
Assessment of Neuromuscular and Psychological Function in People with Recurrent Neck Pain during a Period of Remission: Cross-Sectional and Longitudinal Analyses

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.2.1. RNP Eligibility Criteria
2.2.2. CNP Eligibility Criteria
2.2.3. Healthy Participants Eligibility Criteria
2.2.4. Exclusion Criteria of All Groups
2.3. Recruitment
2.4. Baseline Measures (Candidate Predictors)
Patient-Reported Outcome Measures
2.5. Testing Procedures
2.5.1. Cervical Kinematics
2.5.2. Neck Proprioception
2.5.3. Craniocervical Flexion
2.5.4. Maximal Neck Extension/Flexion (Isometric Contractions)
2.6. Instrumentation
2.6.1. Inertial Measurement Unit
2.6.2. NOD Dynamometer and Multi-Cervical Unit (MCU)
2.6.3. Electromyography Analysis
2.7. Baseline Objective Measures (Candidate Predictors)
2.8. Outcome Measures for the Longitudinal Analysis (Prediction Model)
2.8.1. Primary Outcome
2.8.2. Secondary Outcome
2.9. Sample Size
2.10. Statistical Analyses
2.10.1. Cross-Sectional Analysis
2.10.2. Longitudinal Analysis
3. Results
3.1. Characteristics of Participants
3.2. Cervical Kinematics and Proprioception
3.3. EMG Amplitude Assessed during Submaximal CCF Contractions
3.4. Maximal Neck Strength and Perceived Fatigue
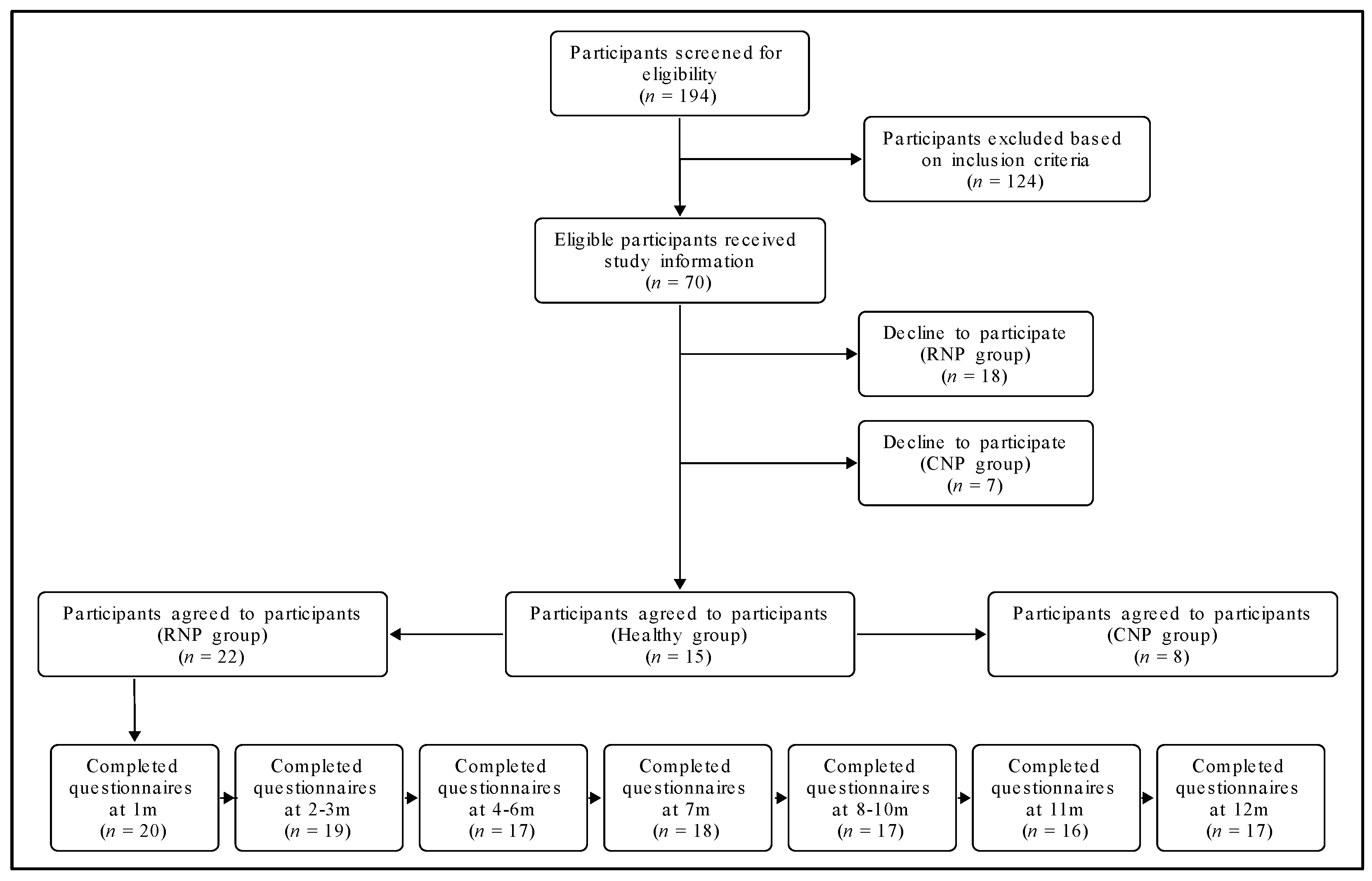
3.5. Participant Follow-Up through the Longitudinal Analysis
3.5.1. Characteristics of Participants
3.5.2. Step 1: Predictor Variable Selection (i.e., Shrinking the Number of Predictors)
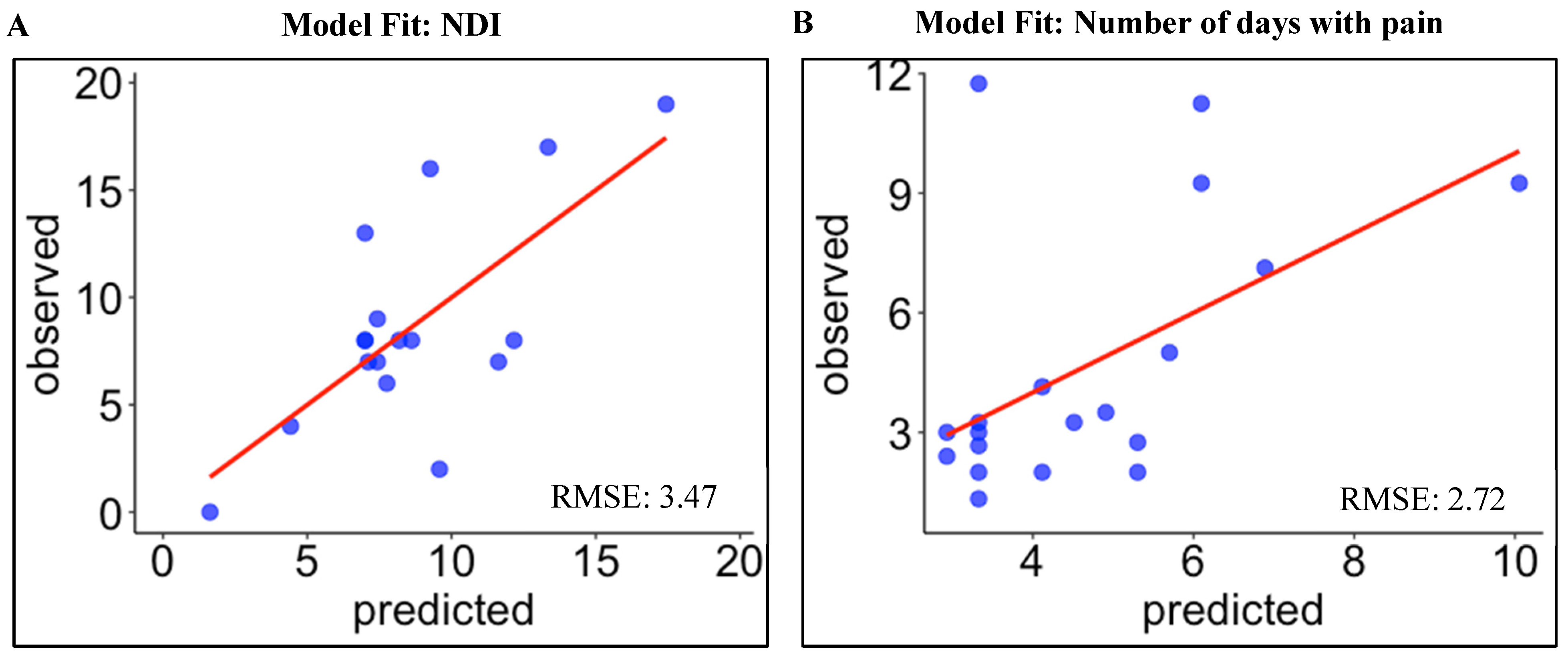
3.5.3. Step 2: Prediction Model Development
Prediction of Neck Pain and Disability at Six Months
Prediction of Future Episodes of Neck Pain over the 12-Month Follow-Up Period
4. Discussion
4.1. Cervical RoM
4.2. Velocity and Smoothness of Neck Movement
4.3. Cervical Proprioception
4.4. EMG Amplitude Assessed during CCF Submaximal Contractions
4.5. Maximal Neck Strength and Perceived Fatigue
4.6. Predicting Neck Disability and Number of Days with Pain
4.7. Model Performance
4.8. Clinical Implications
4.9. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carroll, L.J.; Ferrari, R.; Cassidy, J.D.; Côté, P. Coping and recovery in whiplash-associated disorders: Early use of passive coping strategies is associated with slower recovery of neck pain and pain-related disability. Clin. J. Pain 2014, 30, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Carroll, L.J.; Holm, L.W.; Hogg-Johnson, S.; Côté, P.; Cassidy, J.D.; Haldeman, S.; Nordin, M.; Hurwitz, E.L.; Carragee, E.J.; Van Der Velde, G. Course and prognostic factors for neck pain in whiplash-associated disorders (WAD): Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J. Manip. Physiol. Ther. 2009, 32, S97–S107. [Google Scholar] [CrossRef] [PubMed]
- Hoving, J.L.; O’leary, E.F.; Niere, K.R.; Green, S.; Buchbinder, R. Validity of the neck disability index, Northwick Park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders. Pain 2003, 102, 273–281. [Google Scholar] [CrossRef]
- Pinfold, M.; Niere, K.R.; O’leary, E.F.; Hoving, J.L.; Green, S.; Buchbinder, R. Validity and internal consistency of a whiplash-specific disability measure. Spine 2004, 29, 263–268. [Google Scholar] [CrossRef]
- Spitzer, W.O.; Skovron, M.L.; Salmi, L.R.; Cassidy, J.D.; Duranceau, J.; Suissa, S.; Zeiss, E. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: Redefining “whiplash” and its management. Spine 1995, 20, 1S–73S. [Google Scholar]
- Siegmund, G.P.; Winkelstein, B.A.; Ivancic, P.C.; Svensson, M.Y.; Vasavada, A. The anatomy and biomechanics of acute and chronic whiplash injury. Traffic Inj. Prev. 2009, 10, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Holm, L.W.; Carroll, L.J.; Cassidy, J.D.; Hogg-Johnson, S.; Côté, P.; Guzman, J.; Peloso, P.; Nordin, M.; Hurwitz, E.; van der Velde, G. The burden and determinants of neck pain in whiplash-associated disorders after traffic collisions: Results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J. Manip. Physiol. Ther. 2009, 32, S61–S69. [Google Scholar] [CrossRef]
- Hogg-Johnson, S.; Van Der Velde, G.; Carroll, L.J.; Holm, L.W.; Cassidy, J.D.; Guzman, J.; Côté, P.; Haldeman, S.; Ammendolia, C.; Carragee, E. The burden and determinants of neck pain in the general population. Eur. Spine J. 2008, 17, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Kamper, S.J.; Rebbeck, T.J.; Maher, C.G.; McAuley, J.H.; Sterling, M. Course and prognostic factors of whiplash: A systematic review and meta-analysis. Pain 2008, 138, 617–629. [Google Scholar] [CrossRef]
- Bussières, A.E.; Stewart, G.; Al-Zoubi, F.; Decina, P.; Descarreaux, M.; Haskett, D.; Hincapié, C.; Pagé, I.; Passmore, S.; Srbely, J. Spinal manipulative therapy and other conservative treatments for low back pain: A guideline from the Canadian chiropractic guideline initiative. J. Manip. Physiol. Ther. 2018, 41, 265–293. [Google Scholar] [CrossRef]
