First Case of Human Primary Vertebral Cystic Echinococcosis Due to Echinococcus Ortleppi

 , ,
, ,
Abstract
:1. Introduction
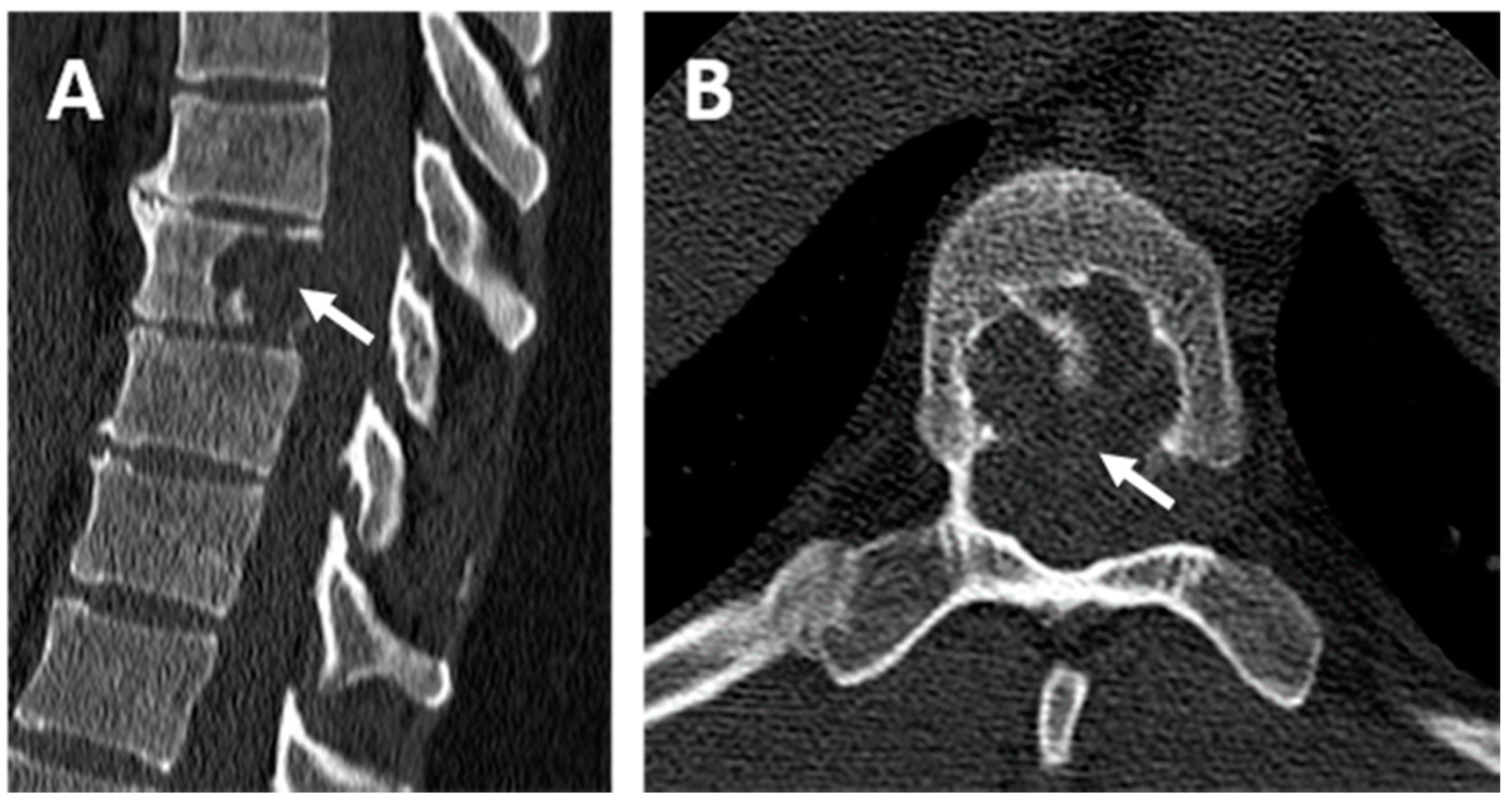
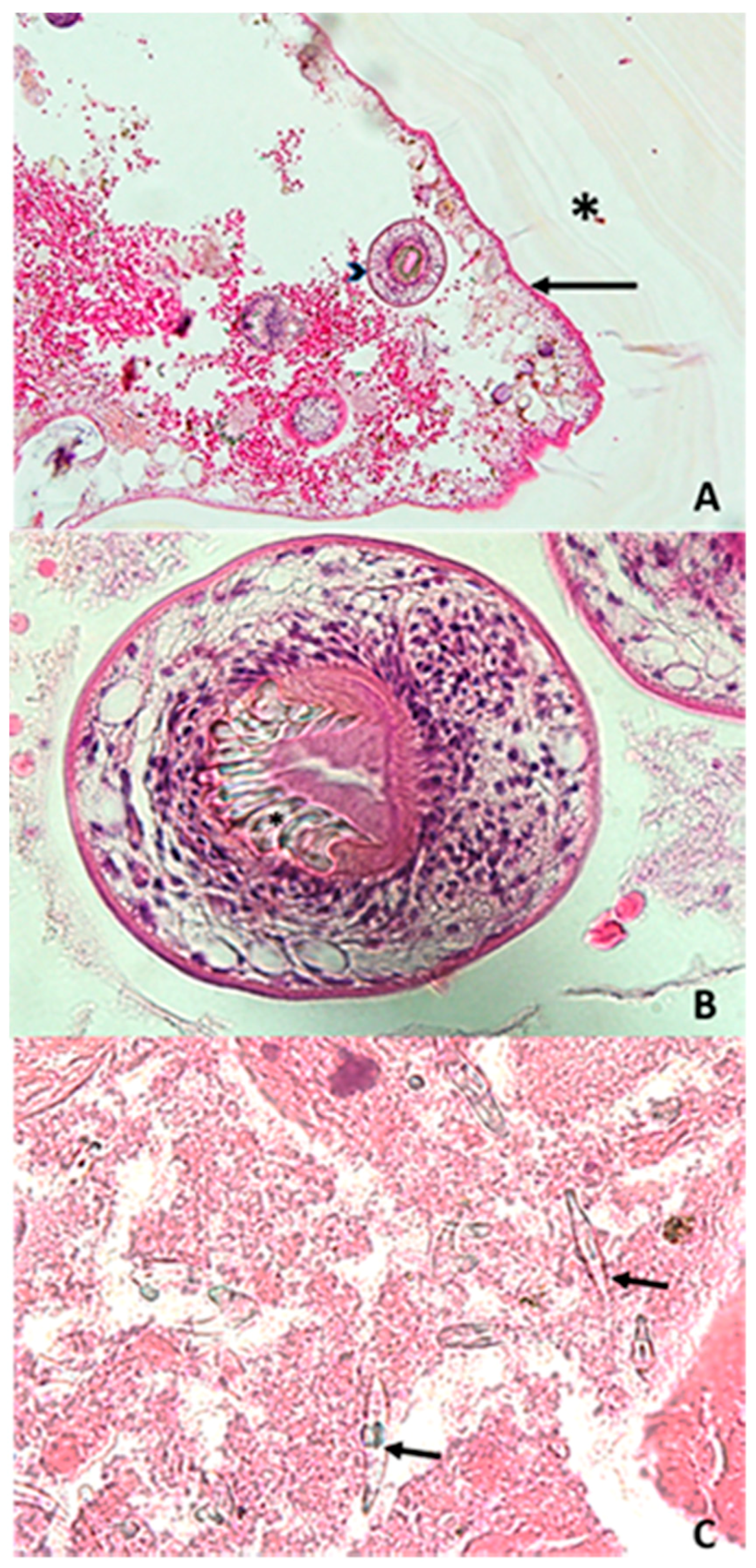
2. Case Report
3. Discussion and Conclusions
Author Contributions
Funding
Publication Ethic
Conflicts of Interest
Abbreviations
| CE | Cystic Echinococcosis |
| CT scan | Computed Tomography Scan |
| MRI | Magnetic Resonance Imaging |
| s.l. | Sensu Lato |
| s.s. | Sensu Stricto |
References
- Torgerson, P.R.; Devleesschauwer, B.; Praet, N.; Speybroeck, N.; Willingham, A.L.; Kasuga, F.; Rokni, M.B.; Zhou, X.N.; Fèvre, E.M.; Sripa, B.; et al. World Health Organization estimates of the global and regional disease burden of 11 foodborne parasitic diseases, 2010: A data synthesis. PLoS Med. 2015, 12, e1001920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, A.; Nakao, M.; Lavikainen, A.; Hoberg, E. Cystic echinococcosis: Future perspectives of molecular epidemiology. Acta Trop. 2017, 165 (Suppl. C), 3–9. [Google Scholar] [CrossRef] [PubMed]
