
Nasolabial Appearance in 5-Year-Old Patients with Repaired Complete Unilateral Cleft Lip and Palate: A Comparison of Two Different Techniques of Lip Repair

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
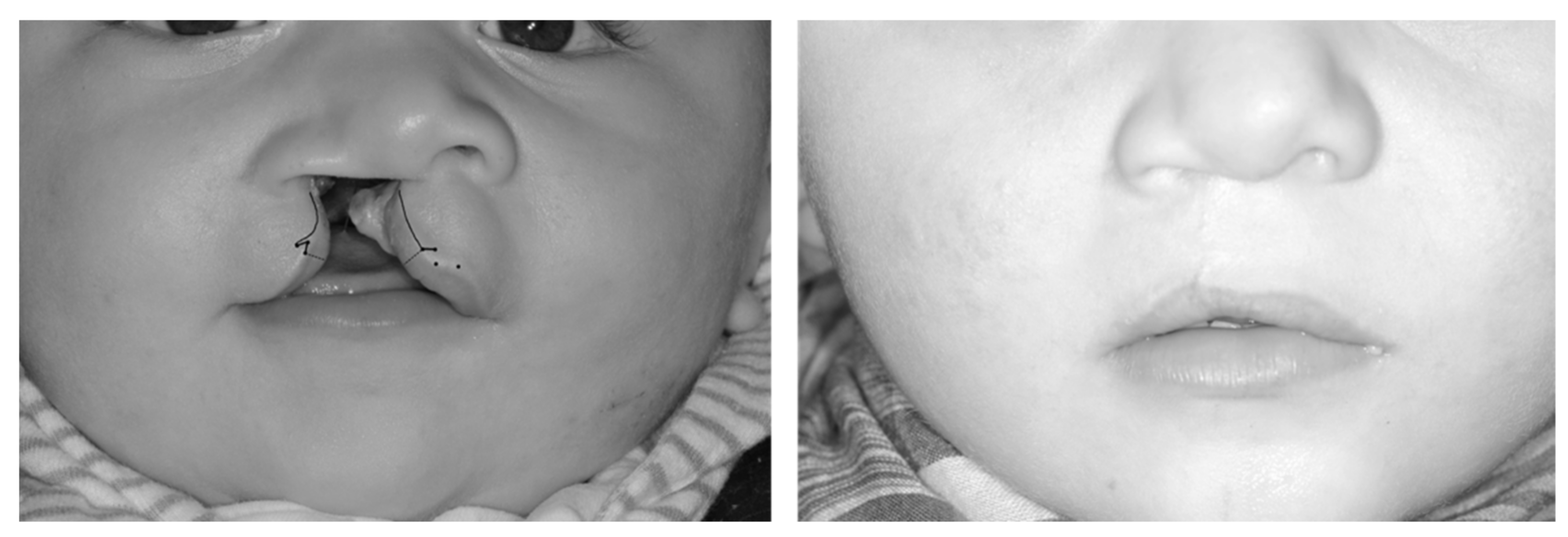
2.2. Surgical Technique
2.2.1. Pfeifer’s “Wave-Line Technique”
2.2.2. Randall’s “Triangular Flap” Technique
2.2.3. Surgeons
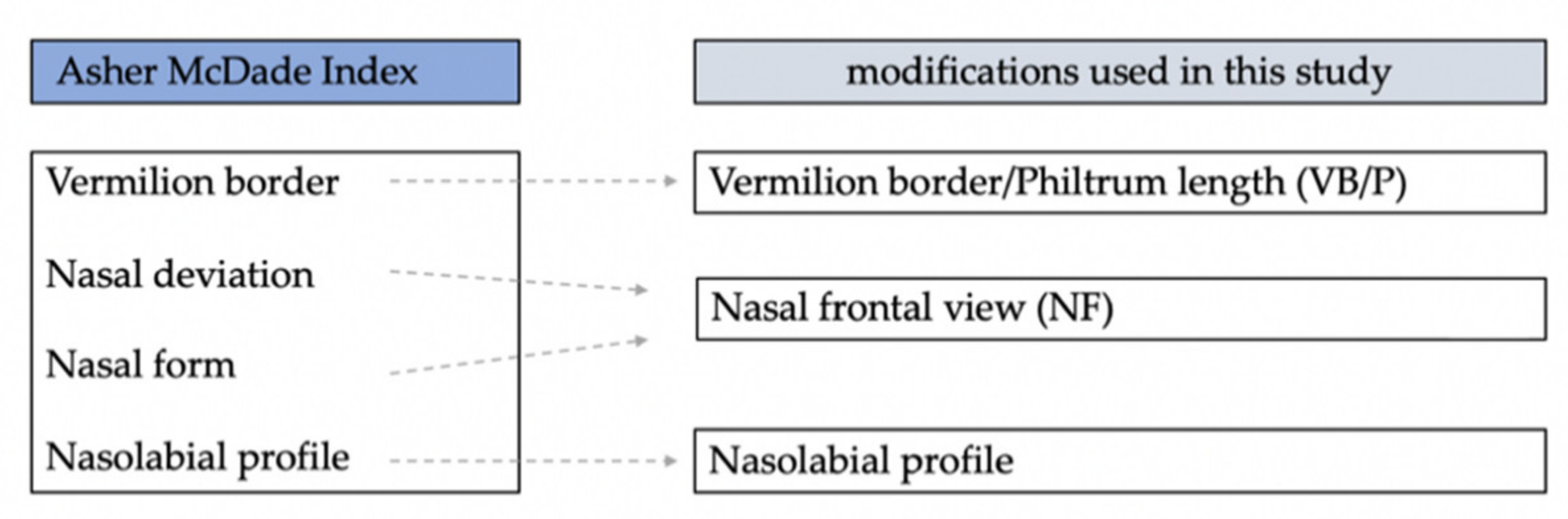
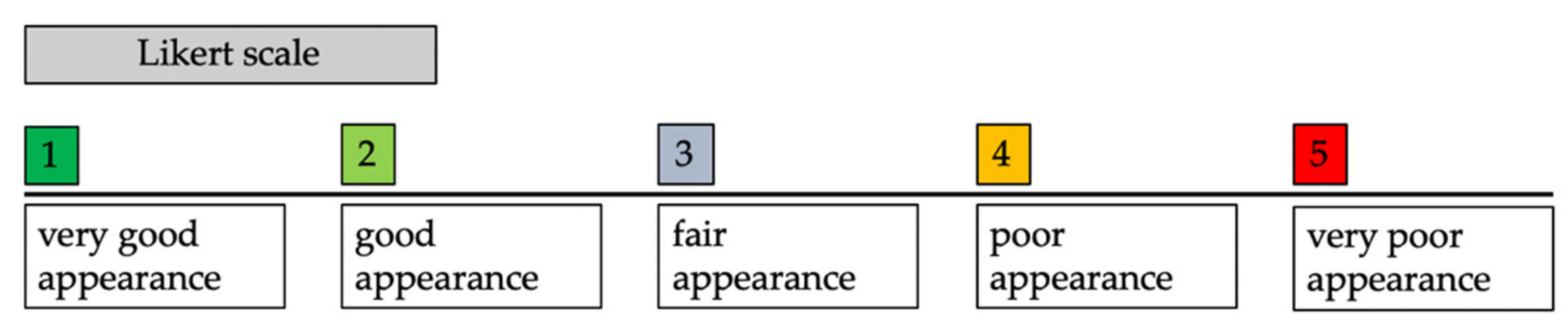
2.3. Aesthetic Outcome Assessment
2.3.1. Nasal Frontal View (NF)
2.3.2. Vermilion Border/Philtrum Length (VB/P)
2.3.3. Nasolabial Profile (NLP)
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Inter-Rater and Intra-Rater Reliability
3.3. Aesthetic Score
3.3.1. Vermilion Border and Philtrum Length (VB/P)
3.3.2. Nasal Frontal View (NF)
3.3.3. Nasolabial Profile (NLP)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canfield, M.A.; Honein, M.A.; Yuskiv, N.; Xing, J.; Mai, C.T.; Collins, J.S.; Devine, O.; Petrini, J.; Ramadhani, T.A.; Hobbs, C.A.; et al. National estimates and race/ethnic-specific variation of selected birth defects in the United States, 1999–2001. Birth Defects Res. Part A Clin. Mol. Teratol. 2006, 76, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Little, J.; Cardy, A.; Munger, R.G. Tobacco smoking and oral clefts: A meta-analysis. Bull. World Health Organ. 2004, 82, 213–218. [Google Scholar] [PubMed]
- Mossey, P.A.; Castilla, E. Global Registry and Database on Craniofacial Anomalies; Report of a WHO Registry Meeting on Craniofacial Anomalies; WHO: Geneva, Switzerland, 2003; Available online: https://apps.who.int/iris/bitstream/handle/10665/42840/9241591102.pdf?sequence=1&isAllowed=y (accessed on 29 March 2022).
