Medication in AN: A Multidisciplinary Overview of Meta-Analyses and Systematic Reviews


 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
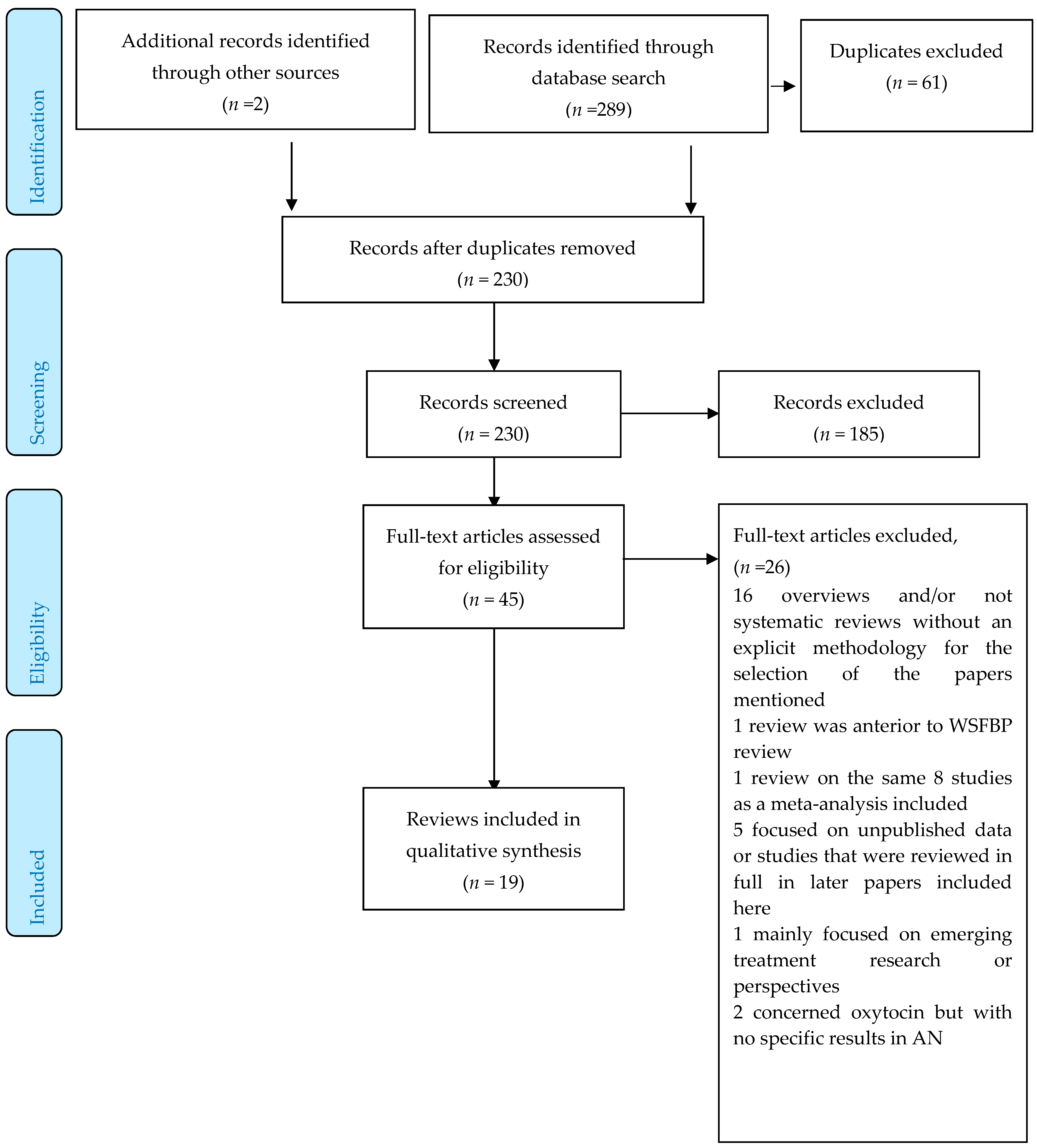
2.1. Data Sources and Search Strategies
2.2. Study selection and Quality Assessment
3. Results
3.1. Papers Selected
3.2. Results: Psychotropic Medications
3.2.1. Methodological Issues
3.2.2. Antidepressants (AD)
Meta-analyses
Tricyclics
Selective Serotonin Reuptake Inhibitors (SSRIs)
Other Antidepressants
Antipsychotics
Meta-Analyses
Typical Antipsychotics other than those Explored in the Meta-Analyses
Other Second-Generation Antipsychotics than those Explored in the Meta-Analyses
3.2.3. Lithium
3.2.4. Appetite Enhancers
Antihistamines
Opiates
Cannabinoids
Ghrelin
3.2.5. Other Medications
Benzodiazepines
Clonidine
N-Methyl-D-Aspartate Agonists and Antagonists
Oxytocin
3.3. Results: Somatic and Nutritional Treatments
3.3.1. Nutritional Support and Refeeding
Approaches to Refeeding
Enteral Feeding (EF)
Oral Nutritional Supplementation
Parenteral Feeding
Micronutrient Supplementation
Zinc
Vitamin B12 and Selenium
Polyunsaturated Fatty Acids (PUFAs)
3.3.2. Functional Digestive Disorders
Drugs Acting on the Gastro-Oesophageal Cardia and Gastric Motility
Other Drugs for the Gastro-Intestinal Tract
Laxatives
Probiotics
3.3.3. Endocrine Medications
Growth Hormone (GH)-Insulin-Like Growth Factor-I (IGF-I) Axis Medication
Hypothalamic-Pituitary-Gonadal Axis Medication
Leptin
3.3.4. Bone and Osteoporosis Medication
Weight Gain/Restoration
Oestrogen Replacement Therapy
Hormonal and Other Somatic Medications
Bisphosphonates
Testosterone
DHEA
IgF1
Teriparatide
Menatetrenone (MED) (Vitamin K2)
Vitamin D and Calcium Supplementation
4. Discussion
4.1. Somatic and Nutritional Aspects
4.2. Psychotropic Drugs
4.3. Use of Psychotropic Medication in AN
4.4. Perspectives
4.5. Strengths and Limitations of This Overview
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Treasure, J.; Claudino, A.M.; Zucker, N. Eating disorders. Lancet Lond. Engl. 2010, 375, 583–593. [Google Scholar] [CrossRef]
- American Psychiatric Association. Practice Guideline for the Treatment of Patients with Eating Disorders; American Psychiatric Association: Philadelphia, PA, USA, 2006. [Google Scholar]
- Haute Autorité de Santé. HAS Anorexia Nervosa Practice Guidelines; HAS: Saint-Denis La Plaine, France, 2010. [Google Scholar]
- National Institute for Health and Care Excellence. NICE Eating Disorders Guidelines: Eating Disorders: Recognition and Treatment; NICE: London, England, 2017. [Google Scholar]
- Herpertz-Dahlmann, B.; van Elburg, A.; Castro-Fornieles, J.; Schmidt, U. ESCAP Expert Paper: New developments in the diagnosis and treatment of adolescent anorexia nervosa—A European perspective. Eur. Child Adolesc. Psychiatry 2015, 24, 1153–1167. [Google Scholar] [CrossRef] [PubMed]
- Aigner, M.; Treasure, J.; Kaye, W.; Kasper, S. WFSBP Task Force on Eating Disorders World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of eating disorders. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2011, 12, 400–443. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M.; Anderson, M.L.; Keiper, C.D.; Whynott, R.; Parker, L. Psychotropic medications in adult and adolescent eating disorders: Clinical practice versus evidence-based recommendations. Eat. Weight Disord. EWD 2016, 21, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Alañón Pardo, M.D.M.; Ferrit Martín, M.; Calleja Hernández, M.Á.; Morillas Márquez, F. Adherence of psychopharmacological prescriptions to clinical practice guidelines in patients with eating behavior disorders. Eur. J. Clin. Pharm. 2017, 73, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Marzola, E.; Nasser, J.A.; Hashim, S.A.; Shih, P.B.; Kaye, W.H. Nutritional rehabilitation in anorexia nervosa: Review of the literature and implications for treatment. BMC Psychiatry 2013, 13, 290. [Google Scholar] [CrossRef] [PubMed]
- Sebaaly, J.C.; Cox, S.; Hughes, C.M.; Kennedy, M.L.H.; Garris, S.S. Use of fluoxetine in anorexia nervosa before and after weight restoration. Ann. Pharm. 2013, 47, 1201–1205. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.E.; Roerig, J.; Steffen, K. Biological therapies for eating disorders. Int. J. Eat. Disord. 2013, 46, 470–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, K.; Peebles, R. Eating disorders in children and adolescents: State of the art review. Pediatrics 2014, 134, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Fazeli, P.K.; Klibanski, A. Anorexia nervosa and bone metabolism. Bone 2014, 66, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Heuvel, L.L.; Jordaan, G.P. The psychopharmacological management of eating disorders in children and adolescents. J. Child Adolesc. Ment. Health 2014, 26, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Starr, T.B.; Kreipe, R.E. Anorexia nervosa and bulimia nervosa: Brains, bones and breeding. Curr. Psychiatry Rep. 2014, 16, 441. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.; Mehler, P.S. Medical complications of anorexia nervosa and their treatments: An update on some critical aspects. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2015, 20, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Saraff, V.; Högler, W. Endocrinology and Adolescence: Osteoporosis in children: Diagnosis and management. Eur. J. Endocrinol. 2015, 173, R185–R197. [Google Scholar] [CrossRef] [PubMed]
