
Robotic Abdominal Surgery and COVID-19: A Systematic Review of Published Literature and Peer-Reviewed Guidelines during the SARS-CoV-2 Pandemic

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment
2.4. Outcomes of Interest
2.5. Data Extraction, Synthesis, and Analysis
3. Results
3.1. Search Results
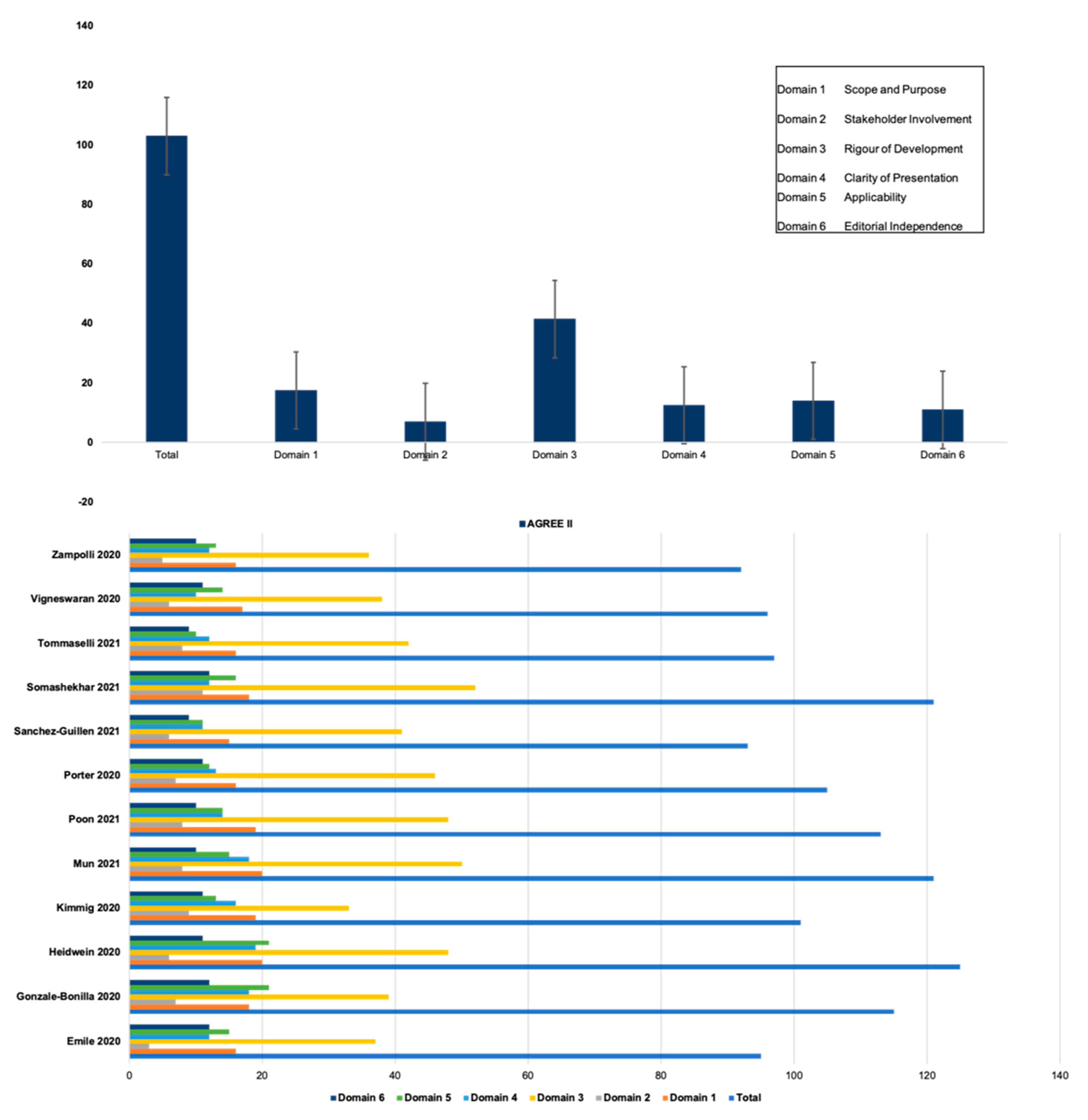
3.2. Quality Assessment and AGREE-II
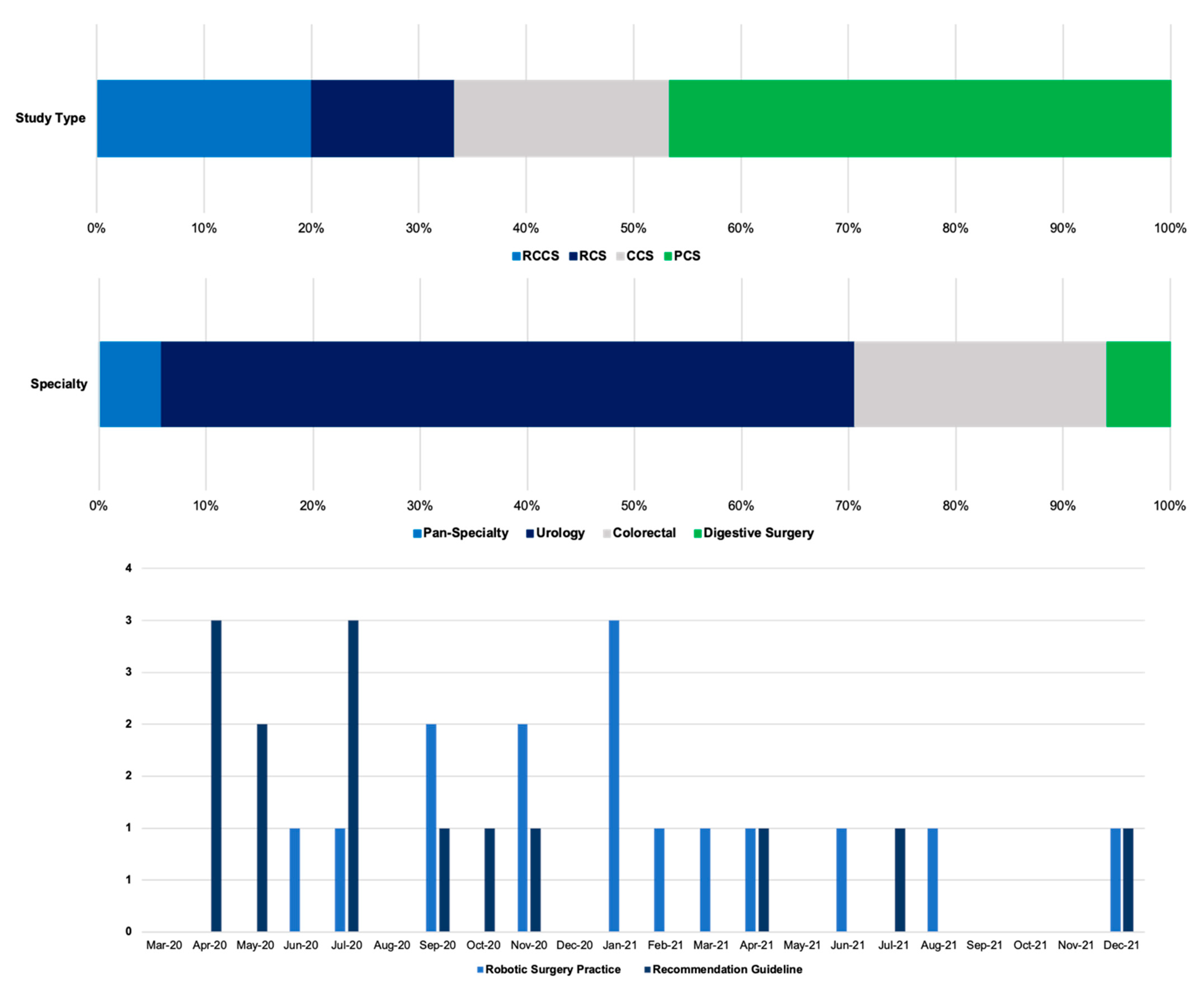
3.3. Publication Trends
3.4. Robotic Surgery Practice during COVID-19 Pandemic
3.5. Guidelines and Review Recommendations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- SAGES. SAGES COVID-19 Guideline. Available online: https://www.sages.org/recommendations-surgical-response-covid-19/ (accessed on 10 January 2022).
- EAES. European Association for Endoscopic Surgery COVID-19 Guidelines. Available online: https://eaes.eu/covid-19-statements/resources-on-smoke-gas-evacuation-during-open-laparoscopic-and-endoscopic-procedures-updated/%0D%0A (accessed on 10 January 2022).
- EAU. EAU Robotic Urology Section (ERUS). ERUS (EAU Robotic Urology Section) Guidelines during COVID-19 Emergency. Available online: https://uroweb.org/wp-content/uploads/ERUS-guidelines-for-COVID-def.pdf (accessed on 10 January 2022).
