Effect of Methotrexate in the Treatment of Distal Interphalangeal Joint Extensor Tendon Enthesopathy in Patients with Nail Psoriasis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Wilson, F.C.; Icen, M.; Crowson, C.S.; McEvoy, M.T.; Gabriel, S.E.; Kremers, H.M. Incidence and clinical predictors of psoriatic arthritis in patients with psoriasis: A population-based study. Arthritis Rheum. 2009, 61, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Williamson, L.; Dalbeth, N.; Dockerty, J.L.; Gee, B.C.; Weatherall, R.; Wordsworth, B.P. Extended report: Nail disease in psoriatic arthritis—Clinically important, potentially treatable and often overlooked. Rheumatology (Oxford) 2004, 43, 790–794. [Google Scholar] [CrossRef]
- McGonagle, D. Enthesitis: An autoinflammatory lesion linking nail and joint involvement in psoriatic disease. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 9–13. [Google Scholar] [CrossRef]
- McGonagle, D.; Tan, A.L.; Benjamin, M. The nail as a musculoskeletal appendage–implications for an improved understanding of the link between psoriasis and arthritis. Dermatology 2009, 218, 97–102. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Ash, Z.R.; Tinazzi, I.; Castillo-Gallego, C.; Kwok, C.; Wilson, C.; Goodfield, M.; Gisondi, P.; Tan, A.L.; Marzo-Ortega, H.; et al. The link between enthesitis and arthritis in psoriatic arthritis: A switch to a vascular phenotype at insertions may play a role in arthritis development. Ann. Rheum. Dis. 2013, 72, 992–995. [Google Scholar] [CrossRef]
- Benjamin, M.; McGonagle, D. The enthesis organ concept and its relevance to the spondyloarthropathies. Adv. Exp. Med. Biol. 2009, 649, 57–70. [Google Scholar]
- Rich, P.; Scher, R.K. Nail Psoriasis Severity Index: A useful tool for evaluation of nail psoriasis. J. Am. Acad. Dermatol. 2003, 49, 206–212. [Google Scholar] [CrossRef]
- Cassell, S.E.; Bieber, J.D.; Rich, P.; Tutuncu, Z.N.; Lee, S.J.; Kalunian, K.C.; Wu, C.W.; Kavanaugh, A. The modified Nail Psoriasis Severity Index: Validation of an instrument to assess psoriatic nail involvement in patients with psoriatic arthritis. J. Rheumatol. 2007, 34, 123–129. [Google Scholar]
