
Guided Bone Regeneration in the Edentulous Atrophic Maxilla Using Deproteinized Bovine Bone Mineral (DBBM) Combined with Platelet-Rich Fibrin (PRF)—A Prospective Study

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Outcomes Assessment
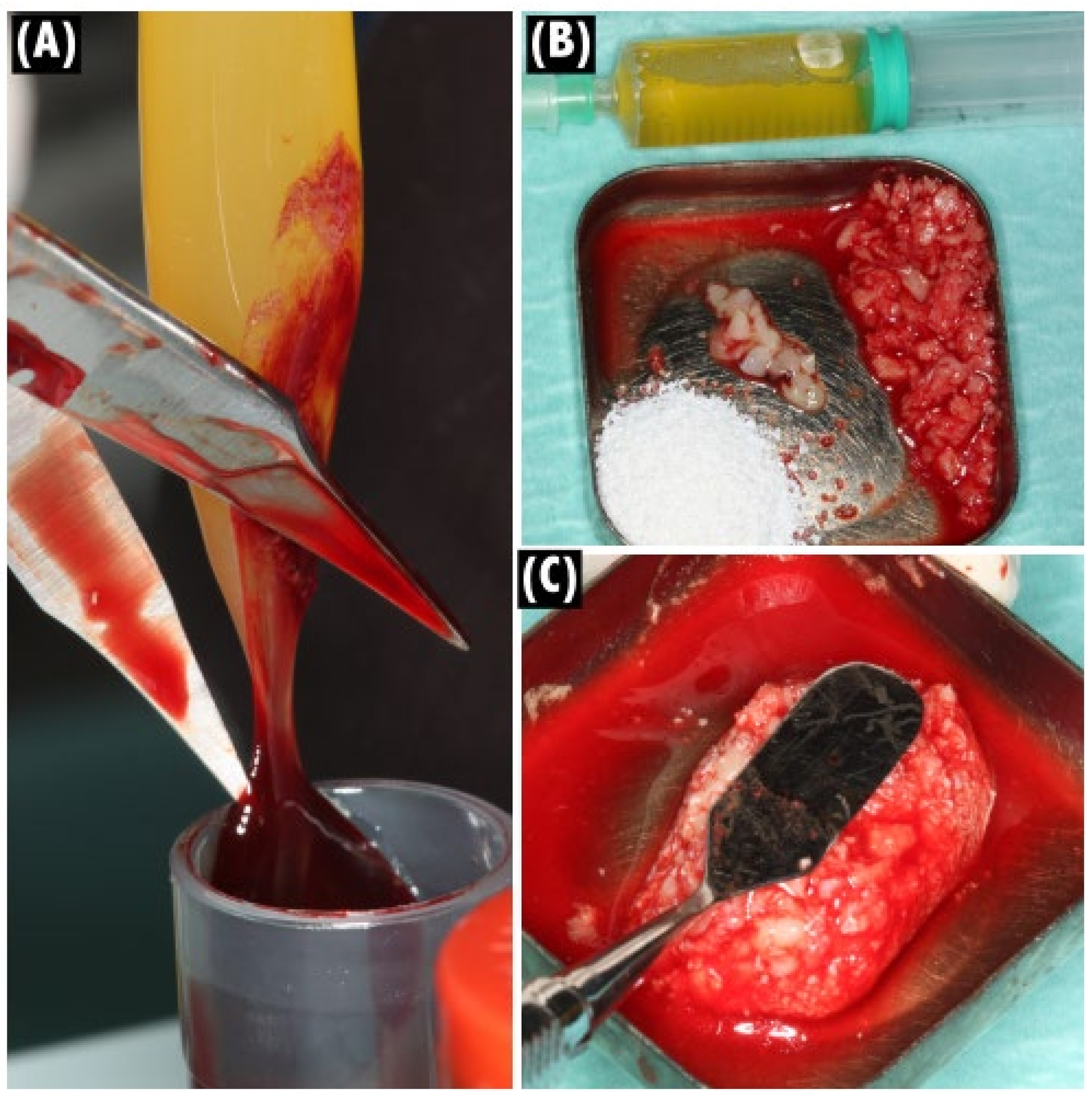
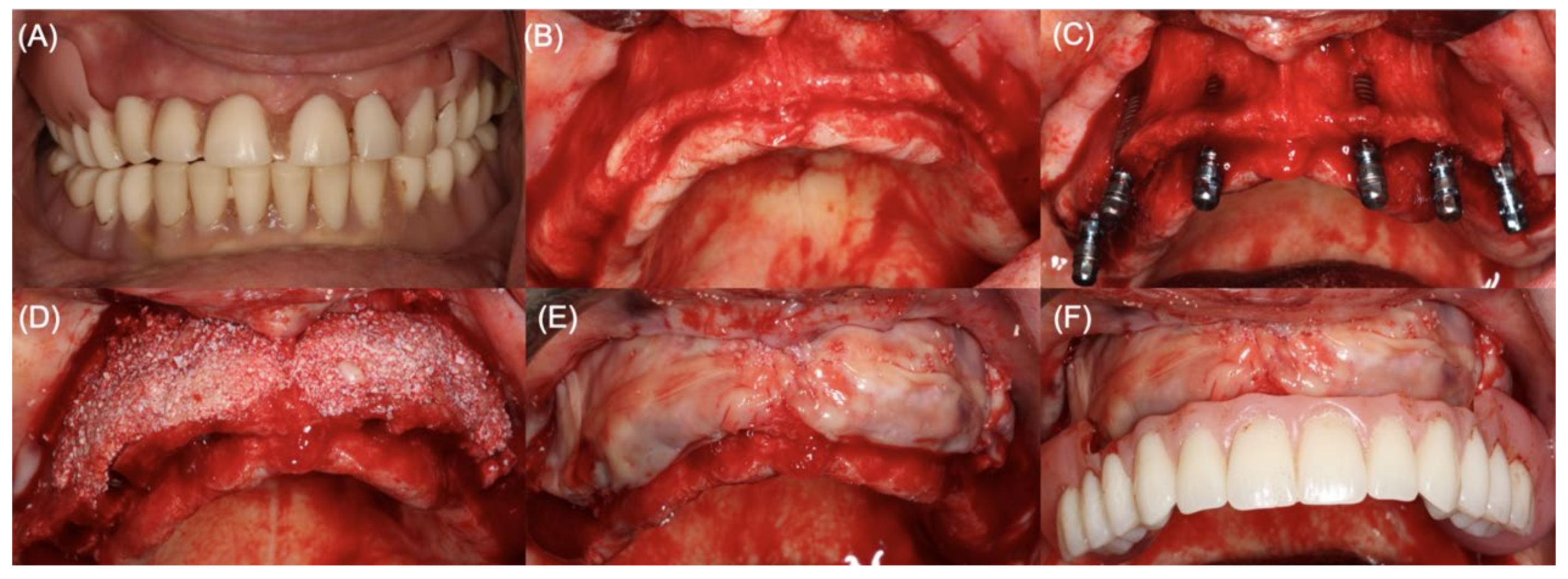
2.3. Clinical Procedures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PRF | Platelet-rich fibrin |
| CBCT | Cone beam computed tomography |
| GBR | Guided bone regeneration |
| APCs | Autologous platelet concentrates (APCs) |
| PDGF | Platelet derived growth factor |
| TGF-β1 | Transforming growth factor β1 |
| IGF | Insulin-like growth factor |
| VEGF | Vascular endothelial growth factor |
| DBBM | Deproteinized bovine bone mineral |
| ASA | American Society of Anesthesiology (physical status classification score I–VI) |
| MRONJ | Medication related to osteonecrosis of the jaw |
| SRs | Systematic reviews |
| ISR | Implant survival rate |
| RCT | Randomized clinical trial |
References
- Mertens, C.; Freier, K.; Engel, M.; Krisam, J.; Hoffmann, J.; Freudlsperger, C. Reconstruction of the severely atrophic edentulous maxillae with calvarial bone grafts. Clin. Oral Implant. Res. 2016, 28, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, G.O.; Avrampou, M.; Taylor, J.C.; Elpers, J.; Thalji, G.; Cooper, L. Maxillary Implant-Supported Fixed Prosthesis: A Survey of Reviews and Key Variables for Treatment Planning. Int. J. Oral Maxillofac. Implant. 2017, 31, s192–s197. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23 (Suppl. S5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Van Der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Chiapasco, M.; Casentini, P. Horizontal bone-augmentation procedures in implant dentistry: Prosthetically guided regeneration. Periodontology 2000 2018, 77, 213–240. [Google Scholar] [CrossRef]
- Sutton, D.; Lewis, B.; Patel, M.; Cawood, J. Changes in facial form relative to progressive atrophy of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 2004, 33, 676–682. [Google Scholar] [CrossRef]