- ACPGBI. ACPGBI COVID-19 Guideline. Available online: https://www.acpgbi.org.uk/_userfiles/import/2020/04/ACPGBI-priorities-during-COVID-19-11-4-20.pdf (accessed on 10 January 2022).
- Arrizabalaga, O.; Otaegui, D.; Vergara, I.; Arrizabalaga, J.; Méndez, E. Open Access of COVID-19-related publications in the first quarter of 2020: A preliminary study based in PubMed. F1000Research 2020, 9, 649. [Google Scholar] [CrossRef] [PubMed]
- Abaza, R.; Kogan, P.; Martinez, O. Impact of the COVID-19 Crisis on Same-day Discharge after Robotic Urologic Surgery. Urology 2021, 3, 54–67. Available online: http://repositorio.unan.edu.ni/2986/1/5624.pdf (accessed on 10 January 2022). [CrossRef] [PubMed]
- Huddy, J.R.; Crockett, M.; Nizar, A.S.; Smith, R.; Malki, M.; Barber, N.; Tilney, H.S. Experiences of a “COVID protected” robotic surgical centre for colorectal and urological cancer in the COVID-19 pandemic. J. Robot. Surg. 2021, 16, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.; Hernán, M.; Reeves, B.; Al, E. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, M.C.; Kerkvliet, K.; Spithof, K. The AGREE reporting checklist: A tool to improve reporting of clinical practice guidelines. BMJ 2016, 352, i1152. [Google Scholar] [CrossRef] [Green Version]
- Abou-Chedid, W.; Nason, G.J.; Evans, A.T.; Yamada, K.; Moschonas, D.; Patil, K.; E Langely, S.; Perry, M.J. The impact of COVID-19 on surgical volume and surgical training at a high-volume pelvic oncology centre. Urol. J. 2021, 039156032110628. [Google Scholar] [CrossRef]
- Teixeira, B.L.; Cabral, J.; Mendes, G.; Madanelo, M.; Rocha, M.A.; Mesquita, S.; Correia, J.; Tavares, C.; Marques-Pinto, A.; Fraga, A. How the COVID-19 pandemic changed urology residency—A nationwide survey from the Portuguese resident’s perspective. Cent. Eur. J. Urol. 2021, 74, 121–127. [Google Scholar] [CrossRef]
- Harke, N.N.; Radtke, J.P.; Hadaschik, B.A.; Bach, C.; Berger, F.P.; Blana, A.; Borgmann, H.; Distler, F.A.; Edeling, S.; Egner, T.; et al. To defer or not to defer? A German longitudinal multicentric assessment of clinical practice in urology during the COVID-19 pandemic. PLoS ONE 2020, 15, e0239027. [Google Scholar] [CrossRef]
- Evans, S.; Taylor, C.; Antoniou, A.; Agarwal, T.; Burns, E.; Jenkins, J.; Miskovic, D. Implementation of a clinical pathway for the surgical treatment of colorectal cancer during the COVID-19 pandemic. Color. Dis. 2020, 22, 1002–1005. [Google Scholar] [CrossRef] [PubMed]
- Motterle, G.; Moro, F.D.; Zanovello, N.; Morlacco, A.; Boemo, D.G.; Zattoni, F.; Zattoni, F. Minimally invasive urologic surgery is safe during COVID-19: Experience from two high-volume centers in Italy. J. Robot. Surg. 2020, 14, 909–911. [Google Scholar] [CrossRef] [PubMed]
- Blanc, T.; Pinar, U.; Anract, J.; Assouad, J.; Audenet, F.; Borghese, B.; De La Taille, A.; El Ghoneimi, A.; Mongiat-Artus, P.; Mordant, P.; et al. Impact of the COVID-19 pandemic on oncological and functional robotic-assisted surgical procedures. J. Robot. Surg. 2021, 15, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Busetto, G.M.; Del Giudice, F.; Mari, A.; Sperduti, I.; Longo, N.; Antonelli, A.; Cerruto, M.A.; Costantini, E.; Carini, M.; Minervini, A.; et al. How Can the COVID-19 Pandemic Lead to Positive Changes in Urology Residency? Front. Surg. 2020, 7, 563006. [Google Scholar] [CrossRef] [PubMed]
- Minervini, A.; Di Maida, F.; Mari, A.; Porreca, A.; Rocco, B.; Celia, A.; Bove, P.; Umari, P.; Volpe, A.; Galfano, A.; et al. Perioperative outcomes of patients undergoing urological elective surgery during the COVID-19 pandemic: A national overview across 28 italian institutions. Cent. Eur. J. Urol. 2021, 74, 259–268. [Google Scholar] [CrossRef]
