
The Relation between Negative Automatic Thoughts and Psychological Inflexibility in Schizophrenia

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Demographics
3.2. Preliminary Analyses
3.3. Differences between Individuals with Schizophrenia and Individuals with End-Stage CKD
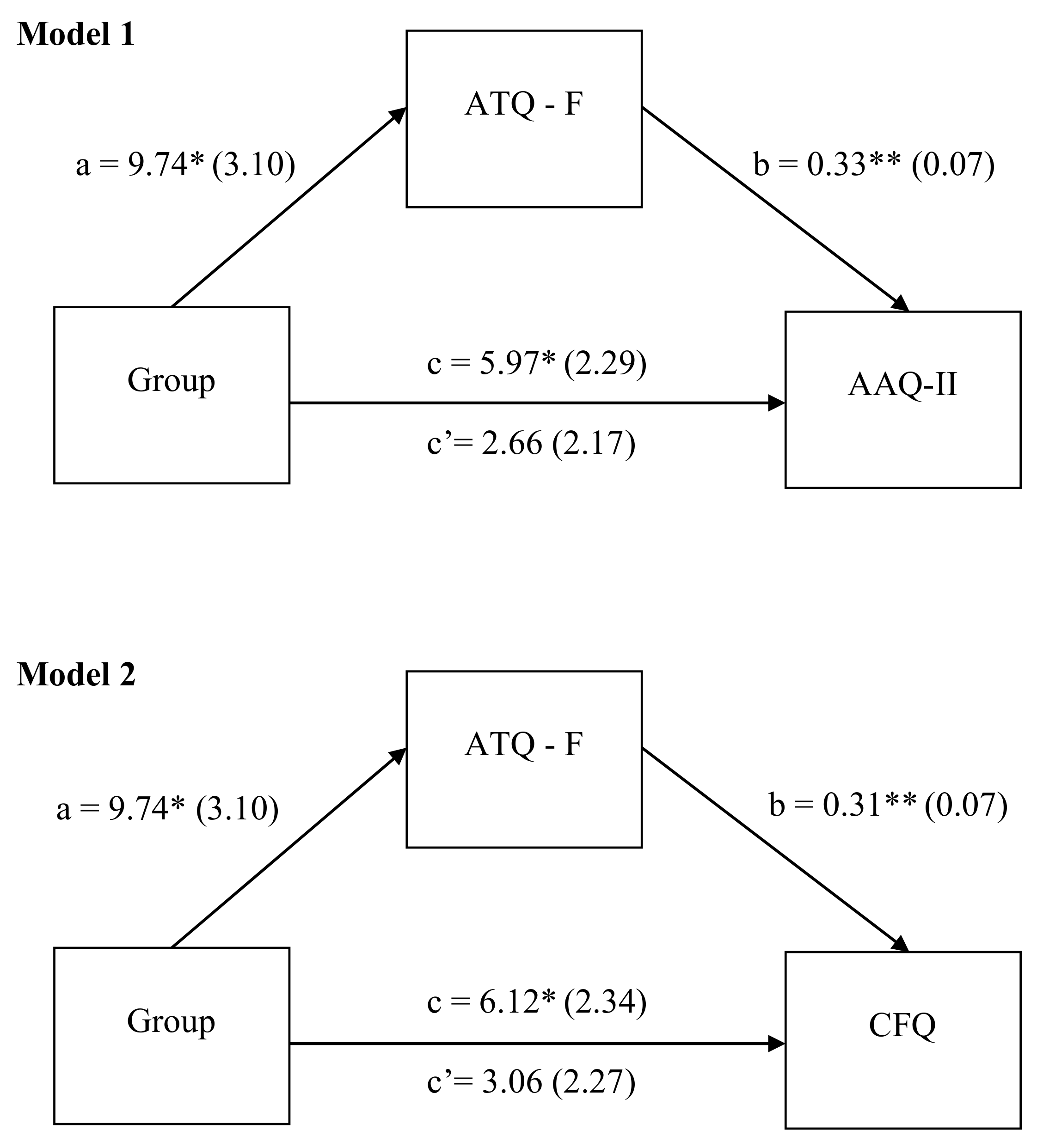
Negative Automatic Thoughts as a Specific Pathway to Experiential Avoidance and Cognitive Fusion
4. Discussion
4.1. Clinical Implications of This Study
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Billeke, P.; Aboitiz, F. Social Cognition in Schizophrenia: From Social Stimuli Processing to Social Engagement. Front. Psychiatry 2013, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Davis, B.J.; Lysaker, P.H.; Salyers, M.P.; Minor, K.S. The insight paradox in schizophrenia: A meta-analysis of the relationship between clinical insight and quality of life. Schizophr. Res. 2020, 223, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Ventura, J.; Subotnik, K.L.; Gitlin, M.J.; Gretchen-Doorly, D.; Ered, A.; Villa, K.F.; Hellemann, G.S.; Nuechterlein, K.H. Negative symptoms and functioning during the first year after a recent onset of schizophrenia and 8years later. Schizophr. Res. 2015, 161, 407–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, C.H.; Harvey, C.J. Systematic review: The relationship between sleep spindle activity with cognitive functions, positive and negative symptoms in psychosis. Sleep Med. X 2020, 2, 100025. [Google Scholar] [CrossRef] [PubMed]
- Ienciu, M.; Romoşan, F.; Bredicean, C.; Romoşan, R. First episode psychosis and treatment delay—Causes and consequences. Psychiatr. Danub. 2010, 22, 540–543. [Google Scholar]
- Moreno-Küstner, B.; Martín, C.; Pastor, L. Prevalence of psychotic disorders and its association with methodological issues. A systematic review and meta-analyses. PLoS ONE 2018, 13, e0195687. [Google Scholar] [CrossRef]
- Fatouros-Bergman, H.; Cervenka, S.; Flyckt, L.; Edman, G.; Farde, L. Meta-analysis of cognitive performance in drug-naïve patients with schizophrenia. Schizophr. Res. 2014, 158, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Karyakina, M.; Shmukler, A. Network analysis of cognitive deficit in patients with schizophrenia spectrum disorders. Schizophr. Res. Cogn. 2021, 26, 100213. [Google Scholar] [CrossRef]
- Maat, A.; Fett, A.K.; Derks, E.; GROUP Investigators. Social cognition and quality of life in schizophrenia. Schizophr. Res. 2012, 137, 212–218. [Google Scholar] [CrossRef]
- Tas, C.; Brown, E.; Cubukcuoglu, Z.; Aydemir, O.; Danaci, A.E.; Brüne, M. Towards an integrative approach to understanding quality of life in schizophrenia: The role of neurocognition, social cognition, and psychopathology. Compr. Psychiatry 2013, 54, 262–268. [Google Scholar] [CrossRef]