- Bidra, A.S. Three-Dimensional Esthetic Analysis in Treatment Planning for Implant-Supported Fixed Prosthesis in the Edentulous Maxilla: Review of the Esthetics Literature. J. Esthet. Restor. Dent. 2011, 23, 219–236. [Google Scholar] [CrossRef]
- Pollini, A.; Goldberg, J.; Mitrani, R.; Morton, D. The Lip-Tooth-Ridge Classification: A Guidepost for Edentulous Maxillary Arches. Diagnosis, Risk Assessment, and Implant Treatment Indications. Int. J. Periodontics Restor. Dent. 2017, 37, 835–841. [Google Scholar] [CrossRef] [Green Version]
- Kuchler, U.; von Arx, T. Horizontal ridge augmentation in conjunction with or prior to implant placement in the anterior maxilla: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Cordaro, M.; Donno, S.; Ausenda, F.; Cordaro, L. Influence of Bone Anatomy on Implant Placement Procedures in Edentulous Arches of Elderly Individuals: A Cross-Sectional Study on Computed Tomography Images. Int. J. Oral Maxillofac. Implant. 2020, 35, 995–1004. [Google Scholar] [CrossRef]
- Pommer, B.; Mailath-Pokorny, G.; Haas, R.; Busenlechner, D.; Fürhauser, R.; Watzek, G. Patients’ preferences towards minimally invasive treatment alternatives for implant rehabilitation of edentulous jaws. Eur. J. Oral Implant. 2014, 7 (Suppl. S2), S91–S109. [Google Scholar]
- Aghaloo, T.L.; Misch, C.; Lin, G.-H.; Iacono, V.J.; Wang, H.-L. Bone Augmentation of the Edentulous Maxilla for Implant Placement: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2017, 31, s19–s30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caramês, J.M.M.; Marques, D.N.D.S.; Caramês, G.B.; Francisco, H.C.O.; Vieira, F.A. Implant Survival in Immediately Loaded Full-Arch Rehabilitations Following an Anatomical Classification System—A Retrospective Study in 1200 Edentulous Jaws. J. Clin. Med. 2021, 10, 5167. [Google Scholar] [CrossRef] [PubMed]
- Elnayef, B.; Monje, A.; Lin, G.-H.; Gargallo-Albiol, J.; Chan, H.-L.; Wang, H.-L.; Hernández-Alfaro, F. Alveolar Ridge Split on Horizontal Bone Augmentation: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2015, 30, 596–606. [Google Scholar] [CrossRef] [Green Version]