- Alvarez Rojas, C.A.; Romig, T.; Lightowlers, M.W. Echinococcus granulosus sensu lato genotypes infecting humans—Review of current knowledge. Int. J. Parasitol. 2014, 44, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Romig, T.; Deplazes, P.; Jenkins, D.; Giraudoux, P.; Massolo, A.; Craig, P.S.; Wassermann, M.; Takahashi, K.; de la Rue, M. Ecology and Life Cycle Patterns of Echinococcus Species. Adv. Parasitol. 2017, 95, 213–314. [Google Scholar] [PubMed]
- Gottstein, B.; Soboslay, P.; Ortona, E.; Wang, J.; Siracusano, A.; Vuitton, D.A. Immunology of Alveolar and Cystic Echinococcosis (AE and CE). Adv. Parasitol. 2017, 96, 1–54. [Google Scholar] [PubMed]
- Eckert, J.; Thompson, R.C.A. Historical Aspects of Echinococcosis. Adv. Parasitol. 2017, 95, 1–64. [Google Scholar] [PubMed]
- Craig, P.S.; McManus, D.P.; Lightowlers, M.W.; Chabalgoity, J.A.; Garcia, H.H.; Gavidia, C.M.; Gilman, R.H.; Gonzalez, A.E.; Lorca, M.; Naquira, C.; et al. Prevention and control of cystic echinococcosis. Lancet Infect. Dis. 2007, 7, 385–394. [Google Scholar] [CrossRef]
- Campos-Bueno, A.; López-Abente, G.; Andrés-Cercadillo, A.M. Risk factors for Echinococcus granulosus infection: A case-control study. Am. J. Trop. Med. Hyg. 2000, 62, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Jacquier, M.; Piroth, L. Vertebral Hydatidosis. N. Engl. J. Med. 2018, 379, e5. [Google Scholar] [CrossRef] [PubMed]
