
Kidney Biopsy in Patients with Cancer along the Last Decade: A Multicenter Study

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Clinical Variables
2.3. Statistical Analysis
3. Results
3.1. Baseline Chracteristics of Population
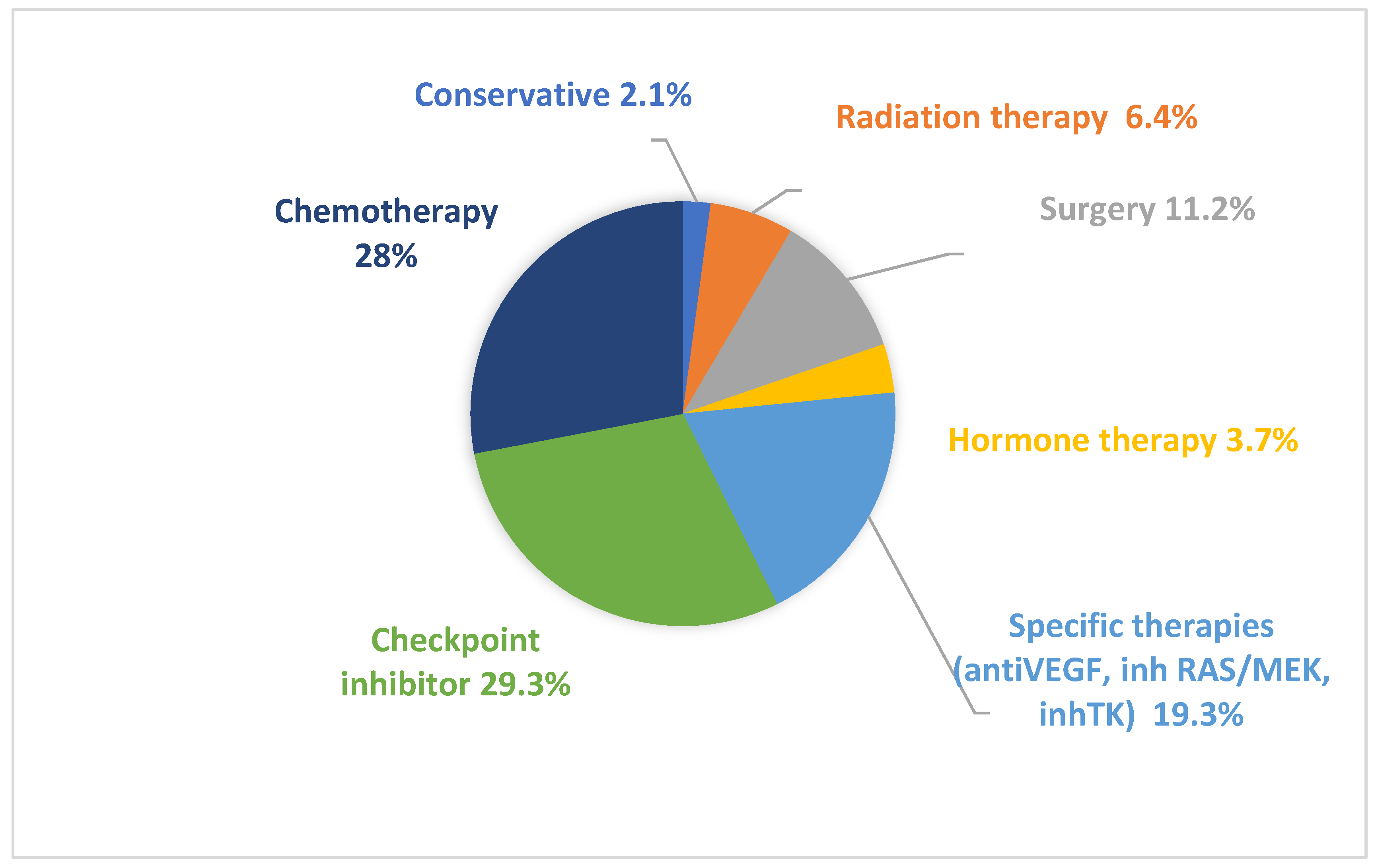
3.2. Administered Therapies
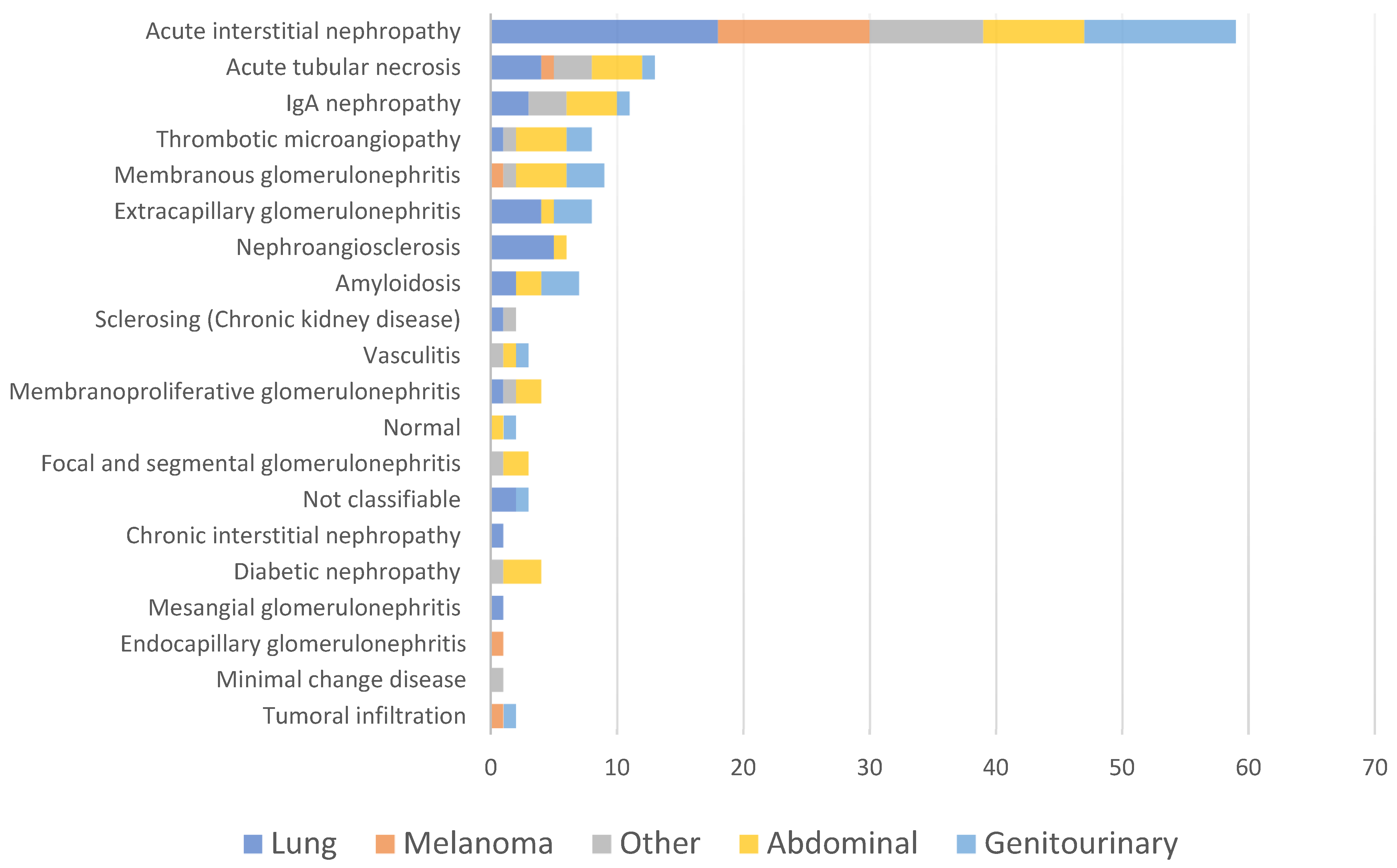
3.3. Renal Biopsy Diagnosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosner, M.H.; Jhaveri, K.D.; McMahon, B.A.; Perazella, M.A. Onconephrology: The intersections between the kidney and cancer. CA Cancer J. Clin. 2021, 71, 47–77. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cosmai, L.; Porta, C.; Perazella, M.A.; Launay-Vacher, V.; Rosner, M.H.; Jhaveri, K.D.; Floris, M.; Pani, A.; Teuma, C.; Szczylik, C.A.; et al. Opening an onconephrology clinic: Recommendations and basic requirements. Nephrol. Dial. Transplant. 2018, 33, 1503–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salahudeen, A.K.; Bonventre, J.V. Onconephrology: The latest frontier in the war against kidney disease. J. Am. Soc. Nephrol. JASN 2013, 24, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Alonso, F.; Auñón, P.; Cavero, T.; Salgueira, M.; Praga, M.; Quiroga, B.; de Francisco, Á.L.M.; Macía, M.; Grupo Español de Onconefrología (ONCONEFRO). Monographic consultation of onconephrology. Rationale and implementation. Nefrologia 2021, 41, 154–164. [Google Scholar] [CrossRef]
