
Usefulness of the C2HEST Score in Predicting the Clinical Outcomes of COVID-19 in Diabetic and Non-Diabetic Cohorts

 , , , , , , ,
, , , , , , ,  , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Follow Up and Outcomes
2.3. C2HEST Score Stratification
- 0–1—low;
- 2–3—medium;
- ≥4—high.
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Studied Population and Comorbidities
3.2. Characteristics of the In-Hospital Laboratory Tests and Treatment Applied
3.2.1. Laboratory Assays
3.2.2. Specific Treatment Applied during the Hospitalization Period
3.2.3. Supportive Treatment Applied during Hospitalization
3.3. Associations of the C2HEST Score with Fatal Outcomes
3.3.1. C2HEST Score Results and Mortality
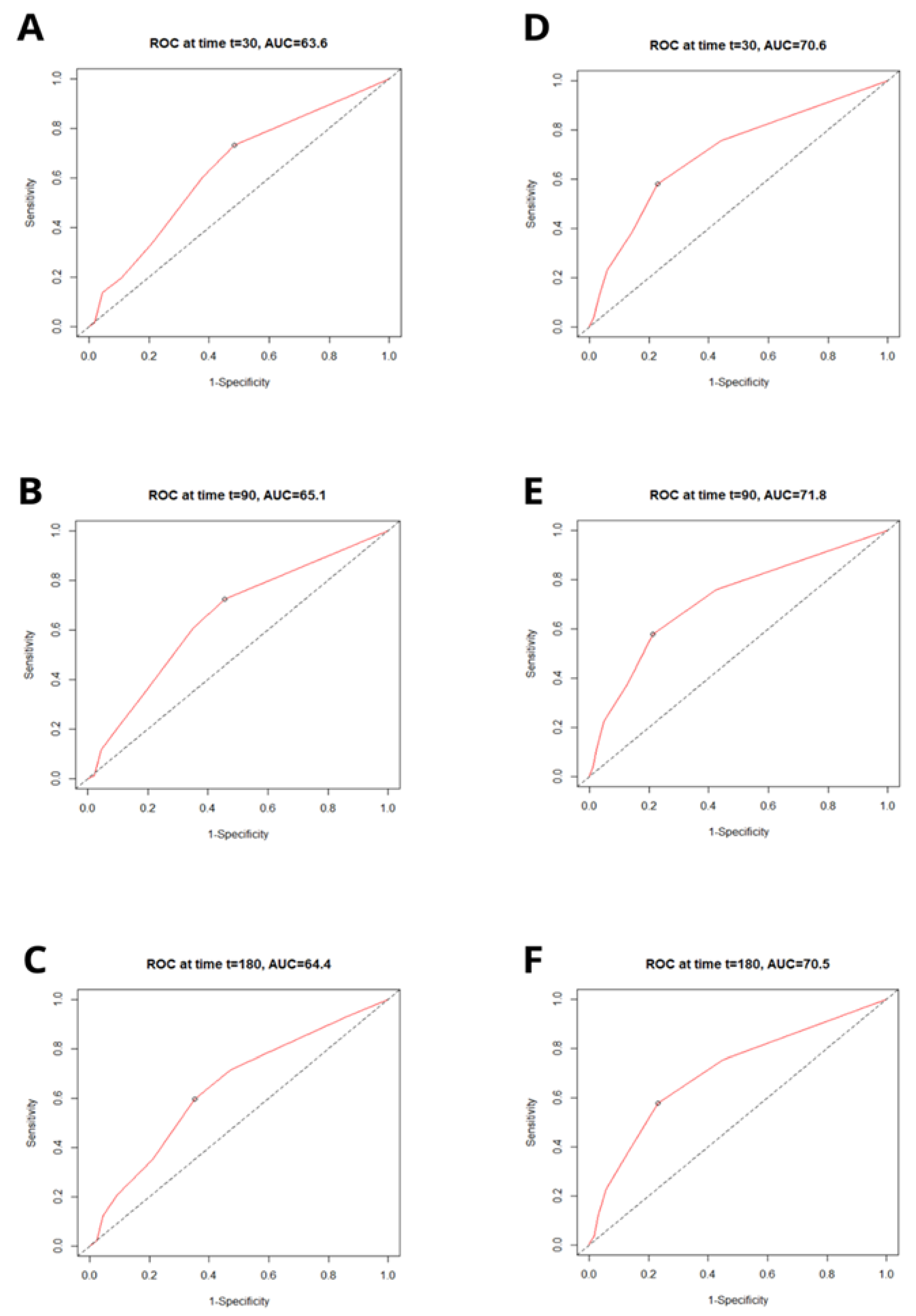
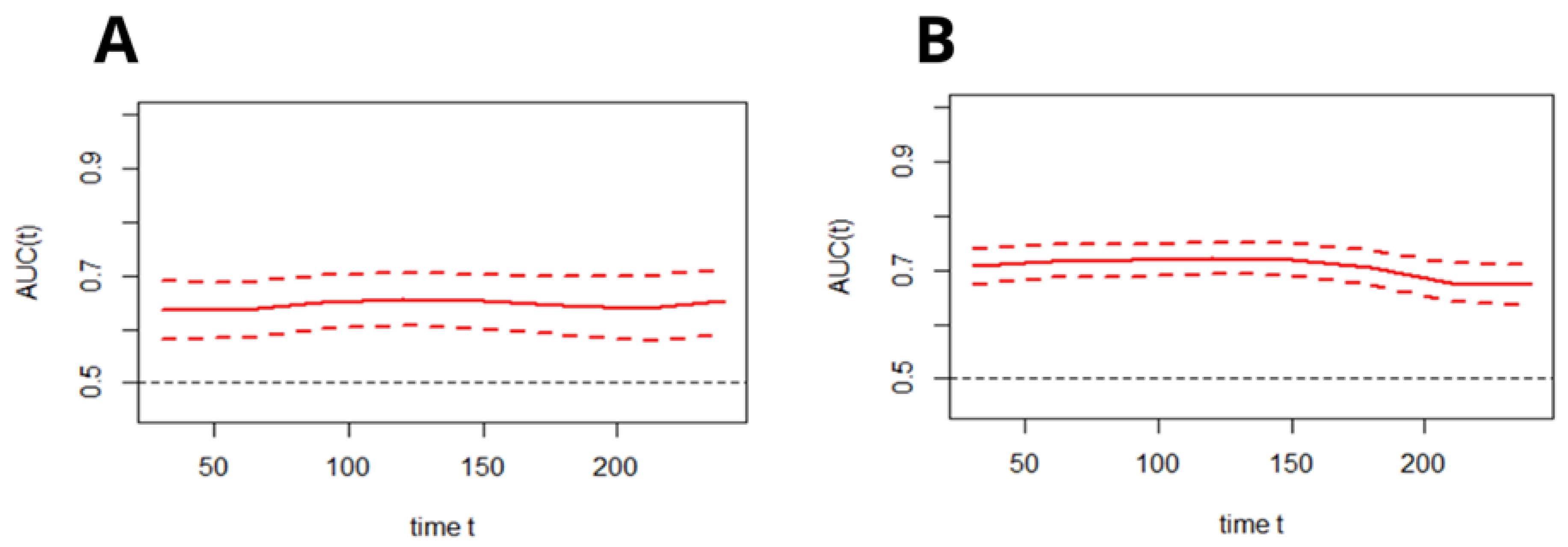
3.3.2. Discriminatory Performance of the C2HEST Score on the Total All-Cause Mortality
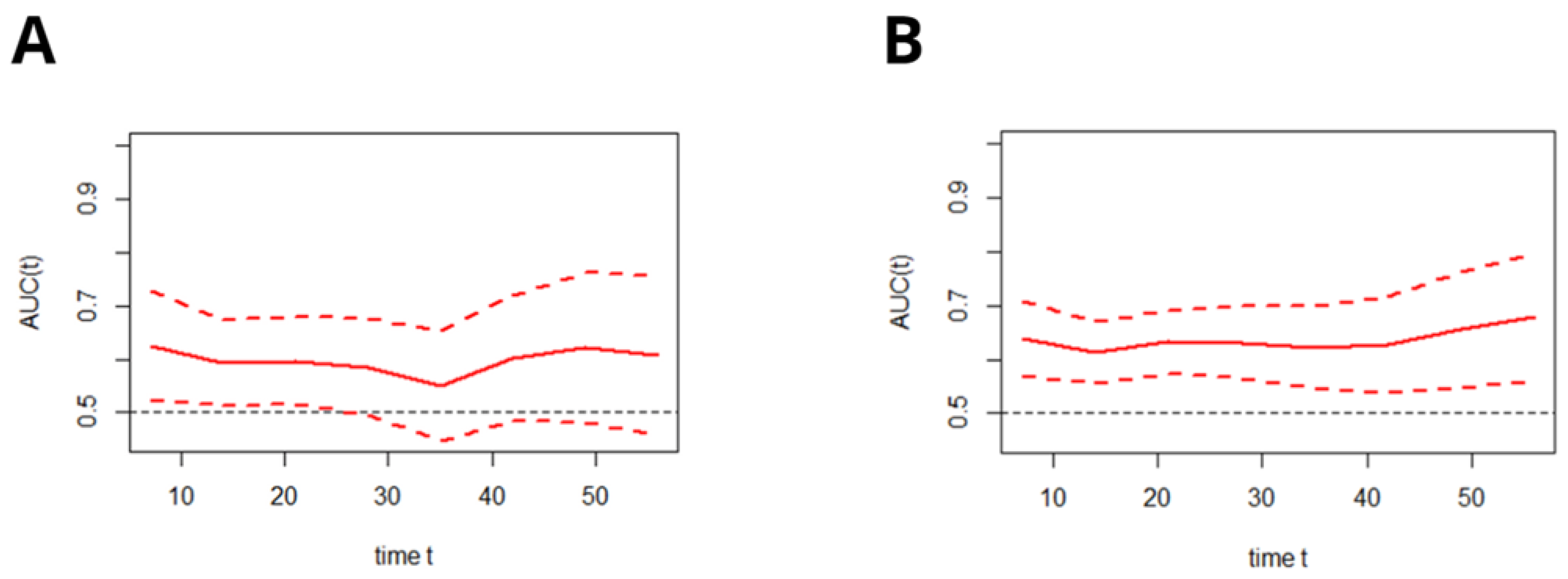
3.3.3. Discriminatory Performance of the C2HEST Score on the In-Hospital All-Cause Mortality–Time–ROC Analysis
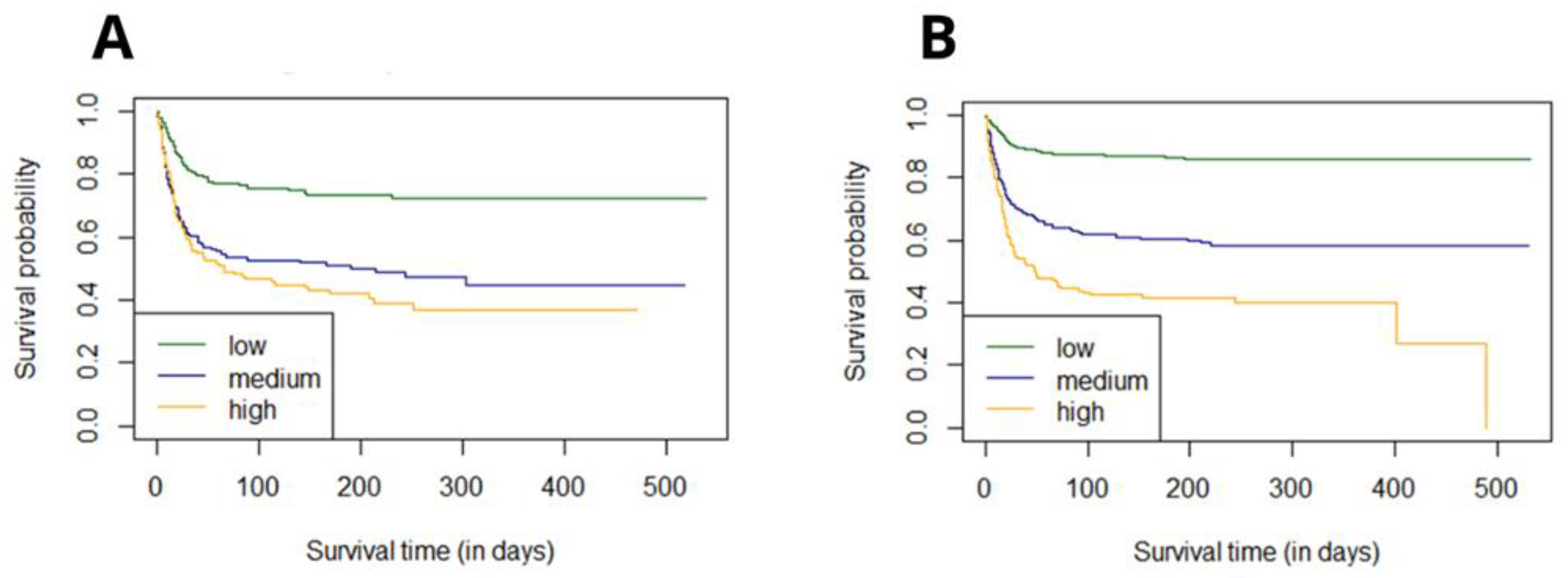
3.3.4. The Survival Probability for Hospitalized COVID-19 Patients
3.3.5. Risk Strata Matching Analysis
- 0–1—low;
- 2–5—medium;
- 6–8—high.
