
Self-Reported Pain and Emotional Reactivity in Bipolar Disorder: A Prospective FACE-BD Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessments
2.2.1. Pain
2.2.2. Affective States
2.2.3. Personality Traits
2.3. Ethical Concerns
2.4. Statistical Analysis
2.4.1. Transversal Analysis
2.4.2. Longitudinal Analysis
3. Results
3.1. Sample Description
3.2. Transversal Analysis
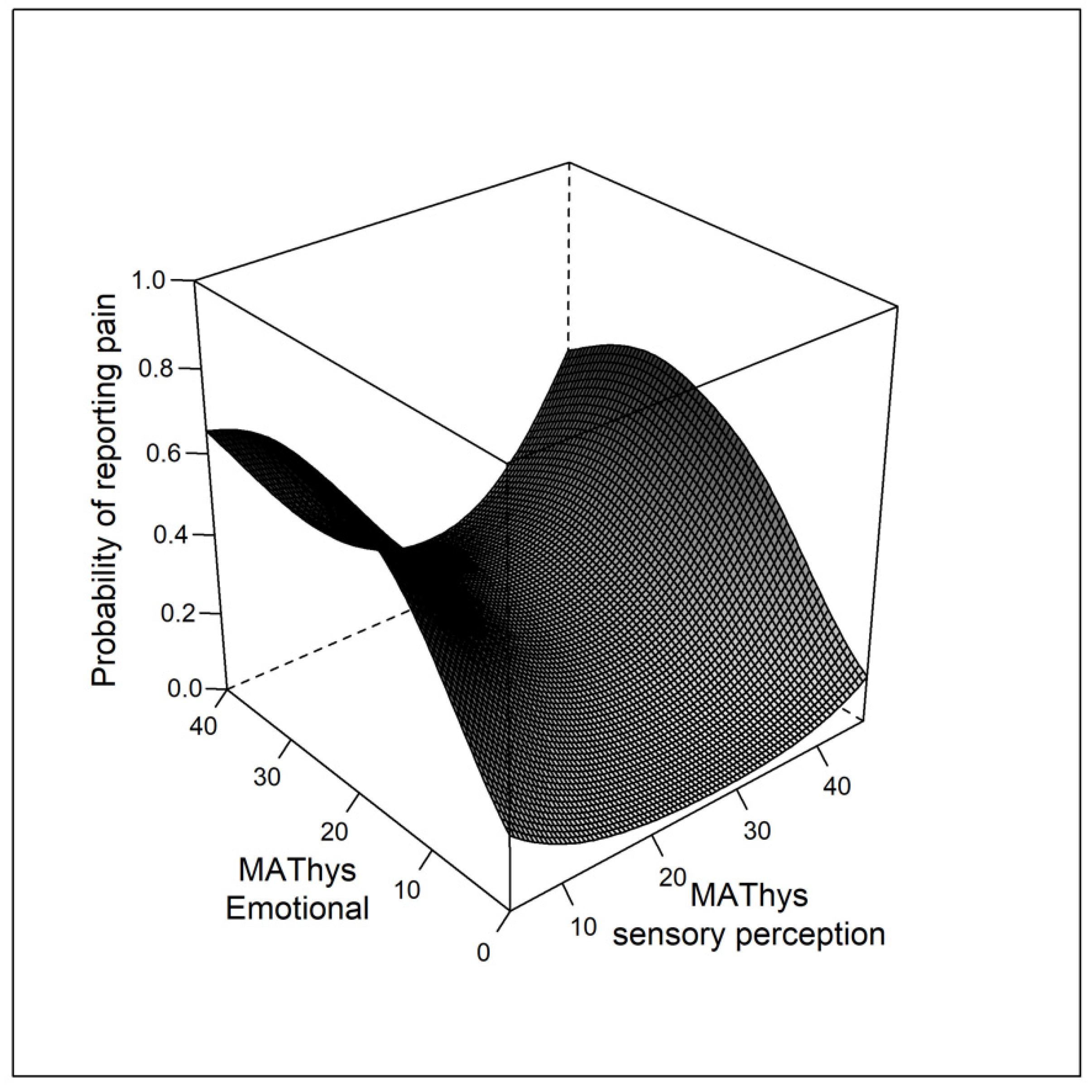
3.2.1. Model 1: Affective States and Self-Reported Pain
3.2.2. Model 2: BD Subtype and Self-Reported Pain
3.2.3. Model 3: Personality Traits and Self-Reported Pain
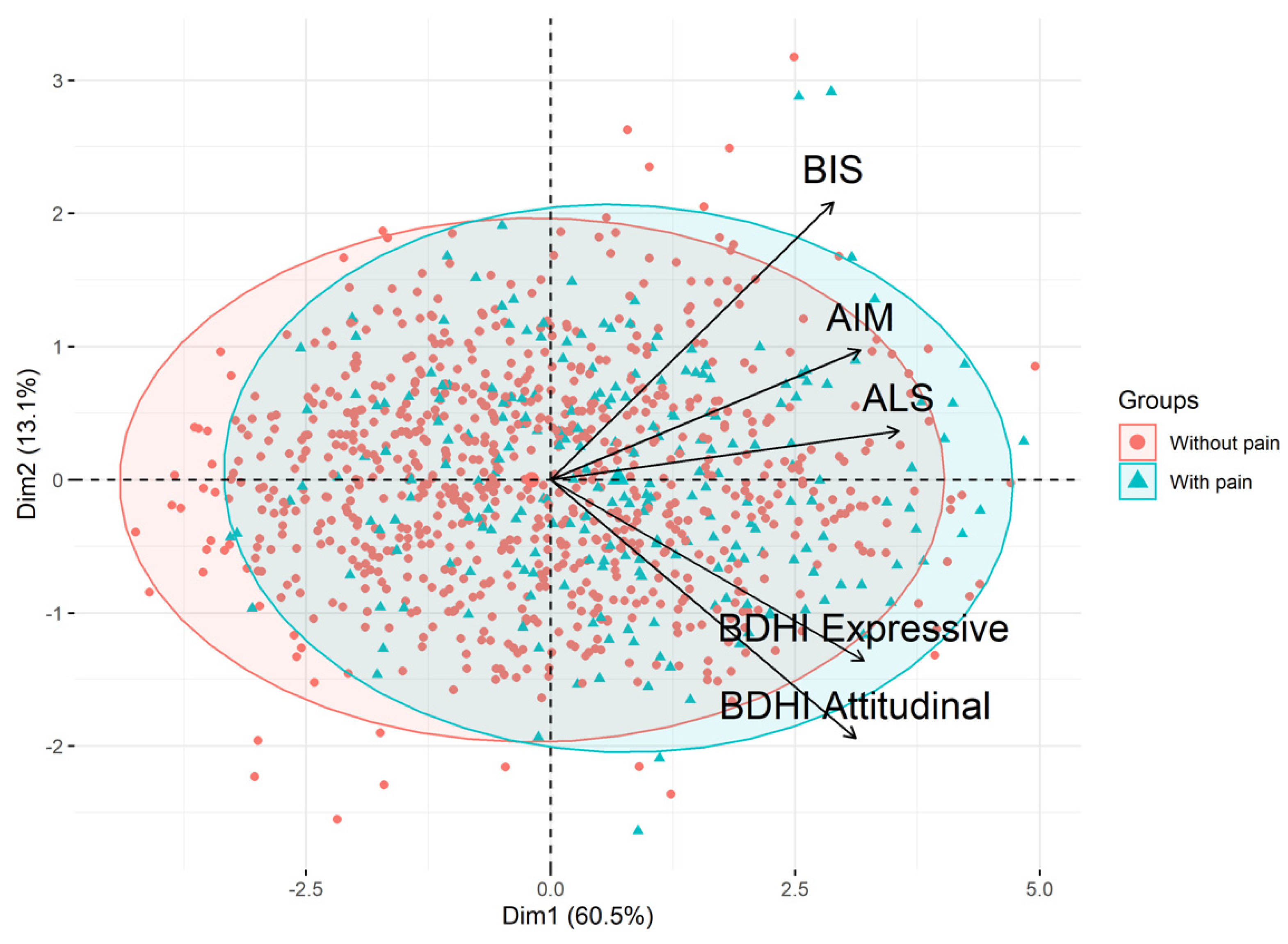
Step 1: Variable Clustering by PCA
Step 2: Association between Pain and “Borderline Personality Traits”
3.3. Longitudinal Analysis
3.3.1. Model 1: Pain at Baseline Is Associated with Global Functioning at One Year
3.3.2. Model 2: Pain at Baseline Is Associated with Depression at One Year
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Godin, O.; Etain, B.; Henry, C.; Bougerol, T.; Courtet, P.; Mayliss, L.; Passerieux, C.; Azorin, J.-M.; Kahn, J.-P.; Gard, S.; et al. Metabolic Syndrome in a French Cohort of Patients with Bipolar Disorder: Results From the FACE-BD Cohort. J. Clin. Psychiatry 2014, 75, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Sundquist, K.; Winkleby, M.A.; Sundquist, J. Comorbidities and Mortality in Bipolar Disorder: A Swedish National Cohort Study. JAMA Psychiatry 2013, 70, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Eggermont, L.; Mitchell, A.J.; De Hert, M.; Correll, C.U.; Soundy, A.; Rosenbaum, S.; Vancampfort, D. The Prevalence of Pain in Bipolar Disorder: A Systematic Review and Large-Scale Meta-Analysis. Acta Psychiatry Scandy 2015, 131, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Robinson, R.L.; Eckert, G.J.; Stang, P.E.; Croghan, T.W.; Kroenke, K. Impact of Pain on Depression Treatment Response in Primary Care. Psychosom. Med. 2004, 66, 17–22. [Google Scholar] [CrossRef]
- Kroenke, K.; Shen, J.; Oxman, T.E.; Williams, J.W.; Dietrich, A.J. Impact of Pain on the Outcomes of Depression Treatment: Results from the RESPECT Trial. Pain 2008, 134, 209–215. [Google Scholar] [CrossRef]
- Calati, R.; Laglaoui Bakhiyi, C.; Artero, S.; Ilgen, M.; Courtet, P. The Impact of Physical Pain on Suicidal Thoughts and Behaviors: Meta-Analyses. J. Psychiatr. Res. 2015, 71, 16–32. [Google Scholar] [CrossRef]
- Pei, J.-H.; Wang, X.-L.; Yu, Y.; Zhang, Y.-B.; Gou, L.; Nan, R.-L.; Chen, H.-X.; Dou, X.-M.; Han, Z.-J. Prevalence of Suicidal Ideation and Suicide Attempt in Patients with Migraine: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2020, 277, 253–259. [Google Scholar] [CrossRef]
- Rice, A.S.C.; Smith, B.H.; Blyth, F.M. Pain and the Global Burden of Disease. Pain 2016, 157, 791–796. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, E.E.; Rabideau, D.J.; Gigler, M.E.; Nierenberg, A.A.; Deckersbach, T.; Sylvia, L.G. Patient Perceptions of Physical Health and Bipolar Symptoms: The Intersection of Mental and Physical Health. J. Affect. Disord. 2016, 189, 203–206. [Google Scholar] [CrossRef] [Green Version]