- Beck, A.T.; Rector, N.A.; Stolar, N.; Grant, P. Schizophrenia: Cognitive Theory, Research, and Therapy; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Bach, P.; Hayes, S.C. The use of acceptance and commitment therapy to prevent the rehospitalization of psychotic patients: A randomized controlled trial. J. Consult. Clin. Psychol. 2002, 70, 1129–1139. [Google Scholar] [CrossRef]
- Beck, J. Cognitive Behavior Therapy, Third Edition: Basics and Beyond, 3rd ed.; Guilford Press: New York, NY, USA, 2021. [Google Scholar]
- Livet, A.; Navarri, X.; Potvin, S.; Conrod, P. Cognitive biases in individuals with psychotic-like experiences: A systematic review and a meta-analysis. Schizophr. Res. 2020, 222, 10–22. [Google Scholar] [CrossRef]
- Pot-Kolder, R.; Veling, W.; Counotte, J.; van der Gaag, M. Self-reported Cognitive Biases Moderate the Associations between Social Stress and Paranoid Ideation in a Virtual Reality Experimental Study. Schizophr. Bull. 2018, 44, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Brown, G.; Steer, R.A.; Weissman, A.N. Factor analysis of the dysfunctional attitude scale in a clinical population. J. Consult. Clin. Psychol. 1991, 3, 478–483. [Google Scholar] [CrossRef]
- Rector, N.A.; Beck, A.T. A clinical review of cognitive therapy for schizophrenia. Curr. Psychiatry Rep. 2002, 4, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.L.; Averbeck, B.B.; Furl, N. Jumping to conclusions in schizophrenia. Neuropsychiatr. Dis. Treat. 2015, 11, 1615–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rausch, F.; Eisenacher, S.; Elkin, H.; Englisch, S.; Kayser, S.; Striepens, N.; Lautenschlager, M.; Heinz, A.; Gudlowski, Y.; Janssen, B.; et al. Evaluation of the ‘Jumping to conclusions’ bias in different subgroups of the at-risk mental state: From cognitive basic symptoms to UHR criteria. Psychol. Med. 2016, 46, 2071–2081. [Google Scholar] [CrossRef]
- Moritz, S.; Lysaker, P.H. Metacognition Research in Psychosis: Uncovering and Adjusting the Prisms That Distort Subjective Reality. Schizophr. Bull. 2019, 45, 17–18. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive Therapy and the Emotional Disorders; Meridian: New York, NY, USA, 1976. [Google Scholar]
- Lysaker, P.H.; Chernov, N.; Moiseeva, T.; Sozinova, M.; Dmitryeva, N.; Alyoshin, V.; Luther, L.; Karpenko, O.; Kostyuk, G. Clinical insight, cognitive insight and metacognition in psychosis: Evidence of mediation. J. Psychiatr. Res. 2021, 140, 1–6. [Google Scholar] [CrossRef]
- Harris, R.; Hayes, S. ACT Made Simple: An Easy-to-Read Primer on Acceptance and Commitment Therapy; New Harbinger Publications: Oackland, CA, USA, 2019. [Google Scholar]
- Hayes, S.C.; Strosahl, K.D.; Bunting, K.; Twohig, M.; Wilson, K.G. What is acceptance and commitment therapy? In A Practical Guide to Acceptance and Commitment Therapy; Springer: New York, NY, USA, 2004; pp. 3–29. [Google Scholar]