3.3.6. Effect of the C2HEST Risk Stratification Result on COVID-19 Survival
3.4. Associations of the C2HEST Score with Other, Non-Fatal Outcomes
3.5. Sensitivity Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tang, X.; Du, R.H.; Wang, R.; Cao, T.Z.; Guan, L.L.; Yang, C.Q.; Zhu, Q.; Hu, M.; Li, X.Y.; Li, Y.; et al. Comparison of Hospitalized Patients with ARDS Caused by COVID-19 and H1N1. Chest 2020, 158, 195–205. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Janus, A.; Szahidewicz-Krupska, E.; Mazur, G.; Doroszko, A. Insulin Resistance and Endothelial Dysfunction Constitute a Common Therapeutic Target in Cardiometabolic Disorders. Mediat. Inflamm. 2016, 2016, 3634948. [Google Scholar] [CrossRef] [Green Version]
- Hussain, A.; Bhowmik, B.; do Vale Moreira, N.C. COVID-19 and diabetes: Knowledge in progress. Diabetes Res. Clin. Pract. 2020, 162, 108142. [Google Scholar] [CrossRef] [PubMed]
- Whyte, M.B.; Vas, P.; Heiss, C.; Feher, M.D. The contribution of diabetic micro-angiopathy to adverse outcomes in COVID-19. Diabetes Res. Clin. Pract. 2020, 164, 108217. [Google Scholar] [CrossRef]
- Katsiki, N.; Gómez-Huelgas, R.; Mikhailidis, D.P.; Pérez-Martínez, P. Narrative review on clinical considerations for patients with diabetes and COVID-19: More questions than answers. Int. J. Clin. Pract. 2021, 75, e14833. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and validation of a clinical risk score to predict the occurrence of critical illness in hospitalized patients with COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Therneau, T. A Package for Survival Analysis in R; R Package Version 3.2-7. Mayo Foundation for Medical Education and Research. 2020. Available online: https://CRAN.R-project.org/package=survival (accessed on 31 October 2021).
- Hothorn, T.; Hornik, K.; Van De Wiel, M.A.; Zeileis, A. A lego system for conditional inference. Am. Stat. 2006, 60, 257–263. [Google Scholar] [CrossRef] [Green Version]
- Muenchow, J.; Schratz, P.; Brenning, A. QGIS: Integrating R with QGIS for statistical geocomputing. R J. (Scopus) 2017, 9, 409–428. [Google Scholar] [CrossRef]
- Seiglie, J.; Platt, J.; Cromer, S.J.; Bunda, B.; Foulkes, A.S.; Bassett, I.V. Diabetes as a Risk Factor for Poor Early Outcomes in Patients Hospitalized With COVID-19. Diabetes Care 2020, 43, 2938–2944. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Abdi, A.; Jalilian, M.; Ahmadi, P.; Vlaisavljevic, Z. Diabetes and COVID-19: A systematic review on the current evidences. Diabetes Res. Clin. Pract. 2020, 166, 108347. [Google Scholar] [CrossRef]
- Huang, I.; Lim, M.A.; Pranata, R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia—a systematic review, meta-analysis, and meta-regression: Diabetes and COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 395–403. [Google Scholar] [CrossRef]
- Volpe, C.M.O.; Villar-Delfino, P.H.; Dos Anjos, P.M.F.; Nogueira-Machado, J.A. Cellular death, reactive oxygen species (ROS) and diabetic complications. Cell Death Dis. 2018, 9, 119. [Google Scholar] [CrossRef]
- Hu, R.; Xia, C.-Q.; Butfiloski, E.; Clare-Salzler, M. Effect of high glucose on cytokine production by human peripheral blood immune cells and type I interferon signaling in monocytes: Implications for the role of hyperglycemia in the diabetes inflammatory process and host defense against infection. Clin. Immunol. 2018, 195, 139–148. [Google Scholar] [CrossRef]
- Guo, J.; Lin, W.W.; Zucker, J.E.; Nandakumar, R.; Uhlemann, A.C.; Wang, S.; Shivakoti, R. Inflammation and mortality in COVID-19 hospitalized patients with and without type 2 diabetes. J. Clin. Endocrinol. Metab. 2022, dgac003, online, ahead of print. [Google Scholar] [CrossRef]
- Sarkar, S.; Das, D.; BorsinghWann, S.; Kalita, J.; Manna, P. Is diabetes mellitus a wrongdoer to COVID-19 severity? Diabetes Res. Clin. Pract. 2021, 178, 108936. [Google Scholar] [CrossRef]
- Harbuwono, D.S.; Handayani, D.O.T.L.; Wahyuningsih, E.S.; Supraptowati, N.; Ananda; Kurniawan, F.; Wafa, S.; Kristanti, M.; Pantoro, N.I.; Sinto, R.; et al. Impact of diabetes mellitus on COVID-19 clinical symptoms and mortality: Jakarta’s COVID-19 epidemiological registry. Prim. Care Diabetes 2021, in press. [Google Scholar] [CrossRef]
- Kumar, A.; Arora, A.; Sharma, P.; Anikhindi, S.A.; Bansal, N.; Singla, V.; Khare, S.; Srivastava, A. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 535–545. [Google Scholar] [CrossRef]
