
Home-Based Nonoperative-Side Quadriceps Neuromuscular Electrical Stimulation Prevents Muscle Weakness Following Anterior Cruciate Ligament Reconstruction


Abstract
:1. Introduction
2. Materials and Methods
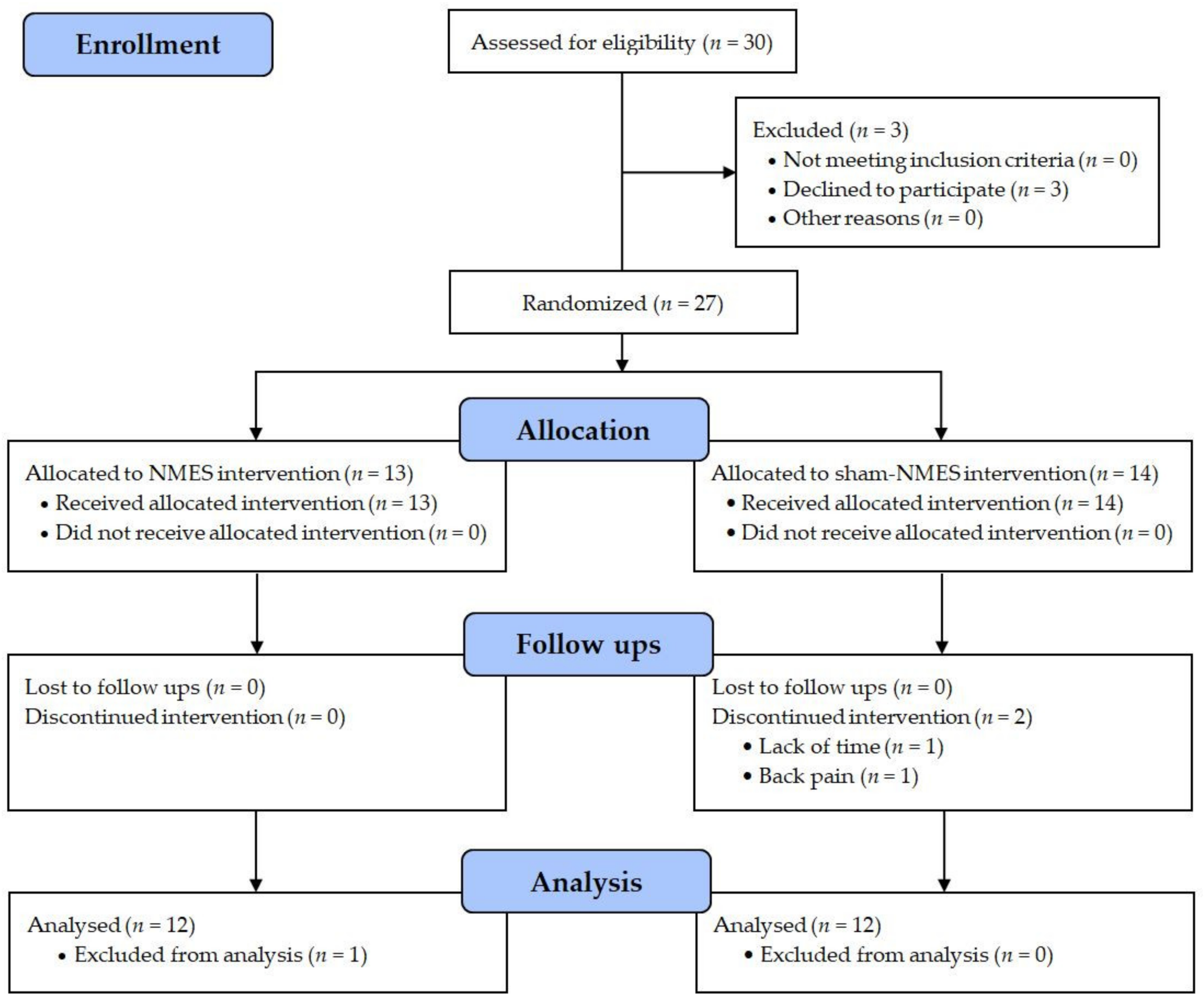
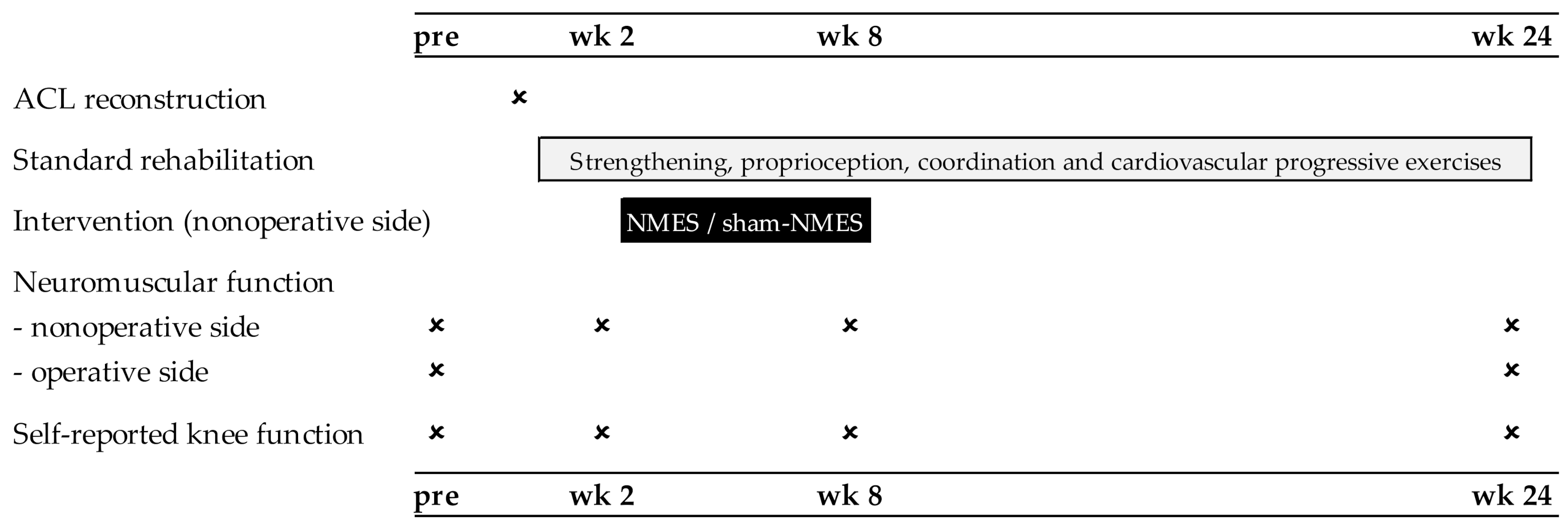
2.1. Patients and Study Design
2.2. Standard Rehabilitation Program
2.3. Interventions (NMES and Sham-NMES)
2.4. Assessments
2.5. Knee Extensor Strength
2.6. Quadriceps Voluntary Activation and Muscle Thickness
2.7. Self-Reported Knee Function
2.8. Statistics
3. Results
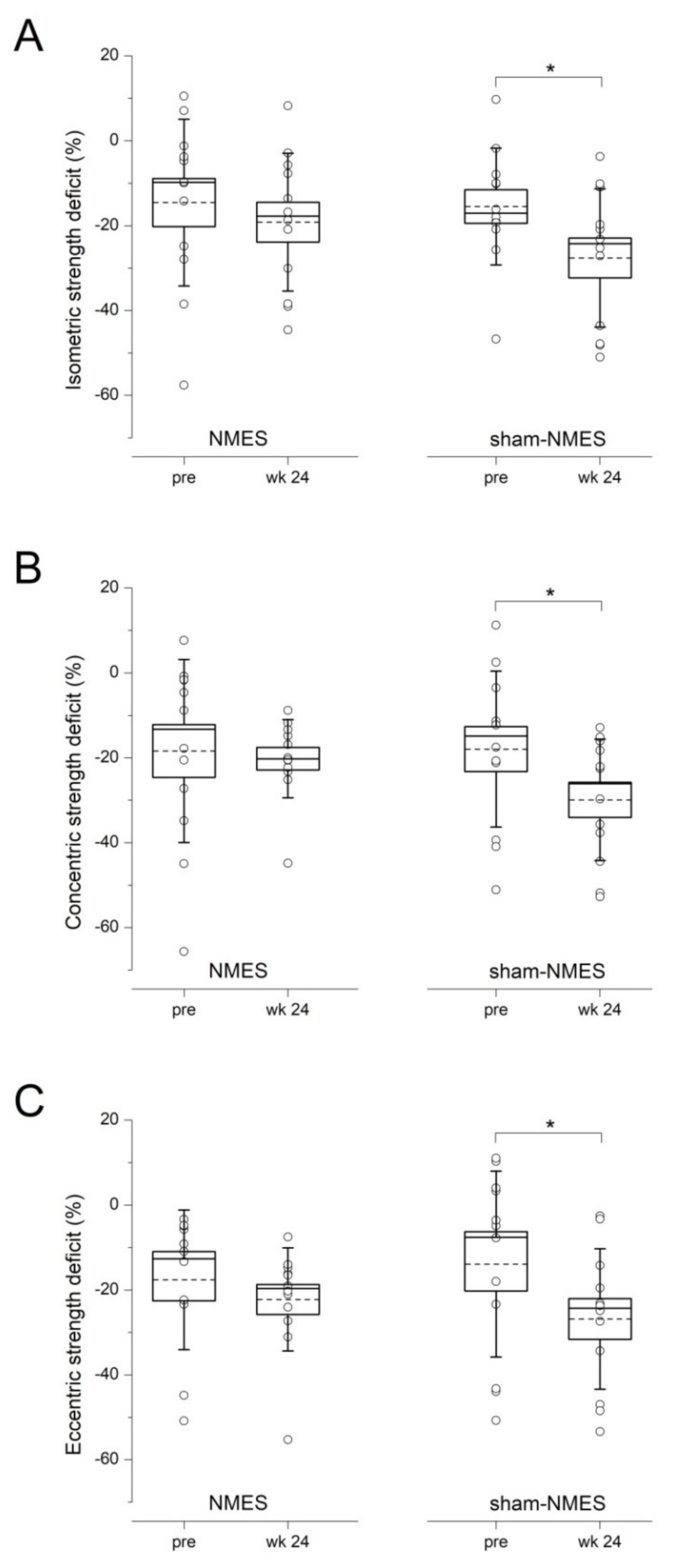
3.1. Primary Outcomes
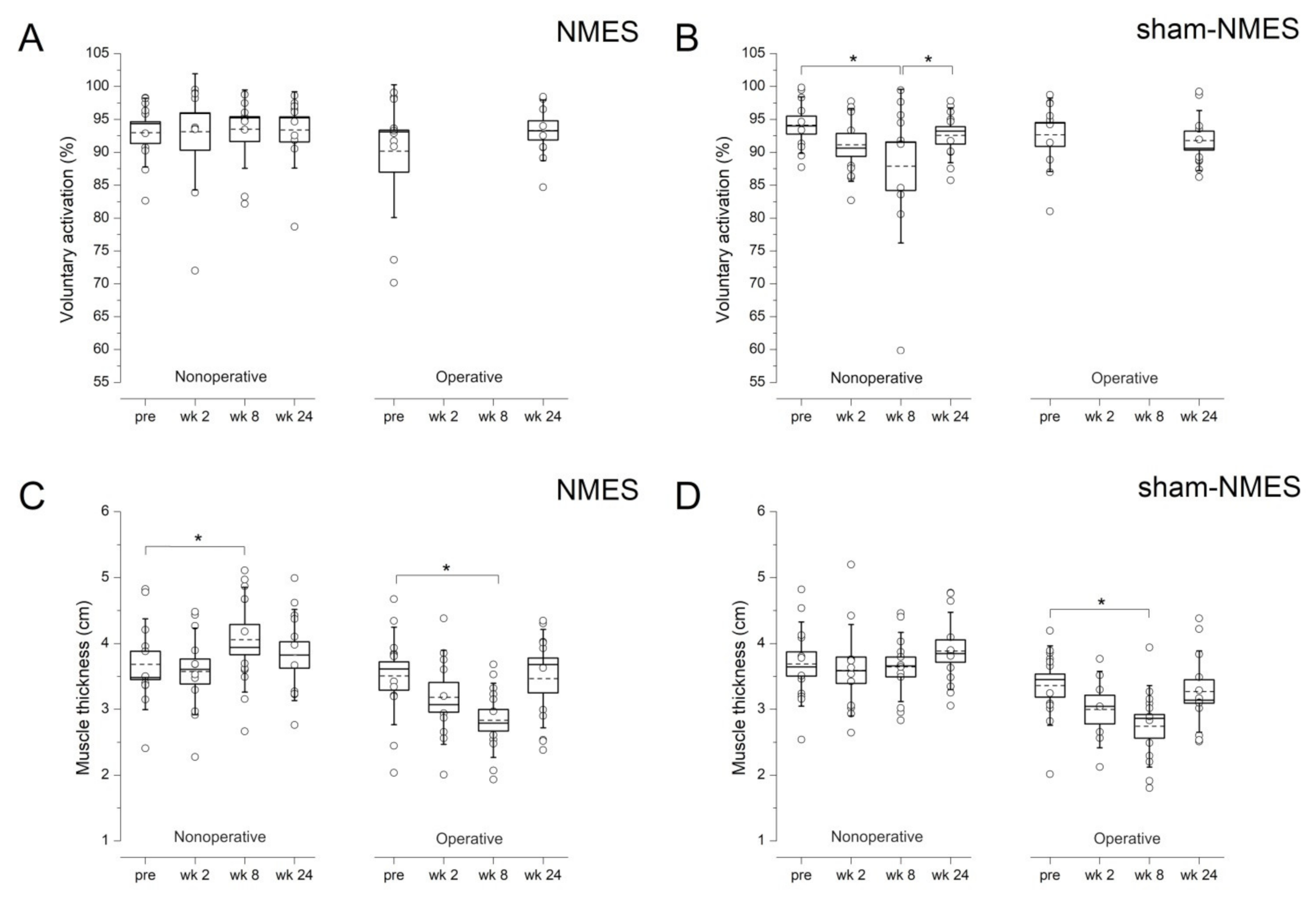
3.2. Secondary Outcomes
4. Discussion
4.1. Main Findings
4.2. NMES Prevented Muscle Weakness 6 Months after Surgery
4.3. NMES Preserved Activation and Increased Mass of the Stimulated Muscle
4.4. NMES Did Not Influence Self-Reported Function
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manca, A.; Dragone, D.; Dvir, Z.; Deriu, F. Cross-education of muscular strength following unilateral resistance training: A meta-analysis. Eur. J. Appl. Physiol. 2017, 117, 2335–2354. [Google Scholar] [CrossRef]
- Munn, J.; Herbert, R.D.; Gandevia, S.C. Contralateral effects of unilateral resistance training: A meta-analysis. J. Appl. Physiol. 2004, 96, 1861–1866. [Google Scholar] [CrossRef]
- Hendy, A.M.; Lamon, S. The cross-education phenomenon: Brain and beyond. Front. Physiol. 2017, 8, 297. [Google Scholar] [CrossRef] [Green Version]
- Hortobagyi, T.; Scott, K.; Lambert, J.; Hamilton, G.; Tracy, J. Cross-education of muscle strength is greater with stimulated than voluntary contractions. Mot. Control 1999, 3, 205–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, L.A.; Gabriel, D.A. The effect of unilateral training on contralateral limb strength in young, older, and patient populations: A meta-analysis of cross education. Phys. Ther. Rev. 2018, 23, 238–249. [Google Scholar] [CrossRef]
