The Emerging Role of Robotic Surgery among Minimally Invasive Surgical Approaches in the Treatment of Hypopharyngeal Carcinoma: Systematic Review and Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
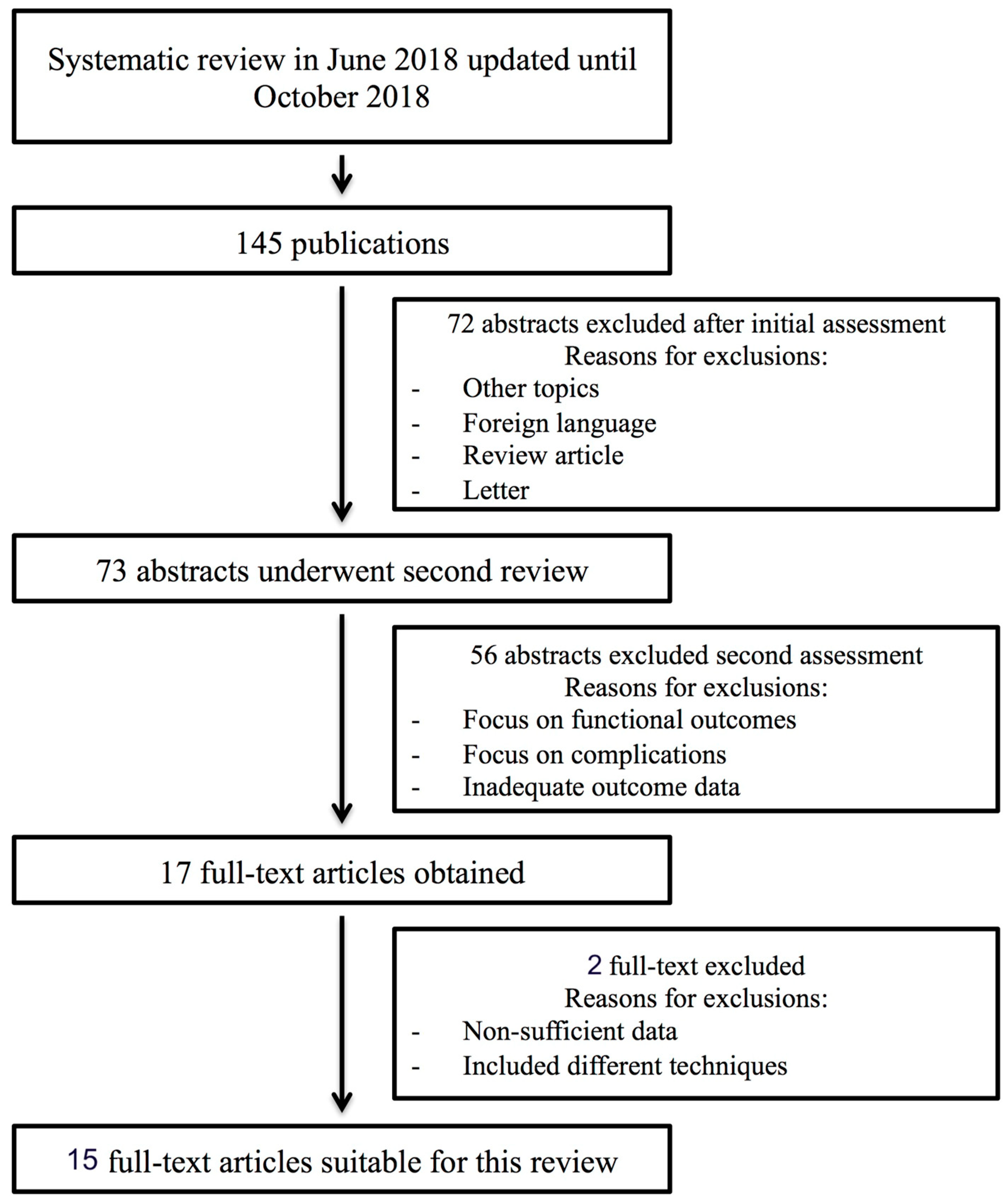
2. Materials and Methods
Data Extraction
3. Results
3.1. TORS Studies
3.2. TLM Studies
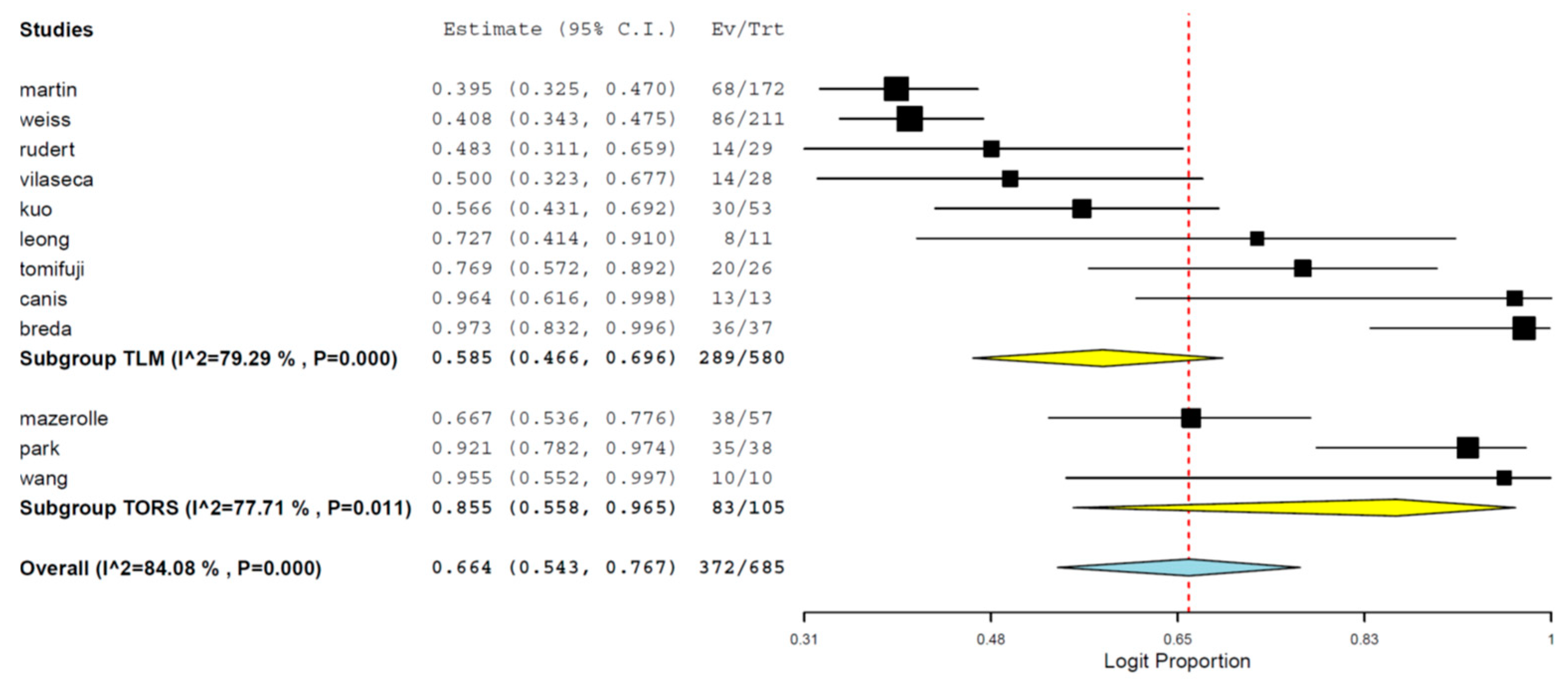
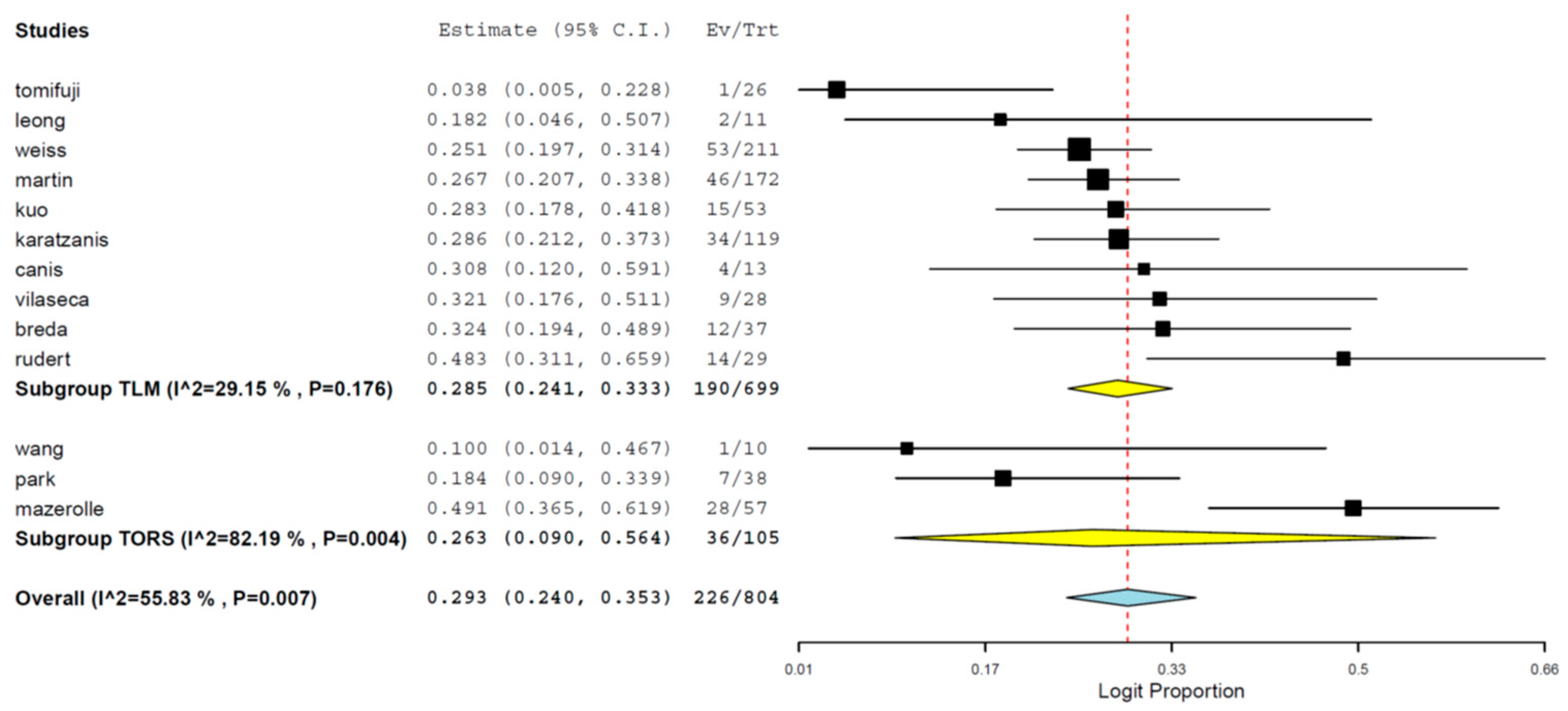
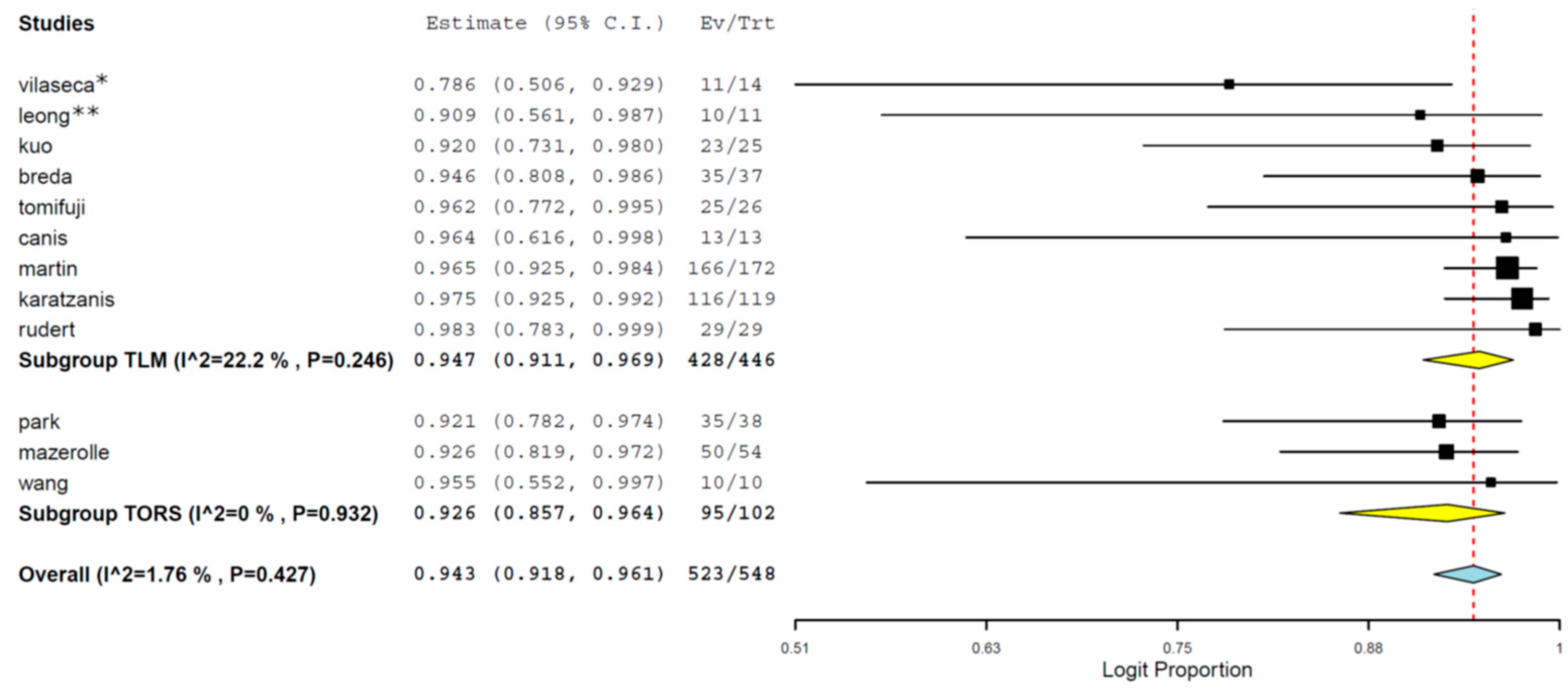
3.3. Cumulative Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Hoffman, H.T.; Karnell, L.H.; Shah, J.P.; Ariyan, S.; Brown, G.S.; Fee, W.E.; Glass, A.G.; Goepfert, H.; Ossoff, R.H.; Fremgen, A.M. Hypopharyngeal cancer patient care evaluation. Laryngoscope 1997, 107, 1005–1017. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.Y.W.; Wei, W.I. Current management strategy of hypopharyngeal carcinoma. Auris Nasus Larynx 2013, 40, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Kraus, D.H.; Zelefsky, M.J.; Brock, H.A.; Huo, J.; Harrison, L.B.; Shah, J.P. Combined surgery and radiation therapy for squamous cell carcinoma of the hypopharynx. Otolaryngol. Head Neck Surg. 1997, 116, 637–641. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Strong, M.S.; Jako, G.J. Laser surgery in the larynx. Early clinical experience with continuous CO2 laser. Ann. Otol. Rhinol. Laryngol. 1972, 81, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Steiner, W. Results of curative laser microsurgery of laryngeal carcinomas. Am. J. Otolaryngol. 1993, 14, 116–121. [Google Scholar] [CrossRef]
- Weinstein, G.S.; O’Malley, B.W., Jr.; Hockstein, N.G. Transoral robotic surgery: Supraglottic laryngectomy in a canine model. Laryngoscope 2005, 115, 1315–1319. [Google Scholar] [CrossRef] [PubMed]