- Seethapathy, H.; Zhao, S.; Chute, D.F.; Zubiri, L.; Oppong, Y.; Strohbehn, I.; Cortazar, F.B.; Leaf, D.E.; Mooradian, M.J.; Villani, A.-C.; et al. The Incidence, Causes, and Risk Factors of Acute Kidney Injury in Patients Receiving Immune Checkpoint Inhibitors. Clin. J. Am. Soc. Nephrol. 2019, 14, 1692–1700. [Google Scholar] [CrossRef]
- García-Carro, C.; Bolufer, M.; Bury, R.; Catañeda, Z.; Muñoz, E.; Felip, E.; Lorente, D.; Josep Carreras, M.; Gabaldon, A.; Agraz, I.; et al. Acute kidney injury as a risk factor for mortality in oncological patients receiving check-point inhibitors. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 37, 887–894. [Google Scholar] [CrossRef]
- Oleas, D.; Bolufer, M.; Agraz, I.; Felip, E.; Muñoz, E.; Gabaldón, A.; Bury, R.; Espinel, E.; Serón, D.; García-Carro, C.; et al. Acute interstitial nephritis associated with immune checkpoint inhibitors: A single-centre experience. Clin. Kidney J. 2020, 14, 1364–1370. [Google Scholar] [CrossRef] [Green Version]
- Cortazar, F.B.; Kibbelaar, Z.A.; Glezerman, I.G.; Abudayyeh, A.; Mamlouk, O.; Motwani, S.S.; Murakami, N.; Herrmann, S.M.; Manohar, S.; Shirali, A.C.; et al. Clinical Features and Outcomes of Immune Checkpoint Inhibitor–Associated AKI: A Multicenter Study. J. Am. Soc. Nephrol. 2020, 31, 435–446. [Google Scholar] [CrossRef]
- Manohar, S.; Kompotiatis, P.; Thongprayoon, C.; Cheungpasitporn, W.; Herrmann, J.; Herrmann, S.M. Programmed cell death protein 1 inhibitor treatment is associated with acute kidney injury and hypocalcemia: Meta-analysis. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2019, 34, 108–117. [Google Scholar] [CrossRef]
