
Renin-Angiotensin-System Inhibitors for the Prevention of Chemotherapy-Induced Peripheral Neuropathy: OncoToxSRA, a Preliminary Cohort Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Outcomes
2.3. Statistical Methods
3. Results
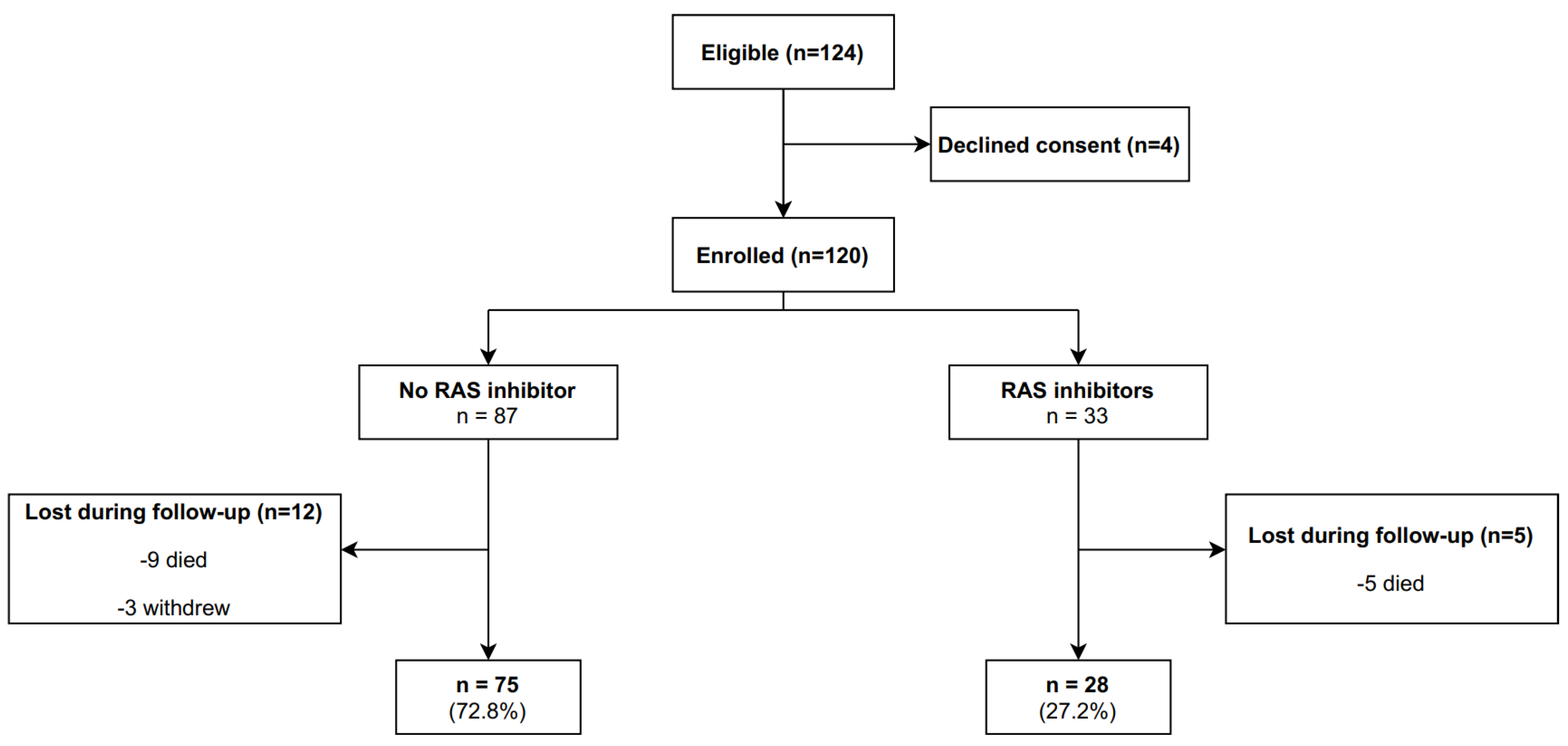
3.1. Patients
3.2. Outcomes
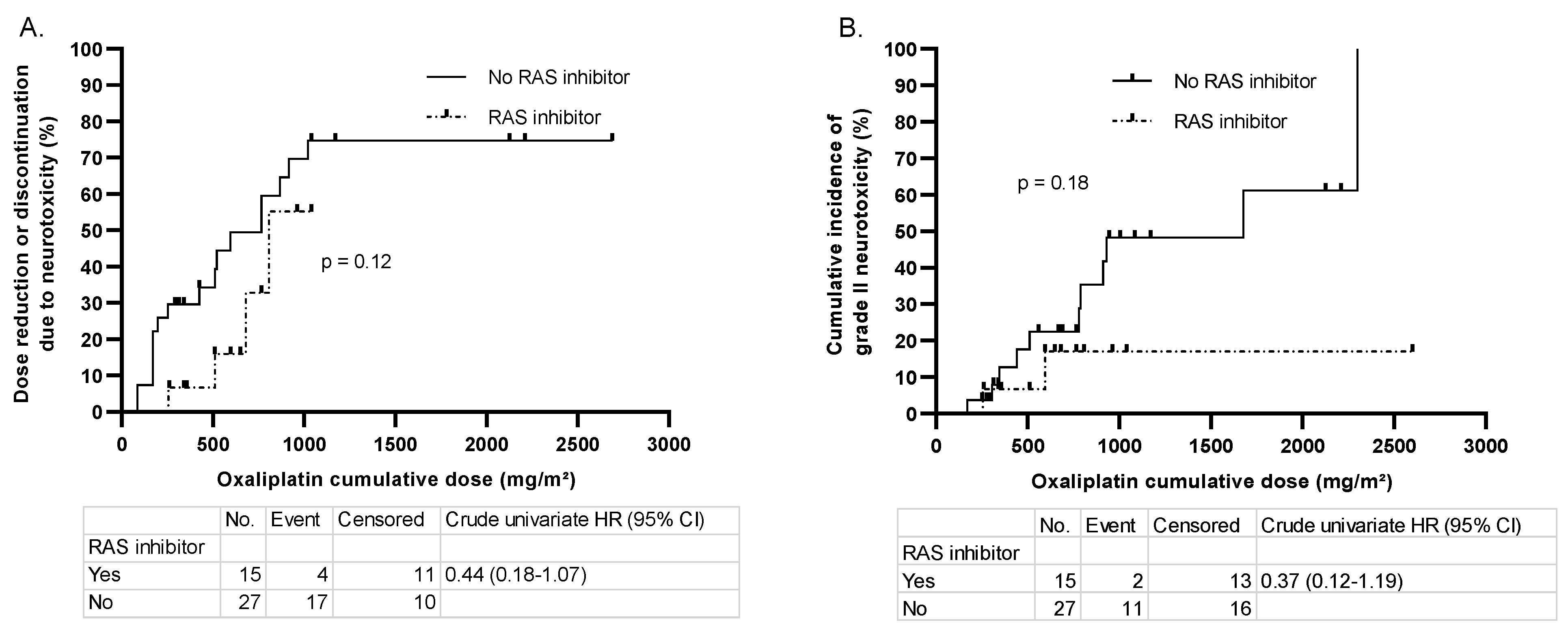
3.3. Oxaliplatin Cumulative Dose to Event
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, Prevalence, and Predictors of Chemotherapy-Induced Peripheral Neuropathy: A Systematic Review and Meta-Analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staff, N.P.; Cavaletti, G.; Islam, B.; Lustberg, M.; Psimaras, D.; Tamburin, S. Platinum-induced Peripheral Neurotoxicity: From Pathogenesis to Treatment. J. Peripher. Nerv. Syst. 2019, 24, S26–S39. [Google Scholar] [CrossRef] [PubMed]
- Tamburin, S.; Park, S.B.; Alberti, P.; Demichelis, C.; Schenone, A.; Argyriou, A.A. Taxane and Epothilone-induced Peripheral Neurotoxicity: From Pathogenesis to Treatment. J. Peripher. Nerv. Syst. 2019, 24, S40–S51. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Bruna, J.; Park, S.B.; Cavaletti, G. Emerging Pharmacological Strategies for the Management of Chemotherapy-Induced Peripheral Neurotoxicity (CIPN), Based on Novel CIPN Mechanisms. Expert Rev. Neurother. 2020, 20, 1005–1016. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [Green Version]
- Argyriou, A.A.; Cavaletti, G.; Park, S.B.; on behalf of the Toxic Neuropathy Consortium (TNC). The Toxic Neuropathy Consortium of the Peripheral Nerve Society. J. Peripher. Nerv. Syst. 2019, 24, S4–S5. [Google Scholar] [CrossRef]
- Paul, M.; Mehr, A.P.; Kreutz, R. Physiology of Local Renin-Angiotensin Systems. Physiol. Rev. 2006, 86, 747–803. [Google Scholar] [CrossRef]
- Anand, U.; Yiangou, Y.; Sinisi, M.; Fox, M.; MacQuillan, A.; Quick, T.; Korchev, Y.E.; Bountra, C.; McCarthy, T.; Anand, P. Mechanisms Underlying Clinical Efficacy of Angiotensin II Type 2 Receptor (AT2R) Antagonist EMA401 in Neuropathic Pain: Clinical Tissue and in Vitro Studies. Mol. Pain 2015, 11, s12990-015. [Google Scholar] [CrossRef] [Green Version]