- Stanton, T.R.; Latimer, J.; Maher, C.G.; Hancock, M.J. A modified Delphi approach to standardize low back pain recurrence terminology. Eur. Spine J. 2011, 20, 744–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falla, D.; Jull, G.; Hodges, P. Feedforward activity of the cervical flexor muscles during voluntary arm movements is delayed in chronic neck pain. Exp. Brain Res. 2004, 157, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.L.; Jull, G.A.; Hodges, P.W. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine 2004, 29, 2108–2114. [Google Scholar] [CrossRef] [PubMed]
- Schomacher, J.; Farina, D.; Lindstroem, R.; Falla, D. Chronic trauma-induced neck pain impairs the neural control of the deep semispinalis cervicis muscle. Clin. Neurophysiol. 2012, 123, 1403–1408. [Google Scholar] [CrossRef]
- Falla, D.; Bilenkij, G.; Jull, G. Patients with chronic neck pain demonstrate altered patterns of muscle activation during performance of a functional upper limb task. Spine 2004, 29, 1436–1440. [Google Scholar] [CrossRef]
- Mazaheri, M.; Abichandani, D.; Kingma, I.; Treleaven, J.; Falla, D. A meta-analysis and systematic review of changes in joint position sense and static standing balance in patients with whiplash-associated disorder. PLoS ONE 2021, 16, e0249659. [Google Scholar] [CrossRef]
- Sterling, M.; Jull, G.; Vicenzino, B.; Kenardy, J.; Darnell, R. Development of motor system dysfunction following whiplash injury. Pain 2003, 103, 65–73. [Google Scholar] [CrossRef]
- Pearson, I.; Reichert, A.; De Serres, S.J.; Dumas, J.-P.; Côté, J.N. Maximal voluntary isometric neck strength deficits in adults with whiplash-associated disorders and association with pain and fear of movement. J. Orthop. Sports Phys. Ther. 2009, 39, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Baydal-Bertomeu, J.M.; Page, Á.F.; Belda-Lois, J.M.; Garrido-Jaén, D.; Prat, J.M. Neck motion patterns in whiplash-associated disorders: Quantifying variability and spontaneity of movement. Clin. Biomech. 2011, 26, 29–34. [Google Scholar] [CrossRef]
- Moghaddas, D.; de Zoete, R.M.J.; Edwards, S.; Snodgrass, S.J. Differences in the kinematics of the cervical and thoracic spine during functional movement in individuals with or without chronic neck pain: A systematic review. Physiotherapy 2019, 105, 421–433. [Google Scholar] [CrossRef]
- Salehi, R.; Rasouli, O.; Saadat, M.; Mehravar, M.; Negahban, H.; Yazdi, M.J.S. Cervical movement kinematic analysis in patients with chronic neck pain: A comparative study with healthy subjects. Musculoskelet. Sci. Pract. 2021, 53, 102377. [Google Scholar] [CrossRef] [PubMed]
- Sjolander, P.; Michaelson, P.; Jaric, S.; Djupsjobacka, M. Sensorimotor disturbances in chronic neck pain--range of motion, peak velocity, smoothness of movement, and repositioning acuity. Man. Ther. 2008, 13, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Bahat, H.S.; Chen, X.; Reznik, D.; Kodesh, E.; Treleaven, J. Interactive cervical motion kinematics: Sensitivity, specificity and clinically significant values for identifying kinematic impairments in patients with chronic neck pain. Man. Ther. 2015, 20, 295–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demirbüken, İ.; Özgül, B.; Kuru Çolak, T.; Aydoğdu, O.; Sarı, Z.; Yurdalan, S.U. Kinesiophobia in relation to physical activity in chronic neck pain. J. Back Musculoskelet. Rehabil. 2016, 29, 41–47. [Google Scholar] [CrossRef]
- Jull, G.; Trott, P.; Potter, H.; Zito, G.; Niere, K.; Shirley, D.; Emberson, J.; Marschner, I.; Richardson, C. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine 2002, 27, 1835–1843. [Google Scholar] [CrossRef]
- Sterling, M.; Jull, G.; Wright, A. The effect of musculoskeletal pain on motor activity and control. J. Pain 2001, 2, 135–145. [Google Scholar] [CrossRef]
- Walton, D.M.; Macdermid, J.C.; Giorgianni, A.A.; Mascarenhas, J.C.; West, S.C.; Zammit, C.A. Risk factors for persistent problems following acute whiplash injury: Update of a systematic review and meta-analysis. J. Orthop. Sports Phys. Ther. 2013, 43, 31–43. [Google Scholar] [CrossRef] [Green Version]
- Daenen, L.; Nijs, J.; Raadsen, B.; Roussel, N.; Cras, P.; Dankaerts, W. Cervical motor dysfunction and its predictive value for long-term recovery in patients with acute whiplash-associated disorders: A systematic review. J. Rehabil. Med. 2013, 45, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Scholten-Peeters, G.G.; Verhagen, A.P.; Bekkering, G.E.; van der Windt, D.A.; Barnsley, L.; Oostendorp, R.A.; Hendriks, E.J. Prognostic factors of whiplash-associated disorders: A systematic review of prospective cohort studies. Pain 2003, 104, 303. [Google Scholar] [CrossRef]