- Farthing, J.P.; Zehr, E.P. Restoring symmetry: Clinical applications of cross-education. Exerc. Sport Sci. Rev. 2014, 42, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Hendy, A.M.; Spittle, M.; Kidgell, D.J. Cross education and immobilisation: Mechanisms and implications for injury rehabilitation. J. Sci. Med. Sport 2012, 15, 94–101. [Google Scholar] [CrossRef]
- Palmieri-Smith, R.M.; Thomas, A.C.; Wojtys, E.M. Maximizing quadriceps strength after ACL reconstruction. Clin. Sports Med. 2008, 27, 405–424. [Google Scholar] [CrossRef]
- Schmitt, L.C.; Paterno, M.V.; Hewett, T.E. The impact of quadriceps femoris strength asymmetry on functional performance at return to sport following anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 2012, 42, 750–759. [Google Scholar] [CrossRef] [Green Version]
- Harput, G.; Ulusoy, B.; Yildiz, T.I.; Demirci, S.; Eraslan, L.; Turhan, E.; Tunay, V.B. Cross-education improves quadriceps strength recovery after ACL reconstruction: A randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 68–75. [Google Scholar] [CrossRef]
- Minshull, C.; Gallacher, P.; Roberts, S.; Barnett, A.; Kuiper, J.H.; Bailey, A. Contralateral strength training attenuates muscle performance loss following anterior cruciate ligament (ACL) reconstruction: A randomised-controlled trial. Eur. J. Appl. Physiol. 2021, 121, 3551–3559. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, M.; Billis, E.; Papathanasiou, G.; Spyropoulos, P.; Papaioannou, N. Cross-exercise on quadriceps deficit after ACL reconstruction. J. Knee Surg. 2013, 26, 51–58. [Google Scholar]