- Fornaro, M.; Stubbs, B. A Meta-Analysis Investigating the Prevalence and Moderators of Migraines among People with Bipolar Disorder. J. Affect. Disord. 2015, 178, 88–97. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Veronese, N.; Thompson, T.; Fornaro, M.; Schofield, P.; Solmi, M.; Mugisha, J.; Carvalho, A.F.; Koyanagi, A. Depression and Pain: Primary Data and Meta-Analysis among 237 952 People across 47 Low- and Middle-Income Countries. Psychol. Med. 2017, 47, 2906–2917. [Google Scholar] [CrossRef]
- Sansone, R.A.; Sansone, L.A. Chronic Pain Syndromes and Borderline Personality. Innov. Clin. Neurosci. 2012, 9, 10–14. [Google Scholar]
- Fond, G.; Boyer, L.; Andrianarisoa, M.; Godin, O.; Bulzacka, E.; Berna, F.; Brunel, L.; Coulon, N.; Aouizerate, B.; Capdevielle, D.; et al. Self-Reported Pain in Patients with Schizophrenia. Results from the National First-Step FACE-SZ Cohort. Prog. Neuropsychopharmacol. Biol. Psychiatry 2018, 85, 62–68. [Google Scholar] [CrossRef]
- Failde, I.; Dueñas, M.; Agüera-Ortíz, L.; Cervilla, J.A.; Gonzalez-Pinto, A.; Mico, J.A. Factors Associated with Chronic Pain in Patients with Bipolar Depression: A Cross-Sectional Study. BMC Psychiatry 2013, 13, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karling, P.; Maripuu, M.; Wikgren, M.; Adolfsson, R.; Norrbäck, K.F. The Association between Affectivity, Perceived Stress and Pain in Patients with Bipolar Disorder. J. Depress. Anxiety 2016, 5, 244. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, B.I.; Houck, P.R.; Karp, J.F. Factors Associated with Pain Interference in an Epidemiologic Sample of Adults with Bipolar I Disorder. J. Affect. Disord. 2009, 117, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, A.K.; Sylvia, L.G. The Role of Sleep in Bipolar Disorder. Nat. Sci. Sleep 2016, 8, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrimpf, M.; Liegl, G.; Boeckle, M.; Leitner, A.; Geisler, P.; Pieh, C. The Effect of Sleep Deprivation on Pain Perception in Healthy Subjects: A Meta-Analysis. Sleep Med. 2015, 16, 1313–1320. [Google Scholar] [CrossRef]
- Krause, A.J.; Prather, A.A.; Wager, T.D.; Lindquist, M.A.; Walker, M.P. The Pain of Sleep Loss: A Brain Characterization in Humans. J. Neurosci. 2019, 39, 2291–2300. [Google Scholar] [CrossRef] [Green Version]
- Aas, M.; Henry, C.; Bellivier, F.; Lajnef, M.; Gard, S.; Kahn, J.-P.; Lagerberg, T.V.; Aminoff, S.R.; Bjella, T.; Leboyer, M.; et al. Affective Lability Mediates the Association between Childhood Trauma and Suicide Attempts, Mixed Episodes and Co-Morbid Anxiety Disorders in Bipolar Disorders. Psychol. Med. 2017, 47, 902–912. [Google Scholar] [CrossRef] [PubMed]
- Etain, B.; Lajnef, M.; Henry, C.; Aubin, V.; Azorin, J.M.; Bellivier, F.; Bougerol, T.; Courtet, P.; Gard, S.; Kahn, J.P.; et al. Childhood Trauma, Dimensions of Psychopathology and the Clinical Expression of Bipolar Disorders: A Pathway Analysis. J. Psychiatr. Res. 2017, 95, 37–45. [Google Scholar] [CrossRef]