- Danigo, A.; Rovini, A.; Bessaguet, F.; Bouchenaki, H.; Bernard, A.; Sturtz, F.; Bourthoumieu, S.; Desmoulière, A.; Magy, L.; Demiot, C. The Angiotensin II Type 2 Receptor, a Target for Protection and Regeneration of the Peripheral Nervous System? Pharmaceuticals 2021, 14, 175. [Google Scholar] [CrossRef]
- Bessaguet, F.; Magy, L.; Desmoulière, A.; Demiot, C. The Therapeutic Potential of Renin Angiotensin Aldosterone System (RAAS) in Chronic Pain: From Preclinical Studies to Clinical Trials. Expert Rev. Neurother. 2016, 16, 331–339. [Google Scholar] [CrossRef]
- Yuksel, T.N.; Halici, Z.; Demir, R.; Cakir, M.; Calikoglu, C.; Ozdemir, G.; Unal, D. Investigation of the Effect of Telmisartan on Experimentally Induced Peripheral Nerve Injury in Rats. Int. J. Neurosci. 2014, 125, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Hashikawa-Hobara, N.; Hashikawa, N.; Inoue, Y.; Sanda, H.; Zamami, Y.; Takatori, S.; Kawasaki, H. Candesartan Cilexetil Improves Angiotensin II Type 2 Receptor-Mediated Neurite Outgrowth via the PI3K-Akt Pathway in Fructose-Induced Insulin-Resistant Rats. Diabetes 2012, 61, 925–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bessaguet, F.; Danigo, A.; Magy, L.; Sturtz, F.; Desmoulière, A.; Demiot, C. Candesartan Prevents Resiniferatoxin-Induced Sensory Small-Fiber Neuropathy in Mice by Promoting Angiotensin II-Mediated AT2 Receptor Stimulation. Neuropharmacology 2017, 126, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Bessaguet, F.; Danigo, A.; Bouchenaki, H.; Duchesne, M.; Magy, L.; Richard, L.; Sturtz, F.; Desmoulière, A.; Demiot, C. Neuroprotective Effect of Angiotensin II Type 2 Receptor Stimulation in Vincristine-Induced Mechanical Allodynia. Pain 2018, 159, 2538–2546. [Google Scholar] [CrossRef] [PubMed]
- Bouchenaki, H.; Danigo, A.; Bernard, A.; Bessaguet, F.; Richard, L.; Sturtz, F.; Balayssac, D.; Magy, L.; Demiot, C. Ramipril Alleviates Oxaliplatin-Induced Acute Pain Syndrome in Mice. Front. Pharmacol. 2021, 12, 712442. [Google Scholar] [CrossRef]
