
An Intervention of 12 Weeks of Nordic Walking and Recreational Walking to Improve Cardiorespiratory Capacity and Fitness in Older Adult Women


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Anthropometric Measurement Variables
2.1.2. Cardiorespiratory Fitness
2.1.3. Heart Rate (HR)
2.1.4. Patient and Public Involvement
2.1.5. Statistical Analysis
3. Results
3.1. Comparison of the Participant Groups (Control, RW, and NW) Relative to Anthropometric Measurement Variables, HR Variables, UKK Test Measurements, and VO2max
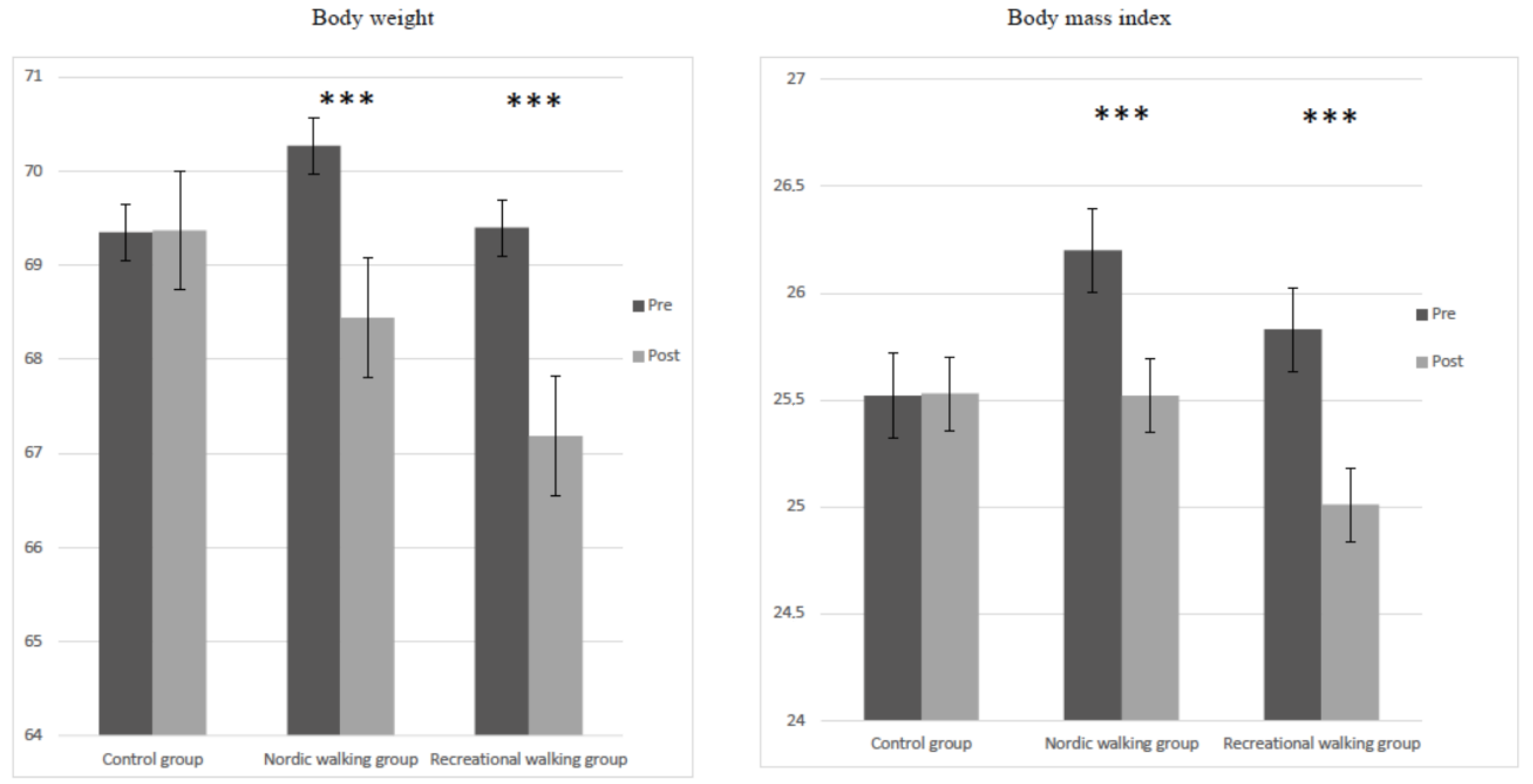
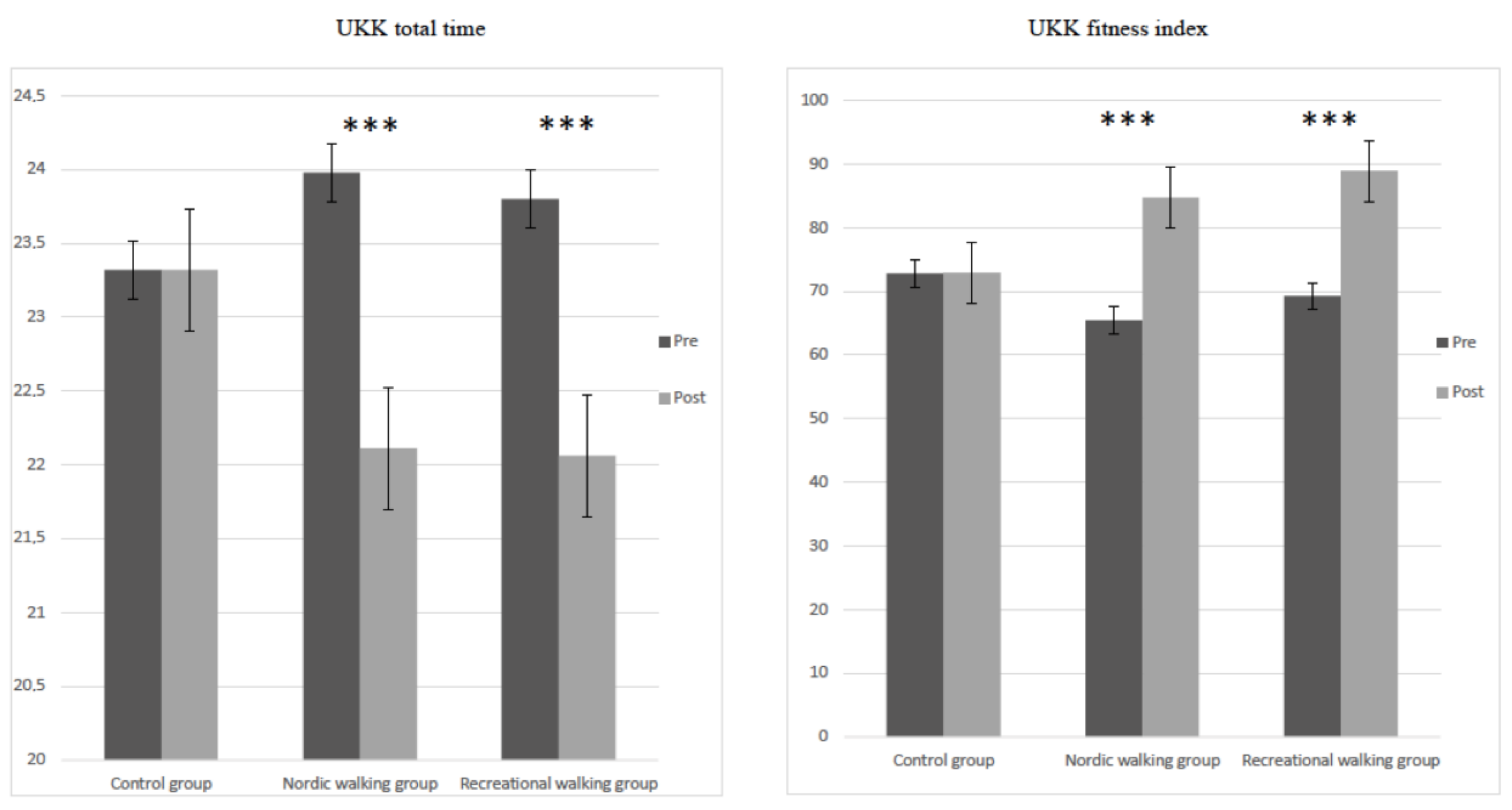
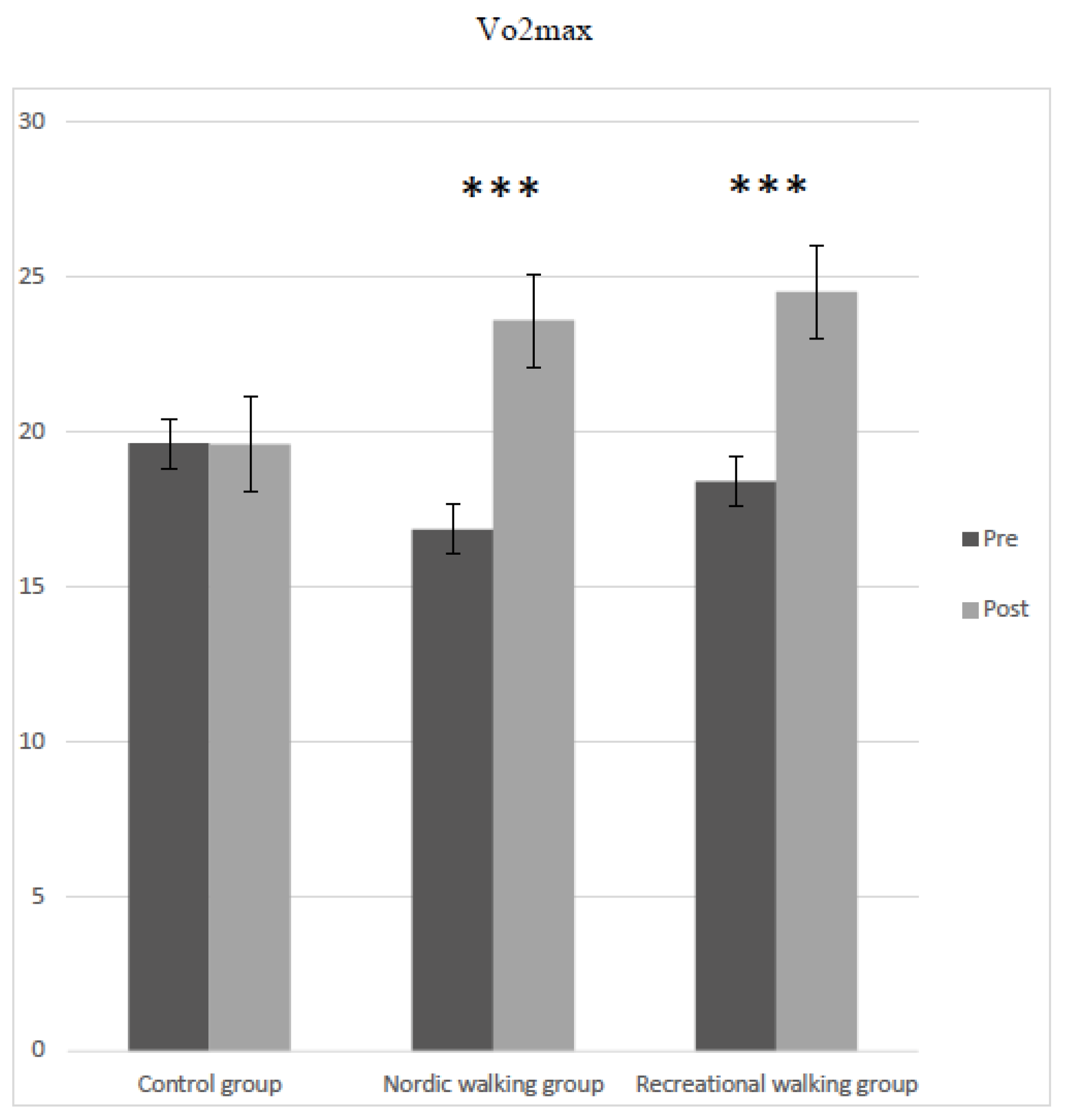
3.2. Differences in Body Composition Variables, HR Variables, UKK Test Measuring, and VO2max between Pretest and Posttest by Participant Group (Control, RW, and NW)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seguin, R.; Lamonte, M.; Tinker, L.; Liu, J.; Woods, N.; Michael, Y.L.; Bushnell, C.; Lacroix, A.Z. Sedentary Behavior and Physical Function Decline in Older Women: Findings from the Women’s Health Initiative. J. Aging Res. 2012, 2012, 271589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manson, J.E.; Greenland, P.; LaCroix, A.Z.; Stefanick, M.L.; Mouton, C.P.; Oberman, A.; Perri, M.G.; Sheps, D.S.; Pettinger, M.B.; Siscovick, D.S. Walking Compared with Vigorous Exercise for the Prevention of Cardiovascular Events in Women. N. Engl. J. Med. 2002, 347, 716–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rader, D.J. Effect of Insulin Resistance, Dyslipidemia, and Intra-Abdominal Adiposity on the Development of Cardiovascular Disease and Diabetes Mellitus. Am. J. Med. 2007, 120, S12–S18. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. American College of Sports Medicine ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2018. [Google Scholar]