- Sarrami, P.; Armstrong, E.; Naylor, J.M.; Harris, I.A. Factors predicting outcome in whiplash injury: A systematic meta-review of prognostic factors. J. Orthop. Traumatol. Off. J. Ital. Soc. Orthop. Traumatol. 2017, 18, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Walton, D.M.; Carroll, L.J.; Kasch, H.; Sterling, M.; Verhagen, A.P.; Macdermid, J.C.; Gross, A.; Santaguida, P.L.; Carlesso, L. An Overview of Systematic Reviews on Prognostic Factors in Neck Pain: Results from the International Collaboration on Neck Pain (ICON) Project. Open Orthop. J. 2013, 7, 494–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devecchi, V.; Rushton, A.B.; Gallina, A.; Heneghan, N.R.; Falla, D. Are neuromuscular adaptations present in people with recurrent spinal pain during a period of remission? A systematic review. PLoS ONE 2021, 16, e0249220. [Google Scholar] [CrossRef] [PubMed]
- Elsig, S.; Luomajoki, H.; Sattelmayer, M.; Taeymans, J.; Tal-Akabi, A.; Hilfiker, R. Sensorimotor tests, such as movement control and laterality judgment accuracy, in persons with recurrent neck pain and controls. A case-control study. Man. Ther. 2014, 19, 555–561. [Google Scholar] [CrossRef]
- Jull, G.A.; Soderlund, A.; Stemper, B.D.; Kenardy, J.; Gross, A.R.; Cote, P.; Treleaven, J.; Bogduk, N.; Sterling, M.; Curatolo, M. Toward optimal early management after whiplash injury to lessen the rate of transition to chronicity: Discussion paper 5. Spine 2011, 36, S335–S342. [Google Scholar] [CrossRef]
- Alalawi, A.; Gallina, A.; Sterling, M.; Falla, D. Are physical factors associated with poor prognosis following a whiplash trauma? A protocol for a systematic review and data synthesis. BMJ Open 2019, 9, e033298. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Fisher, L.D. Comparative reliability and validity of chronic pain intensity measures. Pain 1999, 83, 157–162. [Google Scholar] [CrossRef]
- Vernon, H.; Mior, S. The Neck Disability Index: A study of reliability and validity. J. Manip. Physiol. Ther. 1991, 14, 409–415. [Google Scholar]
- Crawford, J.R.; Khan, R.J.; Varley, G.W. Early management and outcome following soft tissue injuries of the neck—A randomised controlled trial. Injury 2004, 35, 891–895. [Google Scholar] [CrossRef]
- Rosenfeld, M.; Gunnarsson, R.; Borenstein, P. Early intervention in whiplash-associated disorders: A comparison of two treatment protocols. Spine 2000, 25, 1782–1787. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, M.E.; Seferiadis, A.; Carlsson, J.; Gunnarsson, R. Active Intervention in Patients with Whiplash-Associated Disorders Improves Long-Term Prognosis: A Randomized Controlled Clinical Trial. Spine 2003, 28, 2491–2498. [Google Scholar] [CrossRef] [PubMed]
- Langley, G.; Sheppeard, H. The visual analogue scale: Its use in pain measurement. Rheumatol. Int. 1985, 5, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, A.M.; Preuper, H.R.S.; Reneman, M.F.; Posthumus, J.B.; Stewart, R.E. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int. J. Rehabil. Res. 2008, 31, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breivik, E.K.; Björnsson, G.A.; Skovlund, E. A comparison of pain rating scales by sampling from clinical trial data. Clin. J. Pain 2000, 16, 22–28. [Google Scholar] [CrossRef]
- Wainner, R.S.; Fritz, J.M.; Irrgang, J.J.; Boninger, M.L.; Delitto, A.; Allison, S. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine 2003, 28, 52–62. [Google Scholar] [CrossRef]
- Sterling, M.; Jull, G.; Vicenzino, B.; Kenardy, J.; Darnell, R. Physical and psychological factors predict outcome following whiplash injury. Pain 2005, 114, 141–148. [Google Scholar] [CrossRef]
- Lemeunier, N.; da Silva-Oolup, S.; Olesen, K.; Shearer, H.; Carroll, L.; Brady, O.; Côté, E.; Stern, P.; Tuff, T.; Suri-Chilana, M. Reliability and validity of self-reported questionnaires to measure pain and disability in adults with neck pain and its associated disorders: Part 3—A systematic review from the CADRE Collaboration. Eur. Spine J. 2019, 28, 1156–1179. [Google Scholar] [CrossRef]
- Roelofs, J.; Sluiter, J.K.; Frings-Dresen, M.H.; Goossens, M.; Thibault, P.; Boersma, K.; Vlaeyen, J.W. Fear of movement and (re) injury in chronic musculoskeletal pain: Evidence for an invariant two-factor model of the Tampa Scale for Kinesiophobia across pain diagnoses and Dutch, Swedish, and Canadian samples. Pain 2007, 131, 181–190. [Google Scholar] [CrossRef]
- Vlaeyen, J.; Kole-Snijders, A.M.; Boeren, R.G.; Van Eek, H. Fear of movement/(re) injury in chronic low back pain and its relation to behavioral performance. Pain 1995, 62, 363–372. [Google Scholar] [CrossRef]