- Kim, E.; Hwang, S.-H.; Kim, H.-K.; Abdi, S.; Kim, H.K. Losartan, an Angiotensin II Type 1 Receptor Antagonist, Alleviates Mechanical Hyperalgesia in a Rat Model of Chemotherapy-Induced Neuropathic Pain by Inhibiting Inflammatory Cytokines in the Dorsal Root Ganglia. Mol. Neurobiol. 2019, 56, 7408–7419. [Google Scholar] [CrossRef]
- Malik, R.A.; Williamson, S.; Abbott, C.; Carrington, A.L.; Iqbal, J.; Schady, W.; Boulton, A.J. Effect of Angiotensin-Converting-Enzyme (ACE) Inhibitor Trandolapril on Human Diabetic Neuropathy: Randomised Double-Blind Controlled Trial. Lancet 1998, 352, 1978–1981. [Google Scholar] [CrossRef]
- Roldan, C.J.; Song, J.; Engle, M.P.; Dougherty, P.M. Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Modulate the Function of Myelinated Fibers after Chemotherapy: A Quantitative Sensory Testing Study. Pain Physician 2017, 20, 281–292. [Google Scholar] [CrossRef]
- Uchida, M.; Kawazoe, H.; Takatori, S.; Namba, H.; Uozumi, R.; Tanaka, A.; Kawasaki, H.; Araki, H. Preventive Effects of Renin-Angiotensin System Inhibitors on Oxaliplatin-Induced Peripheral Neuropathy: A Retrospective Observational Study. Clin. Therm. 2018, 40, 1214–1222.e1. [Google Scholar] [CrossRef]
- Gebremedhn, E.G.; Shortland, P.J.; Mahns, D.A. The Incidence of Acute Oxaliplatin-Induced Neuropathy and Its Impact on Treatment in the First Cycle: A Systematic Review. BMC Cancer 2018, 18, 410. [Google Scholar] [CrossRef] [Green Version]
- Bouhassira, D.; Attal, N.; Fermanian, J.; Alchaar, H.; Gautron, M.; Masquelier, E.; Rostaing, S.; LanteriMinet, M.; Collin, E.; Grisart, J.; et al. Development and Validation of the Neuropathic Pain Symptom Inventory. Pain 2004, 108, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Binda, D.; Vanhoutte, E.K.; Cavaletti, G.; Cornblath, D.R.; Postma, T.J.; Frigeni, B.; Alberti, P.; Bruna, J.; Velasco, R.; Argyriou, A.A.; et al. Rasch-Built Overall Disability Scale for Patients with Chemotherapy-Induced Peripheral Neuropathy (CIPN-R-ODS). Eur. J. Cancer 2013, 49, 2910–2918. [Google Scholar] [CrossRef] [PubMed]