- Moschovas, M.C.; Bhat, S.; Rogers, T.P.; Onol, F.F.; Roof, S.; Sighinolfi, M.C.; Rocco, B.; Patel, V. Managing Patients with Prostate Cancer during COVID-19 Pandemic: The Experience of a High-Volume Robotic Surgery Center. J. Endourol. 2021, 35, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, Y.; Temiz, A. Surgical treatment of gastrointestinal tumors in a COVID-19 pandemic hospital: Can open versus minimally invasive surgery be safely performed? J. Surg. Oncol. 2021, 124, 1217–1223. [Google Scholar] [CrossRef]
- Sobrado, L.F.; Nahas, C.S.R.; Marques, C.F.S.; Cotti, G.C.C.; Imperiale, A.R.; Averbach, P.; Meira Júnior, J.D.; Horvat, N.; Ribeiro-Júnior, U.; Cecconello, I.; et al. Is it Safe to Perform Elective Colorectal Surgical Procedures during the COVID-19 Pandemic? A Single Institution Experience with 103 Patients. Clinics 2021, 76, e2507. [Google Scholar] [CrossRef]
- Sparwasser, P.; Brandt, M.P.; Haack, M.; Dotzauer, R.; Boehm, K.; Gheith, M.K.; Mager, R.; Jäger, W.; Ziebart, A.; Höfner, T.; et al. Robotic surgery can be safely performed for patients and healthcare workers during COVID-19 pandemic. Int. J. Med. Robot. Comput. Assist. Surg. 2021, 17, e2291. [Google Scholar] [CrossRef]
- Monique, R. Since January 2020 Elsevier has Created a COVID-19 Resource Centre with free Information in English and Mandarin on the Novel Coronavirus COVID-19. The COVID-19 Resource Centre Is Hosted on Elsevier Connect, the Company’ s Public News and Information. January 2020. Available online: https://0-www-elsevier-com.brum.beds.ac.uk/fr-fr/connect/actualites/information-covid-19 (accessed on 10 January 2022).
- Emile, S.H.; Hamid, H.K.S. A critical review of the safety of minimally invasive surgery in the era of COVID-19. Minim. Invasive Ther. Allied Technol. 2020, 31, 370–376. [Google Scholar] [CrossRef]
- Gallo, G.; La Torre, M.; Pietroletti, R.; Bianco, F.; Altomare, D.F.; Pucciarelli, S.; Gagliardi, G.; Perinotti, R. Italian society of colorectal surgery recommendations for good clinical practice in colorectal surgery during the novel coronavirus pandemic. Tech. Coloproctol. 2020, 24, 501–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Bonilla, E.A.; Rosas-Nava, J.E.; Sánchez-Núñez, J.E.; Doria-Lozano, M.I.; Corona-Montes, V.E.; Jaspersen-Gastélum, J. Evidence and Recommendations Regarding Urologic Laparoscopic and Robotic-Assisted Surgery in times of COVID-19. Rev. Mex. Urol. 2020, 80, 1–6. [Google Scholar] [CrossRef]
- Heldwein, F.L.; Loeb, S.; Wroclawski, M.L.; Sridhar, A.N.; Carneiro, A.; Lima, F.S.; Teoh, J.Y.-C. A Systematic Review on Guidelines and Recommendations for Urology Standard of Care during the COVID-19 Pandemic. Eur. Urol. Focus 2020, 6, 1070–1085. [Google Scholar] [CrossRef] [PubMed]
- Kimmig, R.; Verheijen, R.H.M.; Rudnicki, M. Robot assisted surgery during the COVID-19 pandemic, especially for gynecological cancer: A statement of the society of european robotic gynaecological surgery (SERGS). J. Gynecol. Oncol. 2020, 31, e59. [Google Scholar] [CrossRef] [Green Version]
- Mun, D.H.; Pradere, B.; Shariat, S.F.; Remzi, M. Intraoperative aerosol viral transmission in minimally invasive surgery: A scoping review and impact on clinical guidelines and practice during the onset of the coronavirus disease 2019 (COVID-19) pandemic. BJU Int. 2021, 127, 349–360. [Google Scholar] [CrossRef]
- Navarra, G.; Komaei, I.; Currò, G.; Angrisani, L.; Bellini, R.; Cerbone, M.R.; Di Lorenzo, N.; De Luca, M.; Foletto, M.; Gentileschi, P.; et al. Bariatric surgery and the COVID-19 pandemic: SICOB recommendations on how to perform surgery during the outbreak and when to resume the activities in phase 2 of lockdown. Updates Surg. 2020, 72, 259–268. [Google Scholar] [CrossRef]