- Mairs, R.; Nicholls, D. Assessment and treatment of eating disorders in children and adolescents. Arch. Dis. Child. 2016, 101, 1168–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagielska, G.W.; Przedlacki, J.; Bartoszewicz, Z.; Racicka, E. Bone mineralization disorders as a complication of anorexia nervosa—Etiology, prevalence, course and treatment. Psychiatr. Pol. 2016, 50, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Klibanski, A. Anorexia Nervosa and Its Associated Endocrinopathy in Young People. Horm. Res. Paediatr. 2016, 85, 147–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, H.; Attia, E. Pharmacotherapy of eating disorders. Curr. Opin. Psychiatry 2017, 30, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Drabkin, A.; Rothman, M.S.; Wassenaar, E.; Mascolo, M.; Mehler, P.S. Assessment and clinical management of bone disease in adults with eating disorders: A review. J. Eat. Disord. 2017, 5, 42. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.; Micali, N.; Misra, M. Eating disorders and bone metabolism in women. Curr. Opin. Pediatr. 2017, 29, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Himmerich, H.; Treasure, J. Psychopharmacological advances in eating disorders. Expert Rev. Clin. Pharm. 2018, 11, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.J.; Claudino, A.M. Clinical psychopharmacology of eating disorders: A research update. Int. J. Neuropsychopharmacol. 2012, 15, 209–222. [Google Scholar] [CrossRef] [PubMed]
- Brewerton, T.D. Antipsychotic agents in the treatment of anorexia nervosa: Neuropsychopharmacologic rationale and evidence from controlled trials. Curr. Psychiatry Rep. 2012, 14, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Kishi, T.; Kafantaris, V.; Sunday, S.; Sheridan, E.M.; Correll, C.U. Are antipsychotics effective for the treatment of anorexia nervosa? Results from a systematic review and meta-analysis. J. Clin. Psychiatry 2012, 73, e757–e766. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Klibanski, A. Bone health in anorexia nervosa. Curr. Opin. Endocrinol. Diabetes Obes. 2011, 18, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maguire, S.; O’Dell, A.; Touyz, L.; Russell, J. Oxytocin and anorexia nervosa: A review of the emerging literature. Eur. Eat. Disord. Rev. J. Eat. Disord. Assoc. 2013, 21, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Howgate, D.J.; Graham, S.M.; Leonidou, A.; Korres, N.; Tsiridis, E.; Tsapakis, E. Bone metabolism in anorexia nervosa: Molecular pathways and current treatment modalities. Osteoporos. Int. 2013, 24, 407–421. [Google Scholar] [CrossRef] [PubMed]
- Balestrieri, M.; Oriani, M.G.; Simoncini, A.; Bellantuono, C. Psychotropic drug treatment in anorexia nervosa. Search for differences in efficacy/tolerability between adolescent and mixed-age population. Eur. Eat. Disord. Rev. J. Eat. Disord. Assoc. 2013, 21, 361–373. [Google Scholar] [CrossRef] [PubMed]
- McElroy, S.L.; Guerdjikova, A.I.; Mori, N.; Keck, P.E. Psychopharmacologic treatment of eating disorders: Emerging findings. Curr. Psychiatry Rep. 2015, 17, 35. [Google Scholar] [CrossRef] [PubMed]
- Lutter, M. Emerging Treatments in Eating Disorders. Neurother. J. Am. Soc. Exp. Neurother. 2017, 14, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Leppanen, J.; Ng, K.W.; Tchanturia, K.; Treasure, J. Meta-analysis of the effects of intranasal oxytocin on interpretation and expression of emotions. Neurosci. Biobehav. Rev. 2017, 78, 125–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppanen, J.; Ng, K.W.; Kim, Y.-R.; Tchanturia, K.; Treasure, J. Meta-analytic review of the effects of a single dose of intranasal oxytocin on threat processing in humans. J. Affect. Disord. 2018, 225, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Flament, M.F.; Bissada, H.; Spettigue, W. Evidence-based pharmacotherapy of eating disorders. Int. J. Neuropsychopharmacol. 2012, 15, 189–207. [Google Scholar] [CrossRef] [PubMed]
- Lebow, J.; Sim, L.A.; Erwin, P.J.; Murad, M.H. The effect of atypical antipsychotic medications in individuals with anorexia nervosa: A systematic review and meta-analysis. Int. J. Eat. Disord. 2013, 46, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Lebow, J.; Sim, L. The influence of estrogen therapies on bone mineral density in premenopausal women with anorexia nervosa and amenorrhea. Vitam. Horm. 2013, 92, 243–257. [Google Scholar] [PubMed]
- Watson, H.J.; Bulik, C.M. Update on the treatment of anorexia nervosa: Review of clinical trials, practice guidelines and emerging interventions. Psychol. Med. 2013, 43, 2477–2500. [Google Scholar] [CrossRef] [PubMed]
- De Vos, J.; Houtzager, L.; Katsaragaki, G.; van de Berg, E.; Cuijpers, P.; Dekker, J. Meta analysis on the efficacy of pharmacotherapy versus placebo on anorexia nervosa. J. Eat. Disord. 2014, 2, 27. [Google Scholar] [CrossRef] [PubMed]
- Rocks, T.; Pelly, F.; Wilkinson, P. Nutrition Therapy during Initiation of Refeeding in Underweight Children and Adolescent Inpatients with Anorexia Nervosa: A Systematic Review of the Evidence. J. Acad. Nutr. Diet. 2014, 114, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Dold, M.; Aigner, M.; Klabunde, M.; Treasure, J.; Kasper, S. Second-Generation Antipsychotic Drugs in Anorexia Nervosa: A Meta-Analysis of Randomized Controlled Trials. Psychother. Psychosom. 2015, 84, 110–116. [Google Scholar] [CrossRef] [PubMed]
- El Ghoch, M.; Gatti, D.; Calugi, S.; Viapiana, O.; Bazzani, P.V.; Dalle Grave, R. The Association between Weight Gain/Restoration and Bone Mineral Density in Adolescents with Anorexia Nervosa: A Systematic Review. Nutrients 2016, 8, 769. [Google Scholar] [CrossRef] [PubMed]
- Frank, G.K.W.; Shott, M.E. The Role of Psychotropic Medications in the Management of Anorexia Nervosa: Rationale, Evidence and Future Prospects. CNS Drugs 2016, 30, 419–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, A.K.; Sawyer, S.M.; Golden, N.H.; Guarda, A.S.; Katzman, D.K.; Kohn, M.R.; Le Grange, D.; Madden, S.; Whitelaw, M.; Redgrave, G.W. A systematic review of approaches to refeeding in patients with anorexia nervosa: Refeeding in patients with anorexia nervosa. Int. J. Eat. Disord. 2016, 49, 293–310. [Google Scholar] [CrossRef] [PubMed]