- Saad, M.; Psimaras, D.; Tafani, C.; Sallansonnet-Froment, M.; Calvet, J.-H.; Vilier, A.; Tigaud, J.-M.; Bompaire, F.; Lebouteux, M.; de Greslan, T.; et al. Quick, Non-Invasive and Quantitative Assessment of Small Fiber Neuropathy in Patients Receiving Chemotherapy. J. Neuro Oncol. 2016, 127, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Staff, N.P.; Grisold, A.; Grisold, W.; Windebank, A.J. Chemotherapy-induced Peripheral Neuropathy: A Current Review. Ann. Neurol. 2017, 81, 772–781. [Google Scholar] [CrossRef]
- Timmins, H.C.; Li, T.; Goldstein, D.; Trinh, T.; Mizrahi, D.; Harrison, M.; Horvath, L.G.; Friedlander, M.; Kiernan, M.C.; Park, S.B. The Impact of Obesity on Neuropathy Outcomes for Paclitaxel- and Oxaliplatin-Treated Cancer Survivors. J. Cancer Surviv. 2021, 16, 223–232. [Google Scholar] [CrossRef]
- Mizrahi, D.; Park, S.B.; Li, T.; Timmins, H.C.; Trinh, T.; Au, K.; Battaglini, E.; Wyld, D.; Henderson, R.D.; Grimison, P.; et al. Hemoglobin, Body Mass Index, and Age as Risk Factors for Paclitaxel- and Oxaliplatin-Induced Peripheral Neuropathy. JAMA Netw. Open 2021, 4, e2036695. [Google Scholar] [CrossRef]
- Weber, M.A. Interrupting the Renin-Angiotensin System: The Role of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Ii Receptor Antagonists in the Treatment of Hypertension. Am. J. Hypertens. 1999, 12, 189S–194S. [Google Scholar] [CrossRef]
- Gu, J.; Lu, H.; Chen, C.; Gu, Z.; Hu, M.; Liu, L.; Yu, J.; Wei, G.; Huo, J. Diabetes Mellitus as a Risk Factor for Chemotherapy-Induced Peripheral Neuropathy: A Meta-Analysis. Support Care Cancer 2021, 29, 7461–7469. [Google Scholar] [CrossRef]
- Landsberg, L.; Molitch, M. Diabetes and Hypertension: Pathogenesis, Prevention and Treatment. Clin. Exp. Hypertens. 2004, 26, 621–628. [Google Scholar] [CrossRef]
- Ponirakis, G.; Petropoulos, I.N.; Alam, U.; Ferdousi, M.; Asghar, O.; Marshall, A.; Azmi, S.; Jeziorska, M.; Mahfoud, Z.R.; Boulton, A.J.M.; et al. Hypertension Contributes to Neuropathy in Patients with Type 1 Diabetes. Am. J. Hypertens. 2019, 32, 796–803. [Google Scholar] [CrossRef]
- Dumas, G.; Canet, E. Effets Cardiovasculaires Graves Des Chimiothérapies, Thérapies Ciblées et Des Traitements Immunosuppresseurs. Réanimation 2016, 25, 123–136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | No RAS Inhibitor (n = 87) | RAS Inhibitor (n = 33) | p-Values |