- dos Santos, V.R.; Gobbo, L.A. Physical Activity Is Associated with Functional Capacity of Older Women with Osteosarcopenic Obesity: 24-Month Prospective Study. Eur. J. Clin. Nutr. 2020, 74, 912–919. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical Activity and Public Health in Older Adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Pepera, G.; Christina, M.; Katerina, K.; Argirios, P.; Varsamo, A. Effects of Multicomponent Exercise Training Intervention on Hemodynamic and Physical Function in Older Residents of Long-Term Care Facilities: A Multicenter Randomized Clinical Controlled Trial. J. Bodyw. Mov. Ther. 2021, 28, 231–237. [Google Scholar] [CrossRef]
- Bey, L.; Hamilton, M.T. Suppression of Skeletal Muscle Lipoprotein Lipase Activity during Physical Inactivity: A Molecular Reason to Maintain Daily Low-Intensity Activity. J. Physiol. 2003, 551, 673–682. [Google Scholar] [CrossRef]
- Bergamin, M.; Ermolao, A.; Tolomio, S.; Berton, L.; Sergi, G.; Zaccaria, M. Water- versus Land-Based Exercise in Elderly Subjects: Effects on Physical Performance and Body Composition. Clin. Interv. Aging 2013, 8, 1109–1117. [Google Scholar] [CrossRef] [Green Version]
- Crombie, I.K.; Irvine, L.; Williams, B.; McGinnis, A.R.; Slane, P.W.; Alder, E.M.; McMurdo, M.E.T. Why Older People Do Not Participate in Leisure Time Physical Activity: A Survey of Activity Levels, Beliefs and Deterrents. Age Ageing 2004, 33, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Montero, P.J.; Castillo-Rodriguez, A.; Mikalački, M.; Nebojsa, Č.; Korovljev, D. 24-Weeks Pilates-Aerobic and Educative Training To Improve Body Fat Mass in Elderly Serbian Women. Clin. Interv. Aging 2014, 9, 243–248. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ramirez-Vélez, R.; Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Valenzuela, P.L.; Lucia, A.; Izquierdo, M. Safety and Effectiveness of Long-Term Exercise Interventions in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Med. 2020, 50, 1095–1106. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic Exercise Ameliorates Cognitive Function in Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]