- Zult, T.; Gokeler, A.; van Raay, J.; Brouwer, R.W.; Zijdewind, I.; Farthing, J.P.; Hortobagyi, T. Cross-education does not accelerate the rehabilitation of neuromuscular functions after ACL reconstruction: A randomized controlled clinical trial. Eur. J. Appl. Physiol. 2018, 118, 1609–1623. [Google Scholar] [CrossRef] [Green Version]
- van Melick, N.; van Cingel, R.E.; Brooijmans, F.; Neeter, C.; van Tienen, T.; Hullegie, W.; Nijhuis-van der Sanden, M.W. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br. J. Sports Med. 2016, 50, 1506–1515. [Google Scholar] [CrossRef] [Green Version]
- Gregory, C.M.; Bickel, C.S. Recruitment patterns in human skeletal muscle during electrical stimulation. Phys. Ther. 2005, 85, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Huber, R.; Viecelli, C.; Bizzini, M.; Friesenbichler, B.; Dohm-Acker, M.; Rosenheck, T.; Harder, L.; Maffiuletti, N.A. Knee extensor and flexor strength before and after anterior cruciate ligament reconstruction in a large sample of patients: Influence of graft type. Phys. Sportsmed. 2019, 47, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Bizzini, M.; Gorelick, M.; Munzinger, U.; Drobny, T. Joint laxity and isokinetic thigh muscle strength characteristics after anterior cruciate ligament reconstruction: Bone patellar tendon bone versus quadrupled hamstring autografts. Clin. J. Sport Med. 2006, 16, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Feil, S.; Newell, J.; Minogue, C.; Paessler, H.H. The effectiveness of supplementing a standard rehabilitation program with superimposed neuromuscular electrical stimulation after anterior cruciate ligament reconstruction: A prospective, randomized, single-blind study. Am. J. Sports Med. 2011, 39, 1238–1247. [Google Scholar] [CrossRef]
- Fitzgerald, G.K.; Piva, S.R.; Irrgang, J.J. A modified neuromuscular electrical stimulation protocol for quadriceps strength training following anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 2003, 33, 492–501. [Google Scholar] [CrossRef] [Green Version]