- Baraquin, A.; Zait, H.; Grenouillet, F.E.; Moreau, E.; Hamrioui, B.; Grenouillet, F. Large-scale evaluation of a rapid diagnostic test for human cystic echinococcosis. Diagn. Microbiol. Infect. Dis. 2017, 89, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Georges, S.; Villard, O.; Filisetti, D.; Mathis, A.; Marcellin, L.; Hansmann, Y.; Candolfi, E. Usefulness of PCR Analysis for Diagnosis of Alveolar Echinococcosis with Unusual Localizations: Two Case Studies. J. Clin. Microbiol. 2004, 42, 5954–5956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanić, S.; Shaikenov, B.S.; Deplazes, P.; Dinkel, A.; Torgerson, P.R.; Mathis, A. Polymerase chain reaction for detection of patent infections of Echinococcus granulosus (“sheep strain”) in naturally infected dogs. Parasitol. Res. 2004, 92, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Roelfsema, J.H.; Nozari, N.; Pinelli, E.; Kortbeek, L.M. Novel PCRs for differential diagnosis of cestodes. Exp. Parasitol. 2016, 161, 20–26. [Google Scholar] [CrossRef] [PubMed]
- BLAST: Basic Local Alignment Search Tool. Available online: https://blast-ncbi-nlm-nih-gov.gate2.inist.fr/Blast.cgi (accessed on 3 October 2017).