- Lagerberg, T.V.; Aminoff, S.R.; Aas, M.; Bjella, T.; Henry, C.; Leboyer, M.; Pedersen, G.; Bellivier, F.; Icick, R.; Andreassen, O.A.; et al. Alcohol Use Disorders Are Associated with Increased Affective Lability in Bipolar Disorder. J. Affect. Disord. 2017, 208, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Swann, A.C.; Dougherty, D.M.; Pazzaglia, P.J.; Pham, M.; Moeller, F.G. Impulsivity: A Link between Bipolar Disorder and Substance Abuse. Bipolar Disord. 2004, 6, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Jakubczyk, A.; Brower, K.J.; Kopera, M.; Krasowska, A.; Michalska, A.; Łoczewska, A.; Majewska, A.; Ilgen, M.; Fudalej, S.; Wojnar, M. Physical Pain and Impulsivity in Alcohol-Dependent Patients. Addict. Res. Theory 2016, 24, 458–465. [Google Scholar] [CrossRef]
- Tragesser, S.L.; Bruns, D.; Disorbio, J.M. Borderline Personality Disorder Features and Pain: The Mediating Role of Negative Affect in a Pain Patient Sample. Clin. J. Pain 2010, 26, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Gerhart, J.I.; Burns, J.W.; Bruehl, S.; Smith, D.A.; Post, K.M.; Porter, L.S.; Schuster, E.; Buvanendran, A.; Fras, A.M.; Keefe, F.J. Variability in Negative Emotions among Individuals with Chronic Low Back Pain: Relationships with Pain and Function. Pain 2018, 159, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.J.; Carpenter, R.W.; Tragesser, S.L. Accounting for the Association between BPD Features and Chronic Pain Complaints in a Pain Patient Sample: The Role of Emotion Dysregulation Factors. Personal. Disord. Theory Res. Treat. 2018, 9, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Henry, C.; M’Bailara, K.; Mathieu, F.; Poinsot, R.; Falissard, B. Construction and Validation of a Dimensional Scale Exploring Mood Disorders: MAThyS (Multidimensional Assessment of Thymic States). BMC Psychiatry 2008, 8, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiech, K. Deconstructing the Sensation of Pain: The Influence of Cognitive Processes on Pain Perception. Science 2016, 354, 584–587. [Google Scholar] [CrossRef]
- Henry, C.; Etain, B.; Mathieu, F.; Raust, A.; Vibert, J.-F.; Scott, J.; Leboyer, M. A French Network of Bipolar Expert Centres: A Model to Close the Gap between Evidence-Based Medicine and Routine Practice. J. Affect. Disord. 2011, 131, 358–363. [Google Scholar] [CrossRef]
- Henry, C.; Godin, O.; Courtet, P.; Azorin, J.-M.; Gard, S.; Bellivier, F.; Polosan, M.; Kahn, J.-P.; Roux, P.; Aubin, V.; et al. Outcomes for Bipolar Patients Assessed in the French Expert Center Network: A 2-Year Follow-up Observational Study (FondaMental Advanced Centers of Expertise for Bipolar Disorder [FACE-BD]). Bipolar Disord. 2017, 19, 651–660. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh Sleep Quality Index as a Screening Tool for Sleep Dysfunction in Clinical and Non-Clinical Samples: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Rosa, A.R.; Sánchez-Moreno, J.; Martínez-Aran, A.; Salamero, M.; Torrent, C.; Reinares, M.; Comes, M.; Colom, F.; Van Riel, W.; Ayuso-Mateos, J.; et al. Validity and Reliability of the Functioning Assessment Short Test (FAST) in Bipolar Disorder. Clin. Pract. Epidemiol. Ment. Health 2007, 3, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, N.; Li, M.; Chevalier, J.; Lloyd, A.; Herdman, M. A Comparison of the Scaling Properties of the English, Spanish, French, and Chinese EQ-5D Descriptive Systems. Qual. Life Res. 2013, 22, 2237–2243. [Google Scholar] [CrossRef]
- Durham, J.; Steele, J.G.; Breckons, M.; Story, W.; Vale, L. DEEP Study: Does EQ-5D-5L Measure the Impacts of Persistent Oro-Facial Pain? J. Oral Rehabil. 2015, 42, 643–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obradovic, M.; Lal, A.; Liedgens, H. Validity and Responsiveness of EuroQol-5 Dimension (EQ-5D) versus Short Form-6 Dimension (SF-6D) Questionnaire in Chronic Pain. Health Qual. Life Outcomes 2013, 11, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payakachat, N.; Ali, M.M.; Tilford, J.M. Can The EQ-5D Detect Meaningful Change? A Systematic Review. Pharmacoeconomics 2015, 33, 1137–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawiah, A.K.; Al Sayah, F.; Ohinmaa, A.; Johnson, J.A. Discriminative Validity of the EQ-5D-5 L and SF-12 in Older Adults with Arthritis. Health Qual. Life Outcomes 2019, 17, 68. [Google Scholar] [CrossRef]
- Whynes, D.K.; McCahon, R.A.; Ravenscroft, A.; Hodgkinson, V.; Evley, R.; Hardman, J.G. Responsiveness of the EQ-5D Health-Related Quality-of-Life Instrument in Assessing Low Back Pain. Value Health 2013, 16, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Garratt, A.M.; Furunes, H.; Hellum, C.; Solberg, T.; Brox, J.I.; Storheim, K.; Johnsen, L.G. Evaluation of the EQ-5D-3L and 5L Versions in Low Back Pain Patients. Health Qual. Life Outcomes 2021, 19, 155. [Google Scholar] [CrossRef]
- Nobile, B.; Dubois, J.; Aouizerate, B.; Aubin, V.; Loftus, J.; Bellivier, F.; Belzeaux, R.; Dubertret, C.; Gard, S.; Haffen, E.; et al. Characterization of Depressed Bipolar Patients with Current Suicidal Ideation. Aust. N. Z. J. Psychiatry 2021, 55, 289–304. [Google Scholar] [CrossRef]
- Bushman, B.J.; Cooper, H.M.; Lemke, K.M. Meta-Analysis of Factor Analyses: An Illustration Using the Buss-Durkee Hostility Inventory. Pers Soc. Psychol. Bull. 1991, 17, 344–349. [Google Scholar] [CrossRef]
- Fernandez, E.; Day, A.; Boyle, G.J. Measures of Anger and Hostility in Adults. In Measures of Personality and Social Psychological Constructs; Elsevier: Amsterdam, The Netherlands, 2015; pp. 74–100. ISBN 978-0-12-386915-9. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Lê, S.; Josse, J.; Husson, F. FactoMineR: An R Package for Multivariate Analysis. J. Stat. Soft. 2008, 25, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Wood, S.N.; Pya, N.; Säfken, B. Smoothing Parameter and Model Selection for General Smooth Models. J. Am. Stat. Assoc. 2016, 111, 1548–1563. [Google Scholar] [CrossRef]
