
Atrial Fibrillation Global Changes after Pulmonary Vein and Posterior Wall Isolation: A Charge Density Mapping Study

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Procedure
2.3. Pulmonary Vein Isolation and Left Atrial Posterior Wall Isolation with Cryoballoon
2.4. Non-Contact Charge Density Mapping
2.5. Statistical Analysis
3. Results
3.1. Study Population Characteristics
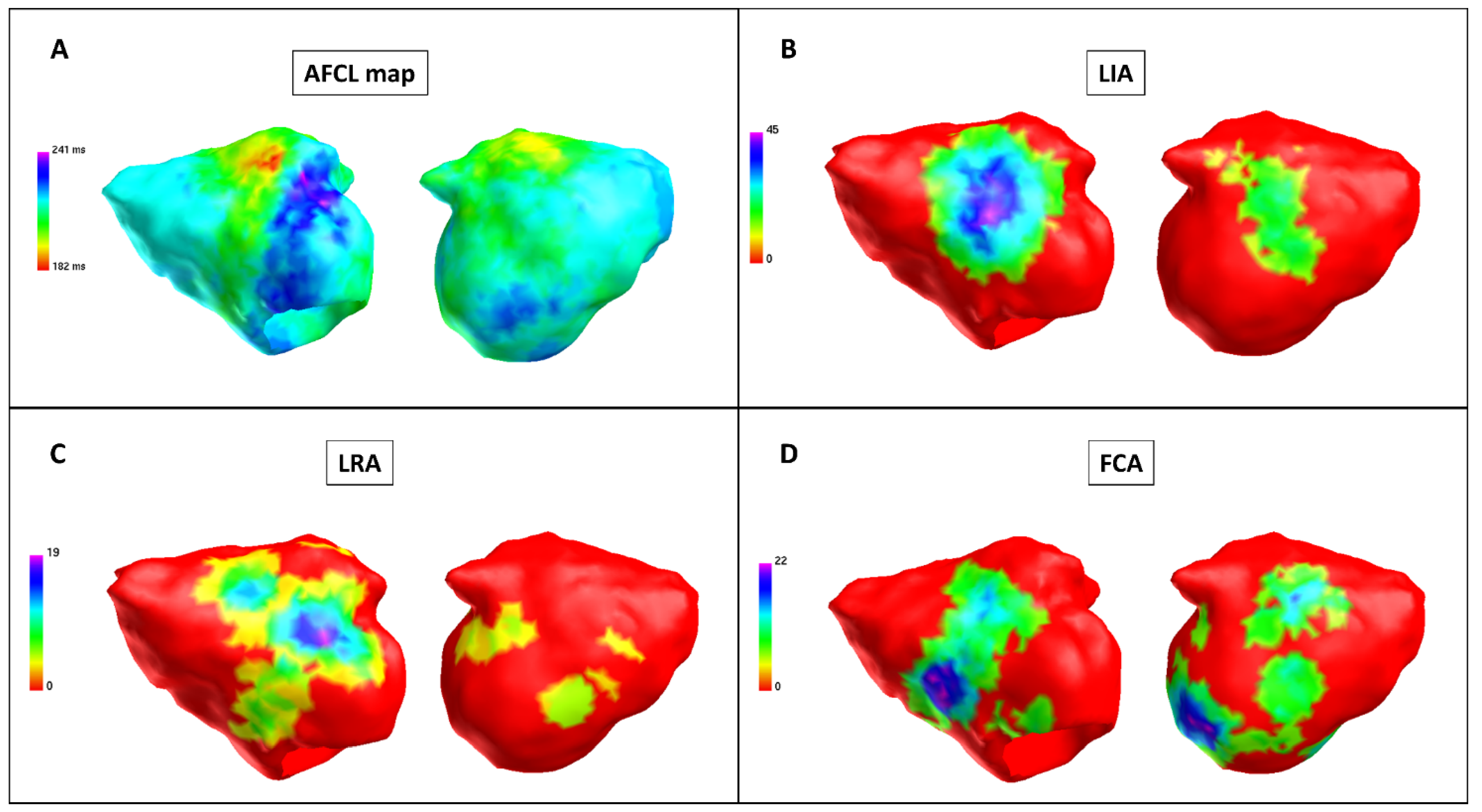
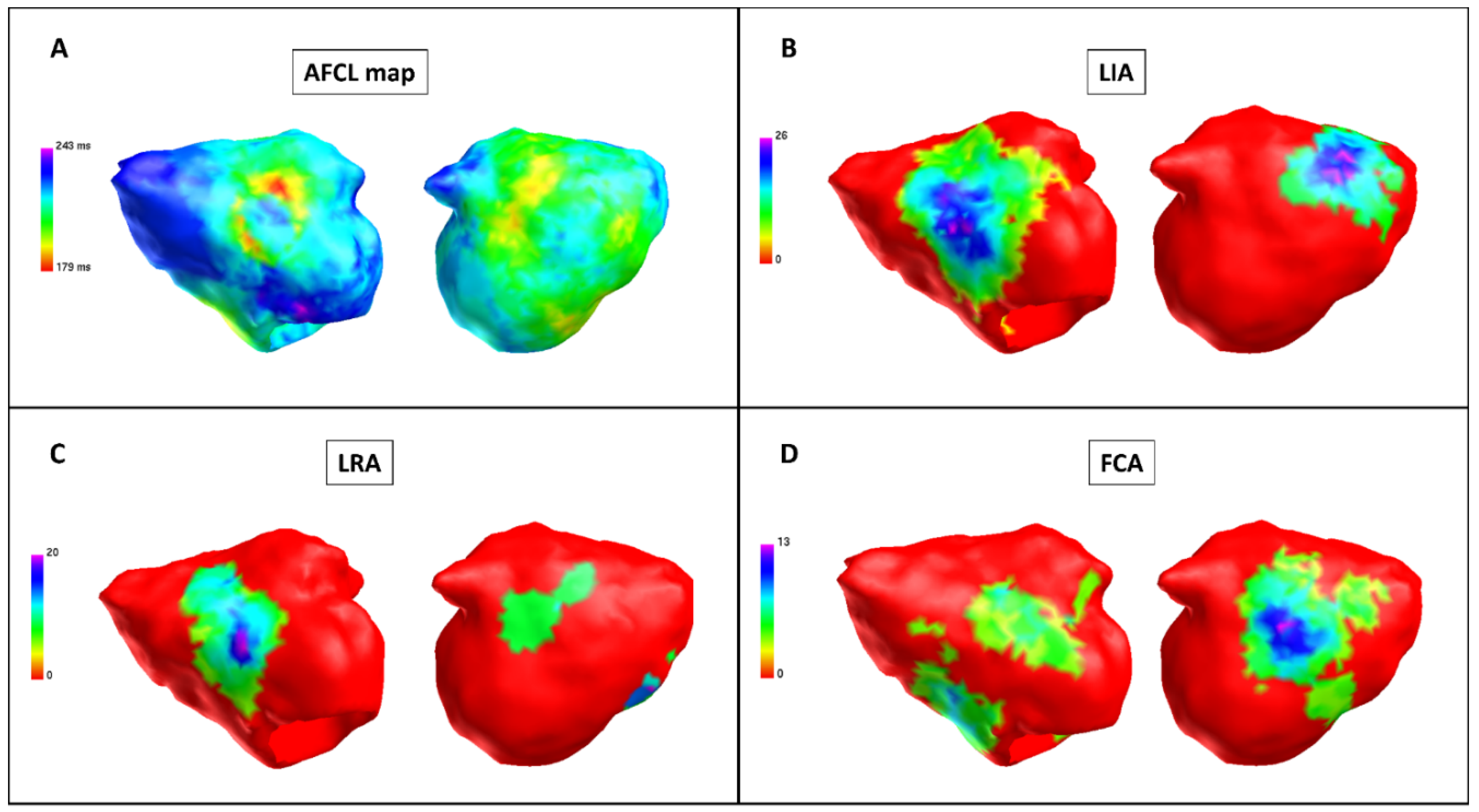
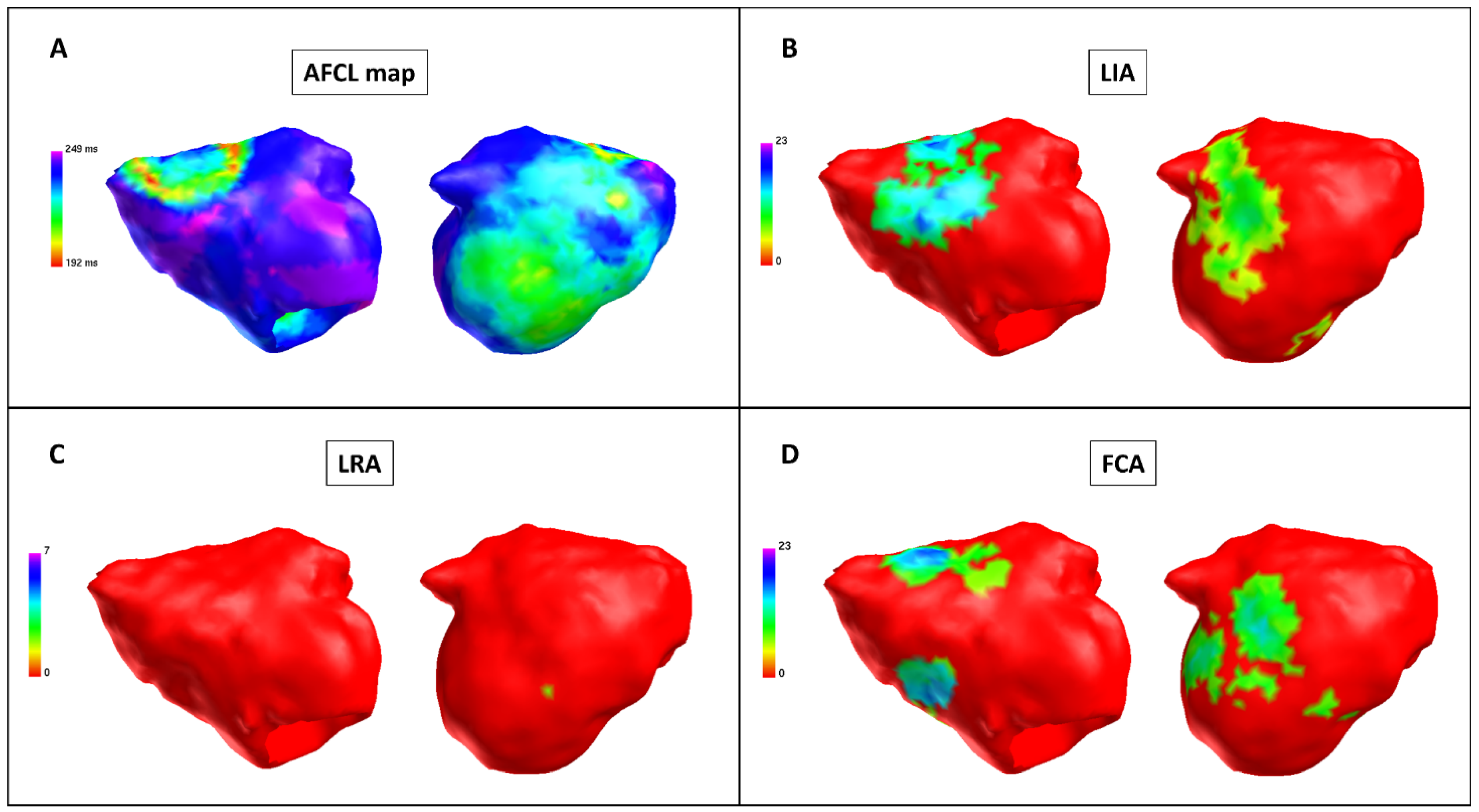
3.2. Pulmonary Vein Isolation and Posterior Wall Isolation in Charge Density Map Analysis
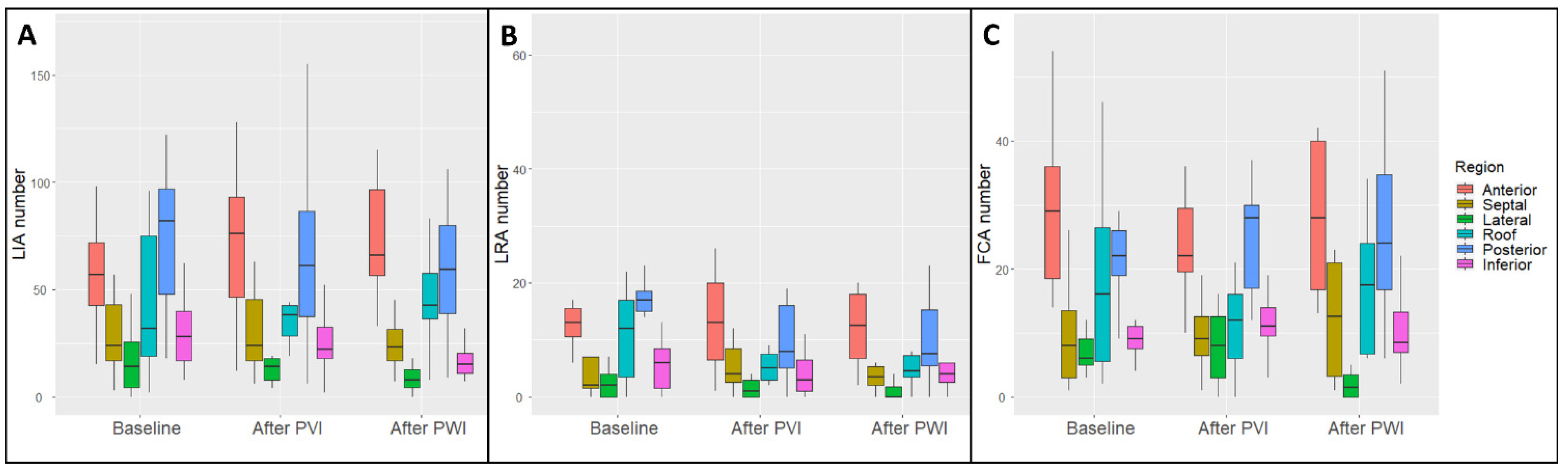
3.3. Regional Charge Density Map Analysis
4. Discussion
4.1. Global Charge Density Mapping in Persistent Atrial Fibrillation
4.2. The Role of Pulmonary Vein Isolation and Posterior Wall Isolation in Persistent Atrial Fibrillation
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.; Dilaveris, P.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.; Jiang, C.; Betts, T.R.; Chen, J.; Deisenhofer, I.; Mantovan, R.; Macle, L.; Morillo, C.; Haverkamp, W.; Weerasooriya, R.; et al. Approaches to Catheter Ablation for Persistent Atrial Fibrillation. N. Engl. J. Med. 2015, 372, 1812–1822. [Google Scholar] [CrossRef] [PubMed]
- Derval, N.; Duchateau, J.; Denis, A.; Ramirez, F.; Mahida, S.; André, C.; Krisai, P.; Nakatani, Y.; Kitamura, T.; Takigawa, M.; et al. Marshall bundle elimination, Pulmonary vein isolation, and Line completion for ANatomical ablation of persistent atrial fibrillation (Marshall-PLAN): Prospective, single-center study. Hear Rhythm. 2021, 18, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Willems, S.; Verma, A.; Betts, T.R.; Murray, S.; Neuzil, P.; Ince, H.; Steven, D.; Sultan, A.; Heck, P.; Hall, M.; et al. Targeting Nonpulmonary Vein Sources in Persistent Atrial Fibrillation Identified by Noncontact Charge Density Mapping: UNCOVER AF Trial. Circ. Arrhythm. Electrophysiol. 2019, 12, e007233. [Google Scholar] [CrossRef]