- Kells, M.; Kelly-Weeder, S. Nasogastric Tube Feeding for Individuals with Anorexia Nervosa: An Integrative Review. J. Am. Psychiatr. Nurses Assoc. 2016, 22, 449–468. [Google Scholar] [CrossRef] [PubMed]
- Miniati, M.; Mauri, M.; Ciberti, A.; Mariani, M.G.; Marazziti, D.; Dell’Osso, L. Psychopharmacological options for adult patients with anorexia nervosa. CNS Spectr. 2016, 21, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Golden, N.H.; Katzman, D.K. State of the Art Systematic Review of Bone Disease in Anorexia Nervosa. Int. J. Eat. Disord. 2016, 49, 276–292. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.; Aldridge, V.; Clark, E.M.; Misra, M.; Micali, N. Pharmacological treatment options for low Bone Mineral Density and secondary osteoporosis in Anorexia Nervosa: A systematic review of the literature. J. Psychosom. Res. 2017, 98, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brockmeyer, T.; Friederich, H.-C.; Schmidt, U. Advances in the treatment of anorexia nervosa: A review of established and emerging interventions. Psychol. Med. 2018, 48, 1228–1256. [Google Scholar] [CrossRef] [PubMed]
- Hale, M.D.; Logomarsino, J.V. The use of enteral nutrition in the treatment of eating disorders: A systematic review. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.M.; Douglas, J.W.; Lawrence, J.C. Enteral Nutrition via Nasogastric Tube for Refeeding Patients with Anorexia Nervosa: A Systematic Review. Nutr. Clin. Pract. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lacey, J.H.; Crisp, A.H. Hunger, food intake and weight: The impact of clomipramine on a refeeding anorexia nervosa population. Postgrad. Med. J. 1980, 56 (Suppl. 1), 79–85. [Google Scholar]
- Halmi, K.A.; Eckert, E.; LaDu, T.J.; Cohen, J. Anorexia nervosa. Treatment efficacy of cyproheptadine and amitriptyline. Arch. Gen. Psychiatry 1986, 43, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Attia, E.; Haiman, C.; Walsh, B.T.; Flater, S.R. Does fluoxetine augment the inpatient treatment of anorexia nervosa? Am. J. Psychiatry 1998, 155, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Walsh, B.T.; Kaplan, A.S.; Attia, E.; Olmsted, M.; Parides, M.; Carter, J.C.; Pike, K.M.; Devlin, M.J.; Woodside, B.; Roberto, C.A.; et al. Fluoxetine after weight restoration in anorexia nervosa: A randomized controlled trial. JAMA 2006, 295, 2605–2612. [Google Scholar] [CrossRef] [PubMed]
- Halmi, K.A. Perplexities of treatment resistance in eating disorders. BMC Psychiatry 2013, 13, 292. [Google Scholar] [CrossRef] [PubMed]
- Crisp, A.H.; Lacey, J.H.; Crutchfield, M. Clomipramine and “drive” in people with anorexia nervosa: An in-patient study. Br. J. Psychiatry J. Ment. Sci. 1987, 150, 355–358. [Google Scholar] [CrossRef]
- Strobel, M.; Warnke, A.; Roth, M.; Schulze, U. Paroxetine versus clomipramine in female adolescents suffering from anorexia nervosa and depressive episode—A retrospective study on tolerability, reasons for discontinuing the antidepressive treatment and different outcome measurements. Z. Kinder. Jugendpsychiatr. Psychother. 2004, 32, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Kaye, W.H.; Nagata, T.; Weltzin, T.E.; Hsu, L.K.; Sokol, M.S.; McConaha, C.; Plotnicov, K.H.; Weise, J.; Deep, D. Double-blind placebo-controlled administration of fluoxetine in restricting- and restricting-purging-type anorexia nervosa. Biol. Psychiatry 2001, 49, 644–652. [Google Scholar] [CrossRef]
- Barbarich, N.C.; McConaha, C.W.; Halmi, K.A.; Gendall, K.; Sunday, S.R.; Gaskill, J.; La Via, M.; Frank, G.K.; Brooks, S.; Plotnicov, K.H.; et al. Use of nutritional supplements to increase the efficacy of fluoxetine in the treatment of anorexia nervosa. Int. J. Eat. Disord. 2004, 35, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, F.; Draisci, A.; Peirone, A.; Brunetta, M. Combined cognitive-behavioral, psychopharmacological and nutritional therapy in eating disorders. 2. Anorexia nervosa—Binge-eating/purging type. Neuropsychobiology 1995, 32, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, F.; Draisci, A.; Peirone, A.; Brunetta, M. Combined cognitive-behavioral, psychopharmacological and nutritional therapy in eating disorders. 1. Anorexia nervosa—Restricted type. Neuropsychobiology 1995, 32, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, G.M.; Laini, V.; Mauri, M.C.; Ferrari, V.M.; Clemente, A.; Lugo, F.; Mantero, M.; Redaelli, G.; Zappulli, D.; Cavagnini, F. A single blind comparison of amisulpride, fluoxetine and clomipramine in the treatment of restricting anorectics. Prog. Neuropsychopharmacol. Biol. Psychiatry 2001, 25, 1049–1059. [Google Scholar] [CrossRef]
- Pallanti, S.; Quercioli, L.; Ramacciotti, A. Citalopram in anorexia nervosa. Eat. Weight Disord. EWD 1997, 2, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Calandra, C.; Gulino, V.; Inserra, L.; Giuffrida, A. The use of citalopram in an integrated approach to the treatment of eating disorders: An open study. Eat. Weight Disord. EWD 1999, 4, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Fassino, S.; Leombruni, P.; Daga, G.; Brustolin, A.; Migliaretti, G.; Cavallo, F.; Rovera, G. Efficacy of citalopram in anorexia nervosa: A pilot study. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2002, 12, 453–459. [Google Scholar] [CrossRef]
- Santonastaso, P.; Friederici, S.; Favaro, A. Sertraline in the treatment of restricting anorexia nervosa: An open controlled trial. J. Child Adolesc. Psychopharmacol. 2001, 11, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, S.H.; Piran, N.; Garfinkel, P.E. Monoamine oxidase inhibitor therapy for anorexia nervosa and bulimia: A preliminary trial of isocarboxazid. J. Clin. Psychopharmacol. 1985, 5, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Stip, E.; Lungu, O.V. Salience network and olanzapine in schizophrenia: Implications for treatment in anorexia nervosa. Can. J. Psychiatry Rev. Can. Psychiatr. 2015, 60, S35–S39. [Google Scholar]