- Woby, S.R.; Roach, N.K.; Urmston, M.; Watson, P.J. Psychometric properties of the TSK-11: A shortened version of the Tampa Scale for Kinesiophobia. Pain 2005, 117, 137–144. [Google Scholar] [CrossRef]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Janssen, M.F.; Birnie, E.; Haagsma, J.A.; Bonsel, G.J. Comparing the standard EQ-5D three-level system with a five-level version. Value Health 2008, 11, 275–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Y.-S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Bahat, H.S.; Weiss, P.L.; Laufer, Y. The effect of neck pain on cervical kinematics, as assessed in a virtual environment. Arch. Phys. Med. Rehabil. 2010, 91, 1884–1890. [Google Scholar] [CrossRef]
- Meisingset, I.; Woodhouse, A.; Stensdotter, A.-K.; Stavdahl, Ø.; Lorås, H.; Gismervik, S.; Andresen, H.; Austreim, K.; Vasseljen, O. Evidence for a general stiffening motor control pattern in neck pain: A cross sectional study. BMC Musculoskelet. Disord. 2015, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Alsultan, F.; Cescon, C.; De Nunzio, A.M.; Barbero, M.; Heneghan, N.R.; Rushton, A.; Falla, D. Variability of the helical axis during active cervical movements in people with chronic neck pain. Clin. Biomech. 2019, 62, 50–57. [Google Scholar] [CrossRef]
- Barbero, M.; Falla, D.; Clijsen, R.; Ghirlanda, F.; Schneebeli, A.; Ernst, M.J.; Cescon, C. Can parameters of the helical axis be measured reliably during active cervical movements? Musculoskelet. Sci. Pract. 2017, 27, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Lindstroem, R.; Graven-Nielsen, T.; Falla, D. Current pain and fear of pain contribute to reduced maximum voluntary contraction of neck muscles in patients with chronic neck pain. Arch. Phys. Med. Rehabil. 2012, 93, 2042–2048. [Google Scholar] [CrossRef]
- Chiu, T.T.W.; Lo, S.K. Evaluation of cervical range of motion and isometric neck muscle strength: Reliability and validity. Clin. Rehabil. 2002, 16, 851–858. [Google Scholar] [CrossRef]
- Falla, D.; Dall’Alba, P.; Rainoldi, A.; Merletti, R.; Jull, G. Location of innervation zones of sternocleidomastoid and scalene muscles—A basis for clinical and research electromyography applications. Clin. Neurophysiol. 2002, 113, 57–63. [Google Scholar] [CrossRef]
- Falla, D.; Farina, D.; Dahl, M.K.; Graven-Nielsen, T. Pain-induced changes in cervical muscle activation do not affect muscle fatigability during sustained isometric contraction. J. Electromyogr. Kinesiol. 2008, 18, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Park, R.J.; Tsao, H.; Claus, A.; Cresswell, A.G.; Hodges, P.W. Recruitment of discrete regions of the psoas major and quadratus lumborum muscles is changed in specific sitting postures in individuals with recurrent low back pain. J. Orthop. Sports Phys. Ther. 2013, 43, 833–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahat, H.S.; Sprecher, E.; Sela, I.; Treleaven, J. Neck motion kinematics: An inter-tester reliability study using an interactive neck VR assessment in asymptomatic individuals. Eur. Spine J. 2016, 25, 2139–2148. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; O’Leary, S.; Farina, D.; Jull, G. The change in deep cervical flexor activity after training is associated with the degree of pain reduction in patients with chronic neck pain. Clin. J. Pain 2012, 28, 628–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jull, G.; Falla, D. Does increased superficial neck flexor activity in the craniocervical flexion test reflect reduced deep flexor activity in people with neck pain? Man. Ther. 2016, 25, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Riley, R.D.; Hayden, J.A.; Steyerberg, E.W.; Moons, K.G.; Abrams, K.; Kyzas, P.A.; Malats, N.; Briggs, A.; Schroter, S.; Altman, D.G. Prognosis Research Strategy (PROGRESS) 2: Prognostic factor research. PLoS Med. 2013, 10, e1001380. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Alalawi, A.; Luque-Suarez, A.; Fernandez-Sanchez, M.; Gallina, A.; Evans, D.; Falla, D. Do measures of physical function enhance the prediction of persistent pain and disability following a whiplash injury? Protocol for a prospective observational study in Spain. BMJ Open 2020, 10, e035736. [Google Scholar] [CrossRef]
- Sterling, M.; Hendrikz, J.; Kenardy, J. Compensation claim lodgement and health outcome developmental trajectories following whiplash injury: A prospective study. Pain 2010, 150, 22–28. [Google Scholar] [CrossRef]
- Michaleff, Z.A.; Maher, C.G.; Lin, C.-W.C.; Rebbeck, T.; Jull, G.; Latimer, J.; Connelly, L.; Sterling, M. Comprehensive physiotherapy exercise programme or advice for chronic whiplash (PROMISE): A pragmatic randomised controlled trial. Lancet 2014, 384, 133–141. [Google Scholar] [CrossRef]
- Sterling, M.; Hendrikz, J.; Kenardy, J.; Kristjansson, E.; Dumas, J.-P.; Niere, K.; Cote, J.; Deserres, S.; Rivest, K.; Jull, G. Assessment and validation of prognostic models for poor functional recovery 12 months after whiplash injury: A multicentre inception cohort study. Pain 2012, 153, 1727–1734. [Google Scholar] [CrossRef] [PubMed]
