Expression of SLC5A5 in Circulating Tumor Cells May Distinguish Follicular Thyroid Carcinomas from Adenomas: Implications for Blood-Based Preoperative Diagnosis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients
2.2. Measurement of mRNA in Peripheral Blood
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
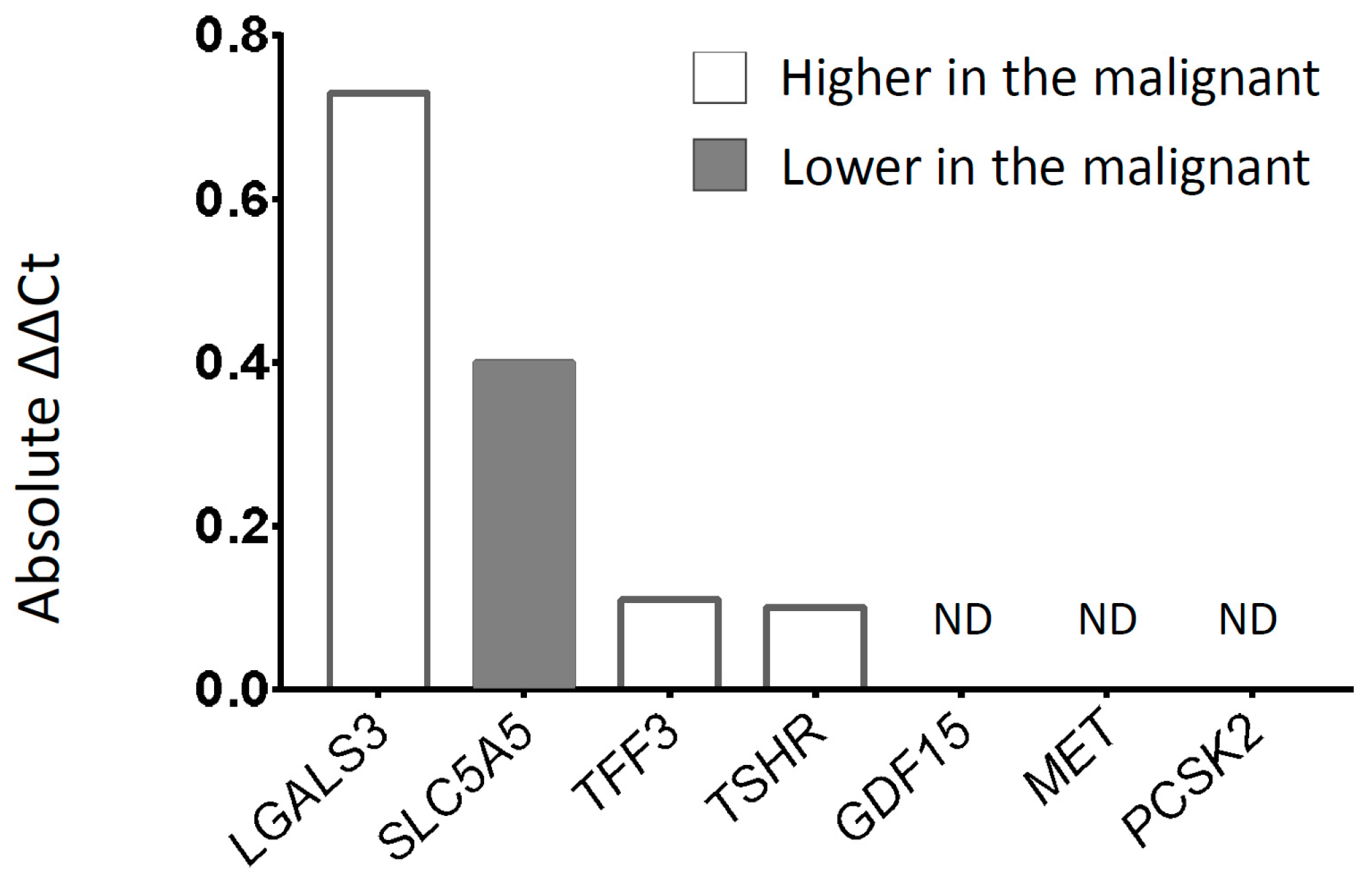
3.2. Discovery Phase Gene Screening
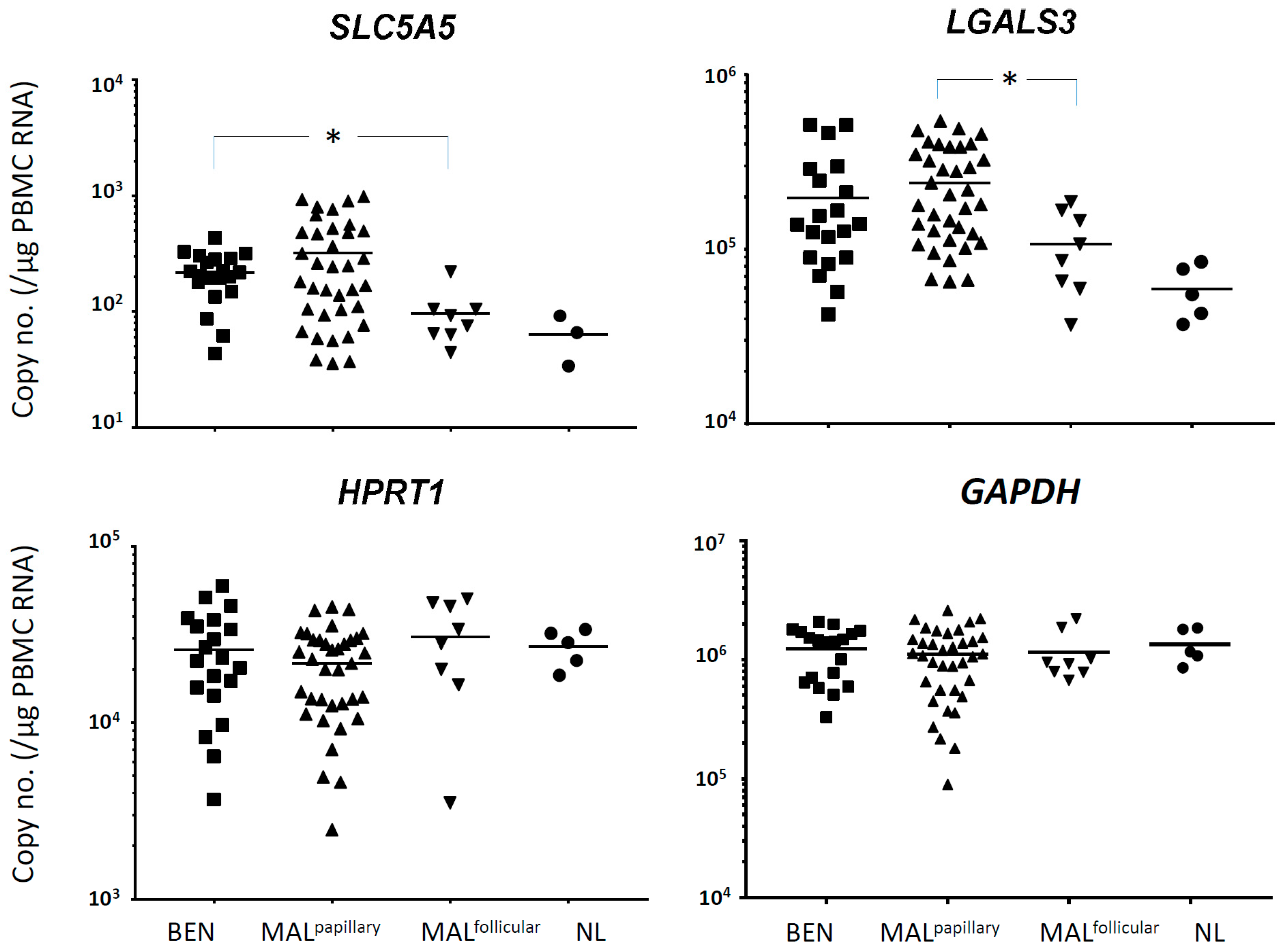
3.3. Validation in a Larger Number of Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vander, J.B.; Gaston, E.A.; Dawber, T.R. The significance of nontoxic thyroid nodules. Final report of a 15-year study of the incidence of thyroid malignancy. Ann. Intern. Med. 1968, 69, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Tunbridge, W.M.; Evered, D.C.; Hall, R.; Appleton, D.; Brewis, M.; Clark, F.; Evans, J.G.; Young, E.; Bird, T.; Smith, P.A. The spectrum of thyroid disease in a community: The Whickham survey. Clin. Endocrinol. 1977, 7, 481–493. [Google Scholar] [CrossRef]
- Tan, G.H.; Gharib, H. Thyroid incidentalomas: Management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann. Intern. Med. 1997, 126, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Guth, S.; Theune, U.; Aberle, J.; Galach, A.; Bamberger, C.M. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur. J. Clin. Investig. 