- Narayan, S.M.; Krummen, D.E.; Shivkumar, K.; Clopton, P.; Rappel, W.J.; Miller, J.M. Treatment of atrial fibrillation by the ablation of localized sources: CONFIRM (Conventional Ablation for Atrial Fibrillation with or Without Focal Impulse and Rotor Modulation) trial. J. Am. Coll. Cardiol. 2012, 60, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Haissaguerre, M.; Hocini, M.; Denis, A.; Shah, A.; Komatsu, Y.; Yamashita, S.; Daly, M.; Amraoui, S.; Zellerhoff, S.; Picat, M.; et al. Driver domains in persistent atrial fibrillation. Circulation 2014, 130, 530–538. [Google Scholar] [CrossRef] [Green Version]
- Grace, A.; Willems, S.; Meyer, C.; Verma, A.; Heck, P.; Zhu, M.; Shi, X.; Chou, D.; Dang, L.; Scharf, C.; et al. High-resolution noncontact charge-density mapping of endocardial activation. JCI Insight 2019, 4, e126422. [Google Scholar] [CrossRef] [Green Version]
- Shi, R.; Chen, Z.; Pope, M.T.; Zaman, J.A.; Debney, M.; Marinelli, A.; Boyalla, V.; Sathishkumar, A.; Karim, N.; Cantor, E.; et al. Individualized ablation strategy to treat persistent atrial fibrillation: Core-to-boundary approach guided by charge-density mapping. Hear. Rhythm. 2021, 18, 862–870. [Google Scholar] [CrossRef]
- Corradi, D.; Callegari, S.; Maestri, R.; Zaman, J.; Debney, M.; Marinelli, A.; Boyalla, V.; Sathishkumar, A.; Karim, N.; Cantor, E.; et al. Differential structural remodeling of the left-atrial posterior wall in patients affected by mitral regurgitation with or without persistent atrial fibrillation: A morphological and molecular study. J. Cardiovasc. Electrophysiol. 2012, 23, 862–870. [Google Scholar] [CrossRef]