- Chase, J.A.D.; Phillips, L.J.; Brown, M. Physical Activity Intervention Effects on Physical Function among Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2017, 25, 149–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to Prevent Falls in Older Adults: An Updated Systematic Review and Meta-Analysis. Br. J. Sports Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.H.; Warburton, D.E.R. Physical Activity and Functional Limitations in Older Adults: A Systematic Review Related to Canada’s Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 1–22. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; Heo, M.; Heshka, S.; Wang, J.; Pierson, R.N.; Albu, J.; Wang, Z.; Heymsfield, S.B.; Gallagher, D. Total Body Potassium Differs by Sex and Race across the Adult Age Span. Am. J. Clin. Nutr. 2003, 78, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Poehlman, E.T.; Toth, M.J.; Fishman, P.S.; Vaitkevicius, P.; Gottlieb, S.S.; Fisher, M.L.; Fonong, T. Sarcopenia in Aging Humans: The Impact of Menopause and Disease. J. Gerontology Ser. A Biol. Sci. Med. Sci. 1995, 50, 73–77. [Google Scholar]
- Katula, J.A.; Sipe, M.; Rejeski, W.J.; Focht, B.C. Strength Training in Older Adults: An Empowering Intervention. Med. Sci. Sports Exerc. 2006, 38, 106–111. [Google Scholar] [CrossRef]
- Mankowski, R.T.; Anton, S.D.; Axtell, R.; Chen, S.H.; Fielding, R.A.; Glynn, N.W.; Hsu, F.C.; King, A.C.; Layne, A.S.; Leeuwenburgh, C.; et al. Device-Measured Physical Activity As a Predictor of Disability in Mobility-Limited Older Adults. J. Am. Geriatr. Soc. 2017, 65, 2251–2256. [Google Scholar] [CrossRef]
- Kim, C.H.; Wheatley, C.M.; Behnia, M.; Johnson, B.D. The Effect of Aging on Relationships between Lean Body Mass and VO2max in Rowers. PLoS ONE 2016, 11, e0160275. [Google Scholar] [CrossRef] [Green Version]
- Fisher, G.; McCarthy, J.P.; Zuckerman, P.A.; Bryan, D.R.; Bickel, C.S.; Hunter, G.R. Frequency of Combined Resistance and Aerobic Training in Older Women. J. Strength Cond. Res. 2013, 27, 1868–1876. [Google Scholar] [CrossRef] [Green Version]
- Campbell, E.; Petermann-Rocha, F.; Welsh, P.; Celis-Morales, C.; Pell, J.P.; Ho, F.K.; Gray, S.R. The Effect of Exercise on Quality of Life and Activities of Daily Life in Frail Older Adults: A Systematic Review of Randomised Control Trials. Exp. Gerontol. 2021, 147, 111287. [Google Scholar] [CrossRef] [PubMed]