- Maffiuletti, N.A.; Gondin, J.; Place, N.; Stevens-Lapsley, J.; Vivodtzev, I.; Minetto, M.A. Clinical use of neuromuscular electrical stimulation for neuromuscular rehabilitation: What are we overlooking? Arch. Phys. Med. Rehabil. 2018, 99, 806–812. [Google Scholar] [CrossRef]
- Nuhr, M.; Crevenna, R.; Gohlsch, B.; Bittner, C.; Pleiner, J.; Wiesinger, G.; Fialka-Moser, V.; Quittan, M.; Pette, D. Functional and biochemical properties of chronically stimulated human skeletal muscle. Eur. J. Appl. Physiol. 2003, 89, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Maffiuletti, N.A. Assessment of hip and knee muscle function in orthopaedic practice and research. J. Bone Joint Surg. Am. 2010, 92, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Wellauer, V.; Morf, C.; Minetto, M.A.; Place, N.; Maffiuletti, N.A. Assessment of quadriceps muscle inactivation with a new electrical stimulation paradigm. Muscle Nerve 2015, 51, 117–124. [Google Scholar] [CrossRef]
- Casartelli, N.C.; Item-Glatthorn, J.F.; Friesenbichler, B.; Bizzini, M.; Salzmann, G.M.; Maffiuletti, N.A. Quadriceps Neuromuscular Impairments after Arthroscopic Knee Surgery: Comparison between Procedures. J. Clin. Med. 2019, 8, 1881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roos, E.M.; Lohmander, L.S. The knee injury and osteoarthritis outcome score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [Green Version]
- Ageberg, E.; Forssblad, M.; Herbertsson, P.; Roos, E.M. Sex differences in patient-reported outcomes after anterior cruciate ligament reconstruction: Data from the Swedish knee ligament register. Am. J. Sports Med. 2010, 38, 1334–1342. [Google Scholar] [CrossRef]
- Hendy, A.M.; Chye, L.; Teo, W.P. Cross-activation of the motor cortex during unilateral contractions of the quadriceps. Front. Hum. Neurosci. 2017, 11, 397. [Google Scholar] [CrossRef] [Green Version]