- Gaudiano, B.A.; Herbert, J.D.; Hayes, S.C. Is It the Symptom or the Relation to It? Investigating Potential Mediators of Change in Acceptance and Commitment Therapy for Psychosis. Behav. Ther. 2010, 41, 543–554. [Google Scholar] [CrossRef] [Green Version]
- Bacon, T.; Farhall, J.; Fossey, E. The Active Therapeutic Processes of Acceptance and Commitment Therapy for Persistent Symptoms of Psychosis: Clients’ Perspectives. Behav. Cogn. Psychother. 2014, 42, 402–420. [Google Scholar] [CrossRef]
- Gaudiano, B.A.; Davis, C.H.; Epstein-Lubow, G.; Johnson, J.E.; Mueser, K.T.; Miller, I.W. Acceptance and Commitment Therapy for Inpatients with Psychosis (the REACH Study): Protocol for Treatment Development and Pilot Testing. Healthcare 2017, 5, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Mieres, H.; Usall, J.; Feixas, G.; Ochoa, S. Placing Cognitive Rigidity in Interpersonal Context in Psychosis: Relationship with Low Cognitive Reserve and High Self-Certainty. Front. Psychiatry 2020, 11, 1308. [Google Scholar] [CrossRef] [PubMed]
- Gillanders, D.; Bolderston, H.; Bond, F.W.; Dempster, M.; Flaxman, P.E.; Campbell, L.; Remington, B. The development and initial validation of the Cognitive Fusion Questionnaire. Behav. Ther. 2014, 45, 83–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, E.M.J. Acceptance and Commitment Therapy. In CBT for Psychosis: Process-Orientated Therapies and the Third Wave; Cupitt, C., Ed.; Routledge: London, UK, 2019. [Google Scholar]
- Popa, C.O.; Predatu, R.; Lee, W.C.; Blaga, P.; Sirbu, E.; Rus, A.V.; Clark, A.; Cojocaru, C.; Schenk, A.; Vacaras, V.; et al. Thought Suppression in Primary Psychotic Disorders and Substance/Medication Induced Psychotic Disorder. Int. J. Environ. Res. Public Health 2021, 18, 116. [Google Scholar] [CrossRef]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and commitment therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Masuda, A.; Bissett, R.; Luoma, J.B.; Guerrero, L.F. DBT, FAP, and ACT: How empirically oriented are the new behavior therapy technologies? Behav. Ther. 2004, 35, 35–54. [Google Scholar] [CrossRef] [Green Version]
- Núñez, D.; Ordóñez-Carrasco, J.L.; Fuentes, R.; Langer, Á.I. Experiential avoidance mediates the association between paranoid ideation and depressive symptoms in a sample from the general population. J. Psychiatr. Res. 2021, 139, 120–124. [Google Scholar] [CrossRef]
- Valiente, C.; Provencio, M.; Espinosa, R.; Duque, A.; Everts, F. Insight in paranoia: The role of experiential avoidance and internalized stigma. Schizophr. Res. 2015, 164, 214–220. [Google Scholar] [CrossRef]