- Roberts-Thomson, K.C.; Stevenson, I.; Kistler, P.M.; Haqqani, H.M.; Spence, S.J.; Goldblatt, J.C.; Sanders, P.; Kalman, J.M. The role of chronic atrial stretch and atrial fibrillation on posterior left atrial wall conduction. Hear Rhythm. 2009, 6, 1109–1117. [Google Scholar] [CrossRef]
- Kalifa, J.; Tanaka, K.; Zaitsev, A.V.; Haqqani, H.; Spence, S.; Goldblatt, J.; Sanders, P.; Kalman, J. Mechanisms of wave fractionation at boundaries of high-frequency excitation in the posterior left atrium of the isolated sheep heart during atrial fibrillation. Circulation 2006, 113, 1109–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaba, R.A.; Momin, A.; Camm, J. Persistent atrial fibrillation: The role of left atrial posterior wall isolation and ablation strategies. J. Clin. Med. 2021, 10, 3129. [Google Scholar] [CrossRef] [PubMed]
- Tokioka, S.; Fukamizu, S.; Kimura, T.; Takahashi, M.; Kitamura, T.; Hojo, R. The effect of posterior wall isolation for persistent atrial fibrillation on recurrent arrhythmia. J. Cardiovasc. Electrophysiol. 2021, 32, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Shim, J.; Park, J.; Yu, H.; Kim, T.; Park, J.; Uhm, S.; Kim, J.; Joung, B.; Lee, M.; et al. The Electrical Isolation of the Left Atrial Posterior Wall in Catheter Ablation of Persistent Atrial Fibrillation. JACC Clin. Electrophysiol. 2019, 5, 1253–1261. [Google Scholar] [CrossRef]
- Ahn, J.; Shin, D.G.; Han, S.-J.; Lim, H.E. Does isolation of the left atrial posterior wall using cryoballoon ablation improve clinical outcomes in patients with persistent atrial fibrillation? A prospective randomized controlled trial. EP Eur. 2022, euac005. [Google Scholar] [CrossRef]
- Aryana, A. Rationale and outcomes of cryoballoon ablation of the left atrial posterior wall in conjunction with pulmonary vein isolation. J. Innov. Card. Rhythm. Manag. 2021, 12, 4633–4646. [Google Scholar] [CrossRef]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for noninvasive evaluation of native valvular regurgitation A report from the american society of echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J. Indian Acad. Echocardiogr. Cardiovasc. Imaging 2020, 4, 58. [Google Scholar] [CrossRef]