- Gupta, S.; Short, S.A.P.; Sise, M.E.; Prosek, J.M.; Madhavan, S.M.; Soler, M.J.; Ostermann, M.; Herrmann, S.M.; Abudayyeh, A.; Anand, S.; et al. Acute kidney injury in patients treated with immune checkpoint inhibitors. J. Immunother. Cancer 2021, 9, e003467. [Google Scholar] [CrossRef] [PubMed]
- Meraz-Muñoz, A.; Amir, E.; Ng, P.; Avila-Casado, C.; Ragobar, C.; Chan, C.; Kim, J.; Wald, R.; Kitchlu, A. Acute kidney injury associated with immune checkpoint inhibitor therapy: Incidence, risk factors and outcomes. J. Immunother. Cancer 2020, 8, e000467. [Google Scholar] [CrossRef] [PubMed]
- Kitchlu, A.; Jhaveri, K.D.; Wadhwani, S.; Deshpande, P.; Harel, Z.; Kishibe, T.; Henriksen, K.; Wanchoo, R. A Systematic Review of Immune Checkpoint Inhibitor-Associated Glomerular Disease. Kidney Int. Rep. 2021, 6, 66–77. [Google Scholar] [CrossRef]
- Perazella, M.A.; Shirali, A.C. Immune checkpoint inhibitor nephrotoxicity: What do we know and what should we do? Kidney Int. 2020, 97, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Porta, C.; Bamias, A.; Danesh, F.R.; Dębska-Ślizień, A.; Gallieni, M.; Gertz, M.A.; Kielstein, J.T.; Tesarova, P.; Wong, G.; Cheung, M.; et al. KDIGO Controversies Conference on onco-nephrology: Understanding kidney impairment and solid-organ malignancies, and managing kidney cancer. Kidney Int. 2020, 98, 1108–1119. [Google Scholar] [CrossRef] [PubMed]
- Perazella, M.A. Kidney Biopsy Should Be Performed to Document the Cause of Immune Checkpoint Inhibitor–Associated Acute Kidney Injury: Commentary. Kidney360 2020, 1, 166–168. [Google Scholar] [CrossRef] [Green Version]
- 2012 AKI Guideline KDIGO. Kidney Int. Suppl. 2012, 2, 1.
