
Association of Albumin-Corrected Serum Calcium Levels with Colorectal Cancer Survival Outcomes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
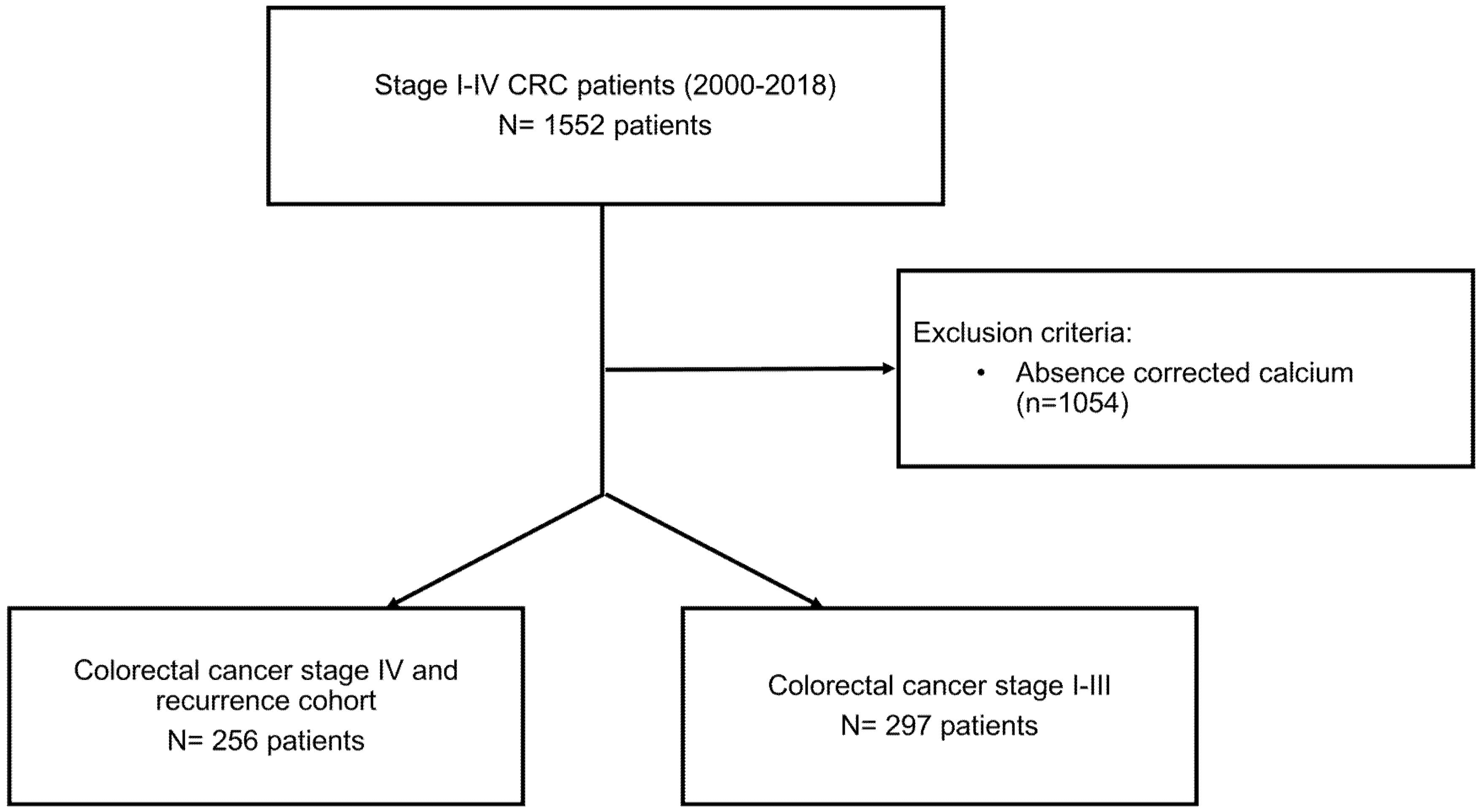
2.1. Study Population
2.2. Body Composition
2.3. Data Collection
2.3.1. Clinical Variables
2.3.2. Biochemical Exam Data
2.3.3. Corrected Calcium Measurement
2.3.4. Systemic Inflammatory Indexes
2.3.5. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patient Disposition and Baseline Characteristics
3.2. Body Composition and Inflammatory Indexes
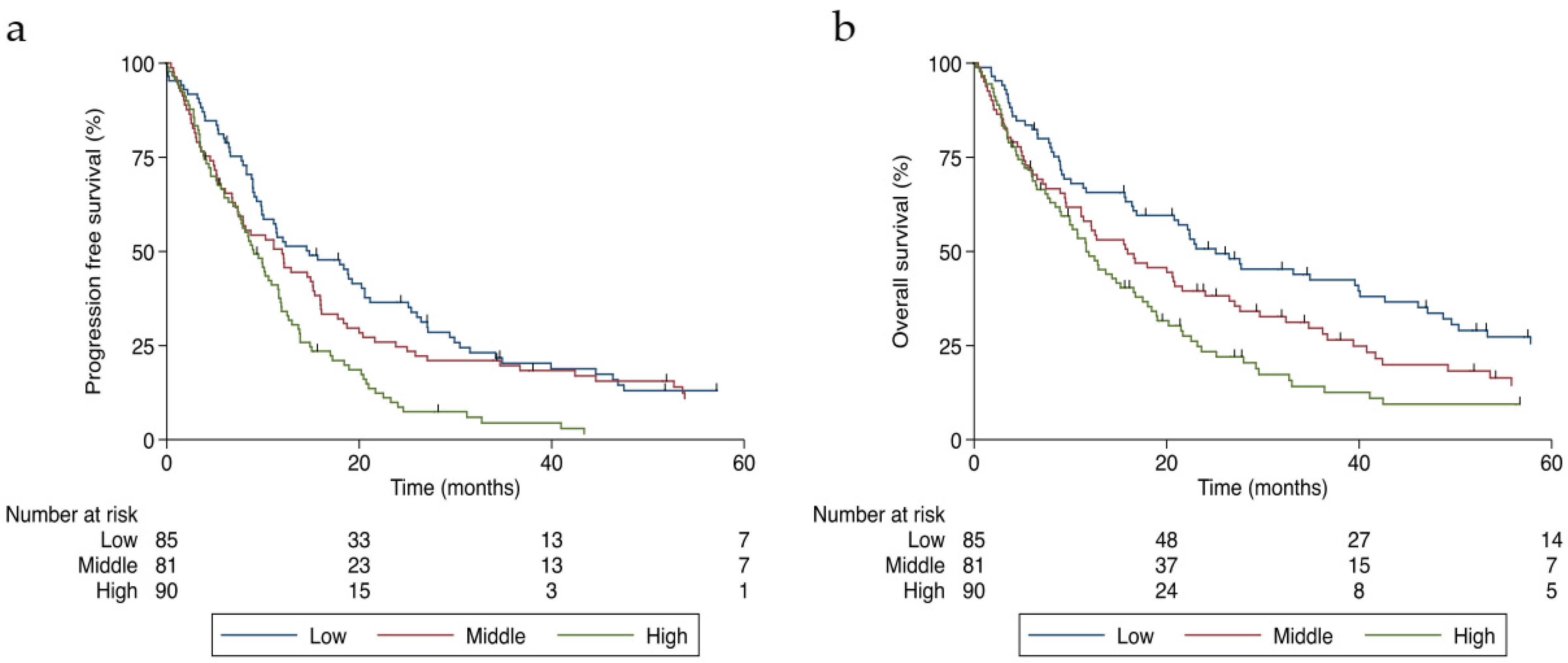
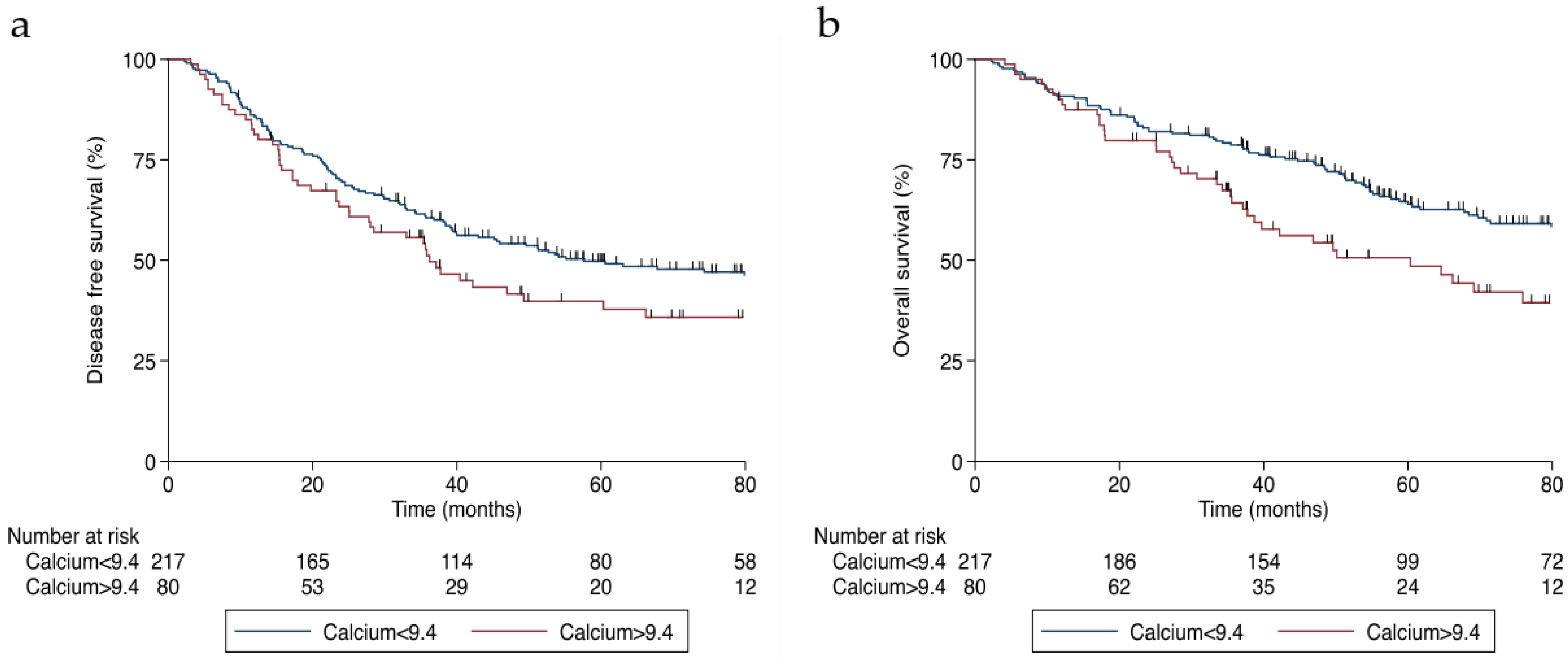
3.3. Survival Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Robertson, A.S.; Rodriguez, C.; Jacobs, E.J.; Chao, A.; Carolyn, J.; Calle, E.E.; Willett, W.C.; Thun, M.J. Calcium, vitamin D, dairy products, and risk of colorectal cancer in the Cancer Prevention Study II Nutrition Cohort (United States). Cancer Causes Control 2003, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Willett, W.C.; Fuchs, C.S.; Colditz, G.A.; Giovannucci, E.L. Calcium intake and risk of colon cancer in women and men. J. Natl. Cancer Inst. 2002, 94, 437–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, C.; Shin, A.; Lee, J.; Lee, J.; Park, J.W.; Oh, J.H.; Kim, J. Dietary calcium intake and the risk of colorectal cancer: A case control study. BMC Cancer 2015, 15, 966. [Google Scholar] [CrossRef] [Green Version]
- Keum, N.; Aune, D.; Greenwood, D.C.; Ju, W.; Giovannucci, E.L. Calcium intake and colorectal cancer risk: Dose-response meta-analysis of prospective observational studies. Int. J. Cancer 2014, 135, 1940–1948. [Google Scholar] [CrossRef]
- Cho, E.; Smith-Warner, S.A.; Spiegelman, D.; Beeson, W.L.; van den Brandt, P.A.; Colditz, G.A.; Folsom, A.R.; Fraser, G.E.; Freudenheim, J.L.; Giovannucci, E.; et al. Dairy foods, calcium, and colorectal cancer: A pooled analysis of 10 cohort studies. J. Natl. Cancer Inst. 2004, 96, 1015–1022. [Google Scholar] [CrossRef] [Green Version]