|---|---|---|---|
| Patients | |||
| Age in years median (range) | 63 (25–86) | 69 (49–81) | 0.024 * |
| Gender (M/F) (%) | 49/51 | 58/42 | 0.553 |
| Body mass index (kg/m²) | 24 | 28.7 | 0.004 ** |
| Diabetes mellitus (%) | 6 | 18 | 0.069 |
| Alcohol consumption (%) | 26 | 24 | 0.991 |
| Hypertension (%) | 26 | 100 | <0.001 *** |
| Performance Status | 0 (0–2) | 0 (0–2) | 0.221 |
| Cancer | |||
| Localization | 0.317 | ||
| Gastrointestinal (%) | 38 | 55 | |
| Gynecologic (%) | 32 | 27 | |
| ORL (%) | 18 | 15 | |
| Urogenital (%) | 12 | 3 | |
| Classification/Line of therapy | 0.907 | ||
| Adjuvant (%) | 56 | 58 | |
| Metastatic (%) | 35 | 36 | |
| Neoadjuvant (%) | 9 | 6 | |
| Chemotherapy and cumulative dose | |||
| Platinum-based (%) | 68.9 | 75.9 | 0.661 |
| Carboplatin (%) | 4.6 | 15.2 | 0.112 |
| Cumulative dose (AUC) | 30 (23.75–33.12) | 30 (30–30) | 0.893 |
| Cisplatin (%) | 31 | 15.2 | 0.105 |
| Cumulative dose (mg/m²) | 660 (562.71–900) | 473.6 (300–675) | 0.183 |
| Oxaliplatin (%) | 33.3 | 45.5 | 0.289 |
| Cumulative dose (mg/m²) | 916.5 (429.6–1152) | 595 (347.8–786) | 0.125 |
| Taxane-based (%) | 37.8 | 30.4 | 0.670 |
| Cabazitaxel (%) | 1.1 | 0 | 1.000 |
| Cumulative dose (mg/m²) | 250 (250–250) | NA | NA |
| Docetaxel (%) | 26.4 | 15.2 | 0.233 |
| Cumulative dose (mg/m²) | 400 (252.1–425.6) | 300 (225.5–400) | 0.880 |
| Paclitaxel (%) | 10.3 | 15.2 | 0.527 |
| Cumulative dose (mg/m²) | 1142.3 (465.6–1840) | 783.8 (700–1304.2) | 0.519 |
| Neurotoxic association (%) | 10.3 | 15.2 | 0.344 |
| Neurotoxic chemotherapy duration (days) | 107 (45–156) | 95.5 (62.3–137) | 0.785 |
| Scores at baseline | |||
| NCI-CTC 4.0 grade (0–4) | 0 (0–0) | 0 (0–0) | |
| mean | 0 | 0.061 | 0.022 * |
| NPSI (0–100) | 0 (0–0) | 0 (0–0) | 0.195 |
| CIPN-RODS (0–100) | 84 (73–100) | 73 (67–87) | 0.010 * |
| EQ5D5L (5–25) | 7 (5.5–9) | 9 (7–10) | 0.066 |
| ESC (µS) | |||
| Hands | 71 (56–81) | 65 (51–80) | 0.486 |
| Feet | 77 (66–82) | 74 (54–83) | 0.525 |
| RAS Inhibitors | Daily Dose (mg) |
|---|---|
| ARB (n = 16) | |
| Irbesartan (n = 11) | 150 (150–300) |
| Candesartan (n = 3) | 8 (4–16) |
| Losartan (n = 1) | 50 |