- Bandinelli, F.; Prignano, F.; Bonciani, D.; Bartoli, F.; Collaku, L.; Candelieri, A.; Lotti, T.; Matucci-Cerinic, M. Ultrasound detects occult entheseal involvement in early psoriatic arthritis independently of clinical features and psoriasis severity. Clin. Exp. Rheumatol. 2013, 31, 219–224. [Google Scholar]
- Soscia, E.; Scarpa, R.; Cimmino, M.A.; Atteno, M.; Peluso, R.; Sirignano, C.; Costa, L.; Iervolino, S.; Caso, F.; del Puente, A.; et al. Magnetic resonance imaging of nail unit in psoriatic arthritis. J. Rheumatol. Suppl. 2009, 83, 42–45. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Ash, Z.; del Galdo, F.; Marzo-Ortega, H.; Wakefield, R.J.; Emery, P.; McGonagle, D. Optical coherence tomography: A new tool to assess nail disease in psoriasis? Dermatology 2011, 222, 311–313. [Google Scholar] [CrossRef]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H.; CASPAR Study Group. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum. 2006, 54, 2665–2673. [Google Scholar] [CrossRef]
- Feldman, S.R.; Clark, A.R.; Venkat, A.P.; Fleischer, A.B.; Anderson, R.T.; Rajagopalan, R. The Self-Administered Psoriasis Area and Severity Index provides an objective measure of psoriasis severity. Br. J. Dermatol. 2005, 152, 382–383. [Google Scholar] [CrossRef]
- Praevoo, M.L.; van’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight-joint counts. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar] [CrossRef]
- Wortsman, X.; Gutie´rrez, M.; Saavedra, T.; Honeyman, J. The role of ultrasound in rheumatic skin and nail lesions: A multi-specialist approach. Clin. Rheumatol. 2011, 30, 739–748. [Google Scholar] [CrossRef]
- Wakefield, R.J.; Balint, P.V.; Szkudlarek, M.; Filippucci, E.; Backhaus, M.; D’Agostino, M.A.; Sanchez, E.N.; Iagnocco, A.; Schmidt, W.A.; Bruyn, G.A.; et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J. Rheumatol. 2005, 32, 2485–2487. [Google Scholar]