- Mazerolle, P.; Philouze, P.; Garrel, R.; Aubry, K.; Morinière, S.; El Bedoui, S.; Ton Van, J.; Ferron, C.; Malard, O.; Jegoux, F.; et al. Oncological and functional outcomes of trans-oral robotic surgery for pyriform sinus carcinoma: A French GETTEC group study. Oral Oncol. 2018, 86, 165–170. [Google Scholar] [CrossRef]
- Park, Y.M.; Jung, C.M.; Cha, D.; Kim, S.H. The long-term oncological and functional outcomes of transoral robotic surgery in patients with hypopharyngeal cancer. Oral Oncol. 2017, 71, 138–143. [Google Scholar] [CrossRef]
- Weiss, B.G.; Ihler, F.; Wolff, H.A.; Schneider, S.; Canis, M.; Steiner, W.; Welz, C. Transoral laser microsurgery for treatment for hypopharyngeal cancer in 211 patients. Head Neck 2017, 39, 1631–1638. [Google Scholar] [CrossRef]
- Breda, E.; Catarino, R.; Monteiro, E. Transoral laser microsurgery as standard approach to hypopharyngeal cancer. Survival analysis in a hospital based population. Acta Otorrinolaringol. Esp. 2018, 69, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Liu, S.A.; Wu, S.H.; Wang, C.P.; Liang, K.L.; Jiang, R.S.; Lin, J.C. Transoral robotic surgery for early T classification hypopharyngeal cancer. Head Neck 2016, 38, 857–862. [Google Scholar] [CrossRef]
- Canis, M.; Wolff, H.A.; Ihler, F.; Matthias, C.; Steiner, W. Oncologic results of transoral laser microsurgery for squamous cell carcinoma of the posterior pharyngeal wall. Head Neck 2015, 37, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Durmus, K.; Kucur, C.; Uysal, I.O.; Dziegielewski, P.T.; Ozer, E. Feasibility and clinical outcomes of transoral robotic surgery and transoral robot-assisted carbon dioxide laser for hypopharyngeal carcinoma. J. Craniofac. Surg. 2015, 26, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Lörincz, B.B.; Busch, C.J.; Möckelmann, N.; Knecht, R. Feasibility and safety of transoral robotic surgery (TORS) for early hypopharyngeal cancer: A subset analysis of the Hamburg University TORS-trial. Eur. Arch. Otorhinolaryngol. 2015, 272, 2993–2998. [Google Scholar] [CrossRef] [PubMed]
