Central Nervous System Effects of Oral Propranolol for Infantile Hemangioma: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Experimental Section
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
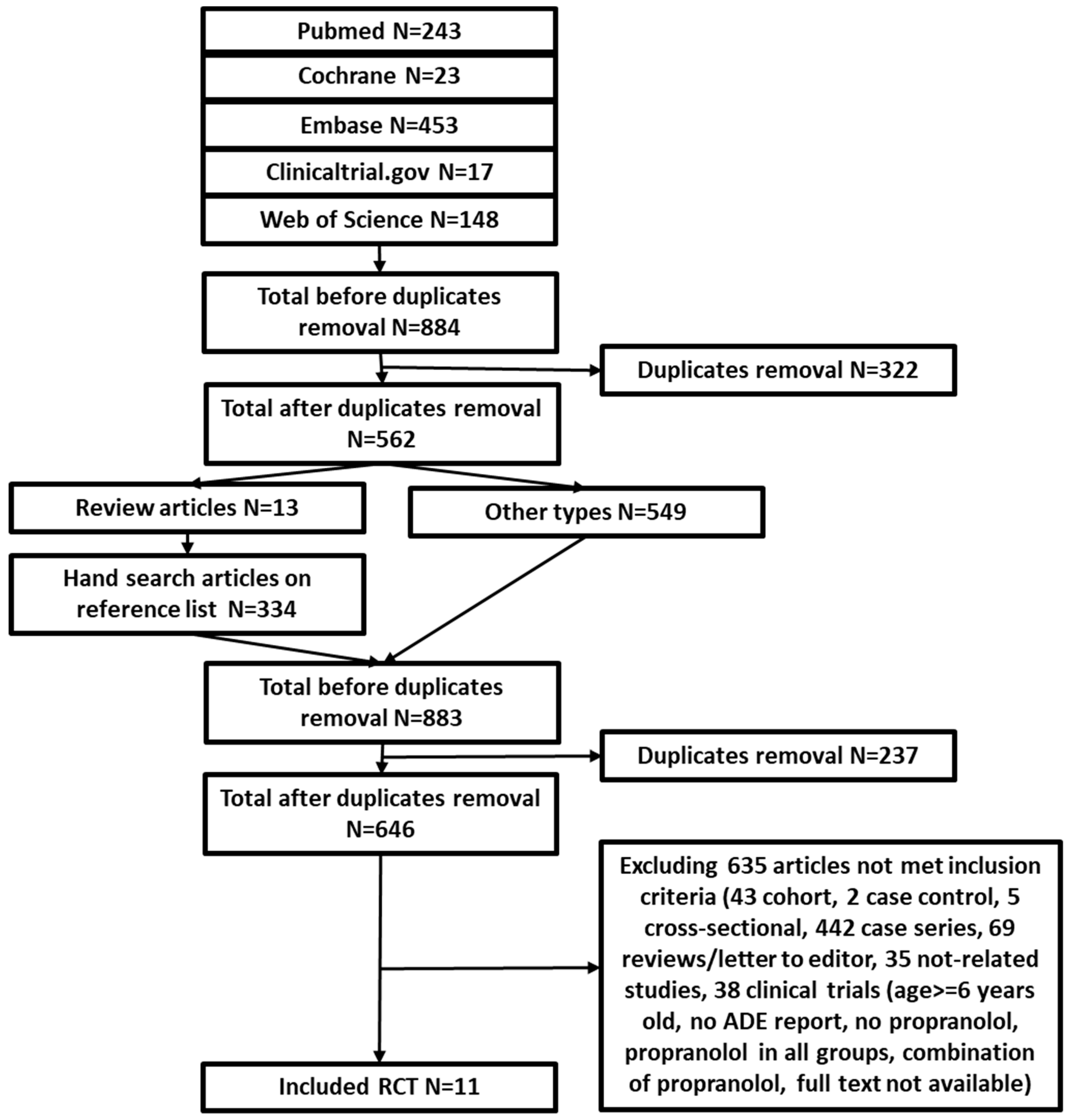
3.1. Study Selection and Characteristics
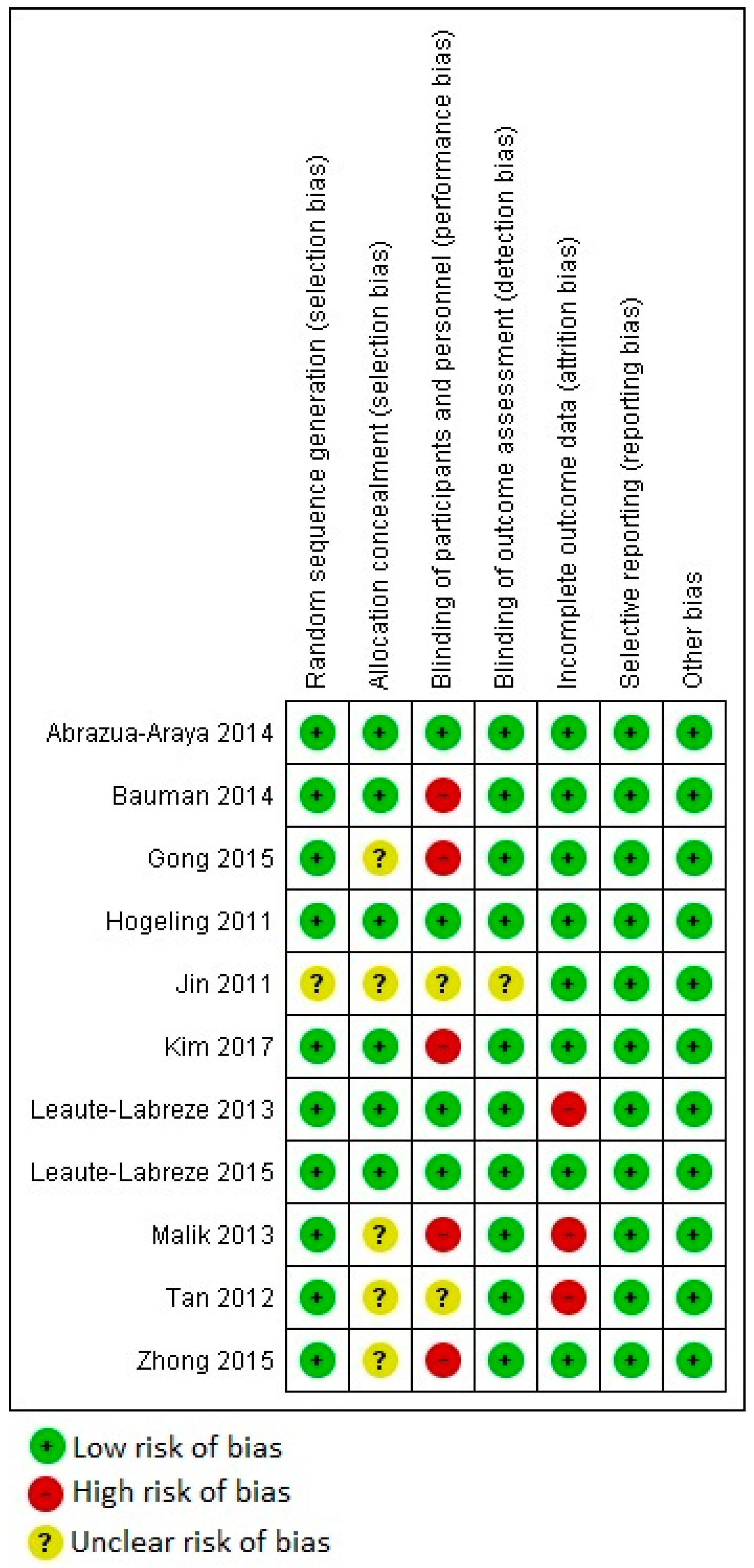
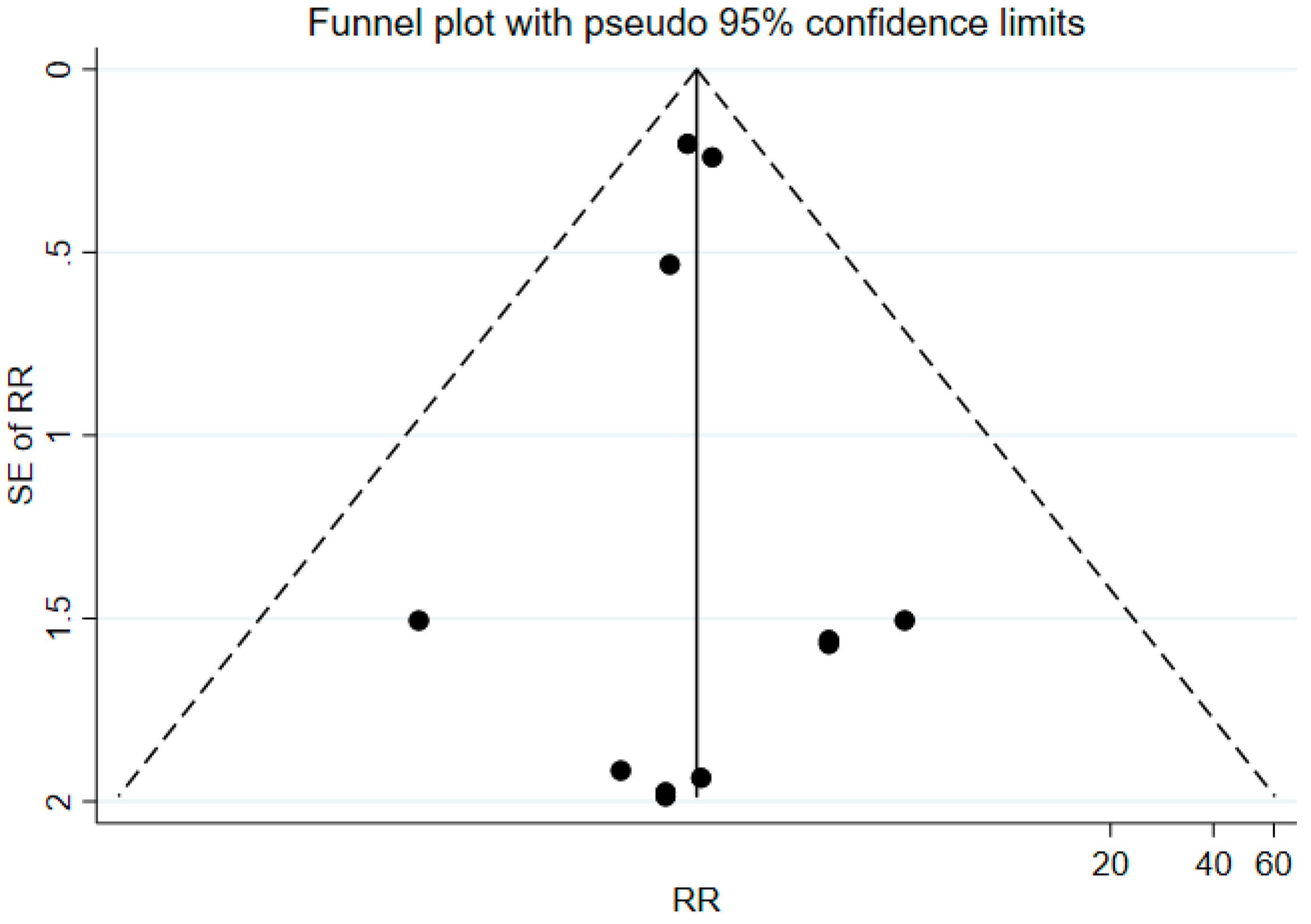
3.2. Study Quality Assessment and Publication Bias Evaluation
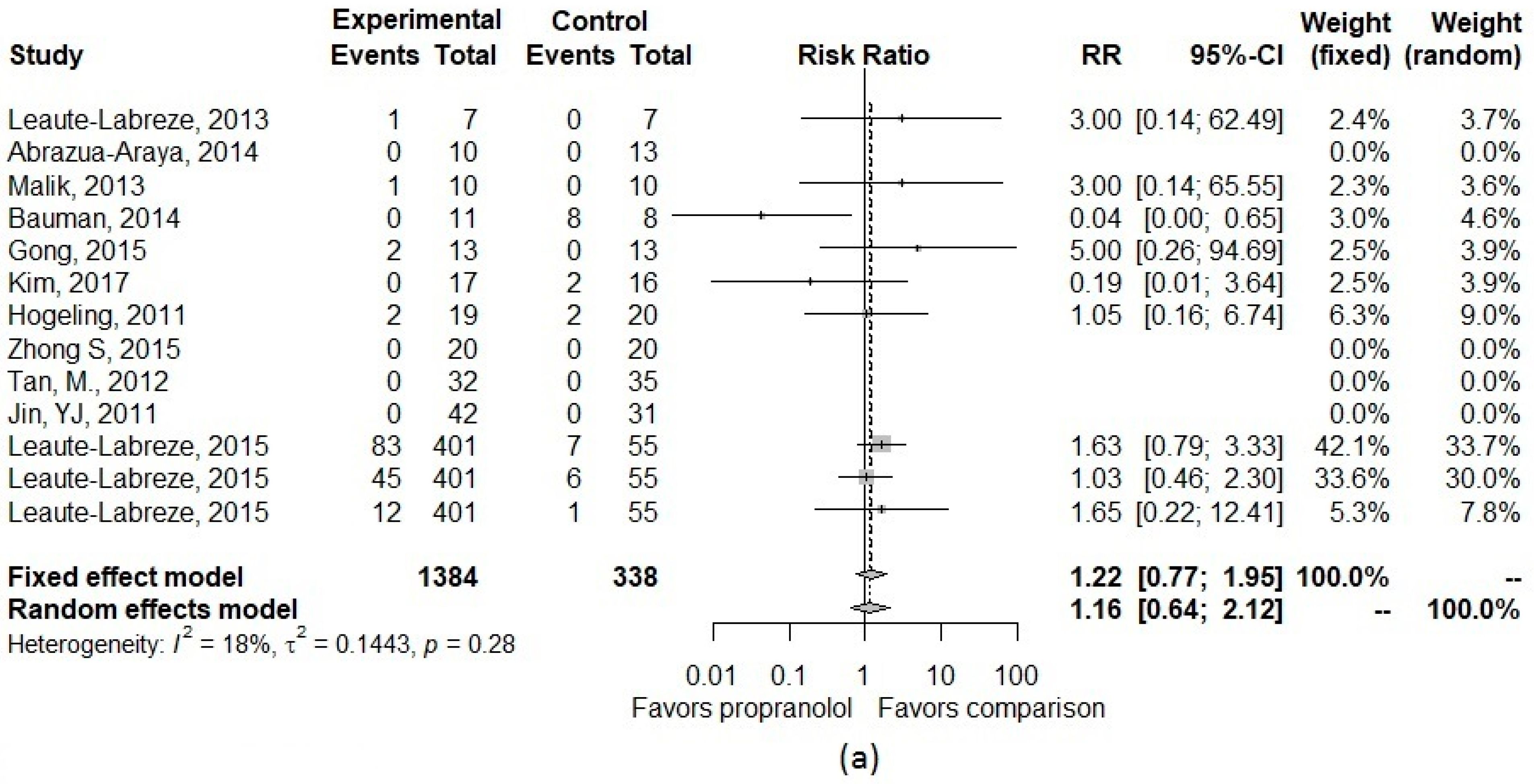
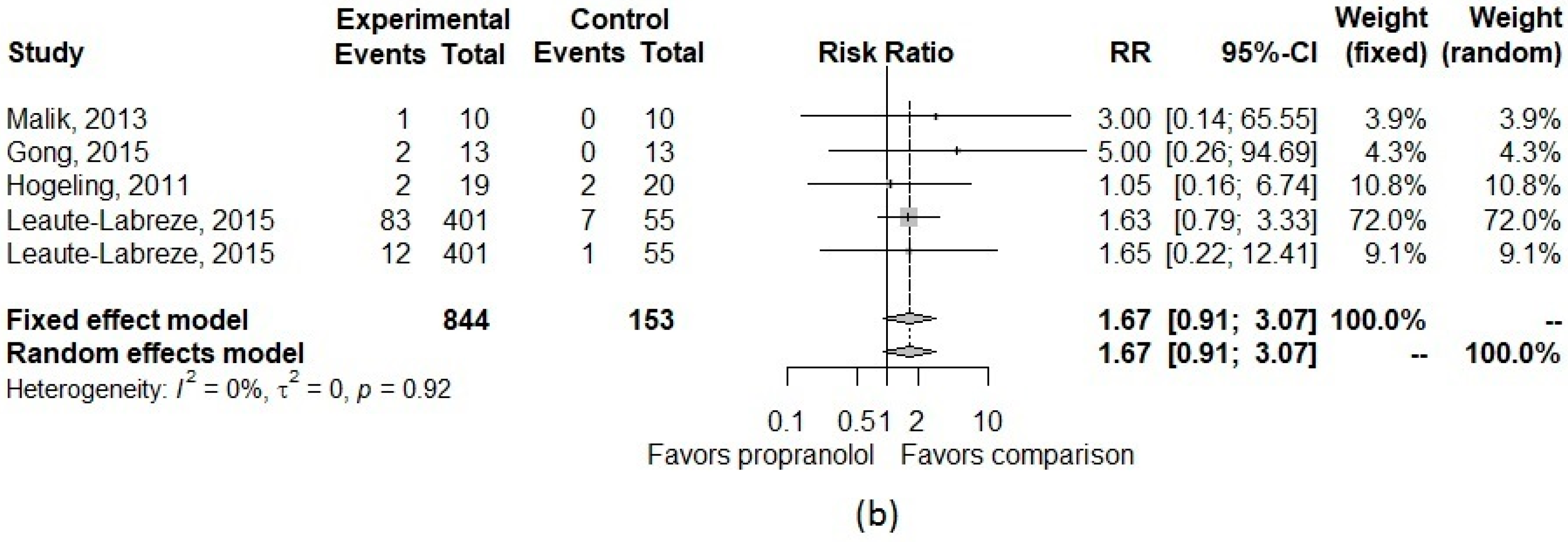
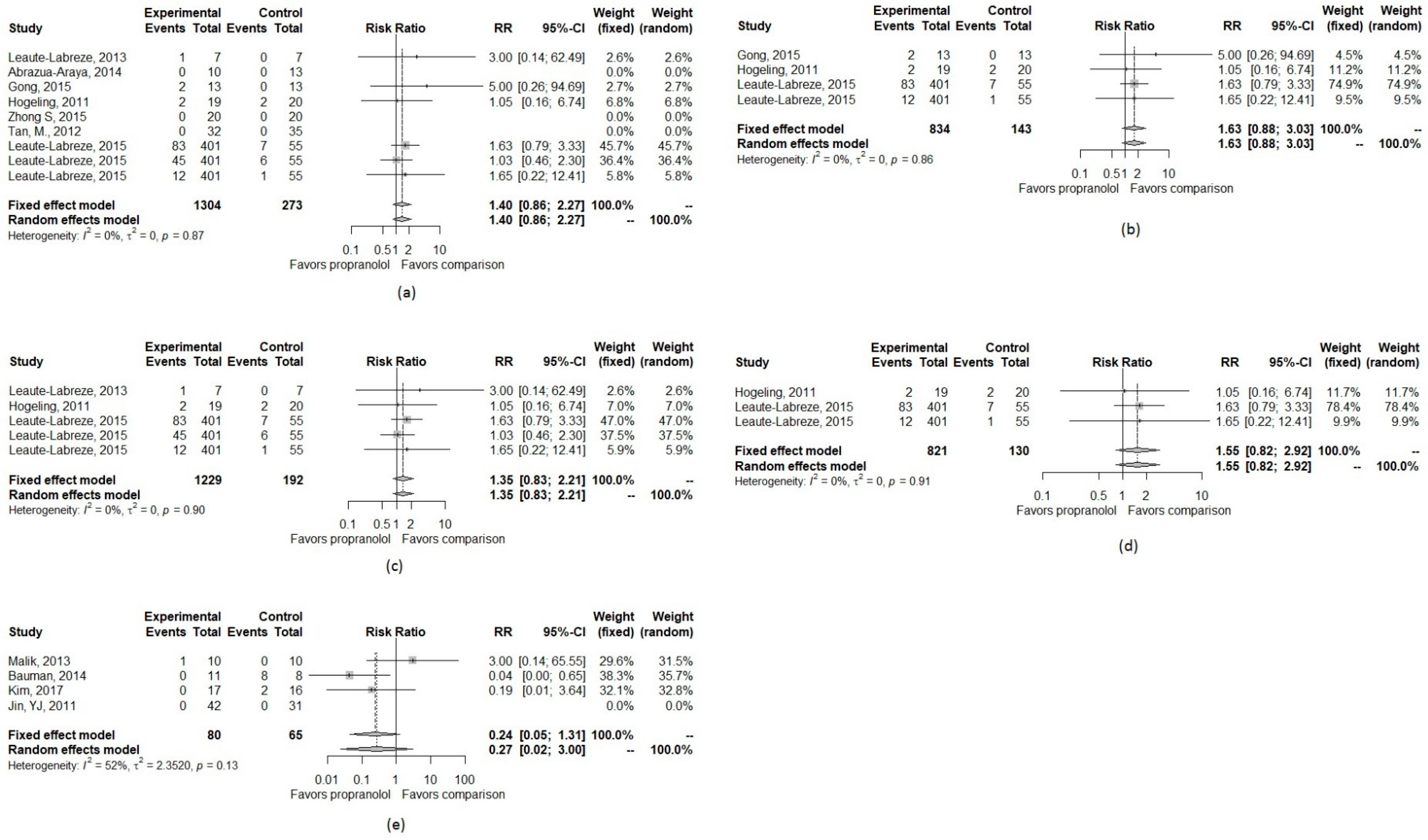
3.3. Pooled Effect Size
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sources | Search Strategy | Number of Studies |
|---|---|---|
| PUBMED | (“infantile hemangioma” OR “infantile haemangioma” OR angioma OR chorioangioma* OR “Kasabach-Merritt Syndrome” OR “Sturge-Weber Syndrome”) and oral and (propranolol OR inderal OR avlocardyl OR remagen OR dexpropranolol OR dociton OR obsidian OR obzidan OR anaprilin* OR betadran) | 243 |
| Cochrane | (“infantile hemangioma” OR “infantile haemangioma” OR angioma OR chorioangioma* OR “Kasabach-Merritt Syndrome” OR “Sturge-Weber Syndrome”) AND (propranolol OR inderal OR avlocardyl OR remagen OR dexpropranolol OR dociton OR obsidian OR obzidan OR anaprilin* OR betadran) AND oral | 23 |