- Scarpa, R.; Soscia, E.; Peluso, R.; Atteno, M.; Manguso, F.; del Puente, A.; Spanò, A.; Sirignano, C.; Oriente, A.; Di Minno, M.N.; et al. Nail and distal interphalangeal joint in psoriatic arthritis. J. Rheumatol. 2006, 33, 1315–1319. [Google Scholar]
- Ash, Z.R.; Tinazzi, I.; Gallego, C.C.; Kwok, C.; Wilson, C.; Goodfield, M.; Gisondi, P.; Tan, A.L.; Marzo-Ortega, H.; Emery, P.; et al. Psoriasis patients with nail disease have a greater magnitude of underlying systemic subclinical enthesopathy than those with normal nails. Ann. Rheum. Dis. 2012, 71, 553–556. [Google Scholar] [CrossRef]
- Acosta-Felquer, M.L.; Ruta, S.; Rosa, J.; Marin, J.; Ferreyra-Garrot, L.; Galimberti, M.L.; Galimberti, R.; Garcia-Monaco, R.; Soriano, E.R. Ultrasound entheseal abnormalities at the distal interphalangeal joints and clinical nail involvement in patients with psoriasis and psoriatic arthritis, supporting the nail-enthesitis theory. Semin. Arthritis Rheum. 2017, 47, 338–342. [Google Scholar] [CrossRef]
- Sandobal, C.; Carbó, E.; Iribas, J.; Roverano, S.; Paira, S. Ultrasound nail imaging on patients with psoriasis and psoriatic arthritis compared with rheumatoid arthritis and control subjects. J. Clin. Rheumatol. 2014, 20, 21–24. [Google Scholar] [CrossRef]
- Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A.; Placek, W.; Wojtkiewicz, M.; Wiktorowicz, A.; Wojtkiewicz, J. Ultrasound Assessment of Changes in Nails in Psoriasis and Psoriatic Arthritis. Biomed. Res. Int. 2018. [Google Scholar] [CrossRef]
- Castellanos-González, M.; Joven, B.E.; Sánchez, J.; Andrés-Esteban, E.M.; Vanaclocha-Sebastián, F.; Romero, P.O.; Díaz, R.R. Nail involvement can predict enthesopathy in patients with psoriasis. J. Dtsch. Dermatol. Ges. 2016, 14, 1102–1107. [Google Scholar] [CrossRef]
- Gutierrez, M.; Filippucci, E.; de Angelis, R.; Salaffi, F.; Filosa, G.; Ruta, S.; Bertolazzi, C.; Grassi, W. Subclinical entheseal involvement in patients with psoriasis: An ultrasound study. Semin. Arthritis Rheum. 2011, 40, 407–412. [Google Scholar] [CrossRef]