- Probst, T.; Baumeister, H.; McCracken, L.M.; Lin, J. Baseline Psychological Inflexibility Moderates the Outcome Pain Interference in a Randomized Controlled Trial on Internet-based Acceptance and Commitment Therapy for Chronic Pain. J. Clin. Med. 2019, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Güner, M.C.; Menekşe, S.Y.; Kumru, Ş.M. Cognitive predictors of depression and anxiety in individuals with newly diagnosed Multiple Sclerosis. Eur. J. Psychiatry 2020, 34, 202–210. [Google Scholar] [CrossRef]
- Berlin, K.S.; Keenan, M.E.; Cook, J.L.; Ankney, R.L.; Klages, K.L.; Semenkovich, K.; Rybak, T.M.; Banks, G.G.; Alemzadeh, R.; Eddington, A.R. Measuring psychological flexibility in youth with type 1 diabetes. Pediatr. Diabetes 2020, 21, 1566–1574. [Google Scholar] [CrossRef]
- Iida, H.; Fujimoto, S.; Wakita, T.; Yanagi, M.; Suzuki, T.; Koitabashi, K.; Yazawa, M.; Kawarazaki, H.; Ishibashi, Y.; Shibagaki, Y.; et al. Psychological Flexibility and Depression in Advanced CKD and Dialysis. Kidney Med. 2020, 2, 684–691.e1. [Google Scholar] [CrossRef] [PubMed]
- Drew, D.A. Psychological Flexibility: A Novel Risk Factor for Depression in Kidney Disease. Kidney Med. 2020, 2, 673–674. [Google Scholar] [CrossRef] [PubMed]
- Osberg, J.W.; Meares, G.J.; McKee, D.C.; Burnett, G.B. Intellectual functioning in renal failure and chronic dialysis. J. Chronic Dis. 1982, 35, 445–457. [Google Scholar] [CrossRef]
- Shirazian, S.; Grant, C.D.; Aina, O.; Mattana, J.; Khorassani, F.; Ricardo, A.C. Depression in Chronic Kidney Disease and End-Stage Renal Disease: Similarities and Differences in Diagnosis, Epidemiology, and Management. Kidney Int. Rep. 2016, 2, 94–107. [Google Scholar] [CrossRef] [Green Version]
- Deckler, E.; Hodgins, G.E.; Pinkham, A.E.; Penn, D.L.; Harvey, P.D. Social Cognition and Neurocognition in Schizophrenia and Healthy Controls: Intercorrelations of Performance and Effects of Manipulations Aimed at Increasing Task Difficulty. Front. Psychiatry 2018, 9, 356. [Google Scholar] [CrossRef] [Green Version]
- Häfner, H.; Maurer, K.; Trendler, G.; an der Heiden, W.; Schmidt, M.; Könnecke, R. Schizophrenia and depression: Challenging the paradigm of two separate diseases—A controlled study of schizophrenia, depression and healthy controls. Schizophr. Res. 2005, 77, 11–24. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Williams, J.B.; Karg, R.S.; Spitzer, R.L. SCID-5-CV: Structured Clinical Interview for DSM-5 Disorders: Clinician Version; American Psychiatric Association Publishing: Washington, DC, USA, 2016. [Google Scholar]
- Hollon, S.D.; Kendall, P.C. Cognitive self-statements in depression: Development of an automatic thoughts questionnaire. Cognit. Ther. Res. 1980, 4, 383–395. [Google Scholar] [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary Psychometric Properties of the Acceptance and Action Questionnaire–II: A Revised Measure of Psychological Inflexibility and Experiential Avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef] [Green Version]