- Kulcsar, K.A.; Coleman, C.M.; Beck, S.E.; Frieman, M.B. Comorbid diabetes results in immune dysregulation and enhanced disease severity following MERS-CoV infection. JCI Insight 2019, 4, e131774. [Google Scholar] [CrossRef] [Green Version]
- Alraddadi, B.M.; Watson, J.T.; Almarashi, A.; Abedi, G.R.; Turkistani, A.; Sadran, M.; Housa, A.; AlMazroa, M.A.; Alraihan, N.; Banjar, A.; et al. Risk Factors for Primary Middle East Respiratory Syndrome Coronavirus Illness in Humans, Saudi Arabia, 2014. Emerg. Infect. Dis. 2016, 22, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Daryabor, G.; Atashzar, M.R.; Kabelitz, D.; Meri, S.; Kalantar, K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front. Immunol. 2020, 11, 1582. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.P.; Sridhar, R.; Nair, D.; Banurekha, V.V.; Nutman, T.B.; Babu, S. Type 2 diabetes mellitus is associated with altered CD8+ T and natural killer cell function in pulmonary tuberculosis. Immunology 2015, 144, 677–686. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.A.; Mantzoros, C.; Sowers, J.R. Commentary: COVID-19 in patients with diabetes. Metabolism 2020, 107, 154217. [Google Scholar] [CrossRef]
- Marcolino, M.S.; Pires, M.C.; Ramos, L.E.F.; Silva, R.T.; Oliveira, L.M.; Carvalho, R.L.; Mourato, R.L.S.; Sánchez-Montalvá, A.; Raventós, B.; Anschau, F.; et al. ABC2-SPH risk score for in-hospital mortality in COVID-19 patients: Development, external validation and comparison with other available scores. Int. J. Infect. Dis. 2021, 110, 281–308. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables, Units | Low Risk (0–1) | Medium (2–3) | High Risk (>4) | ANOVA p Value | p Value for Post Hoc Analysis in Significant ANOVA L–M a L–H b M–H c | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Demographics | Diabetes N = 209 | Non-Diabetes N = 1183 | Diabetes N = 146 | Non-Diabetes N = 337 | Diabetes N = 118 | Non-Diabetes N = 146 | Diabetes | Non-Diabetes | Diabetes | Non- Diabetes |
| Age, years mean ± SD min–max N= | 61.7 ± 11.7 17–74 209 | 49.4 ± 15.8 17–74 1183 | 75.3 ± 9.7 41–97 146 | 76.0 ± 12.5 29–100 337 | 76.9 ± 10.3 38–93 118 | 80.4 ± 8.2 50–100 146 | <0.0001 | <0.0001 | <0.0001 a <0.0001 b 0.409 c | <0.0001 a <0.0001 b 0.000016 c |
| Age ≥ 65 years n, n (%) | 106, (50.7) | 268, (22.7) | 130, (89.0) | 284, (84.3) | 103, (87.3) | 141, (96.6) | <0.0001 | <0.0001 | <0.0001 a <0.0001 b 1.0 c | <0.0001 a <0.0001 b 0.00074c |
| Male sex n, n (%) | 129, (61.7) | 597, (50.5) | 69, (47.3) | 134, (39.8) | 62, (52.5) | 71, (48.6) | 0.022 | 0.0024 | 0.0287a 0.4003 b 1.0 c | 0.002 a 1 b 0.2615 c |
| BMI. kg/m2 mean ± SD min–max N= | 29.6 ± 5.7 17.1–42.4 65 | 27.8 ± 4.7 15.4–49.4 321 | 29.7 ± 3.8 23.0–36.7 27 | 28.9 ± 6.3 18.6–47.8 60 | 29.8 ± 6.3 19.6 -48.2 33 | 25.6 ± 4.6 16.4–34.9 32 | 0.9886 | 0.016 | N/A | 0.445 a 0.034 b 0.015 c |
| Normal body weight (BMI = 18.5–24.9 kg/m2) n, n (%) N= | 14, (21.5) 65 | 85, (26.5) 321 | 5, (18.5) 27 | 14, (23.3) 60 | 8, (24.2) 33 | 14, (43.8) 32 | 0.9961 | 0.0332 | N/A | 1 a 0.0304 b 0.0496 c |
| Underweight (BMI < 18.5 kg/m2) n, n (%) N= | 1, (1.5) 65 | 2, (0.6) 321 | 0, (0.0) 27 | 0, (0.0) 60 | 0, (0.0) 33 | 2, (6.3) 32 | ||||
| Overweight (BMI = 25–29.9 kg/m2) n, n (%) N= | 19, (29.2) 65 | 140, (43.6) 321 | 9, (33.3) 27 | 24, (40.0) 60 | 10, (30.3) 33 | 11, (34.4) 32 | ||||
| Obesity (BMI ≥ 30 kg/m2) n, n (%) N= | 31, (47.7) 65 | 94, (29.3) 321 | 13, (48.1) 27 | 22, (36.7) 60 | 15, (45.5) 33 | 5, (15.6) 32 | ||||
| Cigarette smoking, never/previous/current n, n (%) N= | 194, (92.8%)/6, (2.9%)/9, (4.3) 209 | 1122, (94.8%)/39, (3.3%)/22, (1.9%) 1183 | 131, (90.3%)/8, (5.5%), /6, (4.1%) 145 | 294, (87.8%)/24, (7.2%)/17, (5.1%) 335 | 98, (83.1%) /16, (13.6%) /4, (3.4%) 118 | 116, (80.0%)/17, (11.7%) /12, (8.3%) 145 | 0. 0081 | <0.0001 | 1.0 a 0.0041 b 0.2695 c | 0.0002a <0.0001 b 0.258 c |
| Hypertension, n, n (%) | 145, (69.4) | 264, (22.3) | 129, (88.4) | 219, (65.0) | 108, (91.5) | 131, (89.7) | <0.0001 | <0.0001 | 0.00015 a <0.0001 b 1.0 c | <0.0001 a <0.0001 b <0.0001 c |
| Dyslipidemia, n, n (%) N= | 57, (62.6) 91 | 146, (54.7) 267 | 25, (48.1) 52 | 43, (39.1) 110 | 24, (43.6) 55 | 20, (34.5) 58 | 0.0545 | 0.0019 | N/A | 0.025 a 0.0025b 1.0 c |