- Naredo, E.; Moller, I.; de Miguel, E.; Batlle-Gualda, E.; Acebes, C.; Brito, E.; Mayordomo, L.; Moragues, C.; Uson, J.; de Agustín, J.J.; et al. High prevalence of ultrasonographic synovitis and enthesopathy in patients with psoriasis without psoriatic arthritis: A prospective case-control study. Rheumatology (Oxford) 2011, 50, 1838–1848. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Castillo-Gallego, C.; Ash, Z.R.; Marzo-Ortega, H.; Emery, P.; Wakefield, R.J.; Wittmann, M.; McGonagle, D. Ultrasonographic assessment of nail in psoriatic disease shows a link between onychopathy and distal interphalangeal joint extensor tendon enthesopathy. Dermatology 2012, 225, 231–235. [Google Scholar] [CrossRef]
- Merola, J.S.; Espinoza, L.R.; Fleischmann, R. Distinguishing rheumatoid arthritis from psoriatic arthritis. RMD Open 2018, 4. [Google Scholar] [CrossRef]
- Watad, A.; Cuthbert, R.J.; Howard Amital, H.; McGonagle, D. Enthesitis: Much More Than Focal Insertion Point Inflammation. Curr. Rheumatol. Rep. 2018, 20, 41. [Google Scholar] [CrossRef]
- Mokni, S.; Ameur, K.; Ghariani, N.; Sriha, B.; Belajouza, C.; Denguezli, M.; Nouira, R. A Case of Nail Psoriasis Successfully Treated with Intralesional Methotrexate. Dermatol. Ther. (Heidelb.) 2018. [Google Scholar] [CrossRef]
- Daulatabad, D.; Grover, C.; Singal, A. Role of nail bed methotrexate injections in isolated nail psoriasis: Conventional drug via an unconventional route. Clin. Exp. Dermatol. 2017. [Google Scholar] [CrossRef]
- Mittal, J.; Mahajan, B.B. Intramatricial injections for nail psoriasis: An open-label comparative study of triamcinolone, methotrexate, and cyclosporine. Indian J. Dermatol. Venereol. Leprol. 2018, 84, 419–423. [Google Scholar] [CrossRef]
- Gümüşel, M.; Özdemir, M.; Mevlitoğlu, İ.; Bodur, S. Evaluation of the efficacy of methotrexate and cyclosporine therapies on psoriatic nails: A one-blind, randomized study. J. Eur. Acad. Dermatol. Venereol. 2010, 25, 1080–1084. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y. Severe 20-nail psoriasis successfully treated by low dose methotrexate. Dermatol. Online J. 2009, 15, 8. [Google Scholar] [PubMed]