- Wood, S.N. Generalized Additive Models: An Introduction with R, 2nd ed.; Chapman and Hall/CRC: London, UK, 2017; ISBN 978-1-315-37027-9. [Google Scholar]
- Rush, A.J.; Trivedi, M.H.; Ibrahim, H.M.; Carmody, T.J.; Arnow, B.; Klein, D.N.; Markowitz, J.C.; Ninan, P.T.; Kornstein, S.; Manber, R.; et al. The 16-Item Quick Inventory of Depressive Symptomatology (QIDS), Clinician Rating (QIDS-C), and Self-Report (QIDS-SR): A Psychometric Evaluation in Patients with Chronic Major Depression. Biol. Psychiatry 2003, 54, 573–583. [Google Scholar] [CrossRef]
- Bair, M.J.; Robinson, R.L.; Katon, W.; Kroenke, K. Depression and Pain Comorbidity: A Literature Review. Arch. Intern. Med. 2003, 163, 2433–2445. [Google Scholar] [CrossRef] [Green Version]
- Klauenberg, S.; Maier, C.; Assion, H.-J.; Hoffmann, A.; Krumova, E.K.; Magerl, W.; Scherens, A.; Treede, R.-D.; Juckel, G. Depression and Changed Pain Perception: Hints for a Central Disinhibition Mechanism. Pain 2008, 140, 332–343. [Google Scholar] [CrossRef]
- Tikàsz, A.; Tourjman, V.; Chalaye, P.; Marchand, S.; Potvin, S. Increased Spinal Pain Sensitization in Major Depressive Disorder: A Pilot Study. Psychiatry Res. 2016, 246, 756–761. [Google Scholar] [CrossRef]
- Yarnitsky, D. Conditioned Pain Modulation (the Diffuse Noxious Inhibitory Control-like Effect): Its Relevance for Acute and Chronic Pain States. Curr. Opin. Anaesthesiol. 2010, 23, 611–615. [Google Scholar] [CrossRef]
- Carpenter, R.W.; Tragesser, S.L.; Lane, S.P.; Trull, T.J. Momentary Assessment of Everyday Physical Pain in Outpatients with Borderline Personality Disorder. Personal. Disord. Theory Res. Treat. 2019, 10, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Fornaro, M.; Orsolini, L.; Marini, S.; De Berardis, D.; Perna, G.; Valchera, A.; Ganança, L.; Solmi, M.; Veronese, N.; Stubbs, B. The Prevalence and Predictors of Bipolar and Borderline Personality Disorders Comorbidity: Systematic Review and Meta-Analysis. J. Affect. Disord. 2016, 195, 105–118. [Google Scholar] [CrossRef] [PubMed]
- You, D.S.; Meagher, M.W. Association between Borderline Personality Features and Temporal Summation of Second Pain: A Cross-Sectional Study. Behav. Med. 2017, 43, 208–217. [Google Scholar] [CrossRef] [PubMed]
- De Paepe, A.L.; Crombez, G.; Legrain, V. What’s Coming Near? The Influence of Dynamical Visual Stimuli on Nociceptive Processing. PLoS ONE 2016, 11, e0155864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filbrich, L.; Blandiaux, S.; Manfron, L.; Farnè, A.; De Keyser, R.; Legrain, V. Unimodal and Crossmodal Extinction of Nociceptive Stimuli in Healthy Volunteers. Behav. Brain Res. 2019, 362, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Melzack, R. Pain and the Neuromatrix in the Brain. J. Dent. Educ. 2001, 65, 1378–1382. [Google Scholar] [CrossRef]