- Tomifuji, M.; Araki, K.; Yamashita, T.; Shiotani, A. Transoral videolaryngoscopic surgery for oropharyngeal, hypopharyngeal, and supraglottic cancer. Eur. Arch. Otorhinolaryngol. 2014, 271, 589–597. [Google Scholar] [CrossRef]
- Kuo, C.L.; Lee, T.L.; Chu, P.Y. Conservation surgery for hypopharyngeal cancer: Changing paradigm from open to endoscopic. Acta Otolaryngol. 2013, 133, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Karatzanis, A.D.; Psychogios, G.; Waldfahrer, F.; Zenk, J.; Hornung, J.; Velegrakis, G.A.; Iro, H. T1 and T2 hypopharyngeal cancer treatment with laser microsurgery. Surg. Oncol. 2010, 102, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Leong, S.C.; Kathan, C.; Mortimore, S. Early outcomes after transoral CO2 laser resection of laryngeal and hypopharyngeal squamous cell carcinoma: One centre’s experience. J. Laryngol. Otol. 2010, 124, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Jackel, M.C.; Christiansen, H.; Mahmoodzada, M.; Kron, M.; Steiner, W. Organ-preserving transoral laser microsurgery for cancer of the hypopharynx. Laryngoscope 2008, 118, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Vilaseca, I.; Blanch, J.L.; Bernal-Sprekelsen, M.; Moragas, M. CO2 laser surgery: A larynx preservation alternative for selected hypopharyngeal carcinomas. Head Neck 2004, 26, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Rudert, H.H.; Höft, S. Transoral carbon-dioxide laser resection of hypopharyngeal carcinoma. Eur. Arch. Otorhinolaryngol. 2003, 260, 198–206. [Google Scholar] [PubMed]