- da Silva, T.; Mills, K.; Brown, B.T.; Pocovi, N.; de Campos, T.; Maher, C.; Hancock, M.J. Recurrence of low back pain is common: A prospective inception cohort study. J. Physiother. 2019, 65, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Eklund, A.; Jensen, I.; Lohela-Karlsson, M.; Hagberg, J.; Leboeuf-Yde, C.; Kongsted, A.; Bodin, L.; Axén, I. The Nordic Maintenance Care program: Effectiveness of chiropractic maintenance care versus symptom-guided treatment for recurrent and persistent low back pain—A pragmatic randomized controlled trial. PLoS ONE 2018, 13, e0203029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherlin, M.A.; Mangum, L.C.; Russell, S.; Saliba, S.; Hertel, J.; Hart, J.M. Landing stiffness between individuals with and without a history of low back pain. J. Sport Rehabil. 2020, 29, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Alalawi, A.; Evans, D.W.; Liew, B.; Peolsson, A.; Heneghan, N.; Rushton, A.; Peterson, G.; Barbero, M.; Falla, D. Does Pain Extent Predict Ongoing Pain and Disability in Patients with Chronic Whiplash-Associated Disorders? J. Clin. Med. 2022, 11, 555. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Pavlou, M.; Ambler, G.; Seaman, S.R.; Guttmann, O.; Elliott, P.; King, M.; Omar, R.Z. How to develop a more accurate risk prediction model when there are few events. BMJ 2015, 351, h3868. [Google Scholar] [CrossRef] [Green Version]
- Browne, M.W. Cross-validation methods. J. Math. Psychol. 2000, 44, 108–132. [Google Scholar] [CrossRef] [Green Version]
- Jacobucci, R.; Brandmaier, A.M.; Kievit, R.A. A practical guide to variable selection in structural equation modeling by using regularized multiple-indicators, multiple-causes models. Adv. Methods Pract. Psychol. Sci. 2019, 2, 55–76. [Google Scholar] [CrossRef] [Green Version]
- Riley, R.D.; van der Windt, D.; Croft, P.; Moons, K.G. Prognosis Research in Healthcare: Concepts, Methods, and Impact; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Liew, B.X.; Peolsson, A.; Rugamer, D.; Wibault, J.; Löfgren, H.; Dedering, A.; Zsigmond, P.; Falla, D. Clinical predictive modelling of post-surgical recovery in individuals with cervical radiculopathy: A machine learning approach. Sci. Rep. 2020, 10, 16782. [Google Scholar] [CrossRef]
- Puschmann, A.-K.; Drießlein, D.; Beck, H.; Arampatzis, A.; Catalá, M.M.; Schiltenwolf, M.; Mayer, F.; Wippert, P.-M. Stress and self-efficacy as long-term predictors for chronic low back pain: A prospective longitudinal study. J. Pain Res. 2020, 13, 613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twisk, J.; de Boer, M.; de Vente, W.; Heymans, M. Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J. Clin. Epidemiol. 2013, 66, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Rüschendorf, L. Mathematische Statistik; Springer: Berlin/Heidelberg, Germany, 2014; Volume 62. [Google Scholar]
- Wippert, P.-M.; Puschmann, A.-K.; Drießlein, D.; Arampatzis, A.; Banzer, W.; Beck, H.; Schiltenwolf, M.; Schmidt, H.; Schneider, C.; Mayer, F. Development of a risk stratification and prevention index for stratified care in chronic low back pain. Focus: Yellow flags (MiSpEx network). Pain Rep. 2017, 2, e623. [Google Scholar] [CrossRef]
- Sterling, M.; Chadwick, B.J. Psychologic processes in daily life with chronic whiplash: Relations of posttraumatic stress symptoms and fear-of-pain to hourly pain and uptime. Clin. J. Pain 2010, 26, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Crosbie, J.; Nascimento, D.P.; de Faria Negrão Filho, R.; Ferreira, P. Do people with recurrent back pain constrain spinal motion during seated horizontal and downward reaching? Clin. Biomech. 2013, 28, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Fenety, A.; Kumar, S. Isokinetic trunk strength and lumbosacral range of motion in elite female field hockey players reporting low back pain. J. Orthop. Sports Phys. Ther. 1992, 16, 129–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, D. Low Back Position Awareness in People with and without Recurrent Non-Specific Low Back Pain; King’s College London (University of London): London, UK, 2013. [Google Scholar]
- Hodges, P.W.; Tucker, K. Moving differently in pain: A new theory to explain the adaptation to pain. Pain 2011, 152, S90–S98. [Google Scholar] [CrossRef]
- De Pauw, R.; Coppieters, I.; Palmans, T.; Danneels, L.; Meeus, M.; Cagnie, B. Motor impairment in patients with chronic neck pain: Does the traumatic event play a significant role? A case-control study. Spine J. 2018, 18, 1406–1416. [Google Scholar] [CrossRef]
- Treleaven, J.; LowChoy, N.; Darnell, R.; Panizza, B.; Brown-Rothwell, D.; Jull, G. Comparison of sensorimotor disturbance between subjects with persistent whiplash-associated disorder and subjects with vestibular pathology associated with acoustic neuroma. Arch. Phys. Med. Rehabil. 2008, 89, 522–530. [Google Scholar] [CrossRef]