- Ryu, H.; Kim, K.; Ryu, J.; Son, H.-E.; Ryu, J.-Y.; Kim, S.; Na, K.Y.; Chae, D.W.; Chin, H.J.; Korean GlomeruloNephritis Study Group. Cancer development and mortality differences in patients with glomerulonephritis after renal biopsy: A single center retrospective cohort study. BMC Nephrol. 2020, 21, 221. [Google Scholar] [CrossRef]
- Ashour, T.; Nakhoul, G.; Patil, P.; Funchain, P.; Herlitz, L. Immune Check Point Inhibitor-Associated Glomerulonephritis. Kidney Int. Rep. 2019, 4, 355–359. [Google Scholar] [CrossRef] [Green Version]
- Moledina, D.G.; Wilson, F.P.; Pober, J.S.; Perazella, M.A.; Singh, N.; Luciano, R.L.; Obeid, W.; Lin, H.; Kuperman, M.; Moeckel, G.W.; et al. Urine TNF-α and IL-9 for clinical diagnosis of acute interstitial nephritis. JCI Insight 2019, 4, 127456. [Google Scholar] [CrossRef] [Green Version]
- Rashidi, A.; Shah, C.; Sekulic, M. The role of kidney biopsy in Immune Checkpoint Inhibitor-associated AKI. Kidney360 2022, 3, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.C.; Haas, M.; Reich, H.N. IgA Nephropathy. Clin. J. Am. Soc. Nephrol. 2017, 12, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Janus, N.; Launay-Vacher, V.; Byloos, E.; Machiels, J.-P.; Duck, L.; Kerger, J.; Wynendaele, W.; Canon, J.-L.; Lybaert, W.; Nortier, J.; et al. Cancer and renal insufficiency results of the BIRMA study. Br. J. Cancer 2010, 103, 1815–1821. [Google Scholar] [CrossRef]
- Canter, D.; Kutikov, A.; Sirohi, M.; Street, R.; Viterbo, R.; Chen, D.Y.T.; Greenberg, R.E.; Uzzo, R.G. Prevalence of baseline chronic kidney disease in patients presenting with solid renal tumors. Urology 2011, 77, 781–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosner, M.H.; Perazella, M.A. Acute kidney injury in the patient with cancer. Kidney Res. Clin. Pract. 2019, 38, 295–308. [Google Scholar] [CrossRef] [Green Version]
- Gallieni, M.; Cosmai, L.; Porta, C. Acute Kidney Injury in Cancer Patients. In Contributions to Nephrology; Ding, X., Rosner, M.H., Ronco, C., Eds.; S. Karger AG: Basel, Switzerland, 2018; Volume 193, pp. 137–148. ISBN 978-3-318-06310-3. [Google Scholar]
- Wang, L.-Y.; Wang, J.-N.; Diao, Z.-L.; Guan, Y.-M.; Liu, W.-H. Acute Kidney Injury in Oncology Patients. J. Cancer 2020, 11, 9. [Google Scholar] [CrossRef] [PubMed]
- Salahudeen, A.K.; Doshi, S.M.; Pawar, T.; Nowshad, G.; Lahoti, A.; Shah, P. Incidence rate, clinical correlates, and outcomes of AKI in patients admitted to a comprehensive cancer center. Clin. J. Am. Soc. Nephrol. 2013, 8, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Kitchlu, A.; McArthur, E.; Amir, E.; Booth, C.M.; Sutradhar, R.; Majeed, H.; Nash, D.M.; Silver, S.A.; Garg, A.X.; Chan, C.T.; et al. Acute Kidney Injury in Patients Receiving Systemic Treatment for Cancer: A Population-Based Cohort Study. J. Natl. Cancer Inst. 2019, 111, 727–736. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Size | 148 Patients |
|---|---|
| Age | 66.9 (SD ± 10.5) |
| Gender | 64.2% men |
| Diabetes mellitus | 29.7% |
| Arterial hypertension | 62.2% |
| Systolic blood pressure | 131 [120–146.2 (IQ 25–75)] |
| Non-steroidal anti-inflammatory drugs | 12.2% |
| Renin-angiotensine aldosterone system blockade | 62.8% |
| Cr prior to kidney biopsy (mg/dL) | 1 [0.82–1.3 (IQ 25–75)] |