- van Cauteren, D.; Millon, L.; de Valk, H.; Grenouillet, F. Retrospective study of human cystic echinococcosis over the past decade in France, using a nationwide hospital medical information database. Parasitol. Res. 2016, 115, 4261–4265. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Prasad, G.; Rustagi, T.; Bhojraj, S.Y. Hydatid disease of spine: Multiple meticulous surgeries and a long term followup. Indian J. Orthop. 2014, 48, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Grenouillet, F.; Umhang, G.; Arbez-Gindre, F.; Mantion, G.; Delabrousse, E.; Millon, L.; Boué, F. Echinococcus ortleppi Infections in Humans and Cattle, France. Emerg. Infect. Dis. 2014, 20, 2100. [Google Scholar] [CrossRef] [PubMed]
- Mogoye, B.K.; Menezes, C.N.; Wong, M.L.; Stacey, S.; von Delft, D.; Wahlers, K.; Wassermann, M.; Romig, T.; Kern, P.; Grobusch, M.P.; et al. First insights into species and genotypes of Echinococcus in South Africa. Vet. Parasitol. 2013, 196, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Sehgal, R.; Fomda, B.A.; Malhotra, A.; Malla, N. Molecular Characterization of Echinococcus granulosus Cysts in North Indian Patients: Identification of G1, G3, G5 and G6 Genotypes. PLoS Negl. Trop. Dis. 2013, 7, e2262. [Google Scholar] [CrossRef] [PubMed]
- Kamenetzky, L.; Gutierrez, A.M.; Canova, S.G.; Haag, K.L.; Guarnera, E.A.; Parra, A.; García, G.E.; Rosenzvit, M.C. Several strains of Echinococcus granulosus infect livestock and humans in Argentina. Infect. Genet. Evol. 2002, 2, 129–136. [Google Scholar] [CrossRef]
- Maravilla, P.; Andrew Thompson, R.C.; Palacios-Ruiz, J.A.; Estcourt, A.; Ramirez-Solis, E.; Mondragon-de-la-Peña, C.; Moreno-Moller, M.; Cardenas-Mejia, A.; Mata-Miranda, P.; Aguirre-Alcantara, M.T.; et al. Echinococcus granulosus cattle strain identification in an autochthonous case of cystic echinococcosis in central Mexico. Acta Trop. 2004, 92, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Bowles, J.; Knapen, F.; Mcmanus, D. Cattle strain of Echinococcus granulosus and human infection. Lancet 1992, 339, 1358. [Google Scholar] [CrossRef]
- de la Rue, M.L.; Takano, K.; Brochado, J.F.; Costa, C.V.; Soares, A.G.; Yamano, K.; Yagi, K.; Katoh, Y.; Takahashi, K. Infection of humans and animals with Echinococcus granulosus (G1 and G3 strains) and E. ortleppi in Southern Brazil. Vet. Parasitol. 2011, 177, 97–103. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Years | Age (Years) | Sex | Country (Region) | Clinical Statement | Cyst Localization | References |
|---|---|---|---|---|---|---|
| 2011 | 63 | M | Eastern France (Jura) | Moderate pain in right hypochondrium | Liver | [17] |
| 2012 | 39 | F | Western France (Vendée) | Abdominal pain, fever | Liver | [17] |
| 2010–2012 | * | * | South Africa (Ganteng Province) | * | Liver | [18] |
| 2011–2012 | * | M | North India (Uttarakhand) | * | Liver | [19] |
| 2002 | * | * | Argentina | * | Liver | [20] |
| 2004 | 38 | F | Central Mexico | Intense pain in right hypochondrium | Liver | [21] |
| 1984 | 11 | M | Netherlands | * | Spleen | [22] |
| * | * | * | Brazil (Santana do Livramento) | * | * | [23] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basmaciyan, L.; Burlet, B.; Ramla, S.; Blot, M.; Mahy, S.; Aubriot-Lorton, M.-H.; Valot, S.; Grelat, M.; Sautour, M.; Grenouillet, F.; et al. First Case of Human Primary Vertebral Cystic Echinococcosis Due to Echinococcus Ortleppi. J. Clin. Med. 2018, 7, 443. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110443
Basmaciyan L, Burlet B, Ramla S, Blot M, Mahy S, Aubriot-Lorton M-H, Valot S, Grelat M, Sautour M, Grenouillet F, et al. First Case of Human Primary Vertebral Cystic Echinococcosis Due to Echinococcus Ortleppi. Journal of Clinical Medicine. 2018; 7(11):443. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110443
Chicago/Turabian StyleBasmaciyan, Louise, Bénédicte Burlet, Selim Ramla, Mathieu Blot, Sophie Mahy, Marie-Hélène Aubriot-Lorton, Stéphane Valot, Mickael Grelat, Marc Sautour, Frederic Grenouillet, and et al. 2018. "First Case of Human Primary Vertebral Cystic Echinococcosis Due to Echinococcus Ortleppi" Journal of Clinical Medicine 7, no. 11: 443. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110443