| Atrial fibrillation/flutter, n, n (%) | 16, (7.7) | 31, (2.6) | 35, (24) | 68, (20.2) | 54, (45.8) | 77, (52.7) | <0.0001 | <0.0001 | <0.0001 a <0.0001 b 0.00098 c | <0.0001 a <0.0001 b <0.0001 c |
| Previous coronary revascularization, n, n (%) | 2, (1.0) | 4, (0.3) | 14, (9.6) | 21, (6.2) | 55, (46.6) | 50, (34.2) | <0.0001 | <0.0001 | 0.00096 a <0.0001 b <0.0001 c | <0.0001 a < 0.0001b < 0.0001c |
| Previous myocardial infarction n, n (%) | 2, (1.0) | 9, (0.8) | 28, (19.2) | 32, (9.5) | 55, (46.6) | 57, (39.0) | <0.0001 | <0.0001 | <0.0001 a <0.0001 b <0.0001 c | <0.0001 a <0.0001 b <0.0001 c |
| Heart failure, n, n (%) | 0, (0) | 0, (0) | 20, (13.7) | 32, (9.5) | 94, (79.7) | 100, (68.5) | <0.0001 | <0.0001 | <0.0001 a <0.0001 b <0.0001 c | <0.0001 a <0.0001 b <0.0001 c |
| Moderate/severe valvular heart disease or previous valve heart surgery, n, n (%) | 4, (1.9) | 9, (0.8) | 12, (8.2) | 18, (5.3) | 24, (20.3) | 25, (17.1) | <0.0001 | <0.0001 | 0.0316 a <0.0001 b 0.0226 c | <0.0001 a <0.0001 b 0.00025 c |
| Peripheral artery disease, n, n (%) | 13, (6.2) | 12, (1.0) | 12, (8.2) | 17, (5.0) | 25, (21.2) | 15, (10.3) | <0.0001 | <0.0001 | 1 a 0.00032 b 0.01357 c | <0.0001 a <0.0001 b 0.1354 c |
| Previous stroke/TIA, n, n (%) | 12, (5.7) | 31, (2.6) | 26, (17.8) | 33, (9.8) | 25, (21.2) | 31, (21.2) | <0.0001 | <0.0001 | 0.00172 a 0.00015 b 1 c | <0.0001 a <0.0001 b 0.0034 c |
| Chronic kidney disease n, n (%) | 24, (11.5) | 45, (3.8) | 24, (16.4) | 43, (12.8) | 54, (45.8) | 34, (23.3) | <0.0001 | <0.0001 | 0.7072 a <0.0001 b <0.0001 c | <0.0001 a <0.0001 b 0.017 c |
| Hemodialysis n, n (%) | 6, (2.9) | 13, (1.1) | 8, (5.5) | 11, (3.3) | 13, (11.09) | 5, (3.4) | 0.0095 | 0.0065 | 1 a 0.0164 b 0.463 c | 0.0314 a 0.1176 b 1 c |
| Asthma, n, n (%) | 9, (4.3) | 43, (3.6) | 9, (6.2) | 13, (3.9) | 16, (13.6) | 3, (2.1) | 0.8053 | 0.584676 | N/A | N/A |
| COPD n, n (%) | 1, (0.5) | 5, (0.4) | 9, (6.2) | 15, (4.5) | 16, (13.6) | 25, (17.1) | <0.0001 | <0.0001 | 0.0127 a <0.0001 b 0.2023 c | <0.0001 a <0.0001 b <0.0001 c |
| Hypothyroidism n, n (%) | 10, (4.8) | 62, (5.2) | 17, (11.6) | 49, (14.5) | 33, (28.0) | 28, (19.2) | <0.0001 | <0.0001 | 0.0844 a <0.0001 b 0.004 c | <0.0001 a <0.0001 b 0.7586 c |
| Hyperthyroidism n, n (%) | 0, (0) | 4, (0.3) | 1, (0.7) | 9, (2.7) | 0, (0) | 6, (4.1) | 0.5581 | <0.0001 | N/A | 0.0011 a 0.0007 b 1.0 c |
| Variables, Units | Low Risk (0–1) | Medium (2–3) | High Risk (>4) | ANOVA p Value | p Value for Post Hoc Analysis in Significant ANOVA L–M a L–H b M–H c | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient-Reported Symptoms | Diabetes N = 209 | Non- Diabetes N = 1183 | Diabetes N= 146 | Non- Diabetes N = 337 | Diabetes N = 118 | Non- Diabetes N = 146 | Diabetes | Non- Diabetes | Diabetes | Non- Diabetes |
| Cough, n, n (%) | 52, (24.9) | 392, (33.1) | 34, (23.3) | 89, (26.4) | 25, (21.2) | 38, (26) | 0.749 | 0.0236 | N/A | N/A |
| Dyspnea, n, n (%) | 84, (40.2) | 475, (40.2) | 62, (42.5) | 140, (41.5) | 62, (52.5) | 79, (54.1) | 0.088 | 0.00546 | N/A | 1 a 0.0051 b 0.0431 c |
| Chest pain n, n (%) | 11, (5.3) | 88, (7.4) | 8, (5.5) | 25, (7.4) | 17, (14.4) | 8, (5.5) | 0.006 | 0.68528 | N/A | N/A |
| Hemoptysis n, n (%) | 3, (1.4) | 6, (0.5) | 0, (0) | 2, (0.6) | 2, (1.69) | 2, (1.4) | 0.271 | 0.3467 | N/A | N/A |
| Smell dysfunction n, n (%) | 2, (1) | 57, (4.8) | 2, (1.4) | 8, (2.4) | 3, (2.5) | 2, (1.4) | 0.552 | 0.03057 | N/A | 0.2137 a 0.2698 b 1 c |
| Taste dysfunction n, n (%) | 3, (1.4) | 45, (3.8) | 3, (2.1) | 7, (2.1) | 4, (3.4) | 3, (2.1) | 0.467 | 0.2337 | N/A | N/A |
| Abdominal pain n, n (%) | 21, (10.1) | 83, (7.0) | 7, (4.8) | 19, (5.6) | 5, (4.2) | 12, (8.2) | 0.065 | 0.53339 | N/A | N/A |
| Diarrhea n, n (%) | 14, (6.7) | 61, (5.2) | 9, (6.2) | 24, (7.1) | 4, (3.4) | 15, (10.3) | 0.446 | 0.03065 | N/A | N/A |
| Nausea/vomiting n, n (%) | 8, (3.8) | 48, (4.1) | 11, (7.5) | 16, (4.7) | 5, (4.2) | 9, (6.2) | 0.262 | 0.4694 | N/A | N/A |
| Body temperature, °C mean ± SD min–max N= | 36.9 ± 0.82 34.4–39.5 110 | 37.1 ± 0.89 35.0–40.5 678 | 37 ± 1 35–40 75 | 36.9 ± 0.87 35.5–40.0 154 | 36.8 ± 0.7 35.2–39.3 63 | 37.0 ± 0.97 35.9–40.0 71 | 0.471 | 0.07369 | N/A | N/A |
| Heart rate, beats/minute mean ± SD min–max N= | 87.1 ± 17.2 48–150 160 | 86.3 ± 15.41 48–160 863 | 85.5 ± 16.2 50–150 122 | 83.5 ± 16.7 50–160 257 | 84.6 ± 17.5 47–140 109 | 84.7 ± 18.97 36–150 121 | 0.49 | 0.0486 | N/A | 0.045a 0.626 b 0.84 c |