- Bisignani, A.; Cecchini, F.; Mugnai, G.; Overeinder, I.; Sieira, J.; Osório, T.G.; Miraglia, V.; Monaco, C.; Sofianos, D.; Boveda, S.; et al. Single procedural outcomes in the setting of percutaneous ablation for persistent atrial fibrillation: A propensity-matched score comparison between different strategies. J. Interv. Card. Electrophysiol. 2021, 1–8. [Google Scholar] [CrossRef]
- Bisignani, A.; Overeinder, I.; Kazawa, S.; Iacopino, S.; Cecchini, F.; Miraglia, V.; Osório, T.G.; Boveda, S.; Bala, G.; Mugnai, G.; et al. Posterior box isolation as an adjunctive ablation strategy with the second-generation cryoballoon for paroxysmal atrial fibrillation: A comparison with standard cryoballoon pulmonary vein isolation. J. Interv. Card. Electrophysiol. 2020, 61, 313–319. [Google Scholar] [CrossRef]
- Bisignani, A.; Pannone, L.; Bala, G.; Kazawa, S.; Calburean, P.; Overeinder, I.; Monaco, C.; Lipartiti, F.; Miraglia, V.; Rizzi, S.; et al. Repeat procedures for recurrent persistent atrial fibrillation: A propensity-matched score comparison between left atrial linear ablation with radiofrequency and posterior wall isolation with the cryoballoon. J. Arrhythm. 2021, 37, 1287–1294. [Google Scholar] [CrossRef]
- Osorio, J.; Rajendra, A.; Varley, A.; Henry, R.; Cunningham, J.; Spear, W.; Morales, G. General anesthesia during atrial fibrillation ablation: Standardized protocol and experience. Pacing Clin. Electrophysiol. 2020, 43, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Bala, G.; De Asmundis, C.; Chierchia, G.