| Web of Science | TOPIC:(((((((“infantile hemangioma” OR “infantile haemangioma”) OR angioma) OR chorioangioma*) OR “Kasabach-Merritt Syndrome”) OR “Sturge-Weber Syndrome”) AND (((((((((propranolol OR inderal) OR avlocardyl) OR remagen) OR dexpropranolol) OR decition) OR obsidian) OR obsidan) OR anaprilin*) OR betatron)) AND oral) Timespan: All years. Indexes: SCI-EXPANDED, SSCI. | 148 |
| Embase | (‘infantile hemangioma’/exp OR ‘infantile hemangioma’ OR ‘infantile haemangioma’/exp OR ‘infantile haemangioma’ OR ‘angioma’/exp OR angioma OR chorioangioma* OR ‘kasabach-merritt syndrome’/exp OR ‘kasabach-merritt syndrome’ OR ‘sturge-weber syndrome’/exp OR ‘sturge-weber syndrome’) AND oral AND (‘propranolol’/exp OR propranolol OR ‘inderal’/exp OR inderal OR ‘avlocardyl’/exp OR avlocardyl OR remagen OR ‘dexpropranolol’/exp OR dexpropranolol OR ‘dociton’/exp OR dociton OR ‘obsidian’/exp OR obsidian OR ‘obzidan’/exp OR obzidan OR anaprilin* OR ‘betadran’/exp OR betadran) AND (‘clinical article’/de OR ‘clinical trial’/de OR ‘cohort analysis’/de OR ‘comparative study’/de OR ‘controlled study’/de OR ‘human’/de OR ‘major clinical study’/de OR ‘medical record review’/de OR ‘multicenter study’/de OR ‘observational