| Respiratory rate, breaths/minute mean ± SD min–max N= | 21.1 ± 9.1 12–50 35 | 17.8 ± 4.65 12–40 167 | 18 ± 4 12–28 20 | 18.9 ± 6.05 12–45 44 | 19.9 ± 7.8 12–50 24 | 18.9 ± 3.66 12–25 19 | 0.196 | 0.3055 | N/A | N/A |
| Systolic blood pressure, mmHg mean ± SD min–max N= | 132.9 ± 21.6 60–204 160 | 130.2 ± 21.22 60–240 855 | 134.3 ± 38.8 50–270 121 | 134.1 ± 23.39 60–210 256 | 137.5 ± 23.4 86–210 111 | 132.6 ± 26.11 70–205 123 | 0.253 | 0.05307 | N/A | N/A |
| Diastolic blood pressure, mmHg mean ± SD min–max N= | 78.8 ± 13.6 40–125 159 | 78.5 ± 12.5 40–150 853 | 79.2 ± 14.3 50–150 117 | 77.6 ± 13.1 45–157 255 | 76 ± 14.8 44–143 111 | 76.0 ± 15.66 40–120 123 | 0.190 | 0.19414 | N/A | N/A |
| Pulse pressure mean ± SD min–max N= | 54.6 ± 16 15–110 159 | 51.9 ± 15.28 11–136 853 | 57.5 ± 18.6 20–120 117 | 56.9 ± 18.16 20–120 254 | 61.6 ± 18 30–130 111 | 56.6 ± 19.47 20–120 123 | 0.0049 | <0.0001 | 0.36 a 0.003 b 0.212 c | 0.0002 a 0.03b 0.987 c |
| SpO2 on room air, % (FiO2 = 21%) mean ± SD min–max N= | 91.8 ± 6.8 56–100 106 | 92.9 ± 7.2 48–100 690 | 88.8 ± 10.2 50–100 89 | 90.0 ± 9.45 50–99 187 | 91.5 ± 7.8 60–99 66 | 88.8 ± 9.13 50–99 92 | 0.059 | <0.0001 | N/A | 0.0005a 0.0003b 0.559 c |
| SpO2 < 90%, n, n (%) | 29, (27.4) | 153, (22.2) | 37, (41.6) | 63, (33.7) | 19, (28.8) | 36, (39.1) | 0.081 | <0.0001 | N/A | 0.00496a 0.0018b 1 c |
| GCS, points mean ± SD min–max N= | 14.7 ± 1.3 6–15 77 | 14.6 ± 1.88 3–15 484 | 14.2 ± 2 3–15 56 | 14.6 ± 1.52 3–15 130 | 14.2 ± 2.6 3–15 48 | 14.0 ± 2.38 3–15 66 | 0.202 | 0.15588 | N/A | N/A |
| Cracles n, n (%) | 33, (15.8) | 119, (10.1) | 38, (26) | 61, (18.1) | 33, (28) | 32, (21.9) | 0.014 | <0.0001 | N/A | 0.00025 a 0.0001 b 1 c |
| Wheezing n, n (%) | 15, (7.2) | 79, (6.7) | 20, (13.7) | 35, (10.4) | 32, (27.1) | 35, (24.0) | <0.0001 | <0.0001 | 0.1941 a <0.0001 b 0.0305 c | 0.0917 a <0.0001 b 0.00052 c |
| Pulmonary congestion n, n (%) | 37, (17.7) | 145, (12.3) | 39, (26.7) | 62, (18.4) | 39, (33.1) | 36, (24.7) | 0.006 | <0.0001 | N/A | 0.0149 a 0.0002 b 0.443 c |
| Peripheral edema n, n (%) | 14, (6.7) | 61, (5.2) | 24, (16.4) | 35, (10.4) | 29, (24.6) | 23, (15.8) | <0.0001 | <0.0001 | 0.0181 a <0.0001 b 0.4113 c | 0.0024 a <0.0001 b 0.3899 c |
| Hemiplegia/hemiparesis n, n (%) | 6, (2.9) | 23, (1.9) | 10, (6.9) | 13, (3.9) | 6, (5.1) | 12, (8.2) | 0.209 | 0.0002 | N/A | 0.1931 a 0.0005 b 0.2122 c |
| VES-13, points mean ± SD min–max N= | 5 ± 3.4 1–9 8 | 3.8 ± 2.63 1–9 20 | 6.28 ± 3.6 1–12 18 | 5.1 ± 3.03 1–10 19 | 6.2 ± 2.66 3–10 10 | 6.5 ± 3.2 3–13 14 | 0.671 | 0.045 | N/A | 0.363 a 0.038 b 0.394 c |
| Variables | Low Risk (0–1) | Medium (2–3) | High Risk (>4) | ANOVA p Value | p Value for Post Hoc Analysis in Significant ANOVA L–M a L–H b M–H c | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Diabetes N = 209 | Non- Diabetes N = 1183 | Diabetes N= 146 | Non- Diabetes N = 337 | Diabetes N = 118 | Non- Diabetes N = 146 | Diabetes | Non- Diabetes | Diabetes | Non- Diabetes | |
| Applied treatment and procedures | ||||||||||
| The most advanced respiratory support applied during the hospitalization | 0.0712 | <0.0001 | N/A | 0.0229a <0.0001b 0.0066c | ||||||
| no oxygen | ||||||||||
| n, n (%) | 79, (37.8) | 648, (54.9) | 45, (30.8) | 153, (45.4) | 37, (31.4) | 47, (32.2) | ||||
| low flow oxygen support | ||||||||||
| n, n (%) | 79, (37.8) | 365, (30.9) | 61, (41.8) | 125, (37.1) | 49, (41.5) | 72, (49.3) | ||||
| high flow nasal cannula | ||||||||||
| non-invasive ventilation | ||||||||||
| n, n (%) | 15, (3.2) | 67, (5.7) | 20, (4.2) | 32, (9.5) | 18, (3.8) | 20, (13.7) | ||||
| invasive ventilation | ||||||||||
| n, n (%) | 36, (17.2) | 101, (8.6) | 20, (13.7) | 27, (8.0) | 14, (11.9) | 7, (4.8) | ||||
| Oxygenation parameters from the period of qualification for advanced respiratory support: SpO2, % mean ± SD (min–max) N= | 88.4 ± 8.5 (60–98) 54 | 90.9 ± 7.8 (50–100) 345 | 86.6 ± 10.8 (57–99) 47 | 86.9 ± 9.0 (55–99) 82 | 87.6 ± 8.0 (60–98) 42 | 83.6 ± 11.4 (59–99) 44 | 0.6374 | <0.0001 | N/A | 0.0009a 0.0004b 0.224 c |
| Therapy with catecholamines, n, n (%) | 33, (15.8) | 95, (8.0) | 15, (10.3) | 28, (8.3) | 22, (18.6) | 19, (13.0) | 0.1411 | 0.124667 | N/A | N/A |