- Poon, D.M.; Chan, C.-K.; Chan, T.-W.; Cheung, F.-Y.; Ho, L.-Y.; Kwong, P.W.-K.; Lee, E.K.-C.; Leung, A.K.-C.; Leung, S.Y.-L.; So, H.-S.; et al. Prostate cancer management in the era of COVID-19: Recommendations from the Hong Kong Urological Association and Hong Kong Society of Uro-oncology. Asia-Pac. J. Clin. Oncol. 2021, 17 (Suppl. 3), 48–54. [Google Scholar] [CrossRef]
- Porter, J.; Blau, E.; Gharagozloo, F.; Martino, M.; Cerfolio, R.; Duvvuri, U.; Caceres, A.; Badani, K.; Bhayani, S.; Collins, J.; et al. Society of Robotic Surgery review: Recommendations regarding the risk of COVID-19 transmission during minimally invasive surgery. BJU Int. 2020, 126, 225–234. [Google Scholar] [CrossRef]
- Sánchez-Guillén, L.; Jimenez-Rodriguez, R.M. Special surgical approaches during peri-COVID-19 pandemic: Robotic and transanal minimally invasive surgery. World J. Gastrointest. Surg. 2021, 13, 529–536. [Google Scholar] [CrossRef]
- Somashekhar, S.P.; Acharya, R.; Saklani, A.; Parikh, D.; Goud, J.; Dixit, J.; Gopinath, K.; Kumar, M.V.; Bhojwani, R.; Nayak, S.; et al. Adaptations and Safety Modifications to Perform Safe Minimal Access Surgery (MIS: Laparoscopy and Robotic) during the COVID-19 Pandemic: Practice Modifications Expert Panel Consensus Guidelines from Academia of Minimal Access Surgical Oncology (AMASO). Indian J. Surg. Oncol. 2021, 12, 210–220. [Google Scholar] [CrossRef]
- Tommaselli, G.A.; Grange, P.; Ricketts, C.D.; Clymer, J.W.; Fryrear, R.S., II. Intraoperative Measures to Reduce the Risk of COVID-19 Transmission During Minimally Invasive Procedures: A Systematic Review and Critical Appraisal of Societies’ Recommendations. Surg. Laparosc. Endosc. Percutan. Tech. 2021, 31, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, Y.; Prachand, V.N.; Posner, M.C.; Matthews, J.B.; Hussain, M. What Is the Appropriate Use of Laparoscopy over Open Procedures in the Current COVID-19 Climate? J. Gastrointest. Surg. 2020, 24, 1686–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zampolli, H.C.; Rodriguez, A.R. Laparoscopic and robotic urology surgery during global pandemic COVID-19. Int. Braz. J. Urol. 2020, 46 (Suppl. 1), 215–221. [Google Scholar] [CrossRef] [PubMed]
- Ielpo, B.; Podda, M.; Pellino, G.; Pata, F.; Caruso, R.; Gravante, G.; Di Saverio, S.; ACIE Appy Study Collaborative. Global attitudes in the management of acute appendicitis during COVID-19 pandemic: ACIE Appy Study. Br. J. Surg. 2021, 108, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Surgeons. Available online: https://www.rcseng.ac.uk/coronavirus/joint-guidance-for-surgeons-v2/ (accessed on 28 February 2022).
- American College of Surgeons. COVID-19: Considerations for Optimum Surgeon Protection Before, during, and after Operation. Available online: https://www.facs.org/covid-19/clinical-guidance/surgeon-protection (accessed on 15 April 2020).
- Di Saverio, S.; Khan, M.; Pata, F.; Ietto, G.; De Simone, B.; Zani, E.; Carcano, G. Laparoscopy at all costs? Not now during COVID-19 outbreak and not for acute care surgery and emergency colorectal surgery: A practical algorithm from a hub tertiary teaching hospital in Northern Lombardy, Italy. J. Trauma Acute Care Surg. 2020, 88, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Di Saverio, S.; Pata, F.; Khan, M.; Ietto, G.; Zani, E.; Carcano, G. Convert to open: The new paradigm for surgery during COVID-19? Br. J. Surg. 2020, 107, e194. [Google Scholar] [CrossRef]
- Taylor, N. Pandemic drives US da Vinci robot use down 65%. MEDTECH Dive Brief USA Ind. Dive. 2020. Available online: https://www.medtechdive.com/news/pandemic-drives-us-da-vinci-robot-use-down-65/576246/ (accessed on 10 January 2022).