- Morente-Oria, H.; Jesus Ruiz-Montero, P.; Chiva-Bartoll, O.; Tomas Gonzalez-Fernandez, F. Effects of 8-Weeks Concurrent Strength and Aerobic Training on Body Composition, Physiological and Cognitive Performance in Older Adult Women. Sustainability 2020, 12, 1944. [Google Scholar] [CrossRef] [Green Version]
- Suni, J.; Husu, P.; Rinne, M. Fitness for Health: The ALPHA-FIT Test. Battery for Adults Aged 18–69. Tester’s Manual; European Union DS: Tampere, Finland; UKK Institute for Health Promotion Research: Tampere, Finland, 2009. [Google Scholar]
- Jantunen, H.; Wasenius, N.; Salonen, M.K.; Perälä, M.M.; Osmond, C.; Kautiainen, H.; Simonen, M.; Pohjolainen, P.; Kajantie, E.; Rantanen, T.; et al. Objectively Measured Physical Activity and Physical Performance in Old Age. Age Ageing 2017, 46, 232–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gobbo, S.; Bullo, V.; Roma, E.; Duregon, F.; Bocalini, D.S.; Rica, R.L.; Di Blasio, A.; Cugusi, L.; Vendramin, B.; Bergamo, M.; et al. Nordic Walking Promoted Weight Lost in Overweight and Obese People: A Systematic Review for Future Exercise Prescription. J. Funct. Morphol. Kinesiol. 2019, 4, 36. [Google Scholar] [CrossRef] [Green Version]
- Pellegrini, B.; Boccia, G.; Zoppirolli, C.; Rosa, R.; Stella, F.; Bortolan, L.; Rainoldi, A.; Schena, F. Muscular and Metabolic Responses to Different Nordic Walking Techniques, When Style Matters. PLoS ONE 2018, 13, e0195438. [Google Scholar] [CrossRef] [Green Version]
- Notthoff, N.; Carstensen, L.L. Positive Messaging Promotes Walking in Older Adults. Psychol. Aging 2014, 29, 329–341. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, K.; Oka, J.; Yamakawa, J.; Higuchi, M. A Single Bout of Exercise Influences Natural Killer Cells in Elderly Women, Especially Those Who Are Habitually Active. J. Strength Cond. Res. 2005, 19, 45–50. [Google Scholar] [CrossRef]