- Frieling, H.; Römer, K.D.; Scholz, S.; Mittelbach, F.; Wilhelm, J.; De Zwaan, M.; Jacoby, G.E.; Kornhuber, J.; Hillemacher, T.; Bleich, S. Epigenetic dysregulation of dopaminergic genes in eating disorders. Int. J. Eat. Disord. 2010, 43, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Spettigue, W.; Norris, M.L.; Maras, D.; Obeid, N.; Feder, S.; Harrison, M.E.; Gomez, R.; Fu, M.C.; Henderson, K.; Buchholz, A. Evaluation of the Effectiveness and Safety of Olanzapine as an Adjunctive Treatment for Anorexia Nervosa in Adolescents: An Open-Label Trial. J. Can. Acad. Child Adolesc. Psychiatry J. Acad. Can. Psychiatr. Enfant Adolesc. 2018, 27, 197–208. [Google Scholar]
- Himmerich, H.; Au, K.; Dornik, J.; Bentley, J.; Schmidt, U.; Treasure, J. Olanzapine Treatment for Patients with Anorexia Nervosa. Can. J. Psychiatry Rev. Can. Psychiatr. 2017, 62, 506–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brambilla, F.; Amianto, F.; Dalle Grave, R.; Fassino, S. Lack of efficacy of psychological and pharmacological treatments of disorders of eating behavior: Neurobiological background. BMC Psychiatry 2014, 14, 376. [Google Scholar] [CrossRef] [PubMed]
- Attia, E.; Steinglass, J.E.; Walsh, B.T.; Wang, Y.; Wu, P.; Schreyer, C.; Wildes, J.; Yilmaz, Z.; Guarda, A.S.; Kaplan, A.S.; et al. Olanzapine Versus Placebo in Adult Outpatients with Anorexia Nervosa: A Randomized Clinical Trial. Am. J. Psychiatry 2019. [Google Scholar] [CrossRef] [PubMed]
- Vandereycken, W.; Pierloot, R. Pimozide combined with behavior therapy in the short-term treatment of anorexia nervosa. A double-blind placebo-controlled cross-over study. Acta Psychiatr. Scand. 1982, 66, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Vandereycken, W. Neuroleptics in the short-term treatment of anorexia nervosa. A double-blind placebo-controlled study with sulpiride. Br. J. Psychiatry J. Ment. Sci. 1984, 144, 288–292. [Google Scholar] [CrossRef]
- Cassano, G.B.; Miniati, M.; Pini, S.; Rotondo, A.; Banti, S.; Borri, C.; Camilleri, V.; Mauri, M. Six-month open trial of haloperidol as an adjunctive treatment for anorexia nervosa: A preliminary report. Int. J. Eat. Disord. 2003, 33, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Mondraty, N.; Birmingham, C.L.; Touyz, S.; Sundakov, V.; Chapman, L.; Beumont, P. Randomized controlled trial of olanzapine in the treatment of cognitions in anorexia nervosa. Australas Psychiatry Bull. R. Aust. N. Z. Coll. Psychiatr. 2005, 13, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, F.; Monteleone, P.; Maj, M. Olanzapine-induced weight gain in anorexia nervosa: Involvement of leptin and ghrelin secretion? Psychoneuroendocrinology 2007, 32, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, F.; Garcia, C.S.; Fassino, S.; Daga, G.A.; Favaro, A.; Santonastaso, P.; Ramaciotti, C.; Bondi, E.; Mellado, C.; Borriello, R.; et al. Olanzapine therapy in anorexia nervosa: Psychobiological effects. Int. Clin. Psychopharmacol. 2007, 22, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Bissada, H.; Tasca, G.A.; Barber, A.M.; Bradwejn, J. Olanzapine in the treatment of low body weight and obsessive thinking in women with anorexia nervosa: A randomized, double-blind, placebo-controlled trial. Am. J. Psychiatry 2008, 165, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Attia, E.; Kaplan, A.S.; Walsh, B.T.; Gershkovich, M.; Yilmaz, Z.; Musante, D.; Wang, Y. Olanzapine versus placebo for out-patients with anorexia nervosa. Psychol. Med. 2011, 41, 2177–2182. [Google Scholar] [CrossRef] [PubMed]
- Kafantaris, V.; Leigh, E.; Hertz, S.; Berest, A.; Schebendach, J.; Sterling, W.M.; Saito, E.; Sunday, S.; Higdon, C.; Golden, N.H.; et al. A placebo-controlled pilot study of adjunctive olanzapine for adolescents with anorexia nervosa. J. Child Adolesc. Psychopharmacol. 2011, 21, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Hagman, J.; Gralla, J.; Sigel, E.; Ellert, S.; Dodge, M.; Gardner, R.; O’Lonergan, T.; Frank, G.; Wamboldt, M.Z. A double-blind, placebo-controlled study of risperidone for the treatment of adolescents and young adults with anorexia nervosa: A pilot study. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Powers, P.S.; Klabunde, M.; Kaye, W. Double-blind placebo-controlled trial of quetiapine in anorexia nervosa. Eur. Eat. Disord. Rev. J. Eat. Disord. Assoc. 2012, 20, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Court, A.; Mulder, C.; Kerr, M.; Yuen, H.P.; Boasman, M.; Goldstone, S.; Fleming, J.; Weigall, S.; Derham, H.; Huang, C.; et al. Investigating the effectiveness, safety and tolerability of quetiapine in the treatment of anorexia nervosa in young people: A pilot study. J. Psychiatr. Res. 2010, 44, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Gross, H.A.; Ebert, M.H.; Faden, V.B.; Goldberg, S.C.; Nee, L.E.; Kaye, W.H. A double-blind controlled trial of lithium carbonate primary anorexia nervosa. J. Clin. Psychopharmacol. 1981, 1, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Stheneur, C.; Bergeron, S.; Lapeyraque, A.-L. Renal complications in anorexia nervosa. Eat. Weight Disord. EWD 2014, 19, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.C.; Eckert, E.D.; Halmi, K.A.; Casper, R.C.; Davis, J.M.; Roper, M. Effects of cyproheptadine on symptoms and attitudes in anorexia nervosa. Arch. Gen. Psychiatry 1980, 37, 1083. [Google Scholar] [PubMed]
- Halmi, K.A.; Eckert, E.; Falk, J.R. Cyproheptadine for anorexia nervosa. Lancet Lond. Engl. 1982, 1, 1357–1358. [Google Scholar] [CrossRef]
