther. 1996, 24, 86–90. [Google Scholar] [CrossRef]
- Rossier, P.; Wade, D.T. Validity and reliability comparison of 4 mobility measures in patients presenting with neurologic impairment. Arch. Phys. Med. Rehabil. 2001, 82, 9–13. [Google Scholar] [CrossRef]
- Ishikawa, M.; Hashimoto, M.; Mori, E.; Kuwana, N.; Kazui, H. The value of the cerebrospinal fluid tap test for predicting shunt effectiveness in idiopathic normal pressure hydrocephalus. Fluids Barriers CNS 2012, 9, 1. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, M.; Yamada, S.; Yamamoto, K. Early and delayed assessments of quantitative gait measures to improve the tap test as a predictor of shunt effectiveness in idiopathic normal pressure hydrocephalus. Fluids Barriers CNS 2016, 13, 20. [Google Scholar] [CrossRef] [Green Version]
- Laticevschi, T.; Lingenberg, A.; Armand, S.; Griffa, A.; Assal, F.; Allali, G. Can the radiological scale "iNPH Radscale" predict tap test response in idiopathic normal pressure hydrocephalus? J. Neurol. Sci. 2021, 420, 117239. [Google Scholar] [CrossRef] [PubMed]
- Ko, P.W.; Lee, H.W.; Kang, K. Frontal Assessment Battery and Cerebrospinal Fluid Tap Test in Idiopathic Normal-Pressure Hydrocephalus. Eur. Neurol. 2017, 77, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.; Elster, J.; Eckert, I.; Wiefek, J.; Paulus, W.; von Steinbuechel, N.; Abatih, E.N.; Blocher, J. Cognitive functions after spinal tap in patients with normal pressure hydrocephalus. J. Neurol. 2014, 261, 2344–2350. [Google Scholar] [CrossRef] [PubMed]