- Valdes, O.; Ramirez, C.; Perez, F.; Garcia-Vicencio, S.; Nosaka, K.; Penailillo, L. Contralateral effects of eccentric resistance training on immobilized arm. Scand. J. Med. Sci. Sports 2021, 31, 76–90. [Google Scholar] [CrossRef]
- Lexell, J.; Henriksson-Larsen, K.; Sjostrom, M. Distribution of different fibre types in human skeletal muscles. 2. A study of cross-sections of whole m. vastus lateralis. Acta Physiol. Scand. 1983, 117, 115–122. [Google Scholar] [CrossRef]
- Hart, J.M.; Pietrosimone, B.; Hertel, J.; Ingersoll, C.D. Quadriceps activation following knee injuries: A systematic review. J. Athl. Train. 2010, 45, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Gruther, W.; Benesch, T.; Zorn, C.; Paternostro-Sluga, T.; Quittan, M.; Fialka-Moser, V.; Spiss, C.; Kainberger, F.; Crevenna, R. Muscle wasting in intensive care patients: Ultrasound observation of the M. quadriceps femoris muscle layer. J. Rehabil. Med. 2008, 40, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Shiba, N.; Matsuse, H.; Takano, Y.; Yoshimitsu, K.; Omoto, M.; Hashida, R.; Tagawa, Y.; Inada, T.; Yamada, S.; Ohshima, H. Electrically stimulated antagonist muscle contraction increased muscle mass and bone mineral density of one astronaut—Initial verification on the international space station. PLoS ONE 2015, 10, e0134736. [Google Scholar]
- Maffiuletti, N.A.; Green, D.A.; Vaz, M.A.; Dirks, M.L. Neuromuscular electrical stimulation as a potential countermeasure for skeletal muscle atrophy and weakness during human spaceflight. Front. Physiol. 