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Axon, P.R.; Woolford, T.J.; Hargreaves, S.P.; Yates, P.; Birzgalis, A.R.; Farrington, W.T. A comparison of surgery and radiotherapy in the management of post-cricoid carcinoma. Clin. Otolaryngol. Allied Sci. 1997, 22, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.F.; Groome, P.A.; Irish, J.; O’Sullivan, B. Radiotherapy or surgery for head and neck squamous cell cancer: Establishing the baseline for hypopharyngeal carcinoma? Cancer 2009, 115, 5711–5722. [Google Scholar] [CrossRef] [PubMed]
- Beauvillain, C.; Mahé, M.; Bourdin, S.; Peuvrel, P.; Bergerot, P.; Rivière, A.; Vignoud, J.; Deraucourt, D.; Wesoluch, M. Final results of a randomized trial comparing chemotherapy plus radiotherapy with chemotherapy plus surgery plus radiotherapy in locally advanced resectable hypopharyngeal carcinomas. Laryngoscope 1997, 107, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Tsou, Y.A.; Lin, M.H.; Hua, C.H.; Tseng, H.C.; Chen, S.W.; Yang, S.N.; Liang, J.A.; Tsai, M.H. Survival outcome by early chemoradiation therapy salvage or early surgical salvage for the treatment of hypopharyngeal cancer. Otolaryngol. Head Neck Surg. 2007, 137, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Harris, B.N.; Biron, V.L.; Donald, P.; Farwell, D.G.; Luu, Q.C.; Bewley, A.F.; Chen, A.M.; Daly, M.E. Primary Surgery vs. Chemoradiation Treatment of Advanced-Stage Hypopharyngeal Squamous Cell Carcinoma. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, Y.; Omori, Y.; Saito, H.; Suzuki, S.; Matsuhashi, T.; Yamada, T. An investigation on endoscopic laryngopharyngeal surgery and related outcomes. Wideochir. Inne. Tech. Maloinwazyjne. 2018, 13, 394–400. [Google Scholar] [CrossRef]