2009, 39, 699–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharib, H. Changing trends in thyroid practice: Understanding nodular thyroid disease. Endocr. Pract. 2004, 10, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Hegedus, L. Clinical practice. The thyroid nodule. N. Engl. J. Med. 2004, 351, 1764–1771. [Google Scholar] [CrossRef]
- Haugen, B.R. 2015 American Thyroid Association Management Guidelines for adult patients with Thyroid nodules and differentiated thyroid cancer: What is new and what has changed? Cancer 2017, 123, 372–381. [Google Scholar] [CrossRef]
- Takano, T.; Miyauchi, A.; Yoshida, H.; Kuma, K.; Amino, N. Decreased relative expression level of trefoil factor 3 mRNA to galectin-3 mRNA distinguishes thyroid follicular carcinoma from adenoma. Cancer Lett. 2005, 219, 91–96. [Google Scholar] [CrossRef]
- Al-Hilli, Z.; Strajina, V.; McKenzie, T.J.; Thompson, G.B.; Farley, D.R.; Richards, M.L. The role of lateral neck ultrasound in detecting single or multiple lymph nodes in papillary thyroid cancer. Am. J. Surg. 2016, 212, 1147–1153. [Google Scholar] [CrossRef]
- Greaves, T.S.; Olvera, M.; Florentine, B.D.; Raza, A.S.; Cobb, C.J.; Tsao-Wei, D.D.; Groshen, S.; Singer, P.; Lopresti, J.; Martin, S.E. Follicular lesions of thyroid: A 5-year fine-needle aspiration experience. Cancer 2000, 90, 335–341. [Google Scholar] [CrossRef]