| Median Glomerular Filtration Rate by CKD-EPI (mL/min/1.73 m2) | 61 [24.7–83.8 (IQ 25–75)] |
| Cr prior to kidney biopsy > 1.5 (mg/dL) | 15.5% |
| Malignancies | |
| -Lung | 29.1% |
| -Melanoma | 10.8% |
| -Abdominal | 25.0% |
| -Genitourinary | 19.6% |
| -Others | 15.5% |
| Oncological status | |
| -In remission | 15.2% |
| -Free from disease | 25.5% |
| -Stable | 24.1% |
| -In progression | 35.2% |
| Metastatic neoplasm at the time of kidney biopsy | 49.7% |
| Systolic blood pressure (mmHg) | 131 [120–146.2 (IQ 25–75)] |
| Diastolic blood pressure (mmHg) | 74 [68–81.2 (IQ 25–75)] |
| Median creatinine (mg/dL) | 2.58 [1.81–4.1 (IQ 25–75)] |
| Median Glomerular Filtration Rate by CKD-EPI (mL/min/1.73 m2) | 21.8 [12.7–34 (IQ 25–75)] |
| Urine protein/creatinine ratio (mg/g) | 700 [256–2463 (IQ 25–75)] |
| Urine albuminuria/creatinine ratio (mg/g) | 220 [46–1196 (IQ 25–75)] |
| Nephrotic range proteinuria | 23% |
| Hematuria | 53.1% |
| Eosinophiluria | 10.8% |
| Leukocyturia | 31.8% |
| ANCA (Neutrophil cytoplasmic antibodies) | 6.8% |
| Antinuclear antibodies | 13.5% |
| Low C3 and/or C4 serum levels | 10.1% |
| C3 mg/dL (85–180) | 127.2 (SD ± 36.8) |
| C4 mg/dL (10–40) | 28.8 (SD ± 9.6) |
| pH | 7.35 [7.29–7.39 (IQ 25–75)] |
| Bicarbonate | 21.7 (SD ± 4.9) |
| K (mmol/L) | 4.2 [4.0–4.7 (IQ 25–75)] |
| Na (mmol/L) | 138.1 [136–140 (IQ 25–75)] |
| Ca (mg/dL) | 8.9 [8.5–9.3 (IQ 25–75)] |
| Mg (mg/dL) | 1.9 [1.7–2.2 (IQ 25–75)] |
| P (mg/dL) | 4.1 [3.4–5.3 (IQ 25–75)] |
| Hb (g/dL) | 10.7 (SD ± 2.2) |
| Platelets (×109/L) | 233.5 [189–312 (IQ 25–75)] |
| Haemolytic anemia and/or low platelet | 6.8% |
| Pathological Diagnosis | N (%) |
|---|---|
| Acute interstitial nephritis | 59 (39.9) |
| Acute tubular necrosis | 13 (8.8) |
| IgA nephropathy | 11 (7.4) |
| Membranous nephropathy | 9 (6.1) |
| Thrombotic microangiopathy | 8 (5.4) |
| Extracapillary glomerulonephritis | 8 (5.4) |
| Amyloidosis | 7 (4.7) |
| Nephroangiosclerosis | 6 (4.1) |
| Membranoproliferative glomerulonephritis | 4 (2.7) |
| Diabetic nephropathy | 4 (2.7) |
| Vasculitis | 3 (2) |
| Not classifiable | 3 (2) |
| Focal and segmental glomerulosclerosis | 3 (2) |
| Cancer cells infiltration | 2 (1.4) |
| Sclerosing (Chronic kidney disease) | 2 (1.4) |
| Normal | 2 (1.4) |
| Chronic interstitial nephropathy | 1 (0.7) |
| Endocapillary glomerulonephritis | 1 (0.7) |
| Minimal change disease | 1 (0.7) |
| Mesangial glomerulonephritis | 1 (0.7) |
| Kidney Disease Secondary to Oncological Process–Paraneoplastic | Kidney Disease Secondary to Anticancer Drugs | Others | |
|---|---|---|---|
| Acute Kidney injury | Membranoproliferative GN Amyloidosis Membranous nephropathy IgA Nephropathy Extracapillary GN TMA | Extracapillary GN | |
| AIN | IgA nephropathy | ||
| TMA | AIN | ||
| ATN | Membranoproliferative GN | ||
| Chronic interstitial nephropathy | Vasculitis | ||
| No classificable | Amyloidosis | ||
| Extracapillary GN | ATN | ||
| Extracapillary GN | No classificable | ||
| Nephroangiosclerosis | Nephroangiosclerosis | ||
| Chronic kidney disease | No case | AIN | IgA nephropathy Focal and segmental glomerulosclerosis Nephroangiosclerosis Sclerosing |
| Exacerbated chronic kidney disease | Extracapillary GN | AIN | Amyloidosis Normal AIN |