- Zemmar, A.; Lozano, A.; Nelson, B. The rise of robots in surgical environments during COVID-19. Nat. Med. 2020, 2, 566–572. [Google Scholar]
- Moawad, G.; Rahman, S.; Martino, M.; Al, E. Robotic surgery during the COVID pandemic: Why now and why for the future. J. Robot. Surg. 2020, 14, 917–920. [Google Scholar] [CrossRef]
- Abdelfatah, E.; Jordan, S.; Dexter, E.; Al, E. Robotic thoracic and esophageal surgery: A critical review of comparative outcomes. Ann. Laparosc. Endosc. Surg. 2021, 6, 10. [Google Scholar]
- Childers, C.; Maggard-Gibbons, M. Trends in the use of robotic-assisted surgery during the COVID-19 pandemic. Br. J. Surg. 2021, 108, e330–e331. [Google Scholar] [CrossRef]
- Pellino, G.; Vaizey, C.J.; Maeda, Y.; European Society of Coloproctology (ESCP) Guideline Committee. The COVID-19 pandemic: Considerations for resuming normal colorectal services. Colorectal Dis. 2020, 22, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Sevryugina, Y.V.; Dicks, A.J. Publication practices during the COVID-19 pandemic: Biomedical preprints and peer-reviewed literature. bioRxiv 2021, 2021, 427563. [Google Scholar] [CrossRef]
- Mehra, M.; Ruschitzka, F.; Patel, A. Retraction-Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: A multinational registry analysis. Lancet 2020, 395, 1820. [Google Scholar] [CrossRef]
- The Editors of the Lancet. Learning from a retraction. Lancet 2020, 396, 1056. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Author | Publication Date | Interval to Publication | Specialty | Country | No. Patients | Study Design | Study Timing | Aim | Outcomes | Main Finding | ROBINS-I |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abaza 2021 [6] | January 2021 | 70 | Urology | USA | 131 | RCCS | 16 March to 5 June 2020 | Impact of COVID-19 on SDD following RAS urologic surgery | 30 day morbidity Perioperative pain scores Pathological outcomes | SDD was safely applied during COVID-19 pandemic without increasing complications or readmissions | Low |
| Abou-Chedid 2021 [12] | December 2021 | 241 | Urology | UK | 1998 | RCCS | 23 March to 10 May 2020 | Impact of COVID-19 on RAS surgical volume in urologic oncology | Impact of COVID-19 on RAS surgical training in urologic oncology | Substantial decrease in RAS urological oncology caseload during the COVID pandemic (clean sites can ensure continuity of care for cancer surgery and training needs) | Moderate |
| Blanc 2021 [17] | January 2021 | 23 | Pan-specialty | France | 535 | RCCS | 16 March to 30 April 2020 | Assess impact of COVID-19 pandemic on RAS volume | Perioperative COVID status COVID management | 60% decreases in RAS volume 49% decrease in RAS oncological procedures | Low |
| Busetto 2020 [18] | November 2020 | 151 | Urology | Italy | 387 Residents (RR 67.1%) | CCS | March to April 2020 | Identify positive changes to urology residency due to COVID-19 pandemic | Impact of pandemic on training volume Role of social distancing distance learning and telemedicine | 52.9% used distance teaching for the first time Working in COVID hospital significantly reduced RAS activity (OR 4.64) | Low |
| Evans 2020 [15] | July 2020 | 3 | Colorectal | UK | 38 | PCS | 25 March to 9 April 2020 | Early experience of colorectal cancer surgery clinical pathway during COVID-19 pandemic | 30 day morbidity LOS Pathological outcomes | 78% MIS rate (17% RAS) No major post-operative complications No perioperative diagnosis of COVID-19 | Low |
| Harke 2020 [14] | September 2020 | 61 | Urology | Germany | 27 Urology centres (RR 41%) | CCS | 16 March to 24 May | Changes in urologic practice during the COVID-19 pandemic with particular focus on robotic surgery | Surgeon reported changes in overall capacity, elective/emergency surgery volume, and perceived protection of a robotic surgery approach | 27% reduction in robotic surgery Equal reductions in open and robotic procedures | Moderate |
| Huddy 2021 [7] | February 2021 | 103 | Colorectal and Urology | UK | 60 | PCS | 12 May to 30 July 2020 | Experience at a “COVID protected” robotic surgical centre during the COVID-19 pandemic | Operative time Blood loss Complications Readmissions | Safe delivery of robotic surgery in dedicated unit with acceptable outcomes Reduced LOS due to the dedicated unit | Low |