- Solana, E.; Poca, M.A.; Sahuquillo, J.; Benejam, B.; Junque, C.; Dronavalli, M. Cognitive and motor improvement after retesting in normal-pressure hydrocephalus: A real change or merely a learning effect? J. Neurosurg. 2010, 112, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Lotan, E.; Damadian, B.E.; Rusinek, H.; Griffin, M.; Ades-Aron, B.; Lu, N.; Golomb, J.; George, A.E. Quantitative imaging features predict spinal tap response in normal pressure hydrocephalus. Neuroradiology 2021, 64, 473–483. [Google Scholar] [CrossRef]
- Ammar, A.; Abbas, F.; Al Issawi, W.; Fakhro, F.; Batarfi, L.; Hendam, A.; Hasen, M.; El Shawarby, M.; Al Jehani, H. Idiopathic Normal-Pressure Hydrocephalus Syndrome: Is It Understood? The Comprehensive Idiopathic Normal-Pressure Hydrocephalus Theory (CiNPHT). In Hydrocephalus: What Do We Know? And What Do We Still Not Know? Ammar, A., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 67–82. [Google Scholar]
- Liu, J.; Guo, Y.; Zhang, C.; Zeng, Y.; Luo, Y.; Wang, G. Clearance Systems in the Brain, From Structure to Function. Front. Cell. Neurosci. 2022, 15, 729706. [Google Scholar] [CrossRef]
- Wang, C.; Wang, X.; Tan, C.; Wang, Y.; Tang, Z.; Zhang, Z.; Liu, J.; Xiao, G. Novel therapeutics for hydrocephalus: Insights from animal models. CNS Neurosci. Ther. 2021, 27, 1012–1022. [Google Scholar] [CrossRef]