- Milinkovic, I.; Cordaro, L. Are there specific indications for the different alveolar bone augmentation procedures for implant placement? A systematic review. Int. J. Oral Maxillofac. Surg. 2014, 43, 606–625. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Felice, P.; Karatzopoulos, G.; Worthington, H.; Coulthard, P. The Efficacy of Horizontal and Vertical Bone Augmentation Procedures for Dental Implants: A Cochrane Systematic Review. Eur. J. Oral Implant. 2009, 2, 167–184. [Google Scholar] [CrossRef]
- Wessing, B.; Lettner, S.; Zechner, W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 87–100. [Google Scholar] [CrossRef]
- Elnayef, B.; Porta, C.; Suárez-López del Amo, F.; Mordini, L.; Gargallo-Albiol, J.; Hernández-Alfaro, F. The Fate of Lateral Ridge Augmentation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 622–635. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, P.H.D.A.; Trento, G.D.S.; Moura, L.B.; Cunha, G.; Gabrielli, M.A.C.; Pereira-Filho, V.A. Horizontal ridge augmentation using xenogenous bone graft—Systematic review. Oral Maxillofac. Surg. 2019, 23, 271–279. [Google Scholar] [CrossRef]
- Jung, R.E.; Fenner, N.; Hämmerle, C.H.; Zitzmann, N.U. Long-term outcome of implants placed with guided bone regeneration (GBR) using resorbable and non-resorbable membranes after 12–14 years. Clin. Oral Implant. Res. 2013, 24, 1065–1073. [Google Scholar] [CrossRef] [Green Version]
- Dahlin, C.; Linde, A.; Gottlow, J.; Nyman, S. Healing of Bone Defects by Guided Tissue Regeneration. Plast. Reconstr. Surg. 1988, 81, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.-L.; et al. Use of platelet-rich fibrin in regenerative dentistry: A systematic review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef] [PubMed]
- Fortunato, L.; Barone, S.; Bennardo, F.; Giudice, A. Management of Facial Pyoderma Gangrenosum Using Platelet-Rich Fibrin: A Technical Report. J. Oral Maxillofac. Surg. 2018, 76, 1460–1463. [Google Scholar] [CrossRef] [PubMed]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate.>Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar]
- Dohan Ehrenfest, D.M.; Pinto, N.R.; Pereda, A.; Jiménez, P.; Del Corso, M.; Kang, B.-S.; Nally, M.; Lanata, N.; Wang, H.-L.; Quirynen, M. The impact of the centrifuge characteristics and centrifugation protocols on the cells, growth factors, and fibrin architecture of a leukocyte- and platelet-rich fibrin (L-PRF) clot and membrane. Platelets 2018, 29, 171–184. [Google Scholar] [CrossRef]