study’/de OR ‘prospective study’/de OR ‘randomized controlled trial’/de OR ‘randomized controlled trial (topic)’/de OR ‘retrospective study’/de OR ‘systematic review’/de) AND ([infant]/lim OR [newborn]/lim OR [preschool]/lim) | 453 |
| ClinicalTrials.gov | propranolol OR inderal OR avlocardyl OR remagen OR dexpropranolol OR dociton OR obsidian OR obzidan OR anaprilin* OR betadran | infantile hemangioma OR infantile haemangioma OR angioma OR chorioangioma* OR Kasabach-Merritt Syndrome OR Sturge-Weber Syndrome | propranolol OR inderal OR avlocardyl OR remagen OR dexpropranolol OR dociton OR obsidian OR obzidan OR anaprilin* OR betadran | 17 |
| Stratification | Approaches | CNS Effect | Sleep Related Effect |
|---|---|---|---|
| All included studies | Inverse variance with 0.5 continuity correction (main analysis) | 1.16 (0.64–2.12) | 1.67 (0.91–3.07) |
| Inverse variance with “treatment-arm” continuity correction | 1.14 (0.61–2.11) | 1.35 (0.84–2.17) | |
| Mantel-Haenszel | 1.15 (0.62–2.15) | 1.35 (0.84–2.17) | |
| Beta-binomial with correlated responses | 0.45 (0.14–1.53) | 1.96 (0.46–8.43) | |
| Studies with comparison group of corticosteroids | Inverse variance with 0.5 continuity correction | 0.27 (0.02–3.00) | |