- Benson, D.F.; LeMay, M.; Patten, D.H.; Rubens, A.B. Diagnosis of Normal-Pressure Hydrocephalus. N. Engl. J. Med. 1970, 283, 609–615. [Google Scholar] [CrossRef]
- Capone, P.M.; Bertelson, J.A.; Ajtai, B. Neuroimaging of Normal Pressure Hydrocephalus and Hydrocephalus. Neurol. Clin. 2020, 38, 171–183. [Google Scholar] [CrossRef]
- Korbecki, A.; Zimny, A.; Podgorski, P.; Sasiadek, M.; Bladowska, J. Imaging of cerebrospinal fluid flow: Fundamentals, techniques, and clinical applications of phase-contrast magnetic resonance imaging. Pol. J. Radiology 2019, 84, e240–e250. [Google Scholar] [CrossRef]
- Ferrari, A.; Milletti, D.; Giannini, G.; Cevoli, S.; Oppi, F.; Palandri, G.; Albini-Riccioli, L.; Mantovani, P.; Anderlucci, L.; Cortelli, P.; et al. The effects of cerebrospinal fluid tap-test on idiopathic normal pressure hydrocephalus: An inertial sensors based assessment. J. Neuroeng. Rehabil. 2020, 17, 7. [Google Scholar] [CrossRef] [PubMed]
- Wolfsegger, T.; Hauser, A.; Wimmer, S.; Neuwirth, K.; Assar, H.; Topakian, R. A comprehensive clinico-radiological, neuropsychological and biomechanical analysis approach to patients with idiopathic normal pressure hydrocephalus. Clin. Neurol. Neurosurg. 2021, 201, 106402. [Google Scholar] [CrossRef] [PubMed]
- Marmarou, A.; Bergsneider, M.; Klinge, P.; Relkin, N.; Black, P.M. The value of supplemental prognostic tests for the preoperative assessment of idiopathic normal-pressure hydrocephalus. Neurosurgery 2005, 57, S17–S28. [Google Scholar] [CrossRef] [PubMed]