2019, 10, 1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papandreou, M.G.; Billis, E.V.; Antonogiannakis, E.M.; Papaioannou, N.A. Effect of cross exercise on quadriceps acceleration reaction time and subjective scores (Lysholm questionnaire) following anterior cruciate ligament reconstruction. J. Orthop. Surg. Res. 2009, 4, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spector, P.; Laufer, Y.; Elboim Gabyzon, M.; Kittelson, A.; Stevens Lapsley, J.; Maffiuletti, N.A. Neuromuscular electrical stimulation therapy to restore quadriceps muscle function in patients after orthopaedic surgery: A novel structured approach. J. Bone Joint Surg. Am. 2016, 98, 2017–2024. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NMES (n = 12) | Sham-NMES (n = 12) | p-Value (t-Test) | |
|---|---|---|---|
| Number of women/men | 5/7 | 5/7 | - |
| Age (years) | 29 ± 6 | 30 ± 11 | 0.64 |
| Height (cm) | 172 ± 8 | 171 ± 6 | 0.56 |
| Weight (kg) | 68 ± 13 | 71 ± 14 | 0.56 |
| Time from injury to surgery (months) | 7 ± 8 | 8 ± 5 | 0.77 |
| Number of HTG/PTG | 11/1 | 9/3 | - |
| Number of partial meniscectomies | 6 | 5 | - |
| Number of cartilage repairs | 1 | 1 | - |
| Preinjury Tegner score (0–10) | 6.5 ± 1.7 | 7.2 ± 1.2 | 0.58 |
| Preoperative Tegner score (0–10) | 3.5 ± 1.7 | 3.6 ± 1.6 | 0.70 |
| Group | Side | Pre | Week 2 | Week 8 | Week 24 | |
|---|---|---|---|---|---|---|
| Isometric strength | NMES | Nonoperative | 216 ± 74 | 206 ± 72 a | 197 ± 72 a | 217 ± 77 |
| (Nm) | NMES | Operative | 188 ± 82 * | / | / | 184 ± 70 * |
| sham-NMES | Nonoperative | 204 ± 53 | 186 ± 52 a | 195 ± 56 a | 212 ± 62 | |
| sham-NMES | Operative | 165 ± 56 * | / | / | 155 ± 63 * | |
| Concentric strength | NMES | Nonoperative | 190 ± 55 | 188 ± 55 | 188 ± 56 | 209 ± 11 b |
| (Nm) | NMES | Operative | 158 ± 63 * | / | / | 169 ± 57 * |
| sham-NMES | Nonoperative | 181 ± 49 | 181 ± 44 | 186 ± 45 | 199 ± 54 b | |
| sham-NMES | Operative | 148 ± 49 * | / | / | 141 ± 55 * | |
| Eccentric strength | NMES | Nonoperative | 260 ± 77 | 260 ± 82 | 266 ± 78 c | 286 ± 86 d |