- Marrazzi, M.A.; Bacon, J.P.; Kinzie, J.; Luby, E.D. Naltrexone use in the treatment of anorexia nervosa and bulimia nervosa. Int. Clin. Psychopharmacol. 1995, 10, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Gross, H.; Ebert, M.H.; Faden, V.B.; Goldberg, S.C.; Kaye, W.H.; Caine, E.D.; Hawks, R.; Zinberg, N. A double-blind trial of delta 9-tetrahydrocannabinol in primary anorexia nervosa. J. Clin. Psychopharmacol. 1983, 3, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Andries, A.; Frystyk, J.; Flyvbjerg, A.; Støving, R.K. Dronabinol in severe, enduring anorexia nervosa: A randomized controlled trial. Int. J. Eat. Disord. 2014, 47, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Hotta, M.; Ohwada, R.; Akamizu, T.; Shibasaki, T.; Kangawa, K. Therapeutic potential of ghrelin in restricting-type anorexia nervosa. Methods Enzym. 2012, 514, 381–398. [Google Scholar]
- Steinglass, J.E.; Kaplan, S.C.; Liu, Y.; Wang, Y.; Walsh, B.T. The (lack of) effect of alprazolam on eating behavior in anorexia nervosa: A preliminary report. Int. J. Eat. Disord. 2014, 47, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Casper, R.C.; Schlemmer, R.F.; Javaid, J.I. A placebo-controlled crossover study of oral clonidine in acute anorexia nervosa. Psychiatry Res. 1987, 20, 249–260. [Google Scholar] [CrossRef]
- Levinson, C.A.; Rodebaugh, T.L.; Fewell, L.; Kass, A.E.; Riley, E.N.; Stark, L.; McCallum, K.; Lenze, E.J. D-Cycloserine facilitation of exposure therapy improves weight regain in patients with anorexia nervosa: A pilot randomized controlled trial. J. Clin. Psychiatry 2015, 76, e787–e793. [Google Scholar] [CrossRef] [PubMed]
- Lechin, F.; van der Dijs, B.; Pardey-Maldonado, B.; Baez, S.; Lechin, M.E. Anorexia nervosa versus hyperinsulinism: Therapeutic effects of neuropharmacological manipulation. Clin. Risk Manag. 2011, 7, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.; Maguire, S.; Hunt, G.E.; Kesby, A.; Suraev, A.; Stuart, J.; Booth, J.; McGregor, I.S. Intranasal oxytocin in the treatment of anorexia nervosa: Randomized controlled trial during re-feeding. Psychoneuroendocrinology 2018, 87, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Agostino, H.; Erdstein, J.; Di Meglio, G. Shifting Paradigms: Continuous Nasogastric Feeding with High Caloric Intakes in Anorexia Nervosa. J. Adolesc. Health 2013, 53, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Findlay, S.M.; Toews, H.; Grant, C. Use of Gastrostomy Tubes in Children and Adolescents with Eating Disorders and Related Illnesses. J. Adolesc. Health 2011, 48, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Heruc, G.A.; Little, T.J.; Kohn, M.R.; Madden, S.; Clarke, S.D.; Horowitz, M.; Feinle-Bisset, C. Effects of starvation and short-term refeeding on gastric emptying and postprandial blood glucose regulation in adolescent girls with anorexia nervosa. Am. J. Physiol. Endocrinol. Metab. 2018, 315, E565–E573. [Google Scholar] [CrossRef] [PubMed]
- Hofer, M.; Pozzi, A.; Joray, M.; Ott, R.; Hähni, F.; Leuenberger, M.; von Känel, R.; Stanga, Z. Safe refeeding management of anorexia nervosa inpatients: An evidence-based protocol. Nutrition 2014, 30, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Garber, A.K.; Michihata, N.; Hetnal, K.; Shafer, M.-A.; Moscicki, A.-B. A Prospective Examination of Weight Gain in Hospitalized Adolescents with Anorexia Nervosa on a Recommended Refeeding Protocol. J. Adolesc. Health 2012, 50, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Ozier, A.D.; Henry, B.W. Position of the American Dietetic Association: Nutrition Intervention in the Treatment of Eating Disorders. J. Am. Diet. Assoc. 2011, 111, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, D.; Brondel, L.; Poupard, A.T.; Talonneau, I.; Brun, J.M. A randomized trial on the efficacy of a 2-month tube feeding regimen in anorexia nervosa: A 1-year follow-up study. Clin. Nutr. 2007, 26, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, D.J.; Brayer, V.; Roblot, A.; Brindisi, M.-C.; Vergès, B. Efficacy of Tube Feeding in Binge-Eating/Vomiting Patients: A 2-Month Randomized Trial with 1-Year Follow-Up. J. Parenter. Enter. Nutr. 2011, 35, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Silber, T.J.; Robb, A.S.; Orrell-Valente, J.K.; Ellis, N.; Valadez-Meltzer, A.; Dadson, M.J. Nocturnal nasogastric refeeding for hospitalized adolescent boys with anorexia nervosa. J. Dev. Behav. Pediatr. JDBP 2004, 25, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, D.; Pennacchio, H.; Roblot, A.; Jacquet, M.; Tallonneau, I.; Verges, B. Efficacité de la nutrition entérale à domicile chez 60 malades ayant une anorexie mentale. Presse Médicale 2009, 38, 1739–1745. [Google Scholar] [CrossRef] [PubMed]
- Daniel, R.; Didier, P.; Hélène, P. A 3-month at-home tube feeding in 118 bulimia nervosa patients: A one-year prospective survey in adult patients. Clin. Nutr. 2014, 33, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Gentile, M.G.; Pastorelli, P.; Ciceri, R.; Manna, G.M.; Collimedaglia, S. Specialized refeeding treatment for anorexia nervosa patients suffering from extreme undernutrition. Clin. Nutr. Edinb. Scotl. 2010, 29, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Gentile, M.G. Enteral Nutrition for Feeding Severely Underfed Patients with Anorexia Nervosa. Nutrients 2012, 4, 1293–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rigaud, D.; Tallonneau, I.; Brindisi, M.-C.; Vergès, B. Prognosis in 41 severely malnourished anorexia nervosa patients. Clin. Nutr. 2012, 31, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.; Franklin, R.C.; Russell, J.; Abraham, S. A review of feeding methods used in the treatment of anorexia nervosa. J. Eat. Disord. 2013, 1, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arii, I.; Yamashita, T.; Kinoshita, M.; Shimizu, H.; Nakamura, M.; Nakajima, T. Treatment for inpatients with anorexia nervosa: Comparison of liquid formula with regular meals for improvement from emaciation. Psychiatry Clin. Neurosci. 1996, 50, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.K.; Maloney, M.J.; Jellinek, M.S.; Biederman, J. Treating Anorexia Nervosa Patients in the Era of Manage Care. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 1632–1633. [Google Scholar] [PubMed]