- Woodhouse, A.; Vasseljen, O. Altered motor control patterns in whiplash and chronic neck pain. BMC Musculoskelet. Disord. 2008, 9, 90. [Google Scholar] [CrossRef] [Green Version]
- de Vries, J.; Ischebeck, B.; Voogt, L.; Van Der Geest, J.; Janssen, M.; Frens, M.; Kleinrensink, G.J. Joint position sense error in people with neck pain: A systematic review. Man. Ther. 2015, 20, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Treleaven, J. Dizziness, unsteadiness, visual disturbances, and postural control: Implications for the transition to chronic symptoms after a whiplash trauma. Spine 2011, 36, S211–S217. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; Jull, G.; Edwards, S.; Koh, K.; Rainoldi, A. Neuromuscular efficiency of the sternocleidomastoid and anterior scalene muscles in patients with chronic neck pain. Disabil. Rehabil. 2004, 26, 712–717. [Google Scholar] [CrossRef]
- Jull, G.; Kristjansson, E.; Dall’Alba, P. Impairment in the cervical flexors: A comparison of whiplash and insidious onset neck pain patients. Man. Ther. 2004, 9, 89–94. [Google Scholar] [CrossRef]
- Falla, D.; Farina, D.; Dahl, M.K.; Graven-Nielsen, T. Muscle pain induces task-dependent changes in cervical agonist/antagonist activity. J. Appl. Physiol. 2007, 102, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; Farina, D.; Graven-Nielsen, T. Experimental muscle pain results in reorganization of coordination among trapezius muscle subdivisions during repetitive shoulder flexion. Exp. Brain Res. 2007, 178, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; Farina, D. Neuromuscular adaptation in experimental and clinical neck pain. J. Electromyogr. Kinesiol. 2008, 18, 255–261. [Google Scholar] [CrossRef]
- Falla, D.; Jull, G.; Russell, T.; Vicenzino, B.; Hodges, P. Effect of neck exercise on sitting posture in patients with chronic neck pain. Phys. Ther. 2007, 87, 408–417. [Google Scholar] [CrossRef]
- Jull, G.; Falla, D.; Vicenzino, B.; Hodges, P. The effect of therapeutic exercise on activation of the deep cervical flexor muscles in people with chronic neck pain. Man. Ther. 2009, 14, 696–701. [Google Scholar] [CrossRef]
- Cagnie, B.; Cools, A.; De Loose, V.; Cambier, D.; Danneels, L. Differences in isometric neck muscle strength between healthy controls and women with chronic neck pain: The use of a reliable measurement. Arch. Phys. Med. Rehabil. 2007, 88, 1441–1445. [Google Scholar] [CrossRef]
- Scheuer, R.; Friedrich, M. Reliability of isometric strength measurements in trunk and neck region: Patients with chronic neck pain compared with pain-free persons. Arch. Phys. Med. Rehabil. 2010, 91, 1878–1883. [Google Scholar] [CrossRef] [PubMed]
- Ylinen, J.; Salo, P.; Nykänen, M.; Kautiainen, H.; Häkkinen, A. Decreased isometric neck strength in women with chronic neck pain and the repeatability of neck strength measurements. Arch. Phys. Med. Rehabil. 2004, 85, 1303–1308. [Google Scholar] [CrossRef] [PubMed]
- Ylinen, J.; Ruuska, J. Clinical use of neck isometric strength measurement in rehabilitation. Arch. Phys. Med. Rehabil. 1994, 75, 465–469. [Google Scholar] [CrossRef]
- Jull, G.; Falla, D.; Treleaven, J.; O’Leary, S. Management of Neck Pain Disorders E-Book: A Research Informed Approach; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Kumbhare, D.A.; Balsor, B.; Parkinson, W.L.; Harding Bsckin, P.; Bedard, M.; Papaioannou, A.; Adachi, J.D. Measurement of cervical flexor endurance following whiplash. Disabil. Rehabil. 2005, 27, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Prushansky, T.; Gepstein, R.; Gordon, C.; Dvir, Z. Cervical muscles weakness in chronic whiplash patients. Clin. Biomech. 2005, 20, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Descarreaux, M.; Mayrand, N.; Raymond, J. Neuromuscular control of the head in an isometric force reproduction task: Comparison of whiplash subjects and healthy controls. Spine J. 2007, 7, 647–653. [Google Scholar] [CrossRef]
- Edmondston, S.; Björnsdóttir, G.; Pálsson, T.; Solgård, H.; Ussing, K.; Allison, G. Endurance and fatigue characteristics of the neck flexor and extensor muscles during isometric tests in patients with postural neck pain. Man. Ther. 2011, 16, 332–338. [Google Scholar] [CrossRef]
- Lourenço, A.S.; Lameiras, C.; Silva, A.G. Neck flexor and extensor muscle endurance in subclinical neck pain: Intrarater reliability, standard error of measurement, minimal detectable change, and comparison with asymptomatic participants in a university student population. J. Manip. Physiol. Ther. 2016, 39, 427–433. [Google Scholar] [CrossRef]
- O’Leary, S.; Hoogma, C.; Solberg, Ø.M.; Sundberg, S.; Pedler, A.; Van Wyk, L. Comparative strength and endurance parameters of the craniocervical and cervicothoracic extensors and flexors in females with and without idiopathic neck pain. J. Appl. Biomech. 2019, 35, 209–215. [Google Scholar] [CrossRef]