- Crockett, S.D.; Barry, E.L.; Mott, L.A.; Ahnen, D.J.; Robertson, D.J.; Anderson, J.C.; Wallace, K.; Burke, C.A.; Bresalier, R.S.; Figueiredo, J.C.; et al. Calcium and vitamin D supplementation and increased risk of serrated polyps: Results from a randomised clinical trial. Gut 2018, 68, 475–486. [Google Scholar] [CrossRef]
- Monteith, G.R.; Prevarskaya, N.; Roberts-Thomson, S.J. The calcium-cancer signalling nexus. Nat. Rev. Cancer 2017, 17, 367–380. [Google Scholar] [CrossRef] [Green Version]
- Wulaningsih, W.; Michaelsson, K.; Garmo, H.; Hammar, N.; Jungner, I.; Walldius, G.; Lambe, M.; Holmberg, L.; Van Hemelrijck, M. Serum calcium and risk of gastrointestinal cancer in the Swedish AMORIS study. BMC Public Health 2013, 13, 663. [Google Scholar] [CrossRef] [Green Version]
- Blaine, J.; Chonchol, M.; Levi, M. Renal control of calcium, phosphate, and magnesium homeostasis. Clin. J. Am. Soc. Nephrol. 2015, 10, 1257–1272. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.F. Clinical practice. Hypercalcemia associated with cancer. N. Engl. J. Med. 2005, 352, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Karaplis, A.C.; Luz, A.; Glowacki, J.; Bronson, R.T.; Tybulewicz, V.L.; Kronenberg, H.M.; Mulligan, R.C. Lethal skeletal dysplasia from targeted disruption of the parathyroid hormone-related peptide gene. Genes Dev. 1994, 8, 277–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanske, B.; Karaplis, A.C.; Lee, K.; Luz, A.; Vortkamp, A.; Pirro, A.; Karperien, M.; Defize, L.H.; Ho, C.; Mulligan, R.C.; et al. PTH/PTHrP receptor in early development and Indian hedgehog-regulated bone growth. Science 1996, 273, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Mundy, G.R.; Edwards, J.R. PTH-related peptide (PTHrP) in hypercalcemia. J. Am. Soc. Nephrol. 