- Senkowski, D.; Höfle, M.; Engel, A.K. Crossmodal Shaping of Pain: A Multisensory Approach to Nociception. Trends Cogn. Sci. 2014, 18, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Summers, P.J.; Layne, R.M.; Ortega, A.C.; Harris, G.P.; Bamber, B.A.; Komuniecki, R.W. Multiple Sensory Inputs Are Extensively Integrated to Modulate Nociception in C. Elegans. J. Neurosci. 2015, 35, 10331–10342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goffaux, P.; Léonard, G.; Lévesque, M. Perception de la douleur en santé mentale. In Santé Mentale et Douleur; Springer Paris: Paris, France, 2013; pp. 37–52. ISBN 978-2-8178-0306-7. [Google Scholar]
- Rhudy, J.L.; Williams, A.E.; McCabe, K.M.; Nguye~n, M.A.T.V.; Rambo, P. Affective Modulation of Nociception at Spinal and Supraspinal Levels. Psychophysiology 2005, 42, 579–587. [Google Scholar] [CrossRef]
- Rhudy, J.L. Emotional Modulation of Pain. In Neuroscience of Pain, Stress, and Emotion; Elsevier: Amsterdam, The Netherlands, 2016; pp. 51–75. ISBN 978-0-12-800538-5. [Google Scholar]
- De Hert, M.; Correll, C.U.; Bobes, J.; Cetkovich-Bakmas, M.; Cohen, D.; Asai, I.; Detraux, J.; Gautam, S.; Möller, H.-J.; Ndetei, D.M.; et al. Physical Illness in Patients with Severe Mental Disorders. I. Prevalence, Impact of Medications and Disparities in Health Care. World Psychiatry 2011, 10, 52–77. [Google Scholar] [CrossRef] [Green Version]
- Kilbourne, A.M.; McCarthy, J.F.; Welsh, D.; Blow, F. Recognition of Co-Occurring Medical Conditions among Patients with Serious Mental Illness. J. Nerv. Ment. Dis. 2006, 194, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Lord, O.; Malone, D. Differences in the Prescribing of Medication for Physical Disorders in Individuals with v. without Mental Illness: Meta-Analysis. Br. J. Psychiatry 2012, 201, 435–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elman, I.; Zubieta, J.-K.; Borsook, D. The Missing P in Psychiatric Training: Why It Is Important to Teach Pain to Psychiatrists. Arch. Gen. Psychiatry 2011, 68, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, K.-J.; Tsai, J.-C.; Liu, D.; Lin, C.-H.; Chiu, H.-L.; Chou, K.-R. Efficacy of Cognitive-Behavioral Therapy in Patients with Bipolar Disorder: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2017, 12, e0176849. [Google Scholar] [CrossRef] [Green Version]
- Trauer, J.M.; Qian, M.Y.; Doyle, J.S.; Rajaratnam, S.M.W.; Cunnington, D. Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2015, 163, 191. [Google Scholar] [CrossRef]
- Eccleston, C.; de CWilliams, A.C.; Morley, S. Psychological Therapies for the Management of Chronic Pain (Excluding Headache) in Adults. Cochrane Database Syst. Rev. 2020, 8. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-Based Interventions for Psychiatric Disorders: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S.; Colaiaco, B.; Maher, A.R.; Shanman, R.M.; Sorbero, M.E.; et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-Analysis. Ann. Behav. Med. 2017, 51, 199–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enke, O.; New, H.A.; New, C.H.; Mathieson, S.; McLachlan, A.J.; Latimer, J.; Maher, C.G.; Lin, C.-W.C. Anticonvulsants in the Treatment of Low Back Pain and Lumbar Radicular Pain: A Systematic Review and Meta-Analysis. CMAJ 2018, 190, E786–E793. [Google Scholar] [CrossRef] [Green Version]