| Inverse variance with “treatment-arm” continuity correction | 0.27 (0.03–2.81) | ||
| Mantel-Haenszel | 0.27 (0.02–4.49) | ||
| Beta-binomial with correlated responses | 0.05 (0.003–1.10) | ||
| Studies with comparison group of placebo | Inverse variance with 0.5 continuity correction | 1.35 (0.83–2.11) | 1.55 (0.82–2.92) |
| Inverse variance with “treatment-arm” continuity correction | 1.35 (0.83–2.11) | 1.55 (0.82–2.92) | |
| Mantel-Haenszel | 1.35 (0.83–2.11) | 1.55 (0.82–2.92) | |
| Beta-binomial with correlated responses | 1.40 (0.6–3.30) | 1.44 (0.43–4.84) | |
| Studies with comparison group of non-corticosteroids | Inverse variance with 0.5 continuity correction | 1.40 (0.86–2.27) | 1.63 (0.88–3.03) |
| Inverse variance with “treatment-arm” continuity correction | 1.40 (0.86–2.27) | 1.63 (0.88–3.03) | |
| Mantel-Haenszel | 1.40 (0.86–2.27) | 1.63 (0.88–3.03) | |
| Beta-binomial with correlated responses | 1.70 (0.60–5.16) | 1.77 (0.56–5.55) |


References
- Munden, A.; Butschek, R.; Tom, W.; Marshall, J.S.; Poeltler, D.M.; Krohne, S.; Alió, A.; Ritter, M.; Friedlander, D.; Catanzarite, V.; et al. Prospective study of infantile haemangiomas: Incidence, clinical characteristics and association with placental anomalies. Br. J. Dermatol. 2014, 170, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Léauté-Labrèze, C.; Harper, J.I.; Hoeger, P.H. Infantile haemangioma. Lancet 2017, 390, 85–94. [Google Scholar] [CrossRef]