-B. A novel noncontact high-resolution charge density mapping system to guide ablation of complex atrial arrhythmias: Overview of device technology and application. Expert Rev. Med. Devices 2021, 18, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Ramak, R.; Chierchia, G.B.; Paparella, G.; Monaco, C.; Miraglia, V.; Cecchini, F.; Bisignani, A.; Mojica, J.; Housari, M.; Sofianos, D.; et al. Novel noncontact charge density map in the setting of post-atrial fibrillation atrial tachycardias: First experience with the Acutus SuperMap Algorithm. J. Interv. Card. Electrophysiol. 2021, 61, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Chen, Z.; Butcher, C.; Ab Zaman, J.; Boyalla, V.; Wang, Y.K.; Riad, O.; Bs, A.S.; Norman, M.; Haldar, S.; et al. Diverse activation patterns during persistent atrial fibrillation by noncontact charge-density mapping of human atrium. J. Arrhythm. 2020, 36, 692–702. [Google Scholar] [CrossRef] [PubMed]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Sultan, A.; Lüker, J.; Andresen, D.; Kuck, K.H.; Hoffmann, E.; Brachmann, J.; Hochadel, M.; Willems, S.; Eckardt, L.; Lewalter, T.; et al. Predictors of Atrial Fibrillation Recurrence after Catheter Ablation: Data from the German Ablation Registry. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, M.; da Silva, M.N.; Timoteo, A.T.; Feliciano, J.; Sousa, L.; Santos, S.; Silva-Carvalho, L.; Ferreira, R. Inducibility of atrial fibrillation during electrophysiologic evaluation is associated with increased dispersion of atrial refractoriness. Int. J. Cardiol. 2009, 136, 130–135. [Google Scholar] [CrossRef]
- Kharche, S.; Zhang, H. Simulating the effects of atrial fibrillation induced electrical remodeling: A comprehensive simulation study. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2008, 2008, 593–596. [Google Scholar]
- Heijman, J.; Voigt, N.; Nattel, S.; Dobrev, D. Cellular and molecular electrophysiology of atrial fibrillation initiation, maintenance, and progression. Circ. Res. 2014, 114, 1483–1499. [Google Scholar] [CrossRef] [Green Version]