- Temmerman, A.; Vandessel, J.; Castro, A.; Jacobs, R.; Teughels, W.; Pinto, N.; Quirynen, M. The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: A split-mouth, randomized, controlled clinical trial. J. Clin. Periodontol. 2016, 43, 990–999. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Katagiri, H.; Kono, M.; Schaller, B.; Zhang, Y.; Sculean, A.; Miron, R.J. Improved growth factor delivery and cellular activity using concentrated platelet-rich fibrin (C-PRF) when compared with traditional injectable (i-PRF) protocols. Clin. Oral Investig. 2020, 24, 4373–4383. [Google Scholar] [CrossRef]
- Brancaccio, Y.; Antonelli, A.; Barone, S.; Bennardo, F.; Fortunato, L.; Giudice, A. Evaluation of local hemostatic efficacy after dental extractions in patients taking antiplatelet drugs: A randomized clinical trial. Clin. Oral Investig. 2021, 25, 1159–1167. [Google Scholar] [CrossRef]
- Sanz, M.; Dahlin, C.; Apatzidou, D.; Artzi, Z.; Bozic, D.; Calciolari, E.; De Bruyn, H.; Dommisch, H.; Donos, N.; Eickholz, P.; et al. Biomaterials and regenerative technologies used in bone regeneration in the craniomaxillofacial region: Consensus report of group 2 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 82–91. [Google Scholar] [CrossRef]
- Dragonas, P.; Katsaros, T.; Ortiz, G.A.; Chambrone, L.; Schiavo, J.; Palaiologou, A. Effects of leukocyte–platelet-rich fibrin (L-PRF) in different intraoral bone grafting procedures: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 48, 250–262. [Google Scholar] [CrossRef]
- Mordenfeld, A.; Johansson, C.B.; Albrektsson, T.; Hallman, M. A randomized and controlled clinical trial of two different compositions of deproteinized bovine bone and autogenous bone used for lateral ridge augmentation. Clin. Oral Implant. Res. 2014, 25, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Caramês, J.; Da Mata, A.D.S.P.; Marques, D.N.D.S.; Francisco, H. Ceramic-Veneered Zirconia Frameworks in Full-Arch Implant Rehabilitations: A 6-Month to 5-Year Retrospective Cohort Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 1407–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvani, L.; Michalakis, K.; Hirayama, H. The influence of full-arch implant-retained fixed dental prostheses on upper lip support and lower facial esthetics: Preliminary clinical observations. Eur. J. Esthet. Dent. 2007, 2, 420–428. [Google Scholar]
