
Cytokine Profiles as Potential Prognostic and Therapeutic Markers in SARS-CoV-2-Induced ARDS

 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Study Design
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pelosi, P.; Tonelli, R.; Torregiani, C.; Baratella, E.; Confalonieri, M.; Battaglini, D.; Marchioni, A.; Confalonieri, P.; Clini, E.; Salton, F.; et al. Different Methods to Improve the Monitoring of Noninvasive Respiratory Support of Patients with Severe Pneumonia/ARDS Due to COVID-19: An Update. J. Clin. Med. 2022, 11, 1704. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.N.; Locke, E.; Green, P.; Berry, K.; O’Hare, A.M.; Shah, J.A.; Crothers, K.; Eastment, M.C.; Dominitz, J.A.; Fan, V.S. Risk Factors for Hospitalization, Mechanical Ventilation, or Death among 10131 US Veterans with SARS-CoV-2 Infection. JAMA Netw. Open 2020, 3, 2022310. [Google Scholar] [CrossRef] [PubMed]
- Leisman, D.E.; Ronner, L.; Pinotti, R.; Taylor, M.D.; Sinha, P.; Calfee, C.S.; Hirayama, A.V.; Mastroiani, F.; Turtle, C.J.; Harhay, M.O.; et al. Cytokine elevation in severe and critical COVID-19: A rapid systematic review, meta-analysis, and comparison with other inflammatory syndromes. Lancet Respir. Med. 2020, 8, 1233–1244. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19—Preliminary Report. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Rhen, T.; Cidlowski, J. Antiinflammatory action of glucocorticoids—New mechanisms for old drugs. N. Engl. J. Med. 2005, 353, 1711–1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; Cavalcanti, A.B.; et al. Association between Administration of Systemic Corticosteroids and Mortality among Critically Ill Patients with COVID-19: A Meta-analysis. JAMA J. Am. Med. Assoc. 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Barnes, P.; Adcock, I. Glucocorticoid resistance in inflammatory diseases. Lancet 2009, 373, 1905–1917. [Google Scholar] [CrossRef]
- Meduri, G.U.; Tolley, E.A.; Chrousos, G.P.; Stentz, F. Prolonged methylprednisolone treatment suppresses systemic inflammation in patients with unresolving acute respiratory distress syndrome: Evidence for inadequate endogenous glucocorticoid secretion and inflammation-induced immune cell resistance to glucocorticoids. Am. J. Respir. Crit. Care Med. 2002, 165, 983–991. [Google Scholar] [CrossRef]
- Meduri, G.U.; Annane, D.; Confalonieri, M.; Chrousos, G.P.; Rochwerg, B.; Busby, A.; Ruaro, B.; Meibohm, B. Pharmacological principles guiding prolonged glucocorticoid treatment in ARDS. Intensive Care Med. 2020, 46, 2284–2296. [Google Scholar] [CrossRef]
- Wilson, J.G.; Simpson, L.J.; Ferreira, A.M.; Rustagi, A.; Roque, J.; Asuni, A.; Ranganath, T.; Grant, P.M.; Subramanian, A.; Rosenberg-Hasson, Y.; et al. Cytokine profile in plasma of severe COVID-19 does not differ from ARDS and sepsis. JCI Insight 2020, 5, e140289. [Google Scholar] [CrossRef]
- Ghazavi, A.; Ganji, A.; Keshavarzian, N.; Rabiemajd, S.; Mosayebi, G. Cytokine profile and disease severity in patients with COVID-19. Cytokine 2021, 137, 155323. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin definition. JAMA J. Am. Med. Assoc. 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Confalonieri, M.; Salton, F.; Fabiano, F. Acute respiratory distress syndrome. Eur. Respir. Rev. 2017, 26, 562–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salton, F.; Confalonieri, P.; Umberto Meduri, G.; Santus, P.; Harari, S.; Scala, R.; Lanini, S.; Vertui, V.; Oggionni, T.; Caminati, A.; et al. Prolonged low-dose methylprednisolone in patients with severe COVID-19 pneumonia. Open Forum Infect. Dis. 2020, 7, ofaa421. [Google Scholar] [CrossRef]
- COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 20 August 2021).