2008, 19, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, N.; Yoon, H.-j.; Lee, Y.-h.; Kim, H.R.; Lee, B.W.; Rhee, Y.; Kang, E.S.; Cha, B.-S.; Lee, H.C. Serum PTHrP Predicts Weight Loss in Cancer Patients Independent of Hypercalcemia, Inflammation, and Tumor Burden. J. Clin. Endocrinol. Metab. 2016, 101, 1207–1214. [Google Scholar] [CrossRef] [Green Version]
- Nishihara, M.; Ito, M.; Tomioka, T.; Ohtsuru, A.; Taguchi, T.; Kanematsu, T. Clinicopathological implications of parathyroid hormone-related protein in human colorectal tumours. J. Pathol. 1999, 187, 217–222. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef]
- Mitsiopoulos, N.; Baumgartner, R.N.; Heymsfield, S.B.; Lyons, W.; Gallagher, D.; Ross, R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J. Appl. Physiol. 1998, 85, 115–122. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Payne, R.B.; Little, A.J.; Williams, R.B.; Milner, J.R. Interpretation of serum calcium in patients with abnormal serum proteins. Br. Med. J. 1973, 4, 643–646. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Seruga, B.; Ocaña, A.; Tannock, I.F.; Amir, E. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [Green Version]
- Ralston, S.H.; Gallacher, S.J.; Patel, U.; Campbell, J.; Boyle, I.T. Cancer-associated hypercalcemia: Morbidity and mortality. Clinical experience in 126 treated patients. Ann. Intern. Med. 1990, 112, 499–504. [Google Scholar] [CrossRef]
- Ramos, R.E.O.; Perez Mak, M.; Alves, M.F.S.; Piotto, G.H.M.; Takahashi, T.K.; Gomes da Fonseca, L.; Silvino, M.C.M.; Hoff, P.M.; de Castro, G., Jr. Malignancy-Related Hypercalcemia in Advanced Solid Tumors: Survival Outcomes. J. Glob. Oncol. 2017, 3, 728–733. [Google Scholar] [CrossRef]