- Uhlendorf, Y.; de Mattias Sartori, I.A.; Moreira Melo, A.C.; Uhlendorf, J. Changes in Lip Profile of Edentulous Patients after Placement of Maxillary Implant-Supported Fixed Prosthesis: Is a Wax Try-in a Reliable Diagnostic Tool? Int. J. Oral Maxillofac. Implant. 2017, 32, 593–597. [Google Scholar] [CrossRef] [Green Version]
- Pilipchuk, S.P.; Plonka, A.B.; Monje, A.; Taut, A.D.; Lanis, A.; Kang, B.; Giannobile, W.V. Tissue engineering for bone regeneration and osseointegration in the oral cavity. Dent. Mater. 2015, 31, 317–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valladão, C.A.A., Jr.; Monteiro, M.F.; Joly, J.C. Guided bone regeneration in staged vertical and horizontal bone augmentation using platelet-rich fibrin associated with bone grafts: A retrospective clinical study. Int. J. Implant Dent. 2020, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hartlev, J.; Nørholt, S.E.; Spin-Neto, R.; Kraft, D.; Schou, S.; Isidor, F. Histology of augmented autogenous bone covered by a platelet-rich fibrin membrane or deproteinized bovine bone mineral and a collagen membrane: A pilot randomized controlled trial. Clin. Oral Implant. Res. 2020, 31, 694–704. [Google Scholar] [CrossRef]
- Cortellini, S.; Castro, A.B.; Temmerman, A.; Van Dessel, J.; Pinto, N.; Jacobs, R.; Quirynen, M. Leucocyte- and platelet-rich fibrin block for bone augmentation procedure: A proof-of-concept study. J. Clin. Periodontol. 2018, 45, 624–634. [Google Scholar] [CrossRef]
- Sanz-Sánchez, I.; Ortiz-Vigón, A.; Sanz-Martín, I.; Figuero, E.; Sanz, M. Effectiveness of Lateral Bone Augmentation on the Alveolar Crest Dimension: A Systematic Review and Meta-analysis. J. Dent. Res. 2015, 94 (Suppl. S9), 128s–142s. [Google Scholar] [CrossRef]
- Benic, G.I.; Hämmerle, C.H.F. Horizontal bone augmentation by means of guided bone regeneration. Periodontology 2000 2014, 66, 13–40. [Google Scholar] [CrossRef]