- Park, Y.M.; Kim, W.S.; Byeon, H.K.; Lee, S.Y.; Kim, S.H. Oncological and functional outcomes of transoral robotic surgery for oropharyngeal cancer. Br. J. Oral Maxillofac. Surg. 2013, 51, 408–412. [Google Scholar] [CrossRef]
- Park, Y.M.; Kim, W.S.; De Virgilio, A.; Lee, S.Y.; Seol, J.H.; Kim, S.H. Transoral robotic surgery for hypopharyngeal squamous cell carcinoma: 3-year oncologic and functional analysis. Oral Oncol. 2012, 48, 560–566. [Google Scholar] [CrossRef] [PubMed]
- De Virgilio, A.; Park, Y.M.; Kim, W.S.; Baek, S.J.; Kim, S.H. How to optimize laryngeal and hypopharyngeal exposure in transoral robotic surgery. Auris Nasus Larynx 2013, 40, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.M.; De Virgilio, A.; Kim, W.S.; Chung, H.P.; Kim, S.H. Parapharyngeal space surgery via a transoral approach using a robotic surgical system: Transoral robotic surgery. J. Laparoendosc. Adv. Surg. Tech. A 2013, 23, 231–236. [Google Scholar] [CrossRef] [PubMed]
- De Virgilio, A.; Park, Y.M.; Kim, W.S.; Lee, S.Y.; Seol, J.H.; Kim, S.H. Robotic sialoadenectomy of the submandibular gland via a modified face-lift approach. Int. J. Oral Maxillofac. Surg. 2012, 41, 1325–1329. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Series | Technique | No. Pts | M/F | Age | Early/Advanced | OS 3 years | OS 5 years | DSS 3 years | DSS 5 years | LC 3 years | LC 5 years | DFS 3 years | Complications |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mazerolle et al. 2018 [8] | TORS | 57 | 52/5 | 60 | 56/1 | 84% | 66% | 5% (3) bleeding; 2% (1) pharyngeal fistula; 2% (1) neck hematoma | |||||
| Park et al. 2017 [9] | TORS | 38 | 66.7 | 22/16 | 100% I–II | 100% I–II | 97% | 100% I–II | 100% early | 5% (2) bleeding; 8% (3) aspiration pneumonia | |||
| 74% III–IV | 74% III–IV | 97% | 68.6% advanced | ||||||||||