- Tschentscher, M.; Niederseer, D.; Niebauer, J. Health Benefits of Nordic Walking: A Systematic Review. Am. J. Prev. Med. 2013, 44, 76–84. [Google Scholar] [CrossRef]
- Boccia, G.; Zoppirolli, C.; Bortolan, L.; Schena, F.; Pellegrini, B. Shared and Task-Specific Muscle Synergies of Nordic Walking and Conventional Walking. Scand. J. Med. Sci. Sports 2018, 28, 905–918. [Google Scholar] [CrossRef] [Green Version]
- Takeshima, N.; Islam, M.M.; Rogers, M.E.; Rogers, N.L.; Sengoku, N.; Koizumi, D.; Kitabayashi, Y.; Imai, A.; Naruse, A. Effects of Nordic Walking Compared to Conventional Walking and Band-Based Resistance Exercise on Fitness in Older Adults. J. Sports Sci. Med. 2013, 12, 422–430. [Google Scholar] [PubMed]
- Bullo, V.; Gobbo, S.; Vendramin, B.; Duregon, F.; Cugusi, L.; di Blasio, A.; Bocalini, D.S.; Zaccaria, M.; Bergamin, M.; Ermolao, A. Nordic Walking Can Be Incorporated in the Exercise Prescription to Increase Aerobic Capacity, Strength, and Quality of Life for Elderly: A Systematic Review and Meta-Analysis. Rejuvenation Res. 2018, 21, 141–161. [Google Scholar] [CrossRef] [PubMed]
- Gomeñuka, N.A.; Oliveira, H.B.; Silva, E.S.; Costa, R.R.; Kanitz, A.C.; Liedtke, G.V.; Schuch, F.B.; Peyré-Tartaruga, L.A. Effects of Nordic Walking Training on Quality of Life, Balance and Functional Mobility in Elderly: A Randomized Clinical Trial. PLoS ONE 2019, 14, e0211472. [Google Scholar] [CrossRef] [PubMed]
- Cugusi, L.; Manca, A.; Yeo, T.J.; Bassareo, P.P.; Mercuro, G.; Kaski, J.C. Nordic Walking for Individuals with Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. J. Prev. Cardiol. 2017, 24, 1938–1955. [Google Scholar] [CrossRef]
- Vardeman, S.; Hamburg, M.; Zuwaylif, F.H. Basic Statistics, A Modern Approach. J. Am. Stat. Assoc. 1980, 75, 2287210. [Google Scholar] [CrossRef]
- Ojala, K. UKK Walk Test. Tester’s Guide, 4th ed.; UKK Institute for Health Promotion Research: Tampere, Finland, 2013. [Google Scholar]
- Beam, W.C.; Adams, G.M. Exercise Physiology. Laboratory Manual, 7th ed.; McGraw-Hill: New York, NY, USA, 2014. [Google Scholar]
- Sawilowsky, S.S. New Effect Size Rules of Thumb. J. Mod. Appl. Stat. Methods 2009, 8, 26. [Google Scholar] [CrossRef]