- Osório, F.L.; Loureiro, S.R.; Hallak, J.E.C.; Machado-de-Sousa, J.P.; Ushirohira, J.M.; Baes, C.V.W.; Apolinario, T.D.; Donadon, M.F.; Bolsoni, L.M.; Guimarães, T.; et al. Clinical validity and intrarater and test–retest reliability of the Structured Clinical Interview for DSM-5–Clinician Version (SCID-5-CV). Psychiatry Clin. Neurosci. 2019, 73, 754–760. [Google Scholar] [CrossRef]
- Stefan, S.; Cristea, I.A.; Szentagotai Tatar, A.; David, D. Cognitive-behavioral therapy (CBT) for generalized anxiety disorder: Contrasting various CBT approaches in a randomized clinical trial. J. Clin. Psychol. 2019, 75, 1188–1202. [Google Scholar] [CrossRef]
- Zettle, R.D.; Hayes, S.C. Dysfunctional control by client verbal behavior: The context of reason-giving. Anal. Verbal Behav. 1986, 4, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Netemeyer, R.G.; Williamson, D.A.; Burton, S.; Biswas, D.; Jindal, S.; Landreth, S.; Mills, G.; Primeaux, S. Psychometric Properties of Shortened Versions of the Automatic Thoughts Questionnaire. Educ. Psychol. Meas. 2002, 62, 111–129. [Google Scholar] [CrossRef]
- Moldovan, R. Chestionarul gandurilor automate Automatic thoughts questionnaire. In Sistem de Evaluare Clinica [Clinical Evaluation System]; David, D., Ed.; RTS Publishing: Cluj Napoca, România, 2007. [Google Scholar]
- David, D. Tratat de Psihoterapii Cognitive și Comportamentale (Ed. A III-a Revăzută și Adăugită); Editura Polirom: Iași, România, 2017. [Google Scholar]
- Flynn, M.K.; Hernandez, J.O.; Hebert, E.R.; James, K.K.; Kusick, M.K. Cognitive fusion among hispanic college students: Further validation of the Cognitive Fusion Questionnaire. J. Context. Behav. Sci. 2018, 7, 29–34. [Google Scholar] [CrossRef]
- Szabó, K.-G.; Vargha, J.-L.; Balázsi, R.; Bartalus, J.; Bogdan, V. Measuring Psychological Flexibility: Preliminary Data on the Psychometric Properties of the Romanian Version of the Acceptance and Action Questionnaire (AAQ-II). J. Cogn. Behav. Psychother. 2011, 11, 67–82. [Google Scholar]
- Takeda, T.; Nakataki, M.; Ohta, M.; Hamatani, S.; Matsuura, K.; Yoshida, R.; Kameoka, N.; Tominaga, T.; Umehara, H.; Kinoshita, M.; et al. Negative and positive self-thoughts predict subjective quality of life in people with schizophrenia. Neuropsychiatr. Dis. Treat. 2019, 15, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Budak, F.K.; Yildirim, T.; Özdemir, A. The effect of negative automatic thoughts on hope in patients with schizophrenia. Perspect. Psychiatr. Care 2021, 57, 936–940. [Google Scholar] [CrossRef]
- Beck, A.T.; Himelstein, R.; Grant, P.M. In and out of schizophrenia: Activation and deactivation of the negative and positive schemas. Schizophr. Res. 2019, 203, 55–61. [Google Scholar] [CrossRef]