- Darrow, D.H.; Greene, A.K.; Mancini, A.J.; Nopper, A.J. Diagnosis and Management of Infantile Hemangioma: Executive Summary. Pediatrics 2015, 136, 786. [Google Scholar] [CrossRef] [PubMed]
- Hoeger, P.H.; Harper, J.I.; Baselga, E.; Bonnet, D.; Boon, L.M.; Ciofi Degli Atti, M.; El Hachem, M.; Oranje, A.P.; Rubin, A.T.; Weibel, L.; et al. Treatment of infantile haemangiomas: Recommendations of a European expert group. Eur. J. Pediatr. 2015, 174, 855–865. [Google Scholar] [CrossRef] [PubMed]
- Püttgen, K.B. Diagnosis and Management of Infantile Hemangiomas. Pediatr. Clin. N. Am. 2014, 61, 383–402. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.W.; Wang, X.K.; Qin, Z.P.; Fan, X.D.; Li, K.; Yang, Y.W.; Huo, R.; Liu, S.H.; Zhao, J.H.; Wang, X.Y.; et al. Chinese experts consensus on the use of oral propranolol for treatment of infantile hemangiomas. Shanghai Kou Qiang Yi Xue (Shanghai J. Stomatol.) 2016, 25, 257–260. [Google Scholar]
- U.S. Food and Drug Administration. Hemangeol™ Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/205410s000lbl.pdf (accessed on 12 February 2019).