| Coronary revascularization or/and an indication for coronary revascularization, n, n (%) | 4, (1.9) | 4, (0.3) | 4, (2.7) | 6, (1.8) | 5, (4.2) | 2, (1.4) | 0.4235 | 0.0092 | N/A | 0.0317a 0.4015 b 1 c |
| Hemodialysis, n, n (%) | 15, (7.2) | 31, (2.6) | 7, (4.8) | 5, (1.5) | 8, (6.8) | 3, (2.1) | 0.6466 | 0.5311 | N/A | N/A |
| Variables | Low Risk (0–1) | Medium (2–3) | High Risk (>4) | ANOVA p Value | p Value for Post Hoc Analysis in Significant ANOVA L–M a L–H b M–H c | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Diabetes N = 209 | Non-Diabetes N = 1183 | Diabetes N= 146 | Non-Diabetes N = 337 | Diabetes N = 118 | Non-Diabetes N = 146 | Diabetes | Non-Diabetes | Diabetes | Non- Diabetes | |
| All-cause mortality rate | ||||||||||
| In-hospital mortality, n, n (%) | 32, (15.3) | 85, (7.2) | 42, (28.8) | 65, (19.3) | 41, (34.7) | 54, (37.0) | 0.00014 | <0.0001 | 0.0099 0.0003 1.0 c | <0.0001 a <0.0001 b 0.00017c |
| 3-month mortality, n, n (%) N= | 51, (24.4) 201 | 150, (12.7) 1116 | 69, (47.3) 143 | 125, (37.1) 323 | 63, (53.4) 117 | 81, (55.5) 143 | <0.0001 | <0.0001 | <0.0001 a <0.0001 b 1.0 c | <0.0001 a <0.0001 b 0.0008 c |
| 6-month mortality, n, n (%) N= | 55, (37.2) 118 | 158, (22.3) 447 | 71, (60.7) 109 | 133, (51.4) 214 | 68, (64.8) 91 | 85, (68.0) 116 | <0.0001 | <0.0001 | 0.0007a <0.0001 b 0.5682 c | <0.0001 a <0.0001 b 0.0088 c |
| Hospitalization | ||||||||||
| Duration of hospitalization, days (distribution to be verified) mean ± SD (min–max) | 16.5 ± 17.7 (1–126) | 1.5 ± 12.4 (1–131) | 14.4 ± 14.6 (1–72) | 12.8 ± 13.3 (1–124) | 17.8 ± 18.2 (1–121) | 15.3 ± 14.0 (1–82) | 0.2293 | <0.0001 | 0.011a 0.0004b 0.181 c | |
| End of hospitalization | 0.0003 | <0.0001 | 0.0063 a 0.0004 b 1.0 c | <0.0001 a <0.0001 b 0.0019c | ||||||
| death | ||||||||||
| n, n (%) | 32, (15.3) | 85, (7.2) | 42, (28.8) | 65, (19.3) | 41, (34.7) | 54, (37) | ||||
| discharge to home—full recovery | ||||||||||
| n, n (%) | 120, (57.4) | 851, (71.9) | 56, (38.4) | 164, (48.7) | 43, (36.4) | 56, (38.4) | ||||
| transfer to another hospital—worsening) | ||||||||||
| n, n (%) | 28, (13.4) | 111, (9.4) | 24, (16.4) | 70, (20.8) | 20, (16.9) | 23, (15.8) | ||||
| transfer to another hospital—in recovery | ||||||||||
| n, n (%) | 29, (13.9) | 136, (11.5) | 24, (16.4) | 38, (11.3) | 14, (11.9) | 13, (8.9) | ||||
| Diabetics | Non-Diabetics | |||||
|---|---|---|---|---|---|---|
| Total Deaths | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Overall | 1.25 | 1.163–1.341 | <0.0001 | 1.45 | 1.382–1.525 | <0.0001 |
| Risk strata | ||||||
| Medium- vs. low-risk | 2.34 | 1.658–3.315 | <0.0001 | 3.51 | 2.795–4.414 | <0.0001 |
| High- vs. low-risk | 2.84 | 1.999–4.0329 | <0.0001 | 6.0 | 4.628–7.794 | <0.0001 |
| Diabetics | Non-Diabetics | |||||
|---|---|---|---|---|---|---|
| Total Deaths | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Overall | 1.19 | 1.081–1.314 | <0.0005 | 1.294 | 1.207–1.387 | <0.0001 |
| Risk strata | ||||||
| Medium- vs. low-risk | 2.16 | 1.363–3.437 | 0.00106 | 2.135 | - | - |
| High- vs. low-risk | 2.11 | 1.329–3.356 | 0.00155 | 3.345 | - | - |
| Variables | Low Risk (0–1) | Medium (2–3) | High Risk (>4) | ANOVA p Value | p Value for Post Hoc Analysis in Significant ANOVA L–M a L–H b M–H c | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Diabetes N = 209 | Non-Diabetes N = 1183 | Diabetes N= 146 | Non-Diabetes N = 337 | Diabetes N = 118 | Non-Diabetes N = 146 | Diabetes | Non- Diabetes | Diabetes | Non- Diabetes | |
| Aborted cardiac arrest, n, n (%) | 2, (1.0) | 13, (1.1) | 0, (0.0) | 3, (0.9) | 4, (3.4) | 2, (1.4) | 0.0573 | 0.8520 | N/A | N/A |
| Shock, n, n (%) | 29, (13.9) | 76, (6.4) | 14, (9.6) | 29, (8.6) | 16, (13.6) | 16, (11.0) | 0.4457 | 0.0782 | N/A | N/A |
| Hypovolemic shock, n, n (%) | 5, (2.4) | 17, (1.4) | 3, (2.1) | 4, (1.2) | 1, (0.8) | 5, (3.4) | 0.6946 | 0.1623 | N/A | N/A |
| Cardiogenic shock, n, n (%) | 2, (1.0) | 5, (0.4) | 4, (2.7) | 7, (2.1) | 8, (6.8) | 6, (4.1) | 0.0132 | 0.00011 | 0.7008 a 0.01599 b 0.4287 c | 0.0208a 0.0014b 0.6787 c |
| Septic shock, n, n (%) | 27, (12.9) | 58, (4.9) | 10, (6.8) | 18, (5.3) | 12, (10.2) | 9, (6.2) | 0.1812 | 0.7878 | N/A | N/A |
| Venous thromboembolic disease, n, n (%) | 13, (6.2), | 68, (5.7) | 9, (6.2) | 21, (6.2) | 3, (2.5) | 12, (8.2) | 0.3067 | 0.493 | N/A | N/A |