- Motzer, R.J.; Mazumdar, M.; Bacik, J.; Berg, W.; Amsterdam, A.; Ferrara, J. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J. Clin. Oncol. 1999, 17, 2530–2540. [Google Scholar] [CrossRef] [Green Version]
- Manola, J.; Royston, P.; Elson, P.; McCormack, J.B.; Mazumdar, M.; Negrier, S.; Escudier, B.; Eisen, T.; Dutcher, J.; Atkins, M.; et al. Prognostic model for survival in patients with metastatic renal cell carcinoma: Results from the international kidney cancer working group. Clin. Cancer Res. 2011, 17, 5443–5450. [Google Scholar] [CrossRef] [Green Version]
- Lipkin, M. Preclinical and early human studies of calcium and colon cancer prevention. Ann. N. Y. Acad. Sci. 1999, 889, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Wargovich, M.J.; Jimenez, A.; McKee, K.; Steele, V.E.; Velasco, M.; Woods, J.; Price, R.; Gray, K.; Kelloff, G.J. Efficacy of potential chemopreventive agents on rat colon aberrant crypt formation and progression. Carcinogenesis 2000, 21, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarty, S.; Radjendirane, V.; Appelman, H.; Varani, J. Extracellular calcium and calcium sensing receptor function in human colon carcinomas: Promotion of E-cadherin expression and suppression of beta-catenin/TCF activation. Cancer Res. 2003, 63, 67–71. [Google Scholar] [PubMed]
- Kim, H.; Giovannucci, E. Vitamin D Status and Cancer Incidence, Survival, and Mortality. Adv. Exp. Med. Biol. 2020, 1268, 39–52. [Google Scholar] [CrossRef]
- Martin, M.J.; Calvo, N.; de Boland, A.R.; Gentili, C. Molecular mechanisms associated with PTHrP-induced proliferation of colon cancer cells. J. Cell Biochem. 2014, 115, 2133–2145. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.J.; Lee, J.; Anderson, B.; Lee, B.; Migula, D.; Sauer, A.; Chong, N.; Liu, H.; Wu, P.C.; Dash, A.; et al. Whole-body and adipose tissue metabolic phenotype in cancer patients. J. Cachexia Sarcopenia Muscle 2022, 13, 1124–1133. [Google Scholar] [CrossRef]