| Weiss et al. 2017 [10] | TLM | 211 | 189/22 | 57.4 | 32/179 | 81.5% I–II | 68.2% I–II | 96.7% I–II | 96.7% I–II | 88.1% T1 | 10.4% (22) bleeding; 0.9% (2) pharyngeal fistula | ||
| 79% III | 65.9% III | 86% III | 83.8% III | 74.8% T2 | |||||||||
| 54% IV | 44.5% IV | 71% IV | 62% IV | 77.3% T3 | |||||||||
| 61.8% T4 | |||||||||||||
| Breda et al. 2017 [11] | TLM | 37 | 37/0 | 58.7 | 12/25 | 80.3% I–II | 63.5% I–II | 85.3% I–II | 74.1% I–II | 100% T1 | 2.7 aspiration pneumonia; 8.1% bleeding | ||
| 57.1% III | 39.5% III–IV | 85.7% III | 87.4%T2 | ||||||||||
| 53.1 IV | 39.8 IV | 59% IV | 100%T3 | ||||||||||
| 50%T4 | |||||||||||||
| Wang et al. 2016 [12] | TORS | 10 | 10/0 | 60 | 6/4 | 100% I–II | 100% I–II | 100% I–II | 100% I–II | 100% I–II | 100% T1 | 100% I–II | 0 |
| 50% III–IV | 50% III–IV | 100% III–IV | 100% III–IV | 100% III–IV | 100% T2 | 100% III–IV | |||||||
| Canis et al. 2015 [13] | TLM | 13 | 47.9% | 71.8% | 78.9% | 78.9% | 48.5% | ||||||
| Durmus et al. 2015 [14] | TORS | 5 | 4/1 | 59.8 | 3/2 | 0 | |||||||
| Lorincz et al. 2015 [15] | TORS | 5 | 4/1 | 63.4 | 4/1 | 100% I–II | 100% I–II | 100% I–II | 100% I–II | 100% I–II | 100% T1 | 100% I–II | 0 |
| 0% III–IV | 0% III–IV | 100% III–IV | 100% III–IV | 100% III–IV | 100% T2 | ||||||||
| Tomifuji et al. 2014 [16] | TOVS | 26 | 13/13 | 78% all | 96% all | 90% all | NOS | ||||||
| Kuo et al. 2013 [17] | TLM | 25 | 24/1 | 58 | 9/16 | 79% all | 67% all | 83% all | 76%all | 92% all | 13% (3) aspiration pneumonia; 4% (1) subcutaneous emphysema; 4% (1) local infection | ||
| Karatzanis et al. 2010 [18] | TLM | 119 | 107/12 | 55.4 | 47/72 | 84.4% I | 90% T1 | 90% T1 | 5% (6) bleeding; 4% (5) aspiration; 1% (1) fistula | ||||
| 77.1% II | 88% T2 | 83.1% T2 | |||||||||||
| 68.2% III | 85.4% all | ||||||||||||