- Langenfeld, A.; Humphreys, B.K.; Swanenburg, J.; Peterson, C.K. Prognostic factors for recurrences in neck pain patients up to 1 year after chiropractic care. J. Manip. Physiol. Ther. 2015, 38, 458–464. [Google Scholar] [CrossRef]
- Enthoven, P.; Skargren, E.; Carstensen, J.; Oberg, B. Predictive factors for 1-year and 5-year outcome for disability in a working population of patients with low back pain treated in primary care. Pain 2006, 122, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Croisier, J.-L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.-M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Cronström, A.; Creaby, M.W.; Nae, J.; Ageberg, E. Modifiable factors associated with knee abduction during weight-bearing activities: A systematic review and meta-analysis. Sports Med. 2016, 46, 1647–1662. [Google Scholar] [CrossRef] [PubMed]
- Fousekis, K.; Tsepis, E.; Poulmedis, P.; Athanasopoulos, S.; Vagenas, G. Intrinsic risk factors of non-contact quadriceps and hamstring strains in soccer: A prospective study of 100 professional players. Br. J. Sports Med. 2011, 45, 709–714. [Google Scholar] [CrossRef] [Green Version]
- Ryan, J.; DeBurca, N.; Mc Creesh, K. Risk factors for groin/hip injuries in field-based sports: A systematic review. Br. J. Sports Med. 2014, 48, 1089–1096. [Google Scholar] [CrossRef]
- Linton, S.J.; Gross, D.; Schultz, I.Z.; Main, C.; Côté, P.; Pransky, G.; Johnson, W. Prognosis and the identification of workers risking disability: Research issues and directions for future research. J. Occup. Rehabil. 2005, 15, 459–474. [Google Scholar] [CrossRef] [Green Version]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W.; Moons, K.G.; van der Windt, D.A.; Hayden, J.A.; Perel, P.; Schroter, S.; Riley, R.D.; Hemingway, H.; Altman, D.G.; Group, P. Prognosis Research Strategy (PROGRESS) 3: Prognostic model research. PLoS Med. 2013, 10, e1001381. [Google Scholar] [CrossRef] [Green Version]
- Fonti, V.; Belitser, E. Feature selection using lasso. VU Amst. Res. Pap. Bus. Anal. 2017, 30, 1–25. [Google Scholar]
- Falla, D.; O’Leary, S.; Farina, D.; Jull, G. Association between intensity of pain and impairment in onset and activation of the deep cervical flexors in patients with persistent neck pain. Clin. J. Pain 2011, 27, 309–314. [Google Scholar] [CrossRef]
- Lindstrøm, R.; Schomacher, J.; Farina, D.; Rechter, L.; Falla, D. Association between neck muscle coactivation, pain, and strength in women with neck pain. Man. Ther. 2011, 16, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Bahat, H.S.; Weiss, P.L.T.; Sprecher, E.; Krasovsky, A.; Laufer, Y. Do neck kinematics correlate with pain intensity, neck disability or with fear of motion? Man. Ther. 2014, 19, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Pool, J.J.; Ostelo, R.W.; Knol, D.; Bouter, L.M.; de Vet, H.C. Are psychological factors prognostic indicators of outcome in patients with sub-acute neck pain? Man. Ther. 2010, 15, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Data Collection Point | Domain | Variables | RNP | CNP | Healthy Controls |
|---|---|---|---|---|---|
| Baseline | Demographics | Age | ✓ | ✓ | ✓ |
| Gender | ✓ | ✓ | ✓ | ||
| Height | ✓ | ✓ | ✓ | ||
| Weight | ✓ | ✓ | ✓ | ||
| Patient-reported measures | NDI | ✓ | ✓ | ✓ | |
| TSK-11 | ✓ | ✓ | ✓ | ||
| EQ-5D | ✓ | ✓ | ✓ | ||
| Others | Number of neck pain episodes | ✓ | |||
| Average of pain episodes (VAS) | ✓ | ||||
| Neck pain duration | ✓ | ||||
| Current pain intensity | ✓ | ||||
| Objective measures | Cervical kinematics (RoM, velocity, and smoothness) | ✓ | ✓ | ✓ | |
| Neck proprioception | ✓ | ✓ | ✓ | ||
| Peak score of craniocervical flexion test | ✓ | ✓ | ✓ | ||
| Muscle activity during submaximal CCF contractions | ✓ | ✓ | ✓ | ||
| Maximum neck strength in flexion and extension (MVC flexion and extension [kg]) | ✓ | ✓ | ✓ | ||
| Perceived exertion during the submaximal task in flexion and extension (Borg’s scale) | ✓ | ✓ | ✓ | ||
| Outcome measures | Questionnaires | Number of days with pain | ✓ | ||
| Neck Disability Index (NDI) | ✓ |
| Groups | p-Value | |||
|---|---|---|---|---|
| Healthy Control (n = 15) | RNP (n = 22) | CNP (n = 8) | ||
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Age (years) | 31.1 ± 5.7 | 31.0 ± 11.8 | 33.6 ± 8.7 | 0.24 1 |
| Gender (male:female (%)) | 6:9 (60%) | 8:14 (64%) | 1:7 (88%) | 0.38 2 |
| Height (m) | 1.7 ± 0.1 | 1.7 ± 0.1 | 1.6 ± 0.1 | 0.02 3 |
| Weight (kg) | 69.1 ± 14.8 | 74.7 ± 18.0 | 59.5 ± 9.8 | 0.07 1 |
| NDI (0–50) | 0.7 ± 1.1 | 5.5 ± 3.2 * | 17.5 ± 7.6 *,† | <0.001 1 |
| TSK (17–68) | 29.1 ± 4.3 | 35.2 ± 5.5 * | 40.5 ± 7.5 * | <0.001 3 |
| EQ-5D (0–1) | 0.98 ± 0.04 | 0.92 ± 0.09 * | 0.68 ± 0.21 *,† | <0.001 1 |
| EQ VAS (0–100) | 85.5 ± 10.2 | 78.5 ± 15.4 | 64.1 ± 14.4 *,† | 0.005 1 |