- Rahimov, F.; Jugessur, A.; Murray, J.C. Genetics of nonsyndromic orofacial clefts. Cleft Palate-Craniofac. J. 2012, 49, 73–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francisco, I.; Caramelo, F.; Fernandes, M.H.; Vale, F. Parental Risk Factors and Child Birth Data in a Matched Year and Sex Group Cleft Population: A Case-Control Study. Int. J. Environ. Res. Public Health 2021, 18, 4615. [Google Scholar] [CrossRef]
- Christensen, K.; Juel, K.; Herskind, A.M.; Murray, J.C. Long term follow up study of survival associated with cleft lip and palate at birth. BMJ 2004, 328, 1405. [Google Scholar] [CrossRef] [Green Version]
- Hunt, O.; Burden, D.; Hepper, P.; Johnston, C. The psychosocial effects of cleft lip and palate: A systematic review. Eur. J. Orthod. 2005, 27, 274–285. [Google Scholar] [CrossRef] [Green Version]
- McDowell, F. The classic reprint: Du bec-de-lièvre (new method for the harelip operation) Dr. J.F. Malgaigne, Paris, France, (J. de Chir. de Paris, 2: 1-6, 1844). Plast. Reconstr. Surg. 1976, 57, 359–366. [Google Scholar]
- Pfeifer, G. Über ein entwicklungsgeschichtlich begründetes Verfahren des Verschlusses von Lippenspalten. Dtsch Zahn Mund Kieferheilkd 1970, 54, 69–77. [Google Scholar]
- Millard, D. Complete Unilateral Clefts of the Lip. Plast. Reconstr. Surg. 1960, 25, 595–605. [Google Scholar] [CrossRef]
- Millard, D.R. Extensions of the rotation-advancement principle for wide unilateral cleft lips. Plast. Reconstr. Surg. 1968, 42, 535–544. [Google Scholar] [CrossRef]
- Tennison, C.W. The repair of the unilateral cleft lip by the stencil method. Plast. Reconstr. Surg. 1952, 9, 115–120. [Google Scholar] [CrossRef]
- Randall, P. A triangular flap operation for the primary repair of unilateral clefts of the lip. Plast. Reconstr. Surg. Transplant. Bull. 1959, 23, 331–347. [Google Scholar] [CrossRef]
- Fisher, D.M. Unilateral cleft lip repair: An anatomical subunit approximation technique. Plast. Reconstr. Surg. 2005, 116, 61–71. [Google Scholar] [CrossRef]
- Al-Omari, I.; Millett, D.T.; Ayoub, A.F. Methods of assessment of cleft-related facial deformity: A review. Cleft Palate-Craniofac. J. 2005, 42, 145–156. [Google Scholar] [CrossRef]
- Sharma, V.P.; Bella, H.; Cadier, M.M.; Pigott, R.W.; Goodacre, T.E.; Richard, B.M. Outcomes in facial aesthetics in cleft lip and palate surgery. A systematic review. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1233–1245. [Google Scholar] [CrossRef]
- Mosmuller, D.G.M.; Don Griot, J.P.W.; Bijnen, C.L.; Niessen, F.B. Scoring systems of cleft-related facial deformities: A review of literature. Cleft Palate Craniofac J. 2013, 50, 286–296. [Google Scholar] [CrossRef]
- Mosmuller, D.G.M.; Maal, T.J.; Prahl, C.; Tan, R.A.; Mulder, F.J.; Schwirtz, R.M.F.; de Vet, H.C.W.; Bergé, S.J.; Don Griot, J.P.W. Comparison of two- and three-dimensional assessment methods of nasolabial appearance in cleft lip and palate patients: Do the assessment methods measure the same outcome? J. Craniomaxillofac. Surg. 2017, 45, 1220–1226. [Google Scholar] [CrossRef]
- Asher-McDade, C.; Roberts, C.; Shaw, W.C.; Gallager, C. Development of a method for rating nasolabial appearance in patients with clefts of the lip and palate. Cleft Palate-Craniofac. J. 1991, 28, 385–391. [Google Scholar] [CrossRef]
- Hotz, M.M. Pre- and early postoperative growth-guidance in cleft lip and palate cases by maxillary orthopedics (an alternative procedure to primary bone-grafting). Cleft Palate J. 1969, 6, 368–372. [Google Scholar]
- Brusati, R.; Meazzini, M.C.; Rezzonico, A.; Biglioli, F.; Garattini, G.; Battista, V.M.; Autelitano, L. Evaluation of a Sample of Patients with Unilateral Cleft Lip and Palate Treated with a Two-Stage Protocol. J. Craniofac. Surg. 2018, 29, 2058–2064. [Google Scholar] [CrossRef]