| Leong et al. 2010 [19] | TLM | 12 | 2/9 | 71% | 71% | 71% | |||||||
| Martin et al. 2008 [20] | TLM | 172 | 153/19 | 57 | |||||||||
| Vilaseca et al. 2004 [21] | TLM | 28 | 27/1 | 56.6 | 6/22 | 100% I–II | 100% I–II | 100% | 100% T1 | 10.7% (3) aspiration pneumonia; 7.1% (2) bleeding; 3.5% (1) pharyngeal fistula | |||
| 45.2% III–IV | 45.2% III–IV | 91.6% | 91.6% T2 | ||||||||||
| 56.2% | 56.2% T3 | ||||||||||||
| 100% | 100% T4 | ||||||||||||
| Rudert et al. 2003 [22] | TLM | 29 | 24/5 | 53.1 | 9/20 | 62% | 48% | 70% | 58% | 87.5% T1 | 74% | 3.4% (1) bleeding | |
| 63.2% T2 | |||||||||||||
| 100%T3 | |||||||||||||
| 100% T4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Virgilio, A.; Iocca, O.; Malvezzi, L.; Di Maio, P.; Pellini, R.; Ferreli, F.; Cugini, G.; Colombo, G.; Spriano, G. The Emerging Role of Robotic Surgery among Minimally Invasive Surgical Approaches in the Treatment of Hypopharyngeal Carcinoma: Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 256. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020256
De Virgilio A, Iocca O, Malvezzi L, Di Maio P, Pellini R, Ferreli F, Cugini G, Colombo G, Spriano G. The Emerging Role of Robotic Surgery among Minimally Invasive Surgical Approaches in the Treatment of Hypopharyngeal Carcinoma: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(2):256. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020256
Chicago/Turabian StyleDe Virgilio, Armando, Oreste Iocca, Luca Malvezzi, Pasquale Di Maio, Raul Pellini, Fabio Ferreli, Giovanni Cugini, Giovanni Colombo, and Giuseppe Spriano. 2019. "The Emerging Role of Robotic Surgery among Minimally Invasive Surgical Approaches in the Treatment of Hypopharyngeal Carcinoma: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 2: 256. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020256