- Imbierowicz, K.; Braks, K.; Jacoby, G.E.; Geiser, F.; Conrad, R.; Schilling, G.; Liedtke, R. High-caloric supplements in anorexia treatment. Int. J. Eat. Disord. 2002, 32, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Cockfield, A.; Philpot, U. Managing anorexia from a dietitian’s perspective. Proc. Nutr. Soc. 2009, 68, 281. [Google Scholar] [CrossRef] [PubMed]
- Achamrah, N.; Coëffier, M.; Rimbert, A.; Charles, J.; Folope, V.; Petit, A.; Déchelotte, P.; Grigioni, S. Micronutrient Status in 153 Patients with Anorexia Nervosa. Nutrients 2017, 9, 225. [Google Scholar] [CrossRef] [PubMed]
- Chiurazzi, C.; Cioffi, I.; De Caprio, C.; De Filippo, E.; Marra, M.; Sammarco, R.; Di Guglielmo, M.L.; Contaldo, F.; Pasanisi, F. Adequacy of nutrient intake in women with restrictive anorexia nervosa. Nutrition 2017, 38, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Oudman, E.; Wijnia, J.W.; Oey, M.J.; van Dam, M.J.; Postma, A. Preventing Wernicke’s encephalopathy in anorexia nervosa: A systematic review: Wernicke’s and anorexia nervosa. Psychiatry Clin. Neurosci. 2018, 72, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Asakawa, A.; Li, J.B.; Tsai, M.; Amitani, H.; Ohinata, K.; Komai, M.; Inui, A. Zinc as an appetite stimulator—The possible role of zinc in the progression of diseases such as cachexia and sarcopenia. Recent Pat. Food Nutr. Agric. 2011, 3, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, C.L.; Gritzner, S. How does zinc supplementation benefit anorexia nervosa? Eat. Weight Disord. EWD 2006, 11, e109–e111. [Google Scholar] [CrossRef] [PubMed]
- Franques, J.; Chiche, L.; Mathis, S. Sensory Neuronopathy Revealing Severe Vitamin B12 Deficiency in a Patient with Anorexia Nervosa: An Often-Forgotten Reversible Cause. Nutrients 2017, 9, 281. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, C.L.; Gritzner, S. Heart failure in anorexia nervosa: Case report and review of the literature. Eat. Weight Disord. EWD 2007, 12, e7–e10. [Google Scholar] [CrossRef] [PubMed]
- Perica, M.M.; Delaš, I. Essential Fatty Acids and Psychiatric Disorders. Nutr. Clin. Pract. 2011, 26, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Shih, P.B.; Morisseau, C.; Le, T.; Woodside, B.; German, J.B. Personalized polyunsaturated fatty acids as a potential adjunctive treatment for anorexia nervosa. Prostaglandins Other Lipid Mediat. 2017, 133, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ayton, A.K.; Azaz, A.; Horrobin, D.F. Rapid improvement of severe anorexia nervosa during treatment with ethyl-eicosapentaenoate and micronutrients. Eur. Psychiatry 2004, 19, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Ayton, A.K.; Azaz, A.; Horrobin, D.F. A pilot open case series of ethyl-epa supplementation in the treatment of anorexia nervosa. Prostaglandins Leukot. Essent. Fatty Acids 2004, 71, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Mauler, B.; Dubben, S.; Pawelzik, M.; Pawelzik, D.; Weigle, D.S.; Kratz, M. Hypercaloric diets differing in fat composition have similar effects on serum leptin and weight gain in female subjects with anorexia nervosa. Nutr. Res. 2009, 29, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, S.; Sammet, I.; Rapps, N.; Herzog, W.; Herpertz, S.; Martens, U. Gastrointestinal disturbances in eating disorders: Clinical and neurobiological aspects. Auton. Neurosci. 2006, 129, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Malczyk, Ż.; Oświęcimska, J. Gastrointestinal complications and refeeding guidelines in patients with anorexia nervosa. Psychiatr. Pol. 2017, 51, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Hetterich, L.; Mack, I.; Giel, K.E.; Zipfel, S.; Stengel, A. An update on gastrointestinal disturbances in eating disorders. Mol. Cell. Endocrinol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Luscombe, G.M.; Boyd, C.; Kellow, J.; Abraham, S. Functional gastrointestinal disorders in eating disorder patients: Altered distribution and predictors using ROME III compared to ROME II criteria. World J. Gastroenterol. WJG 2014, 20, 16293–16299. [Google Scholar] [CrossRef] [PubMed]
- Salvioli, B.; Pellicciari, A.; Iero, L.; Di Pietro, E.; Moscano, F.; Gualandi, S.; Stanghellini, V.; De Giorgio, R.; Ruggeri, E.; Franzoni, E. Audit of digestive complaints and psychopathological traits in patients with eating disorders: A prospective study. Dig. Liver Dis. 2013, 45, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Parkman, H.P.; Shafi, M.A.; Abell, T.L.; Gerson, L. Clinical Guideline: Management of Gastroparesis. Am. J. Gastroenterol. 2013, 108, 18–37. [Google Scholar] [CrossRef] [PubMed]
- Mascolo, M.; Geer, B.; Feuerstein, J.; Mehler, P.S. Gastrointestinal comorbidities which complicate the treatment of anorexia nervosa. Eat. Disord. 2017, 25, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Moshiree, B.; McDonald, R.; Hou, W.; Toskes, P.P. Comparison of the Effect of Azithromycin Versus Erythromycin on Antroduodenal Pressure Profiles of Patients with Chronic Functional Gastrointestinal Pain and Gastroparesis. Dig. Dis. Sci. 2010, 55, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Vázquez, M.A.; Vázquez-Elizondo, G.; González-González, J.A.; Gutiérrez-Udave, R.; Maldonado-Garza, H.J.; Bosques-Padilla, F.J. Effect of antispasmodic agents, alone or in combination, in the treatment of Irritable Bowel Syndrome: Systematic review and meta-analysis. Rev. Gastroenterol. México 2012, 77, 82–90. [Google Scholar] [Green Version]