- Litinsky, I.; Balbir-Gurman, A.; Wollman, J.; Arad, U.; Paran, D.; Caspi, D.; Elkayam, O. Ultrasound assessment of enthesis thickening in psoriatic arthritis patients treated with adalimumab compared to methotrexate. Clin. Rheumatol. 2016, 35, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Acquitter, M.; Misery, L.; Saraux, A.; Bressollette, L.; Jousse-Joulin, S. Detection of subclinical ultrasound enthesopathy and nail disease in patients at risk of psoriatic arthritis. Jt. Bone Spine 2017, 84, 703–707. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ps (n = 19) | PsA (n = 13) | p | |
|---|---|---|---|
| male/female (number) | 8/11 | 6/7 | |
| Age (years) | 45.6 ± 9.6 | 46.1 ± 8.8 | 0.307 |
| Ps duration (years) | 15.1 ± 10.3 | 16.3 ± 6.6 | 0.631 |
| PsA duration (years) | - | 6.9 ± 7.5 | - |
| DAS 28 | - | 3.3 ± 0.5 | - |
| PASI | 6.1 ± 3.6 | 5.6 ± 3.8 | 0.087 |
| mNAPSI | 21.1 ± 15.7 | 20.5 ± 16.1 | 0.154 |
| TJC | - | 2.6 ± 1.2 | - |
| SJC | - | 2.0 ± 0.4 | - |
| CRP (mg/dL) | 2.7 ± 1.6 | 9.1 ± 3.5 | p < 0.001 |
| ESR | 11.6 ± 4.6 | 23.5 ± 8.3 | p < 0.001 |
| Wortsman Classification | Ps (n = 174) | PsA (n = 100) |
|---|---|---|
| I | 144 | 15 |
| II | 10 | 74 |
| III | 7 | 9 |
| IV | - | 2 |
| Ps n/n of Fingers Studied (%) | PsA n/n of Fingers Studied (%) | p | |
|---|---|---|---|
| Enthesopathies | 124/190 (65%) | 94/129 (72%) | 0.014 |
| Enthesopathies in fingers with Ps nails | 118/174 (68%) | 89/100 (89%) | <0.001 |
| Enthesopathies in fingers with no Ps changes | 6/16 (37%) | 16/29 (55%) | 0.006 |
| Increased PD signal | 118/190 (62%) | 90/129 (70%) | 0.021 |
| Increased PD signal in fingers with Ps nails | 110/174 (63%) | 83/100 (83%) | <0.001 |
| Increased PD signal in fingers with no Ps changes | 7/16 (43%) | 17/29 (28%) | 0.018 |
| Ps (190/319) Initial | Ps (190/319) after 6 Months of Mtx Treatment | p | |
|---|---|---|---|
| NP thickness (mm) | 0.74 ± 0.04 | 0.73 ± 0.04 | 0.004 |
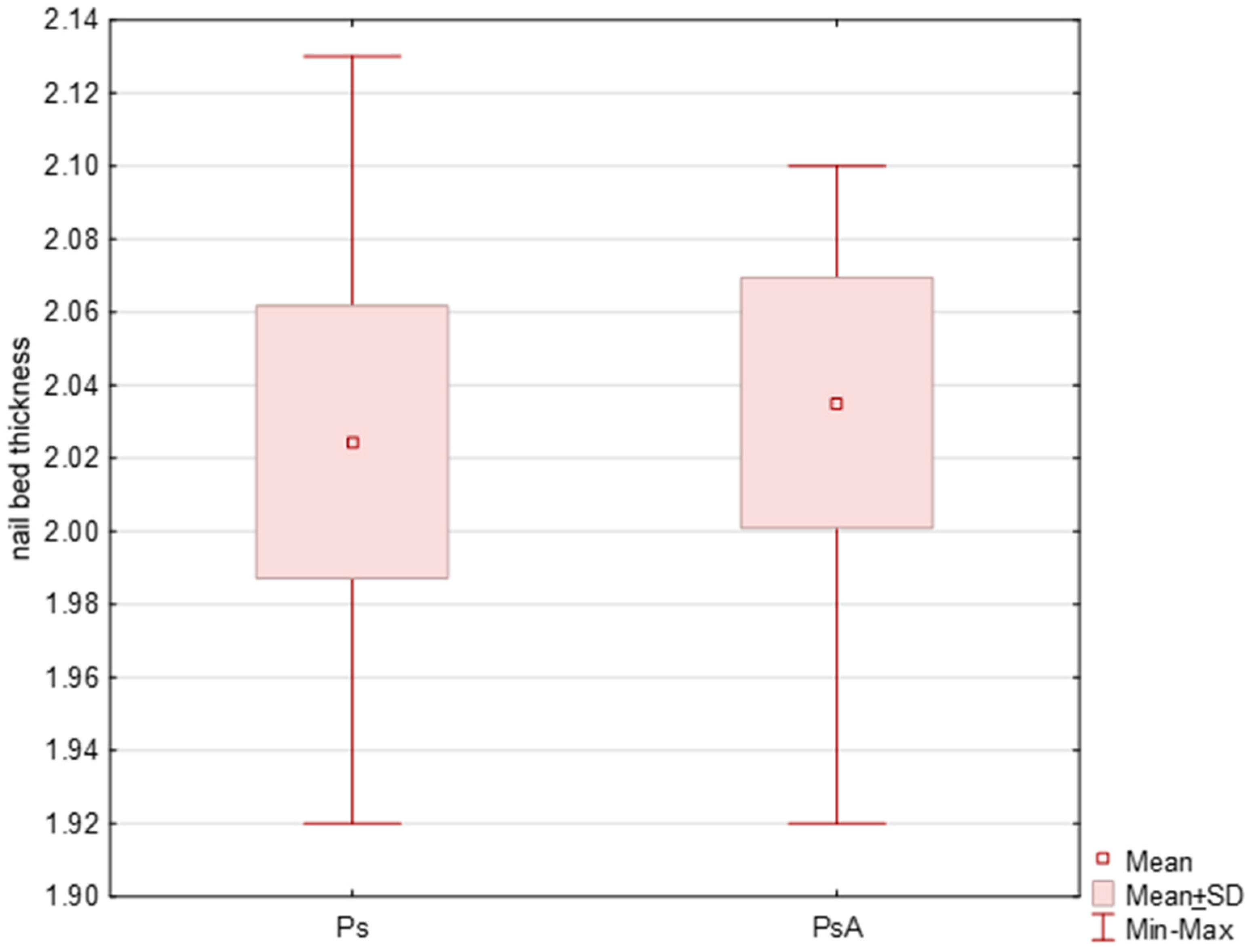
| NB thickness (mm) | 2.02 ± 0.03 | 2.0 ± 0.05 | <0.001 |