- Chinnadurai, S.; Fonnesbeck, C.; Snyder, K.M.; Sathe, N.A.; Morad, A.; Likis, F.E.; McPheeters, M.L. Pharmacologic Interventions for Infantile Hemangioma: A Meta-analysis. Pediatrics 2016, 137, e20153896. [Google Scholar] [CrossRef]
- Marqueling, A.L.; Oza, V.; Frieden, I.J.; Puttgen, K.B. Propranolol and Infantile Hemangiomas Four Years Later: A Systematic Review. Pediatr. Dermatol. 2013, 30, 182–191. [Google Scholar] [CrossRef]
- Langley, A.; Pope, E. Propranolol and central nervous system function: Potential implications for paediatric patients with infantile haemangiomas. Br. J. Dermatol. 2015, 172, 13–23. [Google Scholar] [CrossRef]
- Leaute-Labreze, C.; Boccara, O.; Degrugillier-Chopinet, C.; Mazereeuw-Hautier, J.; Prey, S.; Lebbe, G.; Gautier, S.; Ortis, V.; Lafon, M.; Montagne, A.; et al. Safety of Oral Propranolol for the Treatment of Infantile Hemangioma: A Systematic Review. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [Green Version]
- The Cochrane Statistical Methods Group and the Cochrane Bias Methods Group. Cochrane Risk-of-Bias Tool for Randomized Trials. Available online: http://handbook-5-1.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.htm (accessed on 18 November 2018).