| Telmisartan (n = 1) | 80 |
| ACE inhibitor (n = 17) | |
| Perindopril (n = 7) | 4.5 (2.5–10) |
| Ramipril (n = 6) | 5 (1.25–5) |
| Enalapril (n = 4) | 12.5 (10–20) |
| Platinum-Based | Taxanes | |||||
|---|---|---|---|---|---|---|
| Variables | No RAS Inhibitor (n = 52) | RAS Inhibitor (n = 23) | p-Values | No RAS Inhibitor (n = 29) | RAS Inhibitor (n = 8) | p-Values |
| NCI-CTC 4.0 | 0.7 (0–1) | 0.4 (0–1) | 0.047 * | 0.8 (0–1) | 0.9 (0–1.3) | 0.853 |
| NPSI | 6.8 (0–12.3) | 4.3 (0–7.5) | 0.225 | 6.3 (0–8) | 15 (0–25.3) | 0.734 |
| CIPN-RODS | 79.4 (72.8–94) | 76.7 (68.5–84) | 0.503 | 79 (70–94) | 73.5 (69.8–76) | 0.072 |
| EQ5D5L | 8.7 (6–9.3) | 8 (6–9) | 0.337 | 8.7 (6–10) | 8.8 (8–9.3) | 0.456 |
| ESC (µS) | ||||||
| Hands | 63.3 (58–79) | 66.7 (60–80) | 0.508 | 68.7 (65.5–78.3) | 72.6 (71.5–80.5) | 0.132 |
| Feet | 65.5 (52–81) | 71.1 (61–86) | 0.289 | 74.2 (70.5–81.8) | 67.6 (57.3–84.5) | 0.670 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frachet, S.; Danigo, A.; Labriffe, M.; Bessaguet, F.; Quinchard, B.; Deny, N.; Baffert, K.-A.; Deluche, E.; Sturtz, F.; Demiot, C.; et al. Renin-Angiotensin-System Inhibitors for the Prevention of Chemotherapy-Induced Peripheral Neuropathy: OncoToxSRA, a Preliminary Cohort Study. J. Clin. Med. 2022, 11, 2939. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102939
Frachet S, Danigo A, Labriffe M, Bessaguet F, Quinchard B, Deny N, Baffert K-A, Deluche E, Sturtz F, Demiot C, et al. Renin-Angiotensin-System Inhibitors for the Prevention of Chemotherapy-Induced Peripheral Neuropathy: OncoToxSRA, a Preliminary Cohort Study. Journal of Clinical Medicine. 2022; 11(10):2939. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102939
Chicago/Turabian StyleFrachet, Simon, Aurore Danigo, Marc Labriffe, Flavien Bessaguet, Bianca Quinchard, Nicolas Deny, Kim-Arthur Baffert, Elise Deluche, Franck Sturtz, Claire Demiot, and et al. 2022. "Renin-Angiotensin-System Inhibitors for the Prevention of Chemotherapy-Induced Peripheral Neuropathy: OncoToxSRA, a Preliminary Cohort Study" Journal of Clinical Medicine 11, no. 10: 2939. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102939