- Deans, C.; Wigmore, S.; Paterson-Brown, S.; Black, J.; Ross, J.; Fearon, K.C. Serum parathyroid hormone-related peptide is associated with systemic inflammation and adverse prognosis in gastroesophageal carcinoma. Cancer 2005, 103, 1810–1818. [Google Scholar] [CrossRef]
- Sato, K.; Yamakawa, Y.; Shizume, K.; Satoh, T.; Nohtomi, K.; Demura, H.; Akatsu, T.; Nagata, N.; Kasahara, T.; Ohkawa, H.; et al. Passive immunization with anti-parathyroid hormone-related protein monoclonal antibody markedly prolongs survival time of hypercalcemic nude mice bearing transplanted human PTHrP-producing tumors. J. Bone Miner. Res. 1993, 8, 849–860. [Google Scholar] [CrossRef]
- Li, J.; Karaplis, A.C.; Huang, D.C.; Siegel, P.M.; Camirand, A.; Yang, X.F.; Muller, W.J.; Kremer, R. PTHrP drives breast tumor initiation, progression, and metastasis in mice and is a potential therapy target. J. Clin. Investig. 2011, 121, 4655–4669. [Google Scholar] [CrossRef] [Green Version]
- Carriere, P.; Calvo, N.; Novoa Díaz, M.B.; Lopez-Moncada, F.; Herrera, A.; Torres, M.J.; Alonso, E.; Gandini, N.A.; Gigola, G.; Contreras, H.R.; et al. Role of SPARC in the epithelial-mesenchymal transition induced by PTHrP in human colon cancer cells. Mol. Cell Endocrinol. 2021, 530, 111253. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Corrected Calcium, mg/dL | |||||
|---|---|---|---|---|---|
| Characteristic | All Patients, n = 256 | Low Tertile, n = 85 7.18–8.98 | Middle Tertile, n = 81 9.00–9.44 | High Tertile, n = 90 9.46–14.24 | p |
| Age (years), number (%) | |||||
| <55 | 93 (36.3) | 26 (30.6) | 24 (29.6) | 43 (47.8) | 0.039 a |
| 55–70 | 112 (43.8) | 37 (43.5) | 39 (48.2) | 36 (40.0) | |
| >70 | 51 (19.9) | 22 (25.9) | 18 (22.2) | 11 (12.2) | |
| Sex, number (%) | |||||
| Male | 150 (58.6) | 56 (65.9) | 45 (55.6) | 49 (54.4) | 0.246 a |
| Female | 106 (41.4) | 29 (34.1) | 36 (44.4) | 41 (45.6) | |