| (Nm) | NMES | Operative | 219 ± 88 * | / | / | 224 ± 78 * |
| sham-NMES | Nonoperative | 232 ± 50 | 240 ± 55 | 253 ± 56 c | 244 ± 49 d | |
| sham-NMES | Operative | 198 ± 57 * | / | / | 178 ± 53 * |
| Group | Pre | Week 2 | Week 8 | Week 24 | |
|---|---|---|---|---|---|
| Pain (0–100) | NMES | 88 ± 13 | 66 ± 17 a | 77 ± 16 bc | 87 ± 11 |
| sham-NMES | 79 ± 14 | 66 ± 17 a | 73 ± 7 bc | 85 ± 9 | |
| Symptoms (0–100) | NMES | 80 ± 14 | 54 ± 12 a | 72 ± 17 bc | 84 ± 13 |
| sham-NMES | 74 ± 20 | 49 ± 13 a | 60 ± 17 bc | 79 ± 14 | |
| Activities daily living (0–100) | NMES | 96 ± 5 | 65 ± 18 a | 90 ± 7 bc | 98 ± 3 |
| sham-NMES | 93 ± 10 | 56 ± 16 a | 87 ± 9 bc | 97 ± 3 | |
| Quality of life (0–100) | NMES | 39 ± 15 d | 20 ± 15 a | 41 ± 20 d | 54 ± 23 |
| sham-NMES | 33 ± 16 d | 16 ± 12 a | 35 ± 18 d | 53 ± 22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wellauer, V.; Item, J.F.; Bizzini, M.; Maffiuletti, N.A. Home-Based Nonoperative-Side Quadriceps Neuromuscular Electrical Stimulation Prevents Muscle Weakness Following Anterior Cruciate Ligament Reconstruction. J. Clin. Med. 2022, 11, 466. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020466
Wellauer V, Item JF, Bizzini M, Maffiuletti NA. Home-Based Nonoperative-Side Quadriceps Neuromuscular Electrical Stimulation Prevents Muscle Weakness Following Anterior Cruciate Ligament Reconstruction. Journal of Clinical Medicine. 2022; 11(2):466. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020466
Chicago/Turabian StyleWellauer, Vanessa, Julia F. Item, Mario Bizzini, and Nicola A. Maffiuletti. 2022. "Home-Based Nonoperative-Side Quadriceps Neuromuscular Electrical Stimulation Prevents Muscle Weakness Following Anterior Cruciate Ligament Reconstruction" Journal of Clinical Medicine 11, no. 2: 466. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11020466