- Panou, H.; Giovanis, V.; Tsougos, E.; Angelidis, G. Influence of the Nordic Walking Intervention Program on the Improvement of Functional Parameters in Older Women. Top. Geriatr. Rehabil. 2019, 35, 129–133. [Google Scholar] [CrossRef]
- Sugiyama, K.; Kawamura, M.; Tomita, H.; Katamoto, S. Oxygen Uptake, Heart Rate, Perceived Exertion, and Integrated Electromyogram of the Lower and Upper Extremities during Level and Nordic Walking on a Treadmill. J. Physiol. Anthropol. 2013, 32, 2. [Google Scholar] [CrossRef] [Green Version]
- Beauchet, O.; Annweiler, C.; Lecordroch, Y.; Allali, G.; Dubost, V.; Herrmann, F.R.; Kressig, R.W. Walking Speed-Related Changes in Stride Time Variability: Effects of Decreased Speed. J. NeuroEngineering Rehabil. 2009, 6, 32. [Google Scholar] [CrossRef]
- Figard-Fabre, H.; Fabre, N.; Leonardi, A.; Schena, F. Physiological and Perceptual Responses to Nordic Walking in Obese Middle-Aged Women in Comparison with the Normal Walk. Eur. J. Appl. Physiol. 2010, 108, 1141–1151. [Google Scholar] [CrossRef]
- Sanchez-Lastra, M.A.; Miller, K.J.; Martinez-Lemos, R.I.; Giraldez, A.; Ayan, C. Nordic Walking for Overweight and Obese People: A Systematic Review and Meta-Analysis. J. Phys. Act. Health 2020, 17, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, B.; Peyré-Tartaruga, L.A.; Zoppirolli, C.; Bortolan, L.; Bacchi, E.; Figard-Fabre, H.; Schena, F. Exploring Muscle Activation during Nordic Walking: A Comparison between Conventional and Uphill Walking. PLoS ONE 2015, 10, e0138906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffer, T.; Knicker, A.; Montanarella, M.; Strüder, H.K. Mechanical and Physiological Effects of Varying Pole Weights during Nordic Walking Compared to Walking. Eur. J. Appl. Physiol. 2011, 111, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Hansen, E.A.; Smith, G. Energy Expenditure and Comfort During Nordic Walking With Different Pole Lengths. J. Strength Cond. Res. 2009, 23, 1187–1194. [Google Scholar] [CrossRef] [Green Version]