| BMI (kg/m2), number (%) | |||||
| <18.5 | 24 (9.4) | 7 (8.3) | 5 (6.2) | 12 (13.3) | 0.682 a |
| 18.5–24.9 | 135 (52.7) | 45 (52.9) | 41 (50.6) | 49 (54.4) | |
| 25–29.9 | 63 (24.6) | 22 (25.9) | 22 (27.2) | 19 (21.1) | |
| ≥30 | 34 (13.3) | 11 (12.9) | 13 (16.0) | 10 (11.1) | |
| Weight loss, number (%) | |||||
| <5% | 69 (27) | 30 (35.3) | 21 (25.9) | 18 (20.0) | 0.233 a |
| 5–10% | 39 (15.2) | 10 (11.8) | 13 (16.1) | 16 (17.8) | |
| >10% | 148 (57.8) | 45 (52.9) | 47 (58.0) | 56 (62.2) | |
| Active smoker, number (%) | 116 (45.9) | 40 (47.6) | 38 (47.5) | 38 (42.7) | 0.760 a |
| Active alcohol user, number (%) | 81 (31.9) | 31 (36.5) | 28 (34.6) | 22 (25.0) | 0.222 a |
| Topography, number (%) | |||||
| Left | 208 (81.2) | 70 (82.3) | 68 (84) | 70 (77.8) | 0.558 a |
| Right | 48 (18.8) | 15 (17.7) | 13 (16.0) | 20 (22.2) | |
| ECOG, number (%) | |||||
| 0 | 209 (90.5) | 71 (94.7) | 67 (93.1) | 71 (84.5) | 0.070 b |
| I | 22 (9.5) | 4 (5.3) | 5 (6.9) | 13 (15.5) | |
| II | |||||
| Stage, number (%) | |||||
| I–II | 33 (12.9) | 15 (17.7) | 12 (14.8) | 6 (6.7) | 0.026 b |
| III | 21 (8.2) | 8 (9.4) | 10 (12.3) | 3 (3.3) | |
| IV | 202 (78.9) | 62 (72.9) | 59 (72.8) | 81 (90.0) | |
| Metastasis, number (%) | |||||
| 1 | 143 (55.9) | 54 (63.5) | 44 (54.3) | 45 (50.0) | 0.017 b |
| 2 or more | 104 (40.6) | 26 (30.6) | 33 (40.7) | 45 (50.0) | |
| Local recurrence | 9 (3.5) | 5 (5.9) | 4 (4.9) | 0 (0.0) | |
| CEA (ng/mL), median (IQR) | 30.9 (6.37–157.3) | 20.1 (4.6–74.4) | 26.9 (4.4–122.9) | 87.6 (11.2–406.0) | <0.001 c |
| Prior neoadjuvant or adjuvant treatment, number (%) | 81 (31.6) | 34 (40.0) | 31 (38.3) | 16 (17.8) | 0.002 a |
| Bevacizumab containing regimen, number (%) | 53 (27.0) | 14 (21.9) | 20 (33.9) | 19 (26.0) | 0.315 a |
| Backbone chemotherapy regimen, number (%) | |||||
| Oxaliplatin | 62 (32.8) | 25 (40.3) | 21 (36.2) | 16 (23.2) | 0.016 a |