- Mordenfeld, A.; Hallman, M.; Johansson, C.B.; Albrektsson, T. Histological and histomorphometrical analyses of biopsies harvested 11 years after maxillary sinus floor augmentation with deproteinized bovine and autogenous bone. Clin. Oral Implant. Res. 2010, 21, 961–970. [Google Scholar] [CrossRef]
- Miron, R.J.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Hernandez, M.; Choukroun, J. Platelet-Rich Fibrin and Soft Tissue Wound Healing: A Systematic Review. Tissue Eng. Part B Rev. 2017, 23, 83–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumetti, S.; Galli, C.; Manfredi, E.; Consolo, U.; Marchetti, C.; Ghiacci, G.; Toffoli, A.; Bonanini, M.; Salgarelli, A.; Macaluso, G.M. Correlation between Density and Resorption of Fresh-Frozen and Autogenous Bone Grafts. BioMed Res. Int. 2014, 2014, 508328. [Google Scholar] [CrossRef] [PubMed]
- Castagna, L.; Polido, W.; Soares, L.; Tinoco, E. Tomographic evaluation of iliac crest bone grafting and the use of immediate temporary implants to the atrophic maxilla. Int. J. Oral Maxillofac. Surg. 2013, 42, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Amorfini, L.; Migliorati, M.; Signori, A.; Silvestrini-Biavati, A.; Benedicenti, S. Block Allograft Technique versus Standard Guided Bone Regeneration: A Randomized Clinical Trial. Clin. Implant Dent. Relat. Res. 2013, 16, 655–667. [Google Scholar] [CrossRef]
- Sheridan, R.A.; Chiang, Y.-C.; Decker, A.M.; Sutthiboonyapan, P.; Chan, H.-L.; Wang, H.-L. The Effect of Implant-Induced Artifacts on Interpreting Adjacent Bone Structures on Cone-Beam Computed Tomography Scans. Implant Dent. 2018, 27, 10–14. [Google Scholar] [CrossRef]
- Shibly, O.; Patel, N.; Albandar, J.M.; Kutkut, A. Bone Regeneration around Implants in Periodontally Compromised Patients: A Randomized Clinical Trial of the Effect of Immediate Implant with Immediate Loading. J. Periodontol. 2010, 81, 1743–1751. [Google Scholar] [CrossRef]
- Jiang, X.; Zhou, W.; Wu, Y.; Wang, F. Clinical Outcomes of Immediate Implant Loading with Fixed Prostheses in Edentulous Maxillae: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2021, 36, 503–519. [Google Scholar] [CrossRef]