- Mikalacki, M.; Cokorilo, N.; Katić, R. Effect of Nordic Walking on Functional Ability and Blood Pressure in Elderly Women. Coll. Antropol. 2011, 35, 889–894. [Google Scholar]
- Kukkonen-Harjula, K.; Hiilloskorpi, H.; Mänttäri, A.; Pasanen, M.; Parkkari, J.; Suni, J.; Fogelholm, M.; Laukkanen, R. Self-Guided Brisk Walking Training with or without Poles: A Randomized-Controlled Trial in Middle-Aged Women. Scandinavian J. Med. Sci. Sports 2007, 17, 316–323. [Google Scholar] [CrossRef]
- Pérez-Soriano, P.; Encarnación-Martínez, A.; Aparicio-Aparicio, I.; Giménez, J.; Llana-Belloch, S. Nordic Walking: A Systematic Review. Eur. J. Hum. Mov. 2014, 33, 26–45. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2021 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pretest Intervention | Intervention | Posttest Intervention | ||||||||||||
| Months | July | August | September | October | December | |||||||||
| Week | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
| Control group | Pretest | 35 min of continuous aerobic (60–65% %HRmax) | Posttest | |||||||||||
| Nordic-walking group | Pretest | 40 min of continuous aerobic (65–70% %HRmax) | Posttest | |||||||||||
| Recreational-walking group | Pretest | 45 min of continuous aerobic (75–80% %HRmax) | Posttest | |||||||||||
| Pretest | ||||||
|---|---|---|---|---|---|---|
| Variables Involved in UKK Walking Test | Control Group (n = 60) | Nordic-Walking Group (n = 53) | Recreational-Walking Group (n = 53) | F | p | η2 |
| Body mass (kg) | 69.35 ± 9.26 | 70.27 ± 9.61 | 69.40 ± 8.38 | 0.177 | 0.838 | 0.002 |
| BMI (kg/m2) | 25.52 ± 3.58 | 26.20 ± 3.88 | 25.83 ± 4.13 | 0.436 | 0.648 | 0.005 |
| Walking heart rate (bt/min) | 82.13 ± 9.36 b | 87.12 ± 12.36 ab | 79.17 ± 9.45 a | 7.847 | 0.001 | 0.088 |
| Heart rate at the end of the test (bt/min) | 114.35 ± 12.48 | 112.68 ± 15.75 | 117.26 ± 15.07 | 1.374 | 0.256 | 0.017 |
| UKK total time (min) | 23.32 ± 1.65 | 23.98 ± 1.48 | 23.80 ± 2.12 | 2.123 | 0.123 | 0.025 |
| UKK fitness index | 72.75 ± 15.76 | 65.42 ± 20.61 | 69.28 ± 19.01 | 2.211 | 0.113 | 0.026 |