- Nattel, S.; Heijman, J.; Zhou, L.; Dobrev, D. Molecular Basis of Atrial Fibrillation Pathophysiology and Therapy: A Translational Perspective. Circ. Res. 2020, 127, 51–72. [Google Scholar] [CrossRef]
- Heijman, J.; Sutanto, H.; Crijns, H.J.G.M.; Nattel, S.; Trayanova, N.A. Computational models of atrial fibrillation: Achievements, challenges, and perspectives for improving clinical care. Cardiovasc. Res. 2021, 117, 1682–1699. [Google Scholar] [CrossRef] [PubMed]
- Roney, C.H.; Beach, M.L.; Mehta, A.M.; Sim, I.; Corrado, C.; Bendikas, R.; Solis-Lemus, J.A.; Razeghi, O.; Whitaker, J.; O’Neill, L.; et al. In silico Comparison of Left Atrial Ablation Techniques That Target the Anatomical, Structural, and Electrical Substrates of Atrial Fibrillation. Front. Physiol. 2020, 11, 1145. [Google Scholar] [CrossRef] [PubMed]
- Kawai, S.; Mukai, Y.; Inoue, S.; Mukai, Y.; Inoue, S.; Yakabe, D.; Nagaoka, K.; Sakamoto, K.; Takase, S.; Chishaki, A.; et al. Non-Pulmonary Vein Triggers of Atrial Fibrillation Are Likely to Arise from Low-Voltage Areas in the Left Atrium. Sci. Rep. 2019, 9, 12271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewitz, I.; Willems, S.; Salukhe, T.V.; Steven, D.; Hoffmann, B.; Servatius, H.; Bock, K.; Aydin, M.; Wegscheider, K.; Meinertz, T.; et al. Atrial fibrillation cycle length is a sole independent predictor of a substrate for consecutive arrhythmias in patients with persistent atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2010, 3, 351–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (N = 11) | |
|---|---|
| Age (years) | 59.2 ± 9.9 |
| Gender (male) | 9 (81.8%) |
| Height (cm) | 183.0 ± 3.9 |
| Weight (Kg) | 95.2 ± 12.7 |
| BMI | 29.4 ± 3.9 |
| CHA2DS2VASc | 1.8 ± 0.8 |
| Hypertension | 9 (81.8%) |
| Diabetes | 3 (27.3%) |
| Dyslipidemia | 6 (54.5%) |
| Heart failure | 1 (9.1%) |