- Wikkelsö, C.; Andersson, H.; Blomstrand, C.; Lindqvist, G.; Svendsen, P. Normal pressure hydrocephalus. Predictive value of the cerebrospinal fluid tap-test. Acta Neurol. Scand. 1986, 73, 566–573. [Google Scholar] [CrossRef]
- Sahuquillo, J.; Poca, M.A. To Shunt or Not to Shunt Patients with Idiopathic Normal Pressure Hydrocephalus? A Reappraisal of an Old Question. J. Clin. Med. 2020, 9, 4120. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 45 | Neuropsychological | Gait | ||||||
|---|---|---|---|---|---|---|---|---|
| MMSE | FAB | 5WT Immediate | 5WT Delayed | CLOX-1 | CLOX-2 | 10 m Timed Walk Test: Steps | 10 m Timed Walk Test: Time | |
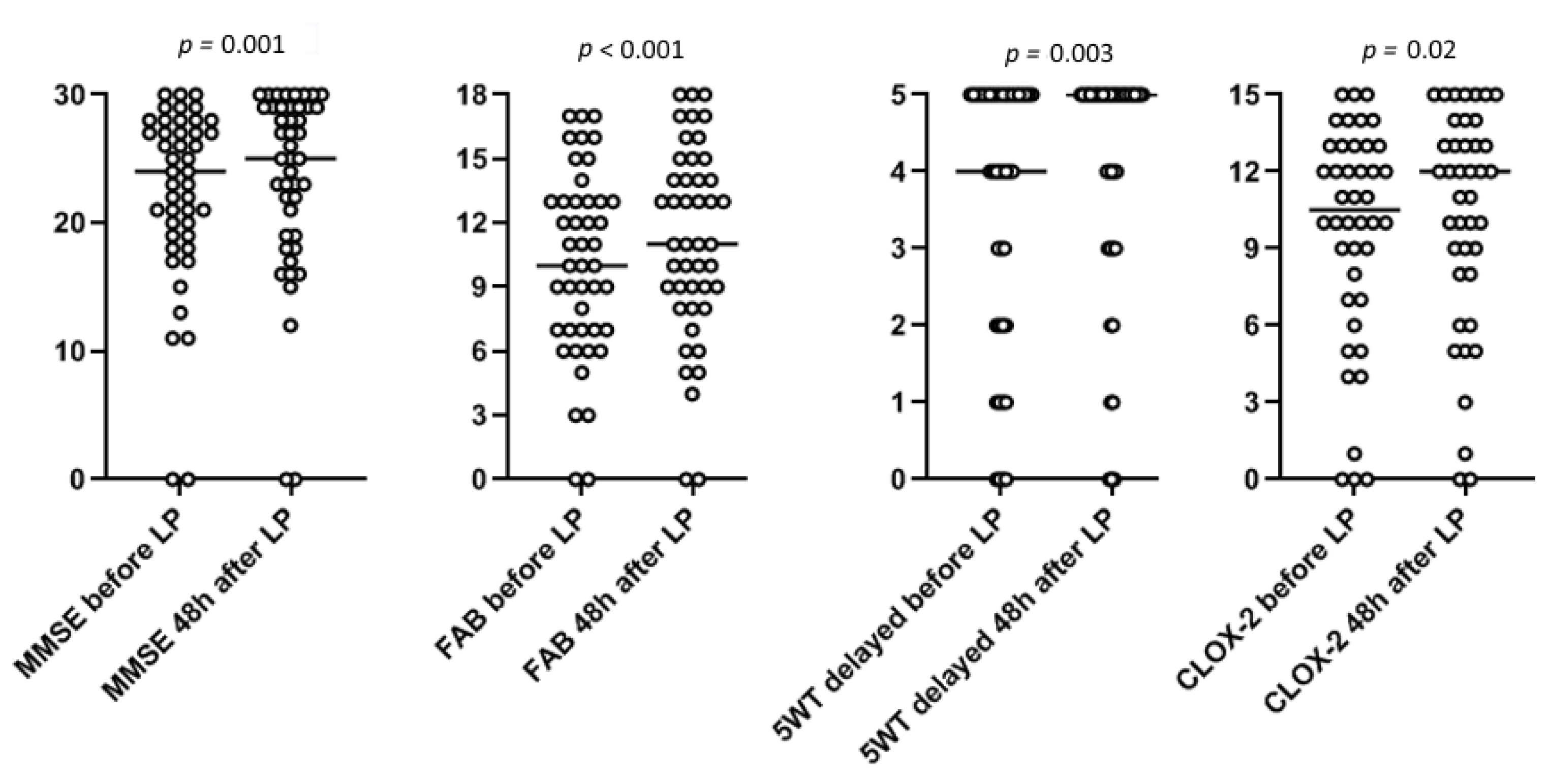
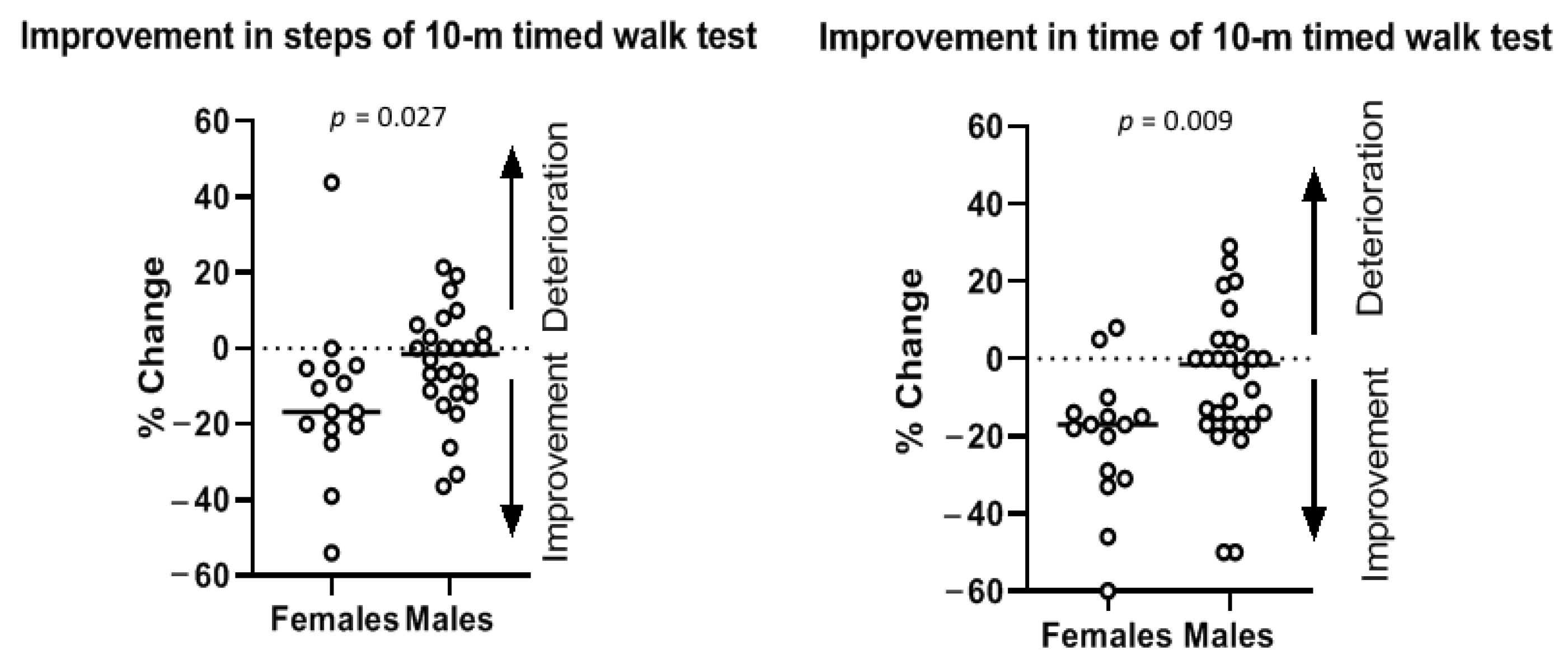
| Before LP | 24 (19–27.5) | 10 (7–13) | 5 (5–5) | 4 (2–5) | 8 (5–11) | 10.5 (7–13) | 22 (17–30.5) | 12 (9.75–19.5) |
| 48 h after LP | 25 (19–29) | 11 (8.5–14.5) | 5 (4.75–5) | 5 (3–5) | 9 (5.5–12) | 12 (8–13.5) | 20 (17–29.5) | 11.50 (8.25–18.5) |
| Median % change | 0.042 | 0.125 | 0.007 | 0.073 | 0.022 | 0.057 | −0.067 | −0.136 |
| p | 0.001 † | 0.000 † | NS † | 0.003 † | NS † | 0.020 † | 0.004 † | 0.004 † |
| Variable | Tap Test Responders N = 19 | Tap Test Non-Responders N = 26 | p |
|---|---|---|---|
| Gender (F/M) | 10/9 | 7/19 | 0.079 † |
| Age | 76 (71–79) | 74 (69.8–78) | 0.526 ‡ |
| Grading scale | 6 (5–7) | 6 (4–7) | 0.870 ‡ |
| Disease duration (months) | 36 (24–60) | 24 (12–48) | 0.225 ‡ |
| Peak flow velocity | 8.2 (5.7–10.6) | 6.8 (4.6–11.9) | 0.589 ‡ |