- Barzon, L.; Boscaro, M.; Pacenti, M.; Taccaliti, A.; Palu, G. Evaluation of circulating thyroid-specific transcripts as markers of thyroid cancer relapse. Int. J. Cancer 2004, 110, 914–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milas, M.; Shin, J.; Gupta, M.; Novosel, T.; Nasr, C.; Brainard, J.; Mitchell, J.; Berber, E.; Siperstein, A. Circulating thyrotropin receptor mRNA as a novel marker of thyroid cancer: Clinical applications learned from 1758 samples. Ann. Surg. 2010, 252, 643–651. [Google Scholar] [CrossRef]
- Gupta, M.K.; Taguba, L.; Arciaga, R.; Siperstein, A.; Faiman, C.; Mehta, A.; Reddy, S.S.K. Detection of circulating thyroid cancer cells by reverse transcription-PCR for thyroid-stimulating hormone receptor and thyroglobulin: The importance of primer selection. Clin. Chem. 2002, 48, 1862–1865. [Google Scholar] [CrossRef]
- Ausavarat, S.; Sriprapaporn, J.; Satayaban, B.; Thongnoppakhun, W.; Laipiriyakun, A.; Amornkitticharoen, B.; Chanachai, R.; Pattanachak, C. Circulating thyrotropin receptor messenger ribonucleic acid is not an effective marker in the follow-up of differentiated thyroid carcinoma. Thyroid. Res. 2015, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- RNA and Protein Expression Summary: GAPDH as an Example; The Human Protein Atlas: Stockholm, Sweden, 2018; Available online: https://www.proteinatlas.org/ENSG00000111640-GAPDH/tissue (accessed on 31 December 2018).