- Mehler, P.S.; Linas, S. Use of a proton-pump inhibitor for metabolic disturbances associated with anorexia nervosa. N. Engl. J. Med. 2002, 347, 373–374. [Google Scholar] [PubMed]
- Walder, A.; Baumann, P. Cardiac Left Bundle Branch Block and Pancytopenia in Anorexia Nervosa: Higher Risk with Mirtazapine and Pantoprazole? Case Report. Pharmacopsychiatry 2009, 42, 79–81. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Fukudo, S. Gastrointestinal symptoms and disorders in patients with eating disorders. Clin. J. Gastroenterol. 2015, 8, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, B.L. Feeding Systems and the Gut Microbiome: Gut-Brain Interactions with Relevance to Psychiatric Conditions. Psychosomatics 2017, 58, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Hanachi, M.; Manichanh, C.; Schoenenberger, A.; Pascal, V.; Levenez, F.; Cournède, N.; Doré, J.; Melchior, J.-C. Altered host-gut microbes symbiosis in severely malnourished anorexia nervosa (AN) patients undergoing enteral nutrition: An explicative factor of functional intestinal disorders? Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Schwensen, H.F.; Kan, C.; Treasure, J.; Høiby, N.; Sjögren, M. A systematic review of studies on the faecal microbiota in anorexia nervosa: Future research may need to include microbiota from the small intestine. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2018, 23, 399–418. [Google Scholar] [CrossRef] [PubMed]
- Misra, M.; Klibanski, A. Endocrine consequences of anorexia nervosa. Lancet Diabetes Endocrinol. 2014, 2, 581–592. [Google Scholar] [CrossRef] [Green Version]
- Schorr, M.; Miller, K.K. The endocrine manifestations of anorexia nervosa: Mechanisms and management. Nat. Rev. Endocrinol. 2017, 13, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Fazeli, P.K.; Lawson, E.A.; Prabhakaran, R.; Miller, K.K.; Donoho, D.A.; Clemmons, D.R.; Herzog, D.B.; Misra, M.; Klibanski, A. Effects of Recombinant Human Growth Hormone in Anorexia Nervosa: A Randomized, Placebo-Controlled Study. J. Clin. Endocrinol. Metab. 2010, 95, 4889–4897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Léger, J.; Fjellestad-Paulsen, A.; Bargiacchi, A.; Doyen, C.; Ecosse, E.; Carel, J.-C.; Le Heuzey, M.-F. Can growth hormone treatment improve growth in children with severe growth failure due to anorexia nervosa? A preliminary pilot study. Endocr. Connect. 2017, 6, 839–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, M.; Katzman, D.K.; Estella, N.M.; Eddy, K.T.; Weigel, T.; Goldstein, M.A.; Miller, K.K.; Klibanski, A. Impact of Physiologic Estrogen Replacement on Anxiety Symptoms, Body Shape Perception, and Eating Attitudes in Adolescent Girls with Anorexia Nervosa: Data from a Randomized Controlled Trial. J. Clin. Psychiatry 2013, 74, e765–e771. [Google Scholar] [CrossRef] [PubMed]
- Germain, N.; Fauconnier, A.; Klein, J.-P.; Wargny, A.; Khalfallah, Y.; Papastathi-Boureau, C.; Estour, B.; Galusca, B. Pulsatile gonadotropin-releasing hormone therapy in persistent amenorrheic weight-recovered anorexia nervosa patients. Fertil. Steril. 2017, 107, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Welt, C.K.; Smith, P.; Mantzoros, C.S. Recombinant Human Leptin in Women with Hypothalamic Amenorrhea. N. Engl. J. Med. 2004, 351, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Modan-Moses, D.; Yaroslavsky, A.; Kochavi, B.; Toledano, A.; Segev, S.; Balawi, F.; Mitrany, E.; Stein, D. Linear Growth and Final Height Characteristics in Adolescent Females with Anorexia Nervosa. PLoS ONE 2012, 7, e45504. [Google Scholar] [CrossRef] [PubMed]
- Nehring, I.; Kewitz, K.; von Kries, R.; Thyen, U. Long-term effects of enteral feeding on growth and mental health in adolescents with anorexia nervosa—Results of a retrospective German cohort study. Eur. J. Clin. Nutr. 2014, 68, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Rozé, C.; Doyen, C.; Le Heuzey, M.-F.; Armoogum, P.; Mouren, M.-C.; Léger, J. Predictors of late menarche and adult height in children with anorexia nervosa. Clin. Endocrinol. 2007, 67, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Skolnick, A.; Schulman, R.C.; Galindo, R.J.; Mechanick, J.I. The endocrinopathies of male anorexia nervosa: Case series. AACE Clin. Case Rep. 2016, 2, e351–e357. [Google Scholar] [CrossRef] [PubMed]
- Dempfle, A.; Herpertz-Dahlmann, B.; Timmesfeld, N.; Schwarte, R.; Egberts, K.M.; Pfeiffer, E.; Fleischhaker, C.; Wewetzer, C.; Bühren, K. Predictors of the resumption of menses in adolescent anorexia nervosa. BMC Psychiatry 2013, 13, 308. [Google Scholar] [CrossRef] [PubMed]
- Chui, H.T.; Christensen, B.K.; Zipursky, R.B.; Richards, B.A.; Hanratty, M.K.; Kabani, N.J.; Mikulis, D.J.; Katzman, D.K. Cognitive Function and Brain Structure in Females with a History of Adolescent-Onset Anorexia Nervosa. Pediatrics 2008, 122, e426–e437. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.L.; Mantzoros, C.S. Role of leptin in energy-deprivation states: Normal human physiology and clinical implications for hypothalamic amenorrhoea and anorexia nervosa. Lancet 2005, 366, 74–85. [Google Scholar] [CrossRef]
- Brown, L.M.; Clegg, D.J. Estrogen and Leptin Regulation of Endocrinological Features of Anorexia Nervosa. Neuropsychopharmacology 2013, 38, 237. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.; Aldridge, V.; Clark, E.M.; Misra, M.; Micali, N. A systematic review and meta-analysis of the association between eating disorders and bone density. Osteoporos. Int. 2016, 27, 1953–1966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, M.; Le Clair, M.; Mendes, N.; Miller, K.K.; Lawson, E.; Meenaghan, E.; Weigel, T.; Ebrahimi, S.; Herzog, D.B.; Klibanski, A. Use of SSRIs may Impact Bone Density in Adolescent and Young Women with Anorexia Nervosa. CNS Spectr. 2010, 15, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.K.; Lee, E.E.; Lawson, E.A.; Misra, M.; Minihan, J.; Grinspoon, S.K.; Gleysteen, S.; Mickley, D.; Herzog, D.; Klibanski, A. Determinants of Skeletal Loss and Recovery in Anorexia Nervosa. J. Clin. Endocrinol. Metab. 2006, 91, 2931–2937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman, D.; Crisp, A.; Rooney, B.; Rackow, C.; Atkinson, R.; Patel, S. Bone density of women who have recovered from anorexia nervosa. Int. J. Eat. Disord. 2000, 28, 107–112. [Google Scholar] [CrossRef]