- Ferraro, M.C.; Bagg, M.K.; Wewege, M.A.; Cashin, A.G.; Leake, H.B.; Rizzo, R.R.N.; Jones, M.D.; Gustin, S.M.; Day, R.; Loo, C.K.; et al. Efficacy, Acceptability, and Safety of Antidepressants for Low Back Pain: A Systematic Review and Meta-Analysis. Syst. Rev. 2021, 10, 62. [Google Scholar] [CrossRef]
- Chou, R.; Deyo, R.; Friedly, J.; Skelly, A.; Weimer, M.; Fu, R.; Dana, T.; Kraegel, P.; Griffin, J.; Grusing, S. Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann. Intern. Med. 2017, 166, 480. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Without Pain Mean (sd)/Number (%) | With Pain Mean (sd)/Number (%) | p-Value | |
|---|---|---|---|---|
| Sociodemographic | ||||
| n | 685 | 195 | ||
| Age (years) | 39.88 (12.83) | 41.83 (11.86) | 0.06 | |
| Sex | Men | 278 (40.6) | 70 (35.9) | 0.27 |
| Women | 407 (59.4) | 125 (64.1) | ||
| Single | No | 350 (51.1) | 103 (52.8) | 0.73 |
| Yes | 335 (48.9) | 92 (47.2) | ||
| Education (High school diploma) | No | 245 (35.8) | 85 (43.6) | 0.06 |
| Yes | 440 (64.2) | 110 (56.4) | ||
| Clinical | ||||
| BD subtype | I | 329 (48) | 80 (41) | 0.19 |
| II | 286 (41.8) | 95 (48.7) | ||
| NOS | 70 (10.2) | 20 (10.3) | ||
| Age at BD onset (years) | 23.48 (9.13) | 23.89 (9.44) | 0.6 | |
| Number of depressive episodes | 4.96 (4.48) | 6.50 (5.71) | 0.0004 | |
| Number of manic episodes | 1.09 (1.99) | 1.00 (2.52) | 0.6 | |
| Number of hypomanic episodes | 3.32 (4.83) | 4.10 (5.44) | 0.1 | |
| Lifetime history of suicide attempt | No | 463 (67.6) | 121 (62.1) | 0.17 |
| Yes | 222 (32.4) | 74 (37.9) | ||
| Current substance use disorder | No | 612 (89.3) | 171 (87.7) | 0.6 |
| Yes | 73 (10.7) | 24 (12.3) | ||
| Lifetime anxiety disorder | No | 435 (63.5) | 96 (49.2) | 0.0004 |
| Yes | 250 (36.5) | 99 (50.8) | ||
| Lifetime eating disorder | No | 560 (81.8) | 150 (76.9) | 0.16 |
| Yes | 125 (18.2) | 45 (23.1) | ||
| Multiple sclerosis | No | 661 (99.5) | 188 (99.5) | 1 |
| Yes | 3 (0.5) | 1 (0.5) | ||
| Cancer | No | 628 (97.2) | 175 (96.7) | 0.9 |
| Yes | 18 (2.8) | 6 (3.3) | ||
| Inflammatory bowel disease | No | 659 (99.2) | 184(98.9) | 0.65 |
| Yes | 5 (0.8) | 2 (1.1) | ||
| Rheumatoid arthritis | No | 670 (99.9) | 191 (100) | 1 |
| Yes | 1 (0.1) | 0 (0) | ||
| Ulcer | No | 644 (97.3) | 176 (94.6) | 0.12 |
| Yes | 18 (2.7) | 10 (5.4) | ||
| QIDS-SR (without item 12) Box–Cox Transformed | 5.13 (2.61) | 6.82 (2.54) | <0.0001 | |
| Suicidal ideation (QIDS-SR item 12) | No (0) | 500 (73) | 106 (54.4) | <0.0001 |
| Yes (>1) | 185 (27) | 89 (45.6) | ||
| YMRS | 0 | 370 (54) | 92 (47.2) | 0.24 |
| (1–7) | 250 (36.5) | 81 (41.5) | ||
| >7 | 65 (9.5) | 22 (11.3) | ||
| PSQI (0–21) | 6.52 (3.58) | 9.021 (4.15) | <0.0001 | |
| STAI-Y (state) (0–60) | 40.88 (14.01) | 48.35 (14.18) | <0.0001 | |
| MAThyS Emotional (0–40) | 20.99 (6.49) | 22.93 (7.12) | 0.0003 | |