- Dent, B.M.; Ogle, L.F.; O’Donnell, R.L.; Hayes, N.; Malik, U.; Curtin, N.J.; Boddy, A.V.; Plummer, E.R.; Edmondson, R.J.; Reeves, H.L.; et al. High-resolution imaging for the detection and characterisation of circulating tumour cells from patients with oesophageal, hepatocellular, thyroid and ovarian cancers. Int. J. Cancer 2016, 138, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Shibru, D.; Hwang, J.; Khanafshar, E.; Duh, Q.Y.; Clark, O.H.; Kebebew, E. Does the 3-gene diagnostic assay accurately distinguish benign from malignant thyroid neoplasms? Cancer 2008, 113, 930–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takano, T.; Miyauchi, A.; Yokozawa, T.; Matsuzuka, F.; Liu, G.; Higashiyama, T.; Morita, S.; Kuma, K.; Amino, N. Accurate and objective preoperative diagnosis of thyroid papillary carcinomas by reverse transcription-PCR detection of oncofetal fibronectin messenger RNA in fine-needle aspiration biopsies. Cancer Res. 1998, 58, 4913–4917. [Google Scholar] [CrossRef] [PubMed]
- Siraj, A.K.; Bavi, P.; Abubaker, J.; Jehan, Z.; Sultana, M.; Al-Dayel, F.; Al-Nuaim, A.; Alzahrani, A.; Ahmed, M.; Al-Sanea, O.; et al. Genome-wide expression analysis of Middle Eastern papillary thyroid cancer reveals c-MET as a novel target for cancer therapy. J. Pathol. 2007, 213, 190–199. [Google Scholar] [CrossRef]
- Imaizumi, Y.; Murota, H.; Kanda, S.; Hishikawa, Y.; Koji, T.; Taguchi, T.; Tanaka, Y.; Yamada, Y.; Ikeda, S.; Kohno, T.; et al. Expression of the c-Met proto-oncogene and its possible involvement in liver invasion in adult T-cell leukemia. Clin. Cancer Res. 2003, 9, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Das, D.K.; Al-Waheeb, S.K.; George, S.S.; Haji, B.I.; Mallik, M.K. Contribution of immunocytochemical stainings for galectin-3, CD44, and HBME1 to fine-needle aspiration cytology diagnosis of papillary thyroid carcinoma. Diagn. Cytopathol. 2014, 42, 498–505. [Google Scholar] [CrossRef]
- Newlaczyl, A.U.; Yu, L.G. Galectin-3—A jack-of-all-trades in cancer. Cancer Lett. 2011, 313, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Abbas, A.K.; Fausto, N.; Robbins, S.L.; Cotran, R.S. Robbins and Cotran Pathologic Basis of Disease, 7th ed.; Elsevier Saunders: Philadelphia, PA, USA, 2005. [Google Scholar]
- Kim, M.J.; Kim, E.K.; Kim, B.M.; Kwak, J.Y.; Lee, E.J.; Park, C.S.; Cheong, W.Y.; Nam, K.H. Thyroglobulin measurement in fine-needle aspirate washouts: The criteria for neck node dissection for patients with thyroid cancer. Clin. Endocrinol. 2009, 70, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, Y.; Choi, J.W.; Kim, Y.S. The association between papillary thyroid carcinoma and histologically proven Hashimoto’s thyroiditis: A meta-analysis. Eur. J. Endocrinol. 2013, 168, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Osman, I.; Bajorin, D.F.; Sun, T.T.; Zhong, H.; Douglas, D.; Scattergood, J.; Zheng, R.; Han, M.; Marshall, K.W.; Liew, C.C. Novel blood biomarkers of human urinary bladder cancer. Clin. Cancer Res. 2006, 12, 3374–3380. [Google Scholar] [CrossRef] [PubMed]