- Mosmuller, D.G.; Mennes, L.M.; Prahl, C.; Kramer, G.J.; Disse, M.A.; Van Couwelaar, G.M.; Frank, B.N.; Don Griot, J.P. The development of the cleft aesthetic rating scale: A new rating scale for the assessment of nasolabial appearance in complete unilateral cleft lip and palate patients. Cleft Palate-Craniofac. J. 2017, 54, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Lorot-Marchand, A.; Guerreschi, P.; Pellerin, P.; Martinot, V.; Gbaguidi, C.C.; Neiva, C.; Devauchelle, B.; Frochisse, C.; Poli-Merol, M.L.; Francois-Fiquet, C. Frequency and socio-psychological impact of taunting in school-age patients with cleft lip-palate surgical repair. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Kramer, F.J.; Gruber, R.; Fialka, F.; Sinikovic, B.; Schliephake, H. Quality of Life and Family Functioning in Children with Nonsyndromic Orofacial Clefts at Preschool Ages. J. Craniofac. Surg. 2008, 19, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Broder, H.L.; Smith, F.B.; Strauss, R.P. Habilitation of patients with clefts: Parent and child ratings of satisfaction with appearance and speech. Cleft Palate-Craniofac. J. 1992, 29, 262–267. [Google Scholar] [CrossRef]
- Patel, T.A.; Patel, K.G. Comparison of the Fisher Anatomical Subunit and Modified Millard Rotation-Advancement Cleft Lip Repairs. Plast Reconstr. Surg. 2019, 144, 238–245. [Google Scholar] [CrossRef]
- Rossell-Perry, P. A 20-year experience in unilateral cleft lip repair: From Millard to the triple unilimb Z-plasty technique. Indian J. Plast. Surg. 2016, 49, 340–349. [Google Scholar] [CrossRef]
- Gundlach, K.K.; Schmitz, R.; Maerker, R.; Bull, H.G. Late results following different methods of cleft lip repair. Cleft Palate J. 1982, 19, 167–171. [Google Scholar]
- Zhu, S.; Jayaraman, J.; Khambay, B. Evaluation of facial appearance in patients with cleft lip and palate by laypeople and professionals: A systematic literature review. Cleft Palate Craniofac. J. 2016, 53, 187–196. [Google Scholar] [CrossRef]
- Schwaiger, M.; Edmondson, S.J.; Wallner, J.; Mischak, I.; Echlin, K.; Paddle, A.; Atherton, D. Influence of different techniques of secondary cleft lip revision surgery on upper lip projection. Int. J. Oral. Maxillofac. Surg. 2020, 49, 726–733. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ‘Pfeifer’ Group | ‘Randall’ Group | |
|---|---|---|
| Number | 28 | 25 |
| Sex | m: 16 f: 12 | m: 14 f: 14 |
| Average age at lip repair (months) | 6.4 (±1.4) | 6.0 (±1.4) |
| Minimum/maximum age at lip repair (months) | 4.7–7.9 | 4.3–7.7 |
| Average age at photograph (months) | 60.6 (±1.9) | 60.8 (±2.0) |
| Cleft side | r: 12; l: 16 | r: 13; l: 12 |
| Parameters | ‘Pfeifer’ Group | ‘Randall’ Group | Mean Diff. | p-Values | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | SD | 95% CI | Min | Max | Mean | SD | 95% CI | |||
| NF | 1.20 | 4.00 | 2.64 | 0.71 | [2.30–2.88] | 1.00 | 3.20 | 2.42 | 0.57 | [2.18–2.65] | 0.22 | p = 0.219 |
| VB/P | 1.00 | 4.30 | 2.51 | 0.92 | [2.10–2.87] | 1.00 | 4.00 | 2.03 | 0.77 | [1.71–2.35] | 0.48 | p = 0.046 |
| NLP | 1.30 | 4.20 | 2.50 | 0.67 | [2.23–2.77] | 1.30 | 4.40 | 2.54 | 0.83 | [2.19–2.88] | −0.03 | p = 0.880 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lux, S.; Mayr, M.; Schwaiger, M.; Edmondson, S.-J.; Steiner, C.; Schachner, P.; Gaggl, A. Nasolabial Appearance in 5-Year-Old Patients with Repaired Complete Unilateral Cleft Lip and Palate: A Comparison of Two Different Techniques of Lip Repair. J. Clin. Med. 2022, 11, 2943. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102943
Lux S, Mayr M, Schwaiger M, Edmondson S-J, Steiner C, Schachner P, Gaggl A. Nasolabial Appearance in 5-Year-Old Patients with Repaired Complete Unilateral Cleft Lip and Palate: A Comparison of Two Different Techniques of Lip Repair. Journal of Clinical Medicine. 2022; 11(10):2943. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102943
Chicago/Turabian StyleLux, Sonja, Matthias Mayr, Michael Schwaiger, Sarah-Jayne Edmondson, Christoph Steiner, Peter Schachner, and Alexander Gaggl. 2022. "Nasolabial Appearance in 5-Year-Old Patients with Repaired Complete Unilateral Cleft Lip and Palate: A Comparison of Two Different Techniques of Lip Repair" Journal of Clinical Medicine 11, no. 10: 2943. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102943