| Number of pain episodes, 12 m | - | 5.9 ± 4.4 | - | |
| Average of pain episodes, VAS (0–100) | - | 56.4 ± 14.5 | - | |
| Current neck pain, VAS (0–100) | - | - | 56.1 ± 19.5 | |
| Neck pain duration, m | - | - | 39.1 ± 41.4 | |
| Groups | p-Value | |||
|---|---|---|---|---|
| Healthy Control (n = 15) | RNP (n = 22) | CNP (n = 8) | ||
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Flexion | ||||
| Vmean (°/s) | 72.8 ± 12.3 | 55.0 ± 18.5 * | 42.9 ± 14.3 * | 0.002 1 |
| Vpeak (°/s) | 149.5 ± 33.9 | 114.0 ± 41.3 * | 90.8 ± 28.8 * | 0.004 |
| NVP (n) | 9.4 ± 4.0 | 17.1 ± 9.4 * | 17.5 ± 8.2 | 0.005 2 |
| Extension | ||||
| Vmean (°/s) | 66.5 ± 15.7 | 55.4 ± 21.2 | 46.7 ± 16.5 | 0.09 1 |
| Vpeak (°/s) | 133.8 ± 31.5 | 111.0 ± 45.1 | 97.2 ± 34.4 | 0.12 |
| NVP (n) | 8.3 ± 4.1 | 17.8 ± 14.0 | 16.5 ± 9.0 | 0.066 1 |
| Right Rotation | ||||
| Vmean (°/s) | 132.5 ± 29.3 | 101.5 ± 41.7 * | 82.5 ± 22.0 * | 0.001 2 |
| Vpeak (°/s) | 244.7 ± 52.5 | 190.5 ± 76.7 | 157.1 ± 37.9 * | 0.001 2 |
| NVP (n) | 5.1 ± 3.3 | 8.6 ± 9.1 | 10.2 ± 6.5 | 0.017 1 |
| JPE | 3.8 ± 2.1 | 4.4 ± 2.5 | 5.5 ± 5.9 * | 0.76 1 |
| Left Rotation | ||||
| Vmean (°/s) | 131.2 ± 30.7 | 100.1 ± 41.0 * | 79.5 ± 22.6 * | 0.001 2 |
| Vpeak (°/s) | 244.5 ± 57.2 | 188.8 ± 71.7 * | 148.7 ± 34.7 * | <0.001 2 |
| NVP (n) | 3.7 ± 2.8 | 9.0 ± 8.8 | 11.6 ± 10.5 | 0.014 1 |
| JPE | 4.2 ± 2.8 | 4.7 ± 2.8 * | 5.2 ± 5.2 * | 0.711 1 |
| Combined RoM | ||||
| Flexion/Extension | 52.6 ± 8.1 | 49.5 ± 7.9 | 42.9 ± 10.2 * | 0.041 |
| Right/Left Rotations | 71.5 ± 6.2 | 67.1 ± 9.4 | 62.1 ± 9.1 * | 0.042 |
| Groups | p-Value | |||
|---|---|---|---|---|
| Healthy Control (n = 15) | RNP (n = 22) | CNP (n = 8) | ||
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Normalized EMG amplitude (%) | ||||
| 20% | 18.8 ± 12.0 | 33.6 ± 22.6 | 52.0 ± 53.1 | 0.11 1 |
| 40% | 35.2 ± 23.9 | 64.3 ± 88.5 | 70.8 ± 36.5 | 0.07 1 |
| 60% | 50.9 ± 15.9 | 58.7 ± 29.0 | 111.8 ± 80.1 *,† | 0.003 |
| 80% | 66.9 ± 21.7 | 79.0 ± 33.6 | 108.6 ± 88.4 | 0.34 1 |
| Maximum craniocervical contraction | ||||
| CCF MVC (N) | 52.1 ± 22.3 | 44.0 ± 23.4 | 47.1 ± 22.8 | 0.57 |
| Groups | p-Value | |||
|---|---|---|---|---|
| Healthy Control (n = 15) | RNP (n = 22) | CNP (n = 8) | ||
| Mean ± SD | Mean ± SD | Mean ± SD | ||
| Maximal strength (MVC) | ||||
| Flexion MVC (kg) | 20.2 ± 9.7 | 14.6 ± 6.4 | 15.3 ± 3.1 | 0.17 1 |
| Extension MVC (kg) | 29.6 ± 18.5 | 15.3 ± 4.4 * | 21.6 ± 9.1 | 0.006 1 |
| Rate of perceived exertion (BORG scale: 6–20) | ||||
| Flexion Borg (6–20) | 12.0 ± 3.1 | 15.0 ± 3.0 * | 14.7 ± 1.7 | 0.01 |
| Extension Borg (6–20) | 8.9 ± 2.5 | 9.9 ± 2.5 | 10.4 ± 2.6 | 0.38 1 |
| NDI at 6 Months | Number of Days with Pain | |
|---|---|---|
| (Intercept) | 8.65 | 4.68 |
| NDI | 0 | 0 |
| TSK | 0 | 0 |
| EQ-VAS | 0 | 0 |
| EQ-5D | 0 | 0 |
| Previous number of pain episodes | 0.68 | 0.57 |
| Average of pain episodes | 0 | 0 |
| ROM in flexions and extension | 0 | 0 |
| ROM in rotations | 0 | 0 |
| NVP in flexions and extension | 0 | 0 |
| JPE | 0 | 0 |
| 20% and 40 of CCF MVC force | 0 | 0 |
| 60%, and 80% of CCF MVC force | 0 | 0 |
| CCF MVC | 0 | 0 |
| MVC during cervical flexion | −0.34 | 0 |
| MVC during cervical extension | 0 | 0 |
| β | SE | t Value | p Value | Low 95%CI | Upper 95% CI | Adjusted R2 | |
|---|---|---|---|---|---|---|---|
| (Intercept) | 10.23 | 2.99 | 3.42 | 0.004 | 3.82 | 16.63 | 0.43 |
| MVC flexion | −0.32 | 0.15 | −2.21 | 0.04 | −0.64 | −0.01 | |
| Previous number of pain episodes | 0.54 | 0.21 | 2.56 | 0.02 | 0.09 | 0.99 |
| β | SE | t Value | p Value | Low 95%CI | Upper 95% CI | Adjusted R2 | |
|---|---|---|---|---|---|---|---|
| (Intercept) | 2.14 | 1.17 | 1.83 | 0.08 | −0.33 | 4.61 | 0.25 |
| Previous number of pain episodes | 0.40 | 0.15 | 2.63 | 0.02 | 0.08 | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alalawi, A.; Devecchi, V.; Gallina, A.; Luque-Suarez, A.; Falla, D. Assessment of Neuromuscular and Psychological Function in People with Recurrent Neck Pain during a Period of Remission: Cross-Sectional and Longitudinal Analyses. J. Clin. Med. 2022, 11, 2042. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072042
Alalawi A, Devecchi V, Gallina A, Luque-Suarez A, Falla D. Assessment of Neuromuscular and Psychological Function in People with Recurrent Neck Pain during a Period of Remission: Cross-Sectional and Longitudinal Analyses. Journal of Clinical Medicine. 2022; 11(7):2042. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072042
Chicago/Turabian StyleAlalawi, Ahmed, Valter Devecchi, Alessio Gallina, Alejandro Luque-Suarez, and Deborah Falla. 2022. "Assessment of Neuromuscular and Psychological Function in People with Recurrent Neck Pain during a Period of Remission: Cross-Sectional and Longitudinal Analyses" Journal of Clinical Medicine 11, no. 7: 2042. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072042