| Absolute stroke volume | 0.14 (0.11–0.32) | 0.11 (0.05–0.36) | 0.352 ‡ |
| Evan’s index | 2 (2–2) | 2 (2–2) | 0.169 ‡ |
| Narrow sulci | 1 (0–1) | 1 (0–1) | 0.214 ‡ |
| Sylvian fissures | 1 (0–1) | 1 (1–1) | 0.577 ‡ |
| Focally enlarged sulci | 0 (0–1) | 0 (0–1) | 0.202 ‡ |
| Temporal horns | 2 (2–2) | 2 (1–2) | 0.646 ‡ |
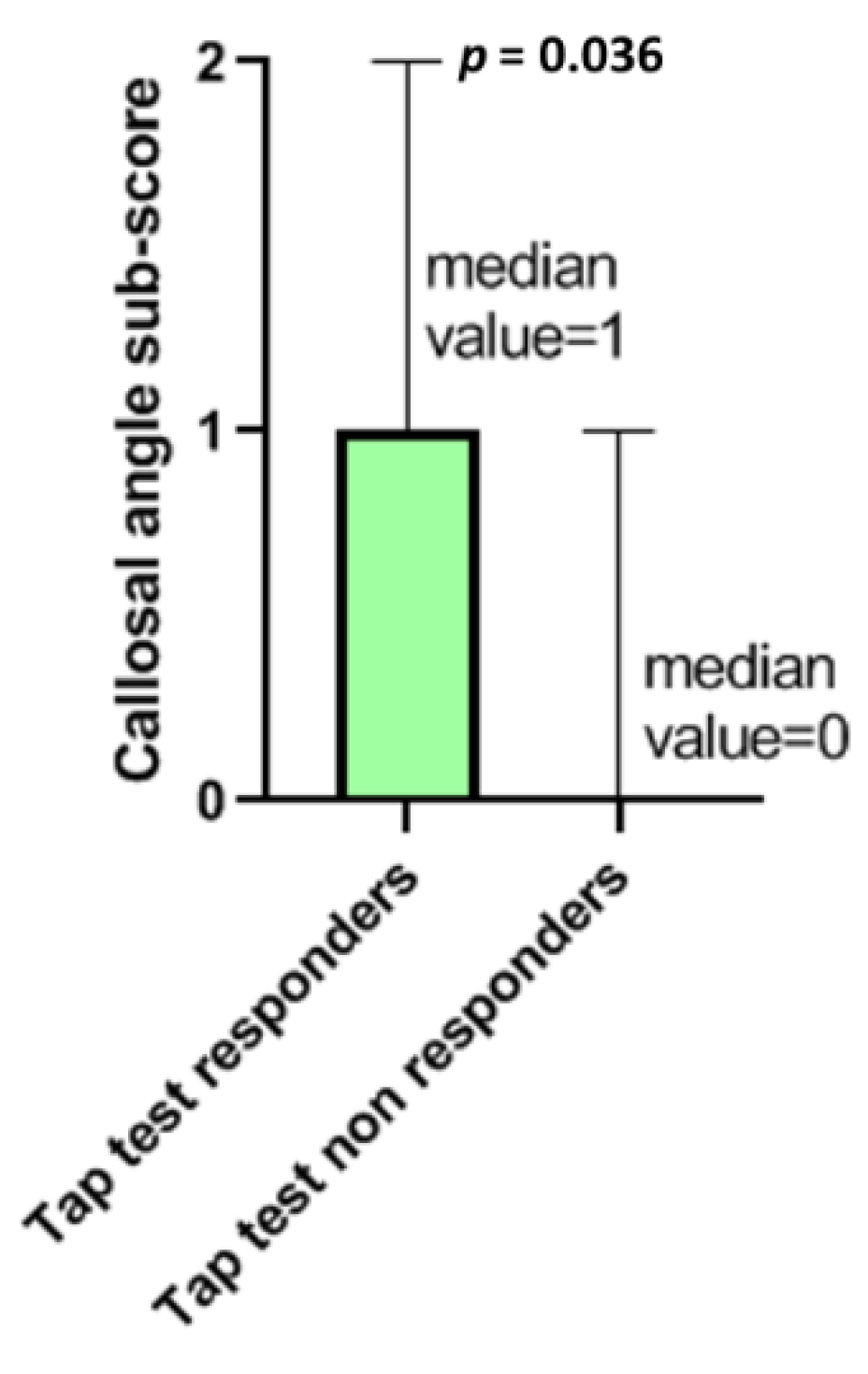
| Callosal angle | 1 (0–1) | 0 (0–0.25) | 0.036 ‡ * |
| Periventricular hyperintensity | 2 (1–2) | 2 (1–2) | 0.522 ‡ |
| Radscale total score | 8 (7–9) | 7 (7–8) | 0.249 ‡ |
| N = 19 | Neuropsychological | Gait | ||||||
|---|---|---|---|---|---|---|---|---|
| MMSE | FAB | 5WT Immediate | 5WT Delayed | CLOX-1 | CLOX-2 | 10 m Timed Walk Test: Steps | 10 m Timed Walk Test: Time | |
| Before LP | 21 (20–26) | 9 (7–12) | 5 (5–5) | 4,5 (3–5) | 7 (6–10) | 10 (6.75–13) | 25 (20–42) | 13 (11–24) |
| 48 h after LP | 23 (21–28) | 10 (9–13) | 5 (5–5) | 5 (4–5) | 7,5 (5 -10.25) | 11 (5.75–14) | 21 (17–30) | 12 (9–20) |
| Median % change | 0.08 | 0.166 | 0.000 | 0.000 | 0.000 | 0.074 | 0.172 | 0.181 |
| p | 0.005 † | 0.001 † | NS † | NS † | NS † | NS † | 0.001 † | 0.005 † |
| N = 26 | Neuropsychological | Gait | ||||||
|---|---|---|---|---|---|---|---|---|
| MMSE | FAB | 5WT Immediate | 5WT Delayed | CLOX-1 | CLOX-2 | 10 m Timed Walk Test: Steps | 10 m Timed Walk Test: Time | |
| Before LP | 25.5 (18.75–28) | 11.5 (6.75–15) | 5 (4–5) | 4 (1–5) | 9 (4–12.75) | 11 (7.5–13) | 19 (16–29.25) | 10.75 (9–16.25) |