| MAThyS Motivation (0–40) | 17.56 (6.65) | 16.07 (8.07) | 0.009 | |
| MAThyS Cognition (0–40) | 20.31 (5.85) | 20.72 (7.05) | 0.4 | |
| MAThyS Sensory perception (0–50) | 25.89 (4.58) | 25.81 (7.16) | 0.86 | |
| MAThyS Psychomotor (0–30) | 12.83 (5.36) | 11.90 (6.22) | 0.04 | |
| AIM | 3.66 (0.69) | 3.93 (0.63) | <0.0001 | |
| ALS | 1.18 (0.67) | 1.55 (0.63) | <0.0001 | |
| BDHI Expressive Component | 20.07 (7.90) | 23.15(8.133) | 0.0001 | |
| BDHI Attitudinal Component | 6.99 (4.28) | 8.97 (4.20) | <0.0001 | |
| BIS-10 | 66.19 (11.12) | 70.51 (11.57) | <0.0001 | |
| Lithium carbonate | No | 425 (62) | 143 (73.3) | 0.005 |
| Yes | 260 (38) | 52 (26.7) | ||
| Anticonvulsant | No | 340 (49.6) | 84 (43.1) | 0.12 |
| Yes | 345 (50.4) | 111 (56.9) | ||
| Antipsychotic | No | 369 (53.9) | 108 (55.4) | 0.77 |
| Yes | 316 (46.1) | 87 (44.6) | ||
| Anxiolytic | No | 521 (76.1) | 136 (69.7) | 0.09 |
| Yes | 164 (23.9) | 59 (30.3) | ||
| Hypnotic | No | 580 (84.7) | 157 (80.5) | 0.2 |
| Yes | 105 (15.3) | 38 (19.5) | ||
| Antidepressant | No | 420 (61.3) | 107 (54.9) | 0.12 |
| Yes | 265 (38.7) | 88 (45.1) |
| Model 1 | Model 2 | Model 3 | |
|---|---|---|---|
| Age | 1.01 (1.00–1.03) | 1.01 (1.00–1.03) | 1.02 (1.00–1.03) |
| Education (high school diploma) | 0.79 (0.56–1.13) | 0.78 (0.54–1.11) | 0.87 (0.60–1.26) |
| PSQI | 1.10 (1.04–1.15) | 1.09 (1.04–1.15) | 1.08 (1.03–1.14) |
| QIDS-SR (without item 12) Box–Cox | 1.19 (1.09–1.30) | 1.19 (1.09–1.30) | 1.14 (1.04–1.25) |
| MAThyS emotional ☨ | |||
| MAThyS sensory ☨ | |||
| BD subtype II ✦ | 1.11 (0.76–1.62) | ||
| BD subtype NOS ✦ | 0.78 (0.42–1.45) | ||
| “Borderline personality traits” ✧ | 1.13 (1.00–1.29) |
| Questionnaires | Correlation with the First PCA Component: “Borderline Personality Traits” ✧ |
|---|---|
| AIM | 0.77 |
| ALS | 0.87 |
| BDHI Attitudinal Component | 0.76 |
| BDHI Expressive Component | 0.78 |
| BIS-10 | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Risch, N.; Dubois, J.; M’bailara, K.; Cussac, I.; Etain, B.; Belzeaux, R.; Dubertret, C.; Haffen, E.; Schwan, R.; Samalin, L.; et al. Self-Reported Pain and Emotional Reactivity in Bipolar Disorder: A Prospective FACE-BD Study. J. Clin. Med. 2022, 11, 893. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030893
Risch N, Dubois J, M’bailara K, Cussac I, Etain B, Belzeaux R, Dubertret C, Haffen E, Schwan R, Samalin L, et al. Self-Reported Pain and Emotional Reactivity in Bipolar Disorder: A Prospective FACE-BD Study. Journal of Clinical Medicine. 2022; 11(3):893. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030893
Chicago/Turabian StyleRisch, Nathan, Jonathan Dubois, Katia M’bailara, Irena Cussac, Bruno Etain, Raoul Belzeaux, Caroline Dubertret, Emmanuel Haffen, Raymund Schwan, Ludovic Samalin, and et al. 2022. "Self-Reported Pain and Emotional Reactivity in Bipolar Disorder: A Prospective FACE-BD Study" Journal of Clinical Medicine 11, no. 3: 893. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030893