- Mak, W.W.S.; Chio, F.H.N.; Chong, K.S.C.; Law, R.W. From Mindfulness to Personal Recovery: The Mediating Roles of Self-Warmth, Psychological Flexibility, and Valued Living. Mindfulness 2021, 12, 994–1001. [Google Scholar] [CrossRef]
- Castilho, P.; Martins, M.J.; Pinto, A.M.; Viegas, R.; Carvalho, S.; Madeira, N. Understanding the effect of attachment styles in paranoid ideation: The mediator role of experiential avoidance. J. Context. Behav. Sci. 2017, 6, 42–46. [Google Scholar] [CrossRef]
- Sedighi, M.; Mansouri, A.; Talaei, A. The relationship between transdiagnostic factors and psychotic symptoms in individuals with schizophrenia disorder. J. Fundam. Ment. Health 2019, 21, 183–193. [Google Scholar] [CrossRef]
- Lawlor, C.; Hepworth, C.; Smallwood, J.; Carter, B.; Jolley, S. Self-reported emotion regulation difficulties in people with psychosis compared with non-clinical controls: A systematic literature review. Clin. Psychol. Psychother. 2020, 27, 107–135. [Google Scholar] [CrossRef]
- Newman-Taylor, K.; Richardson, T.; Lees, R.; Petrilli, K.; Bolderston, H.; Hindocha, C.; Freeman, T.P.; Bloomfield, M.A.P. Cognitive fusion as a candidate psychological vulnerability factor for psychosis: An experimental study of acute ∆9-tetrahydrocannabinol (THC) intoxication. Psychosis 2021, 13, 167–174. [Google Scholar] [CrossRef]
- Krafft, J.; Levin, M.E. Does the Cognitive Fusion Questionnaire measure more than frequency of negative thoughts? J. Context. Behav. Sci. 2021, 22, 63–67. [Google Scholar] [CrossRef]
- Ruiz, F.J.; Odriozola-González, P. The role of psychological inflexibility in Beck’s cognitive model of depression in a sample of undergraduates. An. Psicol. 2016, 32, 441–447. [Google Scholar] [CrossRef]
- Cristea, I.A.; Montgomery, G.H.; Szamoskozi, Ş.; David, D. Key Constructs in “Classical” and “New Wave” Cognitive Behavioral Psychotherapies: Relationships among Each Other and with Emotional Distress. J. Clin. Psychol. 2013, 69, 584–599. [Google Scholar] [CrossRef]
- Moritz, S.; Balzan, R.P.; Bohn, F.; Veckenstedt, R.; Kolbeck, K.; Bierbrodt, J.; Dietrichkeit, M. Subjective versus objective cognition: Evidence for poor metacognitive monitoring in schizophrenia. Schizophr. Res. 2016, 178, 74–79. [Google Scholar] [CrossRef]
- Beck, A.T.; Grant, P.; Inverso, E.; Brinen, A.P.; Perivoliotis, D. Recovery-Oriented Cognitive Therapy for Serious Mental Health Conditions; Guilford Publications: New York, NY, USA, 2020. [Google Scholar]
- Moritz, S.; Klein, J.P.; Lysaker, P.H.; Mehl, S. Metacognitive and cognitive-behavioral interventions for psychosis: New developments. Dialogues Clin. Neurosci. 2019, 21, 309–317. [Google Scholar] [CrossRef]
- Morrison, A.; Renton, J.; Dunn, H.; Williams, S.; Bentall, R. Cognitive Therapy for Psychosis: A Formulation-Based Approach; Routledge: New York, NY, USA, 2004. [Google Scholar]