| Chronic kidney disease | 2 (18.2%) |
| Coronary artery disease | 1 (9.1%) |
| Valvular heart disease | 0 (0.0%) |
| COPD | 1 (9.1%) |
| TIA or CVA | 0 (0.0%) |
| Drugs | |
| AAD Class Ic | 2 (18.2%) |
| Betablockers | 6 (54.5%) |
| AAD Class III | 4 (36.4%) |
| AAD Class IV | 0 (0.0%) |
| OAC | 11 (100.0%) |
| VKA | 0 (0.0%) |
| DOACs | 11 (100.0%) |
| Aspirin | 1 (9.1%) |
| ACEI or ARBs | 8 (2.7%) |
| LVEF (%) | 51.0 ± 16.4 |
| LA volume index (mL/mq) | 43.8 ± 12.0 |
| Baseline (N = 66) | Post-PVI (N = 66) | Baseline + Post-PVI (N = 132) | p Value | |
|---|---|---|---|---|
| Global AFCL mean (ms) | 184.4 ± 14.4 | 198.0 ± 17.3 | 191.2 ± 17.2 | <0.001 * |
| Regional AFCL mean (ms) | 184.5 ± 14.8 | 198.0 ± 18.7 | 191.2 ± 18.1 | <0.001 * |
| Global intra-chamber coherence mean | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.073 |
| Regional intra-chamber coherence mean | 0.4 ± 0.1 | 0.4 ± 0.2 | 0.4 ± 0.1 | 0.095 |
| Global recurrence mean | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.078 |
| Regional recurrence mean | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.078 |
| LIA number (N) | 43.5 ± 32.4 | 42.9 ± 35.4 | 43.2 ± 33.8 | 0.92 |
| LRA number (N) | 9.8 ± 9.8 | 8.7 ± 11.4 | 9.3 ± 10.6 | 0.53 |
| Focal number (N) | 16.3 ± 12.6 | 15.6 ± 11.5 | 15.9 ± 12.1 | 0.74 |
| LIA perc time (N) | 12.5 ± 10.0 | 11.9 ± 10.5 | 12.2 ± 10.2 | 0.77 |
| LRA perc time (N) | 5.4 ± 5.7 | 4.8 ± 6.3 | 5.1 ± 6.0 | 0.58 |
| Focal perc time (N) | 2.0 ± 1.6 | 1.9 ± 1.4 | 2.0 ± 1.5 | 0.67 |
| Baseline (N = 66) | Post-PVI + LAPWI (N = 66) | Baseline + Post-PVI + LAPWI (N = 132) | p Value | |
|---|---|---|---|---|
| Global AFCL mean (ms) | 184.4 ± 14.4 | 201.6 ± 16.8 | 192.1 ± 18.0 | <0.001 * |
| Regional AFCL mean (ms) | 184.5 ± 14.8 | 201.8 ± 17.8 | 192.2 ± 18.6 | <0.001 * |
| Global intra-chamber coherence mean | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.089 |