| Minervini 2021 [19] | April 2021 | 92 | Urology | Italy | 1943 | PCS | 24 February to 30 March 2020 | Surgical outcomes in patients undergoing elective urological surgery during the COVID-19 pandemic | Operative practice trends Perioperative outcomes COVID+ rates and related outcomes | 21.3% of cases were performed robotically One post-operative mortality in robotic cohort due to the fact of pneumonia (SARS-CoV-2 PCR positive) | Low |
| Moschovas 2021 [20] | November 2020 | - | Urology | USA and Italy | 585 | PCS | 1 March to 25 May 2020 | Management of patients with prostate cancer during the COVID-19 pandemic | Management algorithm Selection criteria for surgery Perioperative management | 147 RARRPs performed without complications | Low |
| Motterle 2020 [16] | June 2020 | 6 | Urology | Italy | 77 | PCS | 9 March to 1 May 2020 | MIS urology practice during the COVID-19 “lockdown” period | Practice trends SARS-CoV-2 testing, PPE and aerosolisation reduction strategies | 80.5% of cases performed RAS 7.8% 15 day complication CD > 3 No perioperative patient/staff COVID positive | Low |
| Özdemir 2021 [21] | August 2021 | 2 | Digestive Surgery | Turkey | 129 | PCS | March 2020 to May 2021 | Surgical management of gastrointestinal tumours in a COVID-19 pandemic hospital | List of procedures Operation time LOS Pathological outcomes | 13.2% performed robotic 8 cases of perioperative COVID+, no mortalities | Low |
| Sobrado 2021 [22] | March 2021 | 96 | Colorectal | Brazil | 103 | RCS | 10 March to 9 Sept 2020 | Safety of elective colorectal surgery during the COVID-19 pandemic | Variety of procedures performed Perioperative outcomes Perioperative COVID rates | 90.9% colorectal cancer 9.1% IBD 3% performed RAS | Low |
| Sparwasser 2021 [23] | June 2021 | 65 | Urology | Germany | 61 | RCS | 12 March to 11 May 2020 | Investigate the safety of RAS during the COVID-19 pandemic concerning newly acquired COVID rates | Perioperative outcomes Perioperative COVID+ rates | 11.5% >/= CD Grade III complication 1.6% (n = 1) post-operative COVDI+ | Low |
| Tabourin 2020 [24] | September 2020 | 103 | Urology | France | 68 | PCS | 2 March to 14 April 2020 | To assess potential COVID-19 rates in RAS procedures | Perioperative outcomes Perioperative COVID+ rates | 91.8% RAS procedures for oncology 16.2% symptomatic post-op and 1.5% (n = 1) tested positive | Low |
| Teixeira 2021 [13] | January 2021 | 105 | Urology | Portugal | 43 Residents (RR 54.4%) | CCS | 25 April to 25 May 2020 | Impact of the COVID-19 pandemic on urology residence in Portugal | Impact on operative activity Impact on case-mi xImpact on clinical activities and emergency practice | 34.9% RAS postponed RAS volume reduced by 65.9% | Moderate |
| Author | Specialty | Country | Publication (Month, Year) | Publication Interval (Days) | Overall Aim | Non-Peer-Reviewed Guidelines Included | Basis of Recommendation | Conclusions Relevant to Robotic Surgery | AGREE II Score (/161) |
|---|---|---|---|---|---|---|---|---|---|
| Emile 2020 [25] | Digestive Surgery | International | October 2020 | 84 | Safety of MIS (including robotic surgery) amid the COVID-19 pandemic | ACS EAES RCSEd SAGES | Evidence based | Robotic surgery is safe to continue in abdominal Emergency Caution should be taken to avoid the presumed risk of aerosolisation of the virus particles during procedures | 95 |
| Gallo 2020 [26] | Colorectal Surgery | Italy | April 2020 | 1 | Provide national good clinical practice guidelines during the COVID-19 pandemic | ACPGBI ACS ECCO SAGES | Mixed-evidence based and expert consensus | Potential hazards of robotic surgery need to be weighed against the benefits (shorter length of stay and decreased complication rate) | 113 |
| Gonzalez-Bonilla 2020 [27] | Urology | Mexico | June 2020 | 5 | Evidence and recommendations for urologic-RAS during the COVID-19 pandemic | ACS ASA SAGES | Mixed-evidence based and expert consensus | RAS viable with proper precautions | 115 |