- Hayes, S.C.; Hofmann, S.G. “Third-wave” cognitive and behavioral therapies and the emergence of a process-based approach to intervention in psychiatry. World Psychiatry 2021, 20, 363–375. [Google Scholar] [CrossRef]
- Torrisi, S.A.; Laudani, S.; Contarini, G.; De Luca, A.; Geraci, F.; Managò, F.; Papaleo, F.; Salomone, S.; Drago, F.; Leggio, G.M. Dopamine, Cognitive Impairments and Second-Generation Antipsychotics: From Mechanistic Advances to More Personalized Treatments. Pharmaceuticals 2020, 13, 365. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample Characteristics | Individuals with Schizophrenia (n = 41) | Individuals with End-Stage CKD (n = 40) | Statistical Significance (χ2/t) | p |
|---|---|---|---|---|
| Gender n (%) female, χ2 | 23 (63.9) | 13 (36.1) | 4.56 | 0.033 |
| Age range, M (SD), t | 23–67 44.98 (11.74) | 44–75 60.38 (9.14) | 6.57 | 0.001 |
| Measure | Individuals with Schizophrenia (n = 41) M (SD) | Individuals with End-Stage CKD (n = 40) M (SD) | Statistical Significance (F) | Partial η2 |
|---|---|---|---|---|
| ATQ-F | 38.02 (16.79) | 28.27 (10.35) | F (1, 79) = 9.833; p = 0.002 | 0.111 |
| ATQ-C | 40.24 (17.95) | 33.20 (11.72) | F (1, 79) = 4.348; p = 0.040 | 0.052 |
| AAQ-II | 25.04 (12.17) | 19.07 (7.99) | F (1, 79) = 6.775; p = 0.011 | 0.079 |
| CFQ | 28.17 (12.07) | 20.12 (6.87) | F (1, 79) = 6.834; p = 0.011 | 0.080 |
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. ATQ-F | - | 0.833 ** | 0.511 ** | 0.396 * |
| 2. ATQ-C | - | 0.550 ** | 0.553 ** | |
| 3. AAQ-II | - | 0.801 ** | ||
| 4. CFQ | - |
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. ATQ-F | - | 0.420 ** | 0.329 * | 0.466 ** |
| 2. ATQ-C | - | 0.685 ** | 0.750 ** | |
| 3. AAQ-II | - | 0.815 ** | ||
| 4. CFQ | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popa, C.O.; Rus, A.V.; Lee, W.C.; Cojocaru, C.; Schenk, A.; Văcăraș, V.; Olah, P.; Mureșan, S.; Szasz, S.; Bredicean, C. The Relation between Negative Automatic Thoughts and Psychological Inflexibility in Schizophrenia. J. Clin. Med. 2022, 11, 871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030871
Popa CO, Rus AV, Lee WC, Cojocaru C, Schenk A, Văcăraș V, Olah P, Mureșan S, Szasz S, Bredicean C. The Relation between Negative Automatic Thoughts and Psychological Inflexibility in Schizophrenia. Journal of Clinical Medicine. 2022; 11(3):871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030871
Chicago/Turabian StylePopa, Cosmin O., Adrian V. Rus, Wesley C. Lee, Cristiana Cojocaru, Alina Schenk, Vitalie Văcăraș, Peter Olah, Simona Mureșan, Simona Szasz, and Cristina Bredicean. 2022. "The Relation between Negative Automatic Thoughts and Psychological Inflexibility in Schizophrenia" Journal of Clinical Medicine 11, no. 3: 871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030871