| Regional intra-chamber coherence mean | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.096 |
| Global recurrence mean | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.15 |
| Regional recurrence mean | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.25 |
| LIA number (N) | 43.5 ± 32.4 | 37.8 ± 30.7 | 40.2 ± 31.3 | 0.48 |
| LRA number (N) | 9.8 ± 9.8 | 6.2 ± 6.2 | 8.0 ± 8.4 | 0.04 * |
| Focal number (N) | 16.3 ± 12.6 | 16.2 ± 13.4 | 16.7 ± 13.0 | 0.72 |
| LIA perc time (N) | 12.5 ± 10.0 | 10.6 ± 8.8 | 11.5 ± 9.4 | 0.41 |
| LRA perc time (N) | 5.4 ± 5.7 | 3.5 ± 3.9 | 4.4 ± 5.0 | 0.094 |
| Focal perc time (N) | 2.0 ± 1.6 | 2.0 ± 1.6 | 2.1 ± 1.6 | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pannone, L.; Bisignani, A.; Sorgente, A.; Gauthey, A.; Della Rocca, D.G.; Monaco, C.; Bories, W.; Ramak, R.; Overeinder, I.; Bala, G.; et al. Atrial Fibrillation Global Changes after Pulmonary Vein and Posterior Wall Isolation: A Charge Density Mapping Study. J. Clin. Med. 2022, 11, 2948. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102948
Pannone L, Bisignani A, Sorgente A, Gauthey A, Della Rocca DG, Monaco C, Bories W, Ramak R, Overeinder I, Bala G, et al. Atrial Fibrillation Global Changes after Pulmonary Vein and Posterior Wall Isolation: A Charge Density Mapping Study. Journal of Clinical Medicine. 2022; 11(10):2948. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102948
Chicago/Turabian StylePannone, Luigi, Antonio Bisignani, Antonio Sorgente, Anaïs Gauthey, Domenico G. Della Rocca, Cinzia Monaco, Wim Bories, Robbert Ramak, Ingrid Overeinder, Gezim Bala, and et al. 2022. "Atrial Fibrillation Global Changes after Pulmonary Vein and Posterior Wall Isolation: A Charge Density Mapping Study" Journal of Clinical Medicine 11, no. 10: 2948. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102948