- Kalinich, M.; Bhan, I.; Kwan, T.T.; Miyamoto, D.T.; Javaid, S.; LiCausi, J.A.; Milner, J.D.; Hong, X.; Goyal, L.; Sil, S.; et al. An RNA-based signature enables high specificity detection of circulating tumor cells in hepatocellular carcinoma. Proc. Natl. Acad. Sci. USA 2017, 114, 1123–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, M.; Li, X.; Zhang, S.; Song, H.; Zhang, W.; Shang, X.; Zheng, Y.; Jiang, H.; Lv, Q.; Jiang, Y.; et al. Real-time quantitative RT-PCR detection of circulating tumor cells from breast cancer patients. Int. J. Oncol. 2015, 46, 281–289. [Google Scholar] [CrossRef]
- Biscolla, R.P.; Cerutti, J.M.; Maciel, R.M. Detection of recurrent thyroid cancer by sensitive nested reverse transcription-polymerase chain reaction of thyroglobulin and sodium/iodide symporter messenger ribonucleic acid transcripts in peripheral blood. J. Clin. Endocrinol. Metab. 2000, 85, 3623–3627. [Google Scholar] [CrossRef]
- Lacroix, L.; Lazar, V.; Michiels, S.; Ripoche, H.; Dessen, P.; Talbot, M.; Caillou, B.; Levillain, J.P.; Schlumberger, M.; Bidart, J.M. Follicular thyroid tumors with the PAX8-PPARgamma1 rearrangement display characteristic genetic alterations. Am. J. Pathol. 2005, 167, 223–231. [Google Scholar] [CrossRef]
- Lazar, V.; Bidart, J.M.; Caillou, B.; Mahé, C.; Lacroix, L.; Filetti, S.; Schlumberger, M. Expression of the Na+/I- symporter gene in human thyroid tumors: A comparison study with other thyroid-specific genes. J. Clin. Endocrinol. Metab. 1999, 84, 3228–3234. [Google Scholar] [CrossRef]
- Bernet, V.J.; Anderson, J.; Vaishnav, Y.; Solomon, B.; Adair, C.F.; Saji, M.; Burman, K.D.; Burch, H.B.; Ringel, M.D. Determination of galectin-3 messenger ribonucleic Acid overexpression in papillary thyroid cancer by quantitative reverse transcription-polymerase chain reaction. J. Clin. Endocrinol. Metab. 2002, 87, 4792–4796. [Google Scholar] [CrossRef]
- Larionov, A.; Krause, A.; Miller, W. A standard curve based method for relative real time PCR data processing. BMC Bioinform. 2005, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, M.; Brusetti, L.; Quatrini, P.; Borin, S.; Puglia, A.M.; Rizzi, A.; Zanardini, E.; Sorlini, C.; Corselli, C.; Daffonchio, D. Comparison of different primer sets for use in automated ribosomal intergenic spacer analysis of complex bacterial communities. Appl. Environ. Microbiol. 2004, 70, 6147–6156. [Google Scholar] [CrossRef] [PubMed]
- Ciarloni, L.; Hosseinian, S.; Monnier-Benoit, S.; Imaizumi, N.; Dorta, G.; Ruegg, C.; Group, D.-C.-S. Discovery of a 29-gene panel in peripheral blood mononuclear cells for the detection of colorectal cancer and adenomas using high throughput real-time PCR. PLoS ONE 2015, 10, e0123904. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.Y.; Hwang, Y.T.; Perng, W.C.; Chian, C.F.; Ho, C.L.; Lee, S.C.; Chang, H.; Terng, H.J.; Chao, T.Y. CPEB4 and IRF4 expression in peripheral mononuclear cells are potential prognostic factors for advanced lung cancer. J. Formos. Med. Assoc. 2017, 116, 114–122. [Google Scholar] [CrossRef] [Green Version]