- Efthimiou, O. Practical guide to the meta-analysis of rare events. Evid. Based Ment. Health 2018, 21, 72–76. [Google Scholar] [CrossRef] [PubMed]
- von Hippel, P.T. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, G. General Package for Meta-Analysis. Available online: https://www.r-project.org/ (accessed on 22 November 2018).
- Luo, S.; Chen, Y.; Su, X.; Chu, H. mmeta: Multivariate Meta-Analysis. Available online: https://cran.r-project.org/web/packages/mmeta/index.html (accessed on 22 November 2018).
- Abarzua-Araya, A.; Navarrete-Dechent, C.P.; Heusser, F.; Retamal, J.; Zegpi-Trueba, M.S. Atenolol versus propranolol for the treatment of infantile hemangiomas: A randomized controlled study. J. Am. Acad. Dermatol. 2014, 70, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Choi, T.H.; Choi, Y.; Park, Y.; Hong, K.Y.; Kim, D.Y.; Choe, Y.S.; Lee, H.; Cheon, J.E.; Park, J.B.; et al. Comparison of Efficacy and Safety Between Propranolol and Steroid for Infantile Hemangioma A Randomized Clinical Trial. JAMA Dermatol. 2017, 153, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Leaute-Labreze, C.; Dumas de la Roque, E.; Nacka, F.; Abouelfath, A.; Grenier, N.; Rebola, M.; Ezzedine, K.; Moore, N. Double-blind randomized pilot trial evaluating the efficacy of oral propranolol on infantile haemangiomas in infants < 4 months of age. Br. J. Dermatol. 2013, 169, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.A.; Menon, P.; Rao, K.L.N.; Samujh, R. Effect of propranolol vs prednisolone vs propranolol with prednisolone in the management of infantile hemangioma: A randomized controlled study. J. Pediatr. Surg. 2013, 48, 2453–2459. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Xu, D.P.; Li, Y.X.; Cheng, C.; Li, G.; Wang, X.K. Evaluation of the efficacy and safety of propranolol, timolol maleate, and the combination of the two, in the treatment of superficial infantile haemangiomas. Br. J. Oral Maxillofac. Surg. 2015, 53, 836–840. [Google Scholar] [CrossRef]
- Bauman, N.M.; McCarter, R.J.; Guzzetta, P.C.; Shin, J.J.; Oh, A.K.; Preciado, D.A.; He, J.; Greene, E.A.; Puttgen, K.B. Propranolol vs. prednisolone for symptomatic proliferating infantile hemangiomas: A randomized clinical trial. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 323–330. [Google Scholar] [CrossRef]
- Hogeling, M.; Adams, S.; Wargon, O. A randomized controlled trial of propranolol for infantile hemangiomas. Pediatrics 2011, 128, e259–e266. [Google Scholar] [CrossRef]
- Leaute-Labreze, C.; Hoeger, P.; Mazereeuw-Hautier, J.; Guibaud, L.; Baselga, E.; Posiunas, G.; Phillips, R.J.; Caceres, H.; Gutierrez, J.C.L.; Ballona, R.; et al. A Randomized, Controlled Trial of Oral Propranolol in Infantile Hemangioma. New Eng. J. Med. 2015, 372, 735–746. [Google Scholar] [CrossRef]
- Jin, Y.; Jin, Z.; Cui, X.; Jin, Y. The clinical observation of propranolol taken orally for infantile hemangiomas. Chin. J. Dermatovenereol. 2011, 25, 688–690. [Google Scholar]
- Zhong, S.; Tao, Y.; Zhou, J.; Yao, L.; Uu, Y.; Yan, D.; Li, S. Evaluation on efficacy of low dose propranolol combined with 1 064 nm Nd: YAG laser on mixed and deeper infantile hemangioma. J. Jilin Univ. Med. Ed. 2015, 41, 1032–1035. [Google Scholar]
- Tan, M.; Duan, B.; Zhou, C.M.; Gong, H. The therapeutic effect of propranolol with 1064 nm Nd: YAG laser on proliferating hemangioma in body surface. Zhonghua Zheng Xing Wai Ke Za Zhi 2012, 28, 164–168. [Google Scholar] [PubMed]




| Author (Year) | Sample Size | Inclusion Criteria | Exclusion Criteria | Comparison Treatment | Age | Propranolol Treatment Dosage | Propranolol Treatment Duration | Follow-Up Time | Country | Year of Data Collection |
|---|---|---|---|---|---|---|---|---|---|---|
| Abrazua-Araya (2014) | 23 | IH needing treatment | History of allergy, hypersensitivity and treatment, heart or respiratory disease | Atenolol 1 mg/kg/d for 6 m | 5.2 ± 3.5 m | 2 mg/kg/d | 6 m | 0 m | Chile | 2012–2013 |
| Jin, YJ (2011) | 73 | Diagnosed with IH that influence their appearance were included. | Heart or respiratory disease | Prednisone 3 mg/kg/d, 6 m max | NR | 2 mg/kg/d | 6 m max | 0 m | China | 2009–2010 |