| Heldwein 2020 [28] | Urology | International | June 2020 | - | Summarise guidelines and recommendations on urology of care during the COVID-19 pandemic | EAU | Evidence based | RAS feasible with: -minimum number of OR staff -adequate PPE -avoid positive pressurisation | 125 |
| Kimmig 2020 [29] | Gynaecology (SERGS) | International | April 2020 | 1 | Provide guidance for gynaecology surgery during the COVID-19 pandemic | ACS EAES EAU RCOG SAGES | Mixed-evidence based and expert consensus | RAS feasible Technical recommendations to reduce aerosolisation during RAS | 101 |
| Mun 2021 [30] | MIS-Abdominal | International | September 2020 | - | Evaluate guidelines and clinical activity regarding aerosolisation risk during the COVID-19 pandemic | ACS EAES EAU RCS SAGES | Mixed-evidence based and expert consensus | RAS feasible Lack of evidence that RAS increases risk of viral transmission | 121 |
| Navarra 2020 [31] | Metabolic Surgery | Italy | June 2020 | 3 | Recommendations for triage of surgical procedures in morbidly obese patients during the COVID-19 pandemic | ACS EAES SAGES | Mixed-evidence based and expert consensus | RAS allows for staff and surgeons to be remote from patient Use of ultralow particulate air filters encouraged | 105 |
| Poon 2021 [32] | Urology | China | April 2021 | - | Prostate cancer management recommendations | EAU | Mixed-evidence based and expert consensus | Screen patients for SARS-CoV-2 prior to RAS procedures Exercise caution regarding aerosolisation | 113 |
| Porter 2020 [33] | MIS | International | May 2020 | - | Recommendations to mitigate COVID-19 transmission during MIS | AAGL EAES EAU RCS RCSEd SAGES | Mixed-evidence based and expert consensus | Limit RAS to urgent/emergency procedures Mitigation of aerosolisation risk PPE and minimum OR staff | 105 |
| Sanchez-Guillen 2021 [34] | Coloproctology | Spain | June 2021 | 135 | Approach to robotic and transanal surgery peri-COVID-19 pandemic | ACPGBI EAES ESCP SAGES | Evidence based | RAS offers advantages, e.g., theatre staff safety (additional physical distance from patient) Risk reduction techniques should be exercised | 101 |
| Somashekhar 2021 [35] | MIS | International | November 2020 | 67 | Safety modifications to perform MIS during the COVID-19 pandemic | ACS EAES EAU SAGES | Evidence based | Low risk of transmission during RAS Barrier benefits to surgeons and OR staff Minimises aerosolisation | 121 |
| Tommaselli 2021 [36] | MIS | USA | December 2021 | - | Critically appraise recommendations on measures to reduce the risk of SARS-CoV-2 transmission to OR staff during MIS | ACS EAES EAU RCS RCSEd SAGES | Evidence based | RAS should be performed when needed Strategies to minimise aerosolisation | 97 |
| Vigneswaran 2020 [37] | MIS | USA | April 2020 | Same day | Evaluate safety and use of MIS during the COVID-19 pandemic | SAGES | Evidence based | RAS feasible Strategies to minimise aerosolisation | 96 |
| Zampolli 2020 [38] | MIS | International | May 2020 | 15 | Risk of viral transmission during MIS | - | Evidence based | RAS considered safe Modification of standard procedures to reduce aerosolisation | 92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fleming, C.A.; Fullard, A.; Croghan, S.; Pellino, G.; Pata, F. Robotic Abdominal Surgery and COVID-19: A Systematic Review of Published Literature and Peer-Reviewed Guidelines during the SARS-CoV-2 Pandemic. J. Clin. Med. 2022, 11, 2957. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112957
Fleming CA, Fullard A, Croghan S, Pellino G, Pata F. Robotic Abdominal Surgery and COVID-19: A Systematic Review of Published Literature and Peer-Reviewed Guidelines during the SARS-CoV-2 Pandemic. Journal of Clinical Medicine. 2022; 11(11):2957. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112957
Chicago/Turabian StyleFleming, Christina A., Anna Fullard, Stefanie Croghan, Gianluca Pellino, and Francesco Pata. 2022. "Robotic Abdominal Surgery and COVID-19: A Systematic Review of Published Literature and Peer-Reviewed Guidelines during the SARS-CoV-2 Pandemic" Journal of Clinical Medicine 11, no. 11: 2957. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11112957