| Pulmonary embolism, n, n (%) | 4, (1.9) | 28, (2.4) | 2, (1.4) | 7, (2.1) | 3, (2.5) | 4, (2.7) | 0.98 | 0.7257 | N/A | N/A |
| Myocardial infarction, n, n (%) | 4, (1.9) | 4, (0.3) | 4, (2.7) | 6, (1.8) | 4, (3.4) | 3, (2.1) | 0.657 | 0.0049 | N/A | 0.0317a 0.0978 b 1 c |
| Myocardial injury, 3x, n, n (%) N | 31, (24.6) N = 126 | 78, (14.4) N = 542 | 35, (39.3) N = 89 | 60, (28.7) N = 209 | 36, (41.4) N = 87 | 46, (48.4) N = 95 | 0.0165 | <0.0001 | 0.0934 a 0.0438 b 1.0 c | <0.0001 a <0.0001 b 0.0039c |
| Acute heart failure, n, n (%) | 2(1.0) | 6, (0.5) | 9, (6.2) | 13, (3.9) | 23, (19.5) | 23, (15.8) | <0.0001 | <0.0001 | 0.04a <0.0001b 0.0056c | <0.0001 a <0.0001 b <0.0001c |
| Stroke/TIA, n, n (%) | 4, (1.9) | 13, (1.1) | 8, (5.5) | 10, (30.0) | 2, (1.7) | 3, (2.1) | 0.1361 | 0.0347 | N/A | 0.062 a 1.0 b 1.0 c |
| Pneumonia, n, n (%) | 127, (60.8) | 545, (46.1) | 90, (61.6) | 210, (62.3) | 77, (65.3) | 102, (69.9) | 0.7155 | <0.0001 | N/A | <0.0001a <0.0001b 0.409 c |
| Complete respiratory failure, n, n (%) N | 17, (45.9) N = 37 | 39, (47.0) N = 83 | 20, (62.5) N = 32 | 26, (46.4) N = 56 | 21, (70) N = 30 | 22, (62.9) N = 35 | 0.1195 | 0.2344 | N/A | N/A |
| SIRS, n, n (%) N | 23, (11.2) N = 206 | 116, (10.3) N = 1121 | 17, (11.6) N = 146 | 25, (97.5) N = 334 | 17, (14.4) N = 118 | 19, (13.1) N = 145 | 0.675 | 0.132 | N/A | N/A |
| Sepsis, n, n (%) N | 2, (2.6) N = 77 | 7, (1.4) N = 484 | 4, (7.3) N = 55 | 2, (1.6) N = 122 | 2, (3.6) N = 55 | 5, (7.8) N = 64 | 0.4404 | 0.0109 | N/A | N/A |
| Acute kidney injury, n, n (%) | 28, (13.4) | 81, (6.8) | 27, (18.5) | 39, (11.6) | 31, (26.3) | 25, (17.1) | 0.0149 | <0.0001 | 0.7422 a 0.0175 b 0.5139 c | 0.0194 a <0.0001b 0.396 c |
| Acute liver dysfunction, n, n (%) N | 6, (3.0) N = 198 | 24, (2.3) N = 1034 | 5, (3.7) N = 136 | 17, (5.3) N = 320 | 7, (6.4) N = 109 | 7, (5.2) N = 134 | 0.3388 | 0.001 | N/A | 0.0408 a 0.2311 b 1 c |
| Multiple organ dysfunction syndrome, n, n (%) | 2, (1.0) | 19, (1.6) | 3, (2.1) | 5, (1.5) | 5, (4.2) | 3, (2.1) | 0.1421 | 0.8547 | N/A | N/A |
| Lactic acidosis (on admission), n, n (%) N | 3, (9.7) N = 31 | 6, (8.2) N = 73 | 2, (7.1) N = 28 | 3, (5.9) N = 51 | 6, (22.2) N = 27 | 2, (6.3) N = 32 | 0.2581 | 0.9199 | N/A | N/A |
| Hyperlactatemia (on admission) n, n (%) N | 20, (64.5) N = 31 | 58, (79.5) N = 73 | 17, (60.7) N = 28 | 35, (68.6) N = 51 | 16, (59.3) N = 27 | 21, (65.2) N = 32 | 0.9124 | 0.2317 | N/A | N/A |
| Bleeding, n (%) n, n (%) | 15, (7.2) | 48, (4.1) | 9, (6.2) | 16, (4.7) | 11, (9.3) | 14, (9.6) | 0.6137 | 0.0116 | N/A | 1 a 0.0162 b 0.2066 c |
| Intracranial bleeding, n, n (%) | 3, (1.4) | 9, (0.8) | 3, (2.1) | 5, (1.5) | 0, (0.0) | 1, (0.7) | 0.3846 | 0.3794 | N/A | N/A |
| Respiratory tract bleeding, n, n (%) | 6, (2.9) | 17, (1.4) | 3, (2.1) | 1, (0.3) | 4, (3.4) | 3, (2.1) | 0.774 | 0.1106 | N/A | N/A |
| Gastrointestinal bleeding, n, n (%) | 7, (3.3) | 13, (1.1) | 2, (1.4) | 7, (2.1) | 5, (4.2) | 7, (4.8) | 0.4699 | 0.0031 | N/A | 0.4279 a 0.0047 b 0.3529 c |
| Urinary tract bleeding, n, n (%) | 3, (1.4) | 6, (0.5) | 2, (1.4) | 2, (0.6) | 2, (1.7) | 3, (2.1) | 1.0 | 0.0955 | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajecki, D.; Doroszko, A.; Trocha, M.; Giniewicz, K.; Kujawa, K.; Skarupski, M.; Gawryś, J.; Matys, T.; Szahidewicz-Krupska, E.; Rola, P.; et al. Usefulness of the C2HEST Score in Predicting the Clinical Outcomes of COVID-19 in Diabetic and Non-Diabetic Cohorts. J. Clin. Med. 2022, 11, 873. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030873
Gajecki D, Doroszko A, Trocha M, Giniewicz K, Kujawa K, Skarupski M, Gawryś J, Matys T, Szahidewicz-Krupska E, Rola P, et al. Usefulness of the C2HEST Score in Predicting the Clinical Outcomes of COVID-19 in Diabetic and Non-Diabetic Cohorts. Journal of Clinical Medicine. 2022; 11(3):873. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030873
Chicago/Turabian StyleGajecki, Damian, Adrian Doroszko, Małgorzata Trocha, Katarzyna Giniewicz, Krzysztof Kujawa, Marek Skarupski, Jakub Gawryś, Tomasz Matys, Ewa Szahidewicz-Krupska, Piotr Rola, and et al. 2022. "Usefulness of the C2HEST Score in Predicting the Clinical Outcomes of COVID-19 in Diabetic and Non-Diabetic Cohorts" Journal of Clinical Medicine 11, no. 3: 873. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030873