| Proteinuria | Amyloidosis Membranous nephropathy | TMA Membranous nephropathy | Membranous nephropathy IgA nephropathy TMA Focal and segmental glomerulosclerosis Mesangial GN Nephroangiosclerosis Sclerosing Membranoproliferative GN |
| Antibiotics (n = 4) | Meropenem, Ciprofloxacin, Vancomycin, Cefepime |
| Non-immunotherapy antineoplastics (n = 13) | MEK B-Raf inhibitor (n = 2), Bacillus Calmette Guérin (n = 3), Tyrosine Kinsae Inhibitor (n = 3), Anti-vascular endothelial growth factor (n = 4) and Carboxyplatin. |
| Others (n = 3) | Non-steroidal Anti-inflammatory drugs, Sarcoidosis, unknown cause. |
| Cancer | Time Kidney Biopsy | Clinical Features | PLA2R | Treatment | Renal Outcome | Cancer Outcome |
|---|---|---|---|---|---|---|
| Sigma | +2 years | Cr 1 mg/dL Prot 1.0893 mg/g | + | Rituximab | Progression to CKD | Progression |
| Gastrointestinal stromal tumor | +1 week | Cr 0.8 mg/dL Prot 6 g/24 h | + | Neoplasm treatment | No remission | Death 5 months later |
| Anal | Previous 5 month | Cr 1.06 mg/dL Prot 2.630 mg/g | Unknown | Neoplasm treatment | Partial remission | Progression and death |
| Bladder | +3 month | Cr 1.2 mg/dL Prot 7.800 mg/g | + | Rituximab | Complete remission | Progression |
| Bladder | +4 years | Cr 3.34 mg/dL Prot 9.100 mg/g | − | Rituximab | Partial remission | Partial remission |
| Intestinal | +2 years | Cr 2.6 mg/dL Prot 8.034 mg/g | Unknown | Corticosteroids and cyclophosphamide | Partial remission | Progression |
| Bladder | +8 month | Cr 4.31 mg/dL Prot 13.840 mg/g | − | Empirical corticosteroids | Complete remission | |
| Breast | +5 month | Cr 0.7 mg/dL Prot 7886 mg/g | + | Rituximab | Relapse | Stable disease |
| Melanoma | +8 years | Cr 1.7 mg/dL Prot 1400 mg/g | − | Corticosteroids | Complete remission |
| Drug | Histopathological Diagnosis |
|---|---|
| Anti CTLA4 + PD1/PD-1/PD-L1 | AIN, Extracapillary GN, Membranous nephropathy. |
| Pemetrexed | Chronic interstitial nephropathy |
| Emactuzumab | No classificable |
| Cisplatin | Nephroangioesclerosis |
| MEK/B-RAF | AIN |
| Anti VEGF | TMA |
| Oxiplatino | ATN |
| Alectinib | ATN |
| Capetitabine | ATN |
| Gemcitabine | TMA |
| Tyrosine kinase inhibitor | AIN |
| Bacillus Calmette Guérin | AIN |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolufer, M.; García-Carro, C.; Blasco, M.; Quintana, L.F.; Shabaka, A.; Rabasco, C.; Draibe, J.; Merino, A.; Melero, M.R.; Alonso, F.; et al. Kidney Biopsy in Patients with Cancer along the Last Decade: A Multicenter Study. J. Clin. Med. 2022, 11, 2915. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102915
Bolufer M, García-Carro C, Blasco M, Quintana LF, Shabaka A, Rabasco C, Draibe J, Merino A, Melero MR, Alonso F, et al. Kidney Biopsy in Patients with Cancer along the Last Decade: A Multicenter Study. Journal of Clinical Medicine. 2022; 11(10):2915. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102915
Chicago/Turabian StyleBolufer, Mónica, Clara García-Carro, Miquel Blasco, Luis F. Quintana, Amir Shabaka, Cristina Rabasco, Juliana Draibe, Ana Merino, María Rosa Melero, Fabiola Alonso, and et al. 2022. "Kidney Biopsy in Patients with Cancer along the Last Decade: A Multicenter Study" Journal of Clinical Medicine 11, no. 10: 2915. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102915