- Iebba, V.; Zanotta, N.; Campisciano, G.; Zerbato, V.; Di Bella, S.; Cason, C.; Luzzati, R.; Confalonieri, M.; Palamara, A.; Comar, M. Profiling of Oral Microbiota and Cytokines in COVID-19 Patients. Front. Microbiol. 2021, 12, 1603. [Google Scholar] [CrossRef]
- Confalonieri, M.; Urbino, R.; Potena, A.; Piattella, M.; Parigi, P.; Puccio, G.; Della Porta, R.; Giorgio, C.; Blasi, F.; Umberger, R.; et al. Hydrocortisone infusion for severe community-acquired pneumonia: A preliminary randomized study. Am. J. Respir. Crit. Care Med. 2005, 171, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Zhang, J.; Fang, C.; Zhao, X.; Qian, B.; Sun, Y.; Zhou, Y.; Hu, J.; Huang, Y.; Ma, Q.; et al. The prognostic value of IL-8 for the death of severe or critical patients with COVID-19. Medicine 2021, 100, e23656. [Google Scholar] [CrossRef]
- Escoll, P.; Ranz, I.; Muñoz-Antón, N.; van-den-Rym, A.; Alvarez-Mon, M.; Martínez-Alonso, C.; Sanz, E.; de-la-Hera, A. Sustained interleukin-1β exposure modulates multiple steps in glucocorticoid receptor signaling, promoting split-resistance to the transactivation of prominent anti-inflammatory genes by glucocorticoids. Mediat. Inflamm. 2015, 2015, 347965. [Google Scholar] [CrossRef] [Green Version]
- Smith, V.; Pizzorni, C.; Riccieri, V.; Decuman, S.; Brusselle, G.; De Pauw, M.; Deschepper, E.; Piette, Y.; Ruaro, B.; Sulli, A.; et al. Stabilization of Microcirculation in Patients with Early Systemic Sclerosis with Diffuse Skin Involvement following Rituximab Treatment: An Open-label Study. J. Rheumatol. 2016, 43, 995–996. [Google Scholar] [CrossRef] [Green Version]
- Baratella, E.; Ruaro, B.; Marrocchio, C.; Starvaggi, N.; Salton, F.; Giudici, F.; Quaia, E.; Confalonieri, M.; Cova, M.A. Interstitial Lung Disease at High Resolution CT after SARS-CoV-2-Related Acute Respiratory Distress Syndrome According to Pulmonary Segmental Anatomy. J. Clin. Med. 2021, 10, 3985. [Google Scholar] [CrossRef]
- Chriguer, R.; Elias, L.; da Silva, I.; Vieira, J.; Moreira, A.; de Castro, M. Glucocorticoid sensitivity in young healthy individuals: In vitro and in vivo studies. J. Clin. Endocrinol. Metab. 2005, 90, 5978–5984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baratella, E.; Bussani, R.; Zanconati, F.; Marrocchio, C.; Fabiola, G.; Braga, L.; Maiocchi, S.; Berlot, G.; Volpe, M.C.; Moro, E.; et al. Radiological-pathological signatures of patients with COVID-19-related pneumomediastinum: Is there a role for the Sonic hedgehog and Wnt5a pathways? ERJ Open Res. 2021, 7, 00346-2021. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| NIV (n = 12) | IMV (n = 5) | p-Value ° | |