| Matrix thickness (mm) | 1.93 ± 0.02 | 1.93 ± 0.03 | <0.001 |
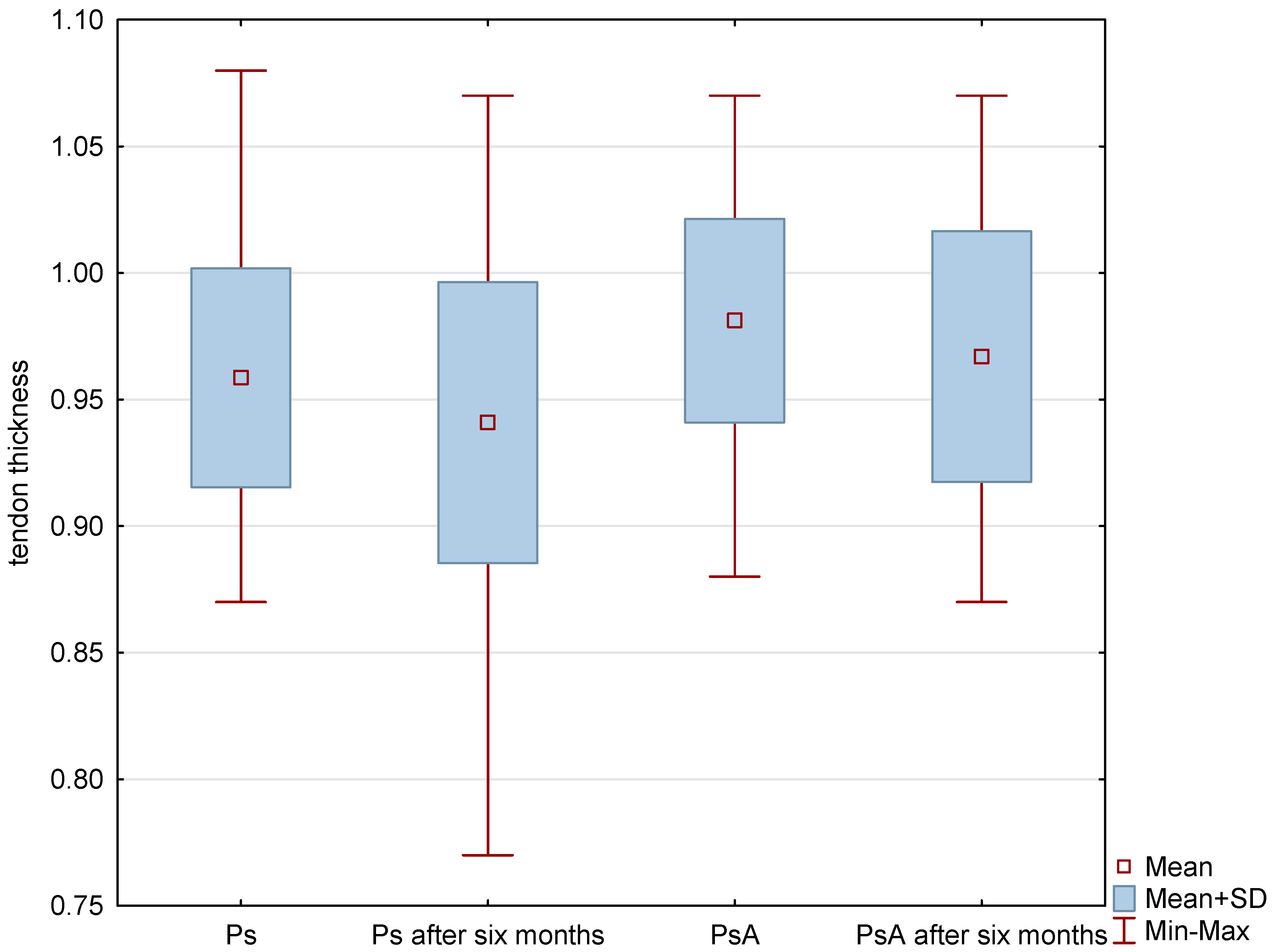
| Tendon thickness (mm) | 0.96 ± 0.04 | 0.94 ± 0.05 | <0.001 |
| PsA (129/319) Initial | PsA (129/319) after 6 Months of Mtx Treatment | p | |
|---|---|---|---|
| NP thickness (mm) | 0.75 ± 0.05 | 0.74 ± 0.05 | 0.002 |
| NB thickness (mm) | 2.04 ± 0.03 | 2.01 ± 0.06 | <0.001 |
| Matrix thickness (mm) | 1.93 ± 0.01 | 1.93 ± 0.01 | 0.002 |
| Tendon thickness (mm) | 0.98 ± 0.04 | 0.97 ± 0.05 | 0.061 |
| NB Thickness (At the Beginning of the Study) | Matrix Thickness (At the Beginning of the Study) | Ps Duration | CRP (At the Beginning of the Study) | Adjusted R2 | |
|---|---|---|---|---|---|
| Ps (fingers, n = 190) | 0.4722 (0.0000) | 0.4410 (0.001) | 0.3921 (0.015) | 0.3641 (0.017) | 0.386 |
| PsA Duration | TJC (At the Beginning of the Study) | SJC (At the Beginning of the Study) | Adjusted R2 | |
|---|---|---|---|---|
| PsA (fingers, n = 129) | 0.4648 (0.0000) | 0.4111 (0.0000) | 0.4003 (0.0000) | 0.317 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A.; Placek, W.; Wojtkiewicz, M.; Wojtkiewicz, J. Effect of Methotrexate in the Treatment of Distal Interphalangeal Joint Extensor Tendon Enthesopathy in Patients with Nail Psoriasis. J. Clin. Med. 2018, 7, 546. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7120546
Krajewska-Włodarczyk M, Owczarczyk-Saczonek A, Placek W, Wojtkiewicz M, Wojtkiewicz J. Effect of Methotrexate in the Treatment of Distal Interphalangeal Joint Extensor Tendon Enthesopathy in Patients with Nail Psoriasis. Journal of Clinical Medicine. 2018; 7(12):546. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7120546
Chicago/Turabian StyleKrajewska-Włodarczyk, Magdalena, Agnieszka Owczarczyk-Saczonek, Waldemar Placek, Maja Wojtkiewicz, and Joanna Wojtkiewicz. 2018. "Effect of Methotrexate in the Treatment of Distal Interphalangeal Joint Extensor Tendon Enthesopathy in Patients with Nail Psoriasis" Journal of Clinical Medicine 7, no. 12: 546. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7120546