| VO2max (mL·min−1·kg−1) | 19.61 ± 5.52 | 16.85 ± 5.42 | 18.39 ± 7.31 | 2.839 | 0.061 | 0.034 |
| Posttest | ||||||
|---|---|---|---|---|---|---|
| Variables Involved in UKK Walking Test | Control Group (n = 60) | Nordic-Walking Group (n = 53) | Recreational-Walking Group (n = 53) | F | p | η2 |
| Body mass (kg) | 69.37 ± 9.25 | 68.44 ± 9.64 | 67.18 ± 8.25 | 0.823 | 0.441 | 0.010 |
| BMI (kg/m2) | 25.53 ± 3.55 | 25.52 ± 3.85 | 25.01 ± 4.05 | 0.332 | 0.718 | 0.004 |
| Walking heart rate (bt/min) | 82.35 ± 9.09 b,c | 79.45 ± 9.36 a,b | 73.54 ± 7.32 a,c | 14.919 | 0.001 | 0.155 |
| Heart rate at the end of the test (bt/min) | 114.13 ± 11.56 a,b | 105.09 ± 11.61 a | 106.51 ± 14.81 b | 8.402 | 0.001 | 0.093 |
| UKK total time (min) | 23.32 ± 1.84 a,b | 22.11 ± 1.76 a | 22.06 ± 1.91 b | 8.748 | 0.001 | 0.097 |
| UKK fitness index | 72.95 ± 18.13 a,b | 84.72 ± 15.94 a | 88.92 ± 19.42 b | 12.230 | 0.001 | 0.130 |
| VO2max (mL·min−1·kg−1) | 19.59 ± 6.14 a,b | 23.58 ± 6.05 a | 24.51 ± 6.41 b | 10.168 | 0.001 | 0.111 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cokorilo, N.; Ruiz-Montero, P.J.; González-Fernández, F.T.; Martín-Moya, R. An Intervention of 12 Weeks of Nordic Walking and Recreational Walking to Improve Cardiorespiratory Capacity and Fitness in Older Adult Women. J. Clin. Med. 2022, 11, 2900. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102900
Cokorilo N, Ruiz-Montero PJ, González-Fernández FT, Martín-Moya R. An Intervention of 12 Weeks of Nordic Walking and Recreational Walking to Improve Cardiorespiratory Capacity and Fitness in Older Adult Women. Journal of Clinical Medicine. 2022; 11(10):2900. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102900
Chicago/Turabian StyleCokorilo, Nebojsa, Pedro Jesús Ruiz-Montero, Francisco Tomás González-Fernández, and Ricardo Martín-Moya. 2022. "An Intervention of 12 Weeks of Nordic Walking and Recreational Walking to Improve Cardiorespiratory Capacity and Fitness in Older Adult Women" Journal of Clinical Medicine 11, no. 10: 2900. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102900