|---|---|---|---|
| Age, mean (SD) | 60.4 (10.2) | 69.0 (3.7) | 0.07 |
| Female sex, no. (%) | 5 (42.0) | 0 (0.0) | 0.24 |
| BMI ≥ 30 kg/m2, no. (%) | 27.7 (6.5) | 28.6 (2.8) | 1.00 |
| Ever smoker, no. (%) | 3 (25.0) | 3 (60.0) | 0.28 |
| Presence of major co-morbidities, no. (%) | 8 (66.7) | 5 (100.0) | 0.26 |
| Hypertension, no. (%) | 3 (25.0) | 1 (20.0) | 1.00 |
| Diabetes, no. (%) | 4 (33.3) | 2 (40.0) | 1.00 |
| Asthma/COPD, no. (%) | 1 (8.3) | 2 (40.0) | 0.19 |
| OSAS/OHS, no. (%) | 1 (8.3) | 2 (40.0) | 0.19 |
| Congestive heart failure, no. (%) | 0 (0.0) | 0 (0.0) | N/A |
| Ischemic cardiovascular disease, no. (%) | 0 (0.0) | 0 (0.0) | N/A |
| Chronic kidney disease, no. (%) | 1 (8.3) | 0 (0.0) | 1.00 |
| History of malignancy, no. (%) | 1 (8.3) | 1 (20.0) | 0.51 |
| PaO2:FiO2, mmHg, mean (SD) | 161.0 (46.09) | 112.9 (27.8) | 0.07 |
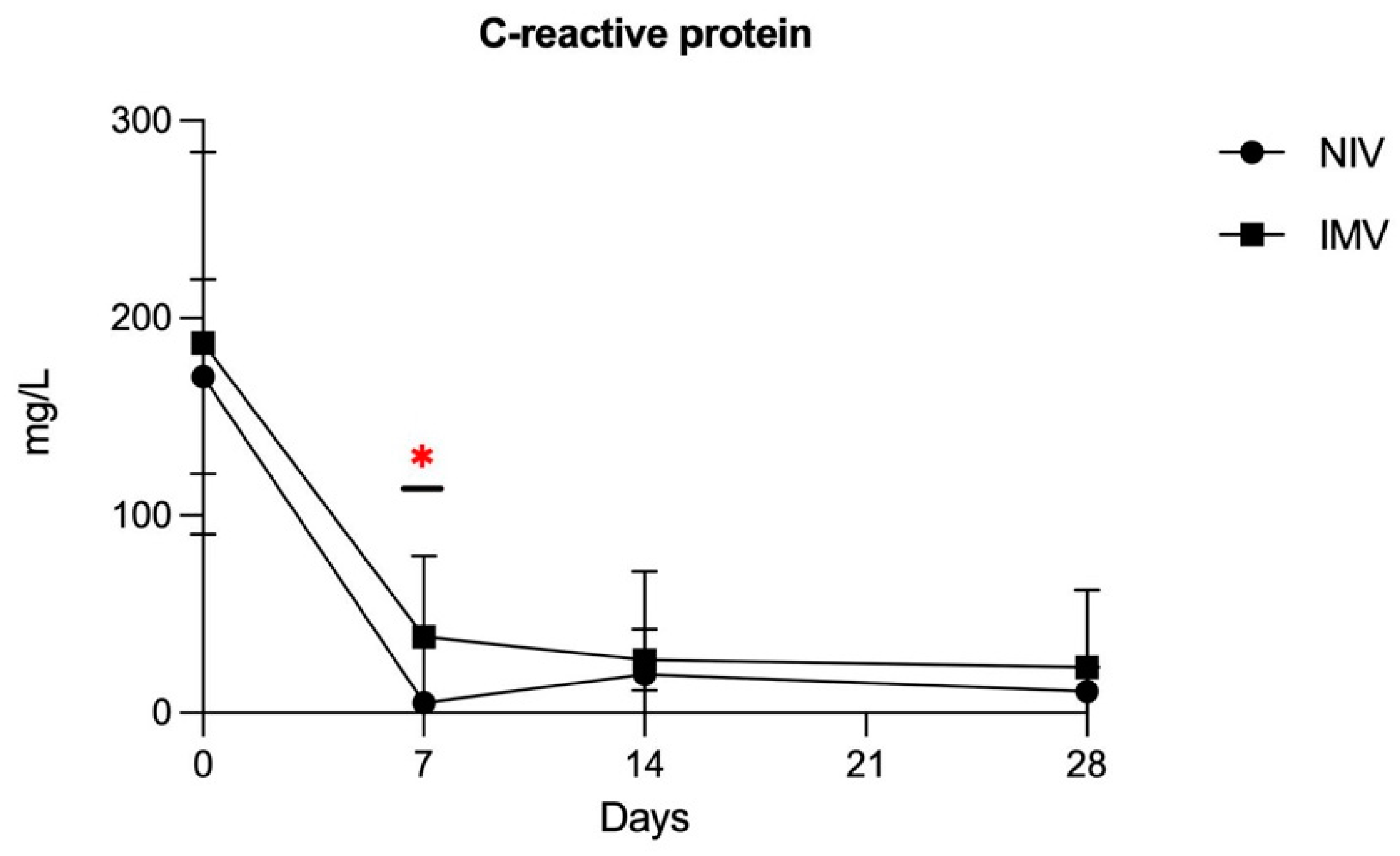
| CRP, mg/L, mean (SD) | 170.4 (39.5) | 187.4 (96.9) | 0.83 |
| D-dimer, ug/FEU/L, mean (SD) | 714.3 (264.6) | 580.0 (300.5) | 0.30 |
| LDH, U/L, mean (SD) | 339.7 (74.4) | 367.4 (81.9) | 0.53 |
| Lymphocyte count, mean (SD) | 902.2 (291.0) | 904.0 (381.2) | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salton, F.; Confalonieri, P.; Campisciano, G.; Cifaldi, R.; Rizzardi, C.; Generali, D.; Pozzan, R.; Tavano, S.; Bozzi, C.; Lapadula, G.; et al. Cytokine Profiles as Potential Prognostic and Therapeutic Markers in SARS-CoV-2-Induced ARDS. J. Clin. Med. 2022, 11, 2951. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112951
Salton F, Confalonieri P, Campisciano G, Cifaldi R, Rizzardi C, Generali D, Pozzan R, Tavano S, Bozzi C, Lapadula G, et al. Cytokine Profiles as Potential Prognostic and Therapeutic Markers in SARS-CoV-2-Induced ARDS. Journal of Clinical Medicine. 2022; 11(11):2951. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112951
Chicago/Turabian StyleSalton, Francesco, Paola Confalonieri, Giuseppina Campisciano, Rossella Cifaldi, Clara Rizzardi, Daniele Generali, Riccardo Pozzan, Stefano Tavano, Chiara Bozzi, Giulia Lapadula, and et al. 2022. "Cytokine Profiles as Potential Prognostic and Therapeutic Markers in SARS-CoV-2-Induced ARDS" Journal of Clinical Medicine 11, no. 11: 2951. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112951