- Ross, R.W.; Galsky, M.D.; Scher, H.I.; Magidson, J.; Wassmann, K.; Lee, G.S.; Katz, L.; Subudhi, S.K.; Anand, A.; Fleisher, M.; et al. A whole-blood RNA transcript-based prognostic model in men with castration-resistant prostate cancer: A prospective study. Lancet Oncol. 2012, 13, 1105–1113. [Google Scholar] [CrossRef]
- Dumeaux, V.; Ursini-Siegel, J.; Flatberg, A.; Fjosne, H.E.; Frantzen, J.O.; Holmen, M.M.; Rodegerdts, E.; Schlichting, E.; Lund, E. Peripheral blood cells inform on the presence of breast cancer: A population-based case-control study. Int. J. Cancer 2015, 136, 656–667. [Google Scholar] [CrossRef] [PubMed]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. of Patients | Age (years) | Gender, Female (%) | Tumor Size (cm) | |
|---|---|---|---|---|
| Discovery Phase | ||||
| Benign | n = 10 | 48.4 (18–70) | 0.80 | 2.0 (1.2–2.9) |
| Malignant | n = 10 | 46.5 (28–63) | 0.80 | 2.0 (1.2–2.8) |
| Validation Phase | ||||
| BEN | n = 20 | 48.6 (18–70) | 0.75 | 2.3 (1.0–4.8) |
| MAL | n = 44 | 44.5 (17–83) | 0.75 | 2.3 (1.1–5.5) |
| Validation Phase (MAL Subgroups, n = 44) | ||||
| MALLT− | n = 35 | 45.1 (17–83) | 0.71 | 2.3 (1.1–5.5) |
| MALLT+ | n = 9 | 42.1 (27–65) | 0.89 | 2.2 (1.3–4.1) |
| MALmulti− | n = 31 | 43.4 (17–83) | 0.74 | 2.4 (1.2–5.5) |
| MALmulti+ | n = 13 | 47.2 (23–70) | 0.77 | 2.1 (1.1–3.2) |
| MALpapillary | n = 36 | 44.6 (17–83) | 0.72 | 2.3 (1.2–5.5) |
| MALfollicular | n = 8 | 44.0 (21–56) | 0.88 | 2.4 (1.1–5.0) |
| SLC5A5 | LGALS3 | |
|---|---|---|
| AUC | 0.831 | 0.681 |
| 95% CI | 0.668–0.994 | 0.466–0.897 |
| p-value | 0.007 | 0.140 |
| Cut-off a | <2.40 × 103 | <2.24 × 106 |
| Sensitivity% | 87.5 | 62.5 |
| Specificity% | 85.0 | 70.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jee, H.-G.; Kim, B.-A.; Kim, M.; Yu, H.W.; Choi, J.Y.; Kim, S.-j.; Lee, K.E. Expression of SLC5A5 in Circulating Tumor Cells May Distinguish Follicular Thyroid Carcinomas from Adenomas: Implications for Blood-Based Preoperative Diagnosis. J. Clin. Med. 2019, 8, 257. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020257
Jee H-G, Kim B-A, Kim M, Yu HW, Choi JY, Kim S-j, Lee KE. Expression of SLC5A5 in Circulating Tumor Cells May Distinguish Follicular Thyroid Carcinomas from Adenomas: Implications for Blood-Based Preoperative Diagnosis. Journal of Clinical Medicine. 2019; 8(2):257. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020257
Chicago/Turabian StyleJee, Hyeon-Gun, Byoung-Ae Kim, Minjun Kim, Hyeong Won Yu, June Young Choi, Su-jin Kim, and Kyu Eun Lee. 2019. "Expression of SLC5A5 in Circulating Tumor Cells May Distinguish Follicular Thyroid Carcinomas from Adenomas: Implications for Blood-Based Preoperative Diagnosis" Journal of Clinical Medicine 8, no. 2: 257. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020257