- Gapski, R.; Wang, H.-L.; Mascarenhas, P.; Lang, N.P. Critical review of immediate implant loading. Clin. Oral Implant. Res. 2003, 14, 515–527. [Google Scholar] [CrossRef]
- Attanasio, F.; Antonelli, A.; Brancaccio, Y.; Averta, F.; Figliuzzi, M.M.; Fortunato, L.; Giudice, M. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dent. J. 2020, 8, 21. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
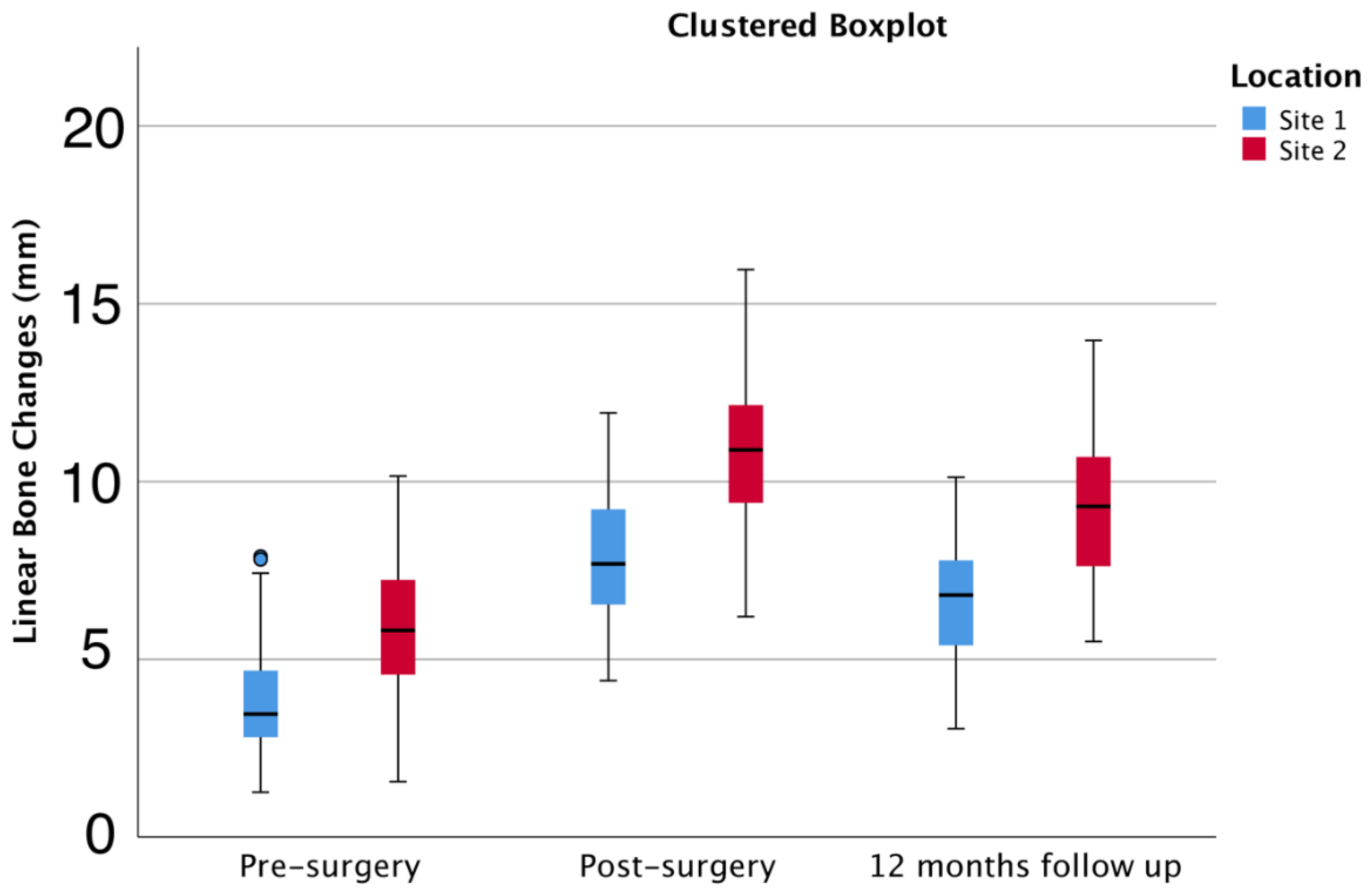
| Pre-Surgery | Post-Surgery | 12-Month Follow-Up | Bone Gain (12 Months—Pre-Surgery) | ||
|---|---|---|---|---|---|
| Site 1 | Mean | 3.52 | 7.79 | 6.53 | 3.01 |
| 95% CI | 3.19–3.85 | 7.30–8.28 | 6.09–6.96 | 2.51–3.50 | |
| Range | 6.16 | 7.53 | 6.6 | 8.17 | |
| Site 2 | Mean | 5.5 | 10.84 | 8.99 | 3.5 |
| 95% CI | 5.04–5.95 | 10.19–11.48 | 8.42–9.57 | 2.87–4.13 | |
| Range | 8.59 | 9.76 | 8.47 | 8.46 | |
| Total | Mean | 4.47 | 9.25 | 7.71 | 3.24 |
| 95% CI | 4.13–4.80 | 8.76–9.75 | 7.28–8.14 | 2.85–3.64 | |
| Range | 8.89 | 11.56 | 10.92 | 8.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caramês, J.M.M.; Vieira, F.A.; Caramês, G.B.; Pinto, A.C.; Francisco, H.C.O.; Marques, D.N.d.S. Guided Bone Regeneration in the Edentulous Atrophic Maxilla Using Deproteinized Bovine Bone Mineral (DBBM) Combined with Platelet-Rich Fibrin (PRF)—A Prospective Study. J. Clin. Med. 2022, 11, 894. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030894
Caramês JMM, Vieira FA, Caramês GB, Pinto AC, Francisco HCO, Marques DNdS. Guided Bone Regeneration in the Edentulous Atrophic Maxilla Using Deproteinized Bovine Bone Mineral (DBBM) Combined with Platelet-Rich Fibrin (PRF)—A Prospective Study. Journal of Clinical Medicine. 2022; 11(3):894. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030894
Chicago/Turabian StyleCaramês, João Manuel Mendez, Filipe Araújo Vieira, Gonçalo Bártolo Caramês, Ana Catarina Pinto, Helena Cristina Oliveira Francisco, and Duarte Nuno da Silva Marques. 2022. "Guided Bone Regeneration in the Edentulous Atrophic Maxilla Using Deproteinized Bovine Bone Mineral (DBBM) Combined with Platelet-Rich Fibrin (PRF)—A Prospective Study" Journal of Clinical Medicine 11, no. 3: 894. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030894