| Kim, K. H. (2017) | 34 | IH had 10–20% volume increase in 2–4 w or IH-related dysfunction or aesthetic problem | Without normal heart function or having treatment history | Prednisolone 2 mg/kg/d | 3.3 m | 2 mg/kg/d | 16 w | 4 w | Korea | 2013–2014 |
| Leaute-Labreze, C. (2013) | 14 | ≥ 1 nonthreatening IH > 1 cm; without vital or functional impairment; not justifying oral corticosteroids | Requiring urgent IH treatment; contraindications or history of treatment | Placebo | 12 w | 3–4 mg/kg/d | 1 m | 0 m | France | 2008–2010 |
| Malik, M. A. (2013) | 20 | Problematic IH | Presence or history of heart, bronchoobstructive, metabolic, or liver disease, visceral lesions, prematurity | Prednisolone 1 mg/kg/d | 4–5 m | 1–3 mg/kg/d | 1 y max | 6 m | India | 2011–2012 |
| Gong, H. (2015) | 26 | Superficial hemangiomas, no previous treatment | Deep/mixed haemangiomas, respiratory or heart disease, fever, diarrhea | 0.5% timolol maleate eye drops | NR | 1.5 mg/kg/d | 5.3 m | 3–12 m | China | 2012–2013 |
| Zhong S (2015) | 40 | Mixed or deeper IH >8 mm diameter, treatment naïve; complete treatment and follow-up | Heart and respiratory disease | Laser | 3.69 m | 1.5 mg/kg/d | 6 m | 0 m | China | 2013–2014 |
| Bauman (2014) | 19 | Proliferating and symptomatic IH | Inadequate social support, received other IH treatment for IH, having a co-morbidity | Prednisolone 2 mg/kg/d | 2.5–4 m | 2 mg/kg/d | 323 d average | 0 m | US | 2010–2012 |
| Hogeling, M. (2011) | 39 | IHs with a deep component, impair function, or aesthetic disfigurement, late or failed to respond to corticosteroid therapy. | Requiring urgent treatment, contraindications to propranolol, extracutaneous IH | Placebo | 67–71 w | 1–2 mg/kg/d | 6.5 m | 0 m | Australia | 2009–2010 |
| Leaute-Labreze, C. (2015) | 456 | A proliferating IH required systematic therapy | Patients with life-threatening, function-threatening, or severely ulcerated hemangiomas | Placebo | 103.8 d | 1–3 mg/kg/d | 3 or 6 m | 72 w | Multiple | 2010–2011 |
| Tan, M. (2012) | 97 | IH diagnosis, treatment naïve | Respiratory, cardiovascular diseases, other systematic chronic diseases | Laser | NR | 0.5–1 mg/kg/d | 6 m | 0 m | China | 2010–2011 |
| Number | Author, Year | Total Sample Size | Propranolol (n) | Comparison (n) | Type of CNS Effect | Number Patients with CNS Effect in | |
|---|---|---|---|---|---|---|---|
| Propranolol Group | Control Group | ||||||
| 1 | Abrazua-Araya, 2014 | 25 | 10 | 13 | Adverse event related to CNS | 0 | 0 |
| 2 | Kim, 2017 | 35 | 17 | 16 | Growth disability | 0 | 2 |
| 3 | Leaute-Labreze, 2013 | 16 | 7 | 7 | Drowsiness | 1 | 0 |
| 4 | Malik, 2013 | 22 | 10 | 10 | Somnolence | 1 | 0 |
| 5 | Gong, 2015 | 28 | 13 | 13 | Lethargy | 2 | 0 |
| 6 | Bauman, 2014 | 21 | 11 | 8 | Growth and development | 0 | 8 |
| 7 | Hogeling, 2011 | 39 | 19 | 20 | Sleep disturbances | 2 | 2 |
| 8 | Leaute-Labreze, 2015 | 456 | 401 | 55 | Sleep disorder | 83 | 7 |
| 456 | 401 | 55 | Agitation | 45 | 6 | ||
| 456 | 401 | 55 | Somnolence | 12 | 1 | ||
| 9 | Tan, M., 2012 | 69 | 33 | 36 | Adverse event related to CNS | 0 | 0 |
| 10 | Zhong S, 2015 | 42 | 21 | 21 | Adverse event related to CNS | 0 | 0 |
| 11 | Jin, YJ, 2011 | 75 | 43 | 32 | Adverse event related to CNS | 0 | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thai, T.; Wang, C.-Y.; Chang, C.-Y.; Brown, J.D. Central Nervous System Effects of Oral Propranolol for Infantile Hemangioma: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 268. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020268
Thai T, Wang C-Y, Chang C-Y, Brown JD. Central Nervous System Effects of Oral Propranolol for Infantile Hemangioma: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(2):268. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020268
Chicago/Turabian StyleThai, Thuy, Ching-Yu Wang, Ching-Yuan Chang, and Joshua D. Brown. 2019. "Central Nervous System Effects of Oral Propranolol for Infantile Hemangioma: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 2: 268. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020268