| 48 h after LP | 27 (17.5–29) | 13 (7.75–15.25) | 5 (4–5) | 5 (2–5) | 10 (6–14) | 12 (9–13) | 19 (15.75–28.5) | 10.25 (7.5–18.25) |
| Median % change | 0.0345 | 0.068 | 0.000 | 0.000 | 0.000 | 0.000 | 0.015 | 0.057 |
| p | 0.012 † | NS † | NS † | NS † | NS † | NS † | NS † | NS † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyrgelis, E.-S.; Paraskevas, G.P.; Constantinides, V.C.; Boufidou, F.; Velonakis, G.; Stefanis, L.; Kapaki, E. Callosal Angle Sub-Score of the Radscale in Patients with Idiopathic Normal Pressure Hydrocephalus Is Associated with Positive Tap Test Response. J. Clin. Med. 2022, 11, 2898. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102898
Pyrgelis E-S, Paraskevas GP, Constantinides VC, Boufidou F, Velonakis G, Stefanis L, Kapaki E. Callosal Angle Sub-Score of the Radscale in Patients with Idiopathic Normal Pressure Hydrocephalus Is Associated with Positive Tap Test Response. Journal of Clinical Medicine. 2022; 11(10):2898. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102898
Chicago/Turabian StylePyrgelis, Efstratios-Stylianos, George P. Paraskevas, Vasilios C. Constantinides, Fotini Boufidou, Georgios Velonakis, Leonidas Stefanis, and Elisabeth Kapaki. 2022. "Callosal Angle Sub-Score of the Radscale in Patients with Idiopathic Normal Pressure Hydrocephalus Is Associated with Positive Tap Test Response" Journal of Clinical Medicine 11, no. 10: 2898. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102898