| Irinotecan | 105 (55.6) | 33 (53.2) | 34 (58.6) | 38 (55.1) | |
| 5-Fluorouracil | 22 (11.6) | 4 (6.5) | 3 (5.2) | 15 (21.7) | |
| Corrected Calcium, mg/dL [HR (95% CI)] | ||||
|---|---|---|---|---|
| Low Calcium | Middle Calcium | High Calcium | p | |
| (7.18–8.98) | (9.00–9.44) | (9.46–14.24) | ||
| Progression-free survival | ||||
| Number of events/at risk | 68/85 | 74/81 | 84/90 | |
| Unadjusted | Referent | 1.27 (0.91–1.76) | 1.94 (1.41–2.69) | <0.001 |
| Adjusted a | Referent | 1.17 (0.80–1.71) | 1.85 (1.27–2.69) | 0.001 |
| Overall survival | ||||
| Number of events/at risk | 63/85 | 67/81 | 77/90 | |
| Unadjusted | Referent | 1.44 (1.02–2.04) | 1.98 (1.41–2.79) | <0.001 |
| Adjusted a | Referent | 1.16 (0.78–1.74) | 1.86 (1.26–2.74) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silveira, M.N.; Pozzuto, L.; Mendes, M.C.S.; da Cunha, L.P.; Costa, F.O.; Macedo, L.T.; Brambilla, S.R.; Carvalheira, J.B.C. Association of Albumin-Corrected Serum Calcium Levels with Colorectal Cancer Survival Outcomes. J. Clin. Med. 2022, 11, 2928. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102928
Silveira MN, Pozzuto L, Mendes MCS, da Cunha LP, Costa FO, Macedo LT, Brambilla SR, Carvalheira JBC. Association of Albumin-Corrected Serum Calcium Levels with Colorectal Cancer Survival Outcomes. Journal of Clinical Medicine. 2022; 11(10):2928. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102928
Chicago/Turabian StyleSilveira, Marina Nogueira, Lara Pozzuto, Maria Carolina Santos Mendes, Lorena Pires da Cunha, Felipe Osório Costa, Lígia Traldi Macedo, Sandra Regina Brambilla, and José Barreto Campello Carvalheira. 2022. "Association of Albumin-Corrected Serum Calcium Levels with Colorectal Cancer Survival Outcomes" Journal of Clinical Medicine 11, no. 10: 2928. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102928