- Castro, J.; Toro, J.; Lázaro, L.; Pons, F.; Halperin, I. Bone Mineral Density in Male Adolescents with Anorexia Nervosa. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Seeman, E.; Szmukler, G.I.; Formica, C.; Tsalamandris, C.; Mestrovic, R. Osteoporosis in anorexia nervosa: The influence of peak bone density, bone loss, oral contraceptive use, and exercise. J. Bone Min. Res. 2009, 7, 1467–1474. [Google Scholar] [CrossRef] [PubMed]
- Elkazaz, A.Y.; Salama, K. The effect of oral contraceptive different patterns of use on circulating IGF-1 and bone mineral density in healthy premenopausal women. Endocrine 2015, 48, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Hergenroeder, A.C.; Smith, E.O.; Shypailo, R.; Jones, L.A.; Klish, W.J.; Ellis, K. Bone mineral changes in young women with hypothalamic amenorrhea treated with oral contraceptives, medroxyprogesterone, or placebo over 12 months. Am. J. Obs. Gynecol. 1997, 176, 1017–1025. [Google Scholar] [CrossRef]
- Misra, M.; Katzman, D.; Miller, K.K.; Mendes, N.; Snelgrove, D.; Russell, M.; Goldstein, M.A.; Ebrahimi, S.; Clauss, L.; Weigel, T.; et al. Physiologic estrogen replacement increases bone density in adolescent girls with anorexia nervosa. J. Bone Min. Res. 2011, 26, 2430–2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golden, N.H.; Iglesias, E.A.; Jacobson, M.S.; Carey, D.; Meyer, W.; Schebendach, J.; Hertz, S.; Shenker, I.R. Alendronate for the Treatment of Osteopenia in Anorexia Nervosa: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Endocrinol. Metab. 2005, 90, 3179–3185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.K.; Grieco, K.A.; Mulder, J.; Grinspoon, S.; Mickley, D.; Yehezkel, R.; Herzog, D.B.; Klibanski, A. Effects of Risedronate on Bone Density in Anorexia Nervosa. J. Clin. Endocrinol. Metab. 2004, 89, 3903–3906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.K.; Meenaghan, E.; Lawson, E.A.; Misra, M.; Gleysteen, S.; Schoenfeld, D.; Herzog, D.; Klibanski, A. Effects of Risedronate and Low-Dose Transdermal Testosterone on Bone Mineral Density in Women with Anorexia Nervosa: A Randomized, Placebo-Controlled Study. J. Clin. Endocrinol. Metab. 2011, 96, 2081–2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.K.; Grieco, K.A.; Klibanski, A. Testosterone Administration in Women with Anorexia Nervosa. J. Clin. Endocrinol. Metab. 2005, 90, 1428–1433. [Google Scholar] [CrossRef] [PubMed]
- DiVasta, A.D.; Feldman, H.A.; Beck, T.J.; LeBoff, M.S.; Gordon, C.M. Does Hormone Replacement Normalize Bone Geometry in Adolescents with Anorexia Nervosa? J. Bone Min. Res. Off. J. Am. Soc. Bone Min. Res. 2014, 29, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Grinspoon, S.; Baum, H.; Lee, K.; Anderson, E.; Herzog, D.; Klibanski, A. Effects of short-term recombinant human insulin-like growth factor I administration on bone turnover in osteopenic women with anorexia nervosa. J. Clin. Endocrinol. Metab. 1996, 81, 3864–3870. [Google Scholar] [PubMed]
- Grinspoon, S.; Thomas, L.; Miller, K.; Herzog, D.; Klibanski, A. Effects of Recombinant Human IGF-I and Oral Contraceptive Administration on Bone Density in Anorexia Nervosa. J. Clin. Endocrinol. Metab. 2002, 87, 2883–2891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.K.; Perlis, R.H.; Papakostas, G.I.; Mischoulon, D.; Iosifescu, D.V.; Brick, D.J.; Fava, M. Low-dose Transdermal Testosterone Augmentation Therapy Improves Depression Severity in Women. CNS Spectr. 2009, 14, 688–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazeli, P.K.; Wang, I.S.; Miller, K.K.; Herzog, D.B.; Misra, M.; Lee, H.; Finkelstein, J.S.; Bouxsein, M.L.; Klibanski, A. Teriparatide Increases Bone Formation and Bone Mineral Density in Adult Women with Anorexia Nervosa. J. Clin. Endocrinol. Metab. 2014, 99, 1322–1329. [Google Scholar] [CrossRef] [PubMed]
- Iketani, T.; Kiriike, N.; Stein, M.B.; Nagao, K.; Nagata, T.; Minamikawa, N.; Shidao, A.; Fukuhara, H. Effect of menatetrenone (vitamin K2) treatment on bone loss in patients with anorexia nervosa. Psychiatry Res. 2003, 117, 259–269. [Google Scholar] [CrossRef]
- Misra, M.; Tsai, P.; Anderson, E.J.; Hubbard, J.L.; Gallagher, K.; Soyka, L.A.; Miller, K.K.; Herzog, D.B.; Klibanski, A. Nutrient intake in community-dwelling adolescent girls with anorexia nervosa and in healthy adolescents. Am. J. Clin. Nutr. 2006, 84, 698–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veronese, N.; Solmi, M.; Rizza, W.; Manzato, E.; Sergi, G.; Santonastaso, P.; Caregaro, L.; Favaro, A.; Correll, C.U. Vitamin D status in anorexia nervosa: A meta-analysis: Vitamin D in Anorexia Nervosa. Int. J. Eat. Disord. 2015, 48, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Gatti, D.; El Ghoch, M.; Viapiana, O.; Ruocco, A.; Chignola, E.; Rossini, M.; Giollo, A.; Idolazzi, L.; Adami, S.; Dalle Grave, R. Strong relationship between vitamin D status and bone mineral density in anorexia nervosa. Bone 2015, 78, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Giollo, A.; Idolazzi, L.; Caimmi, C.; Fassio, A.; Bertoldo, F.; Dalle Grave, R.; El Ghoch, M.; Calugi, S.; Bazzani, P.V.; Viapiana, O.; et al. Vitamin D levels strongly influence bone mineral density and bone turnover markers during weight gain in female patients with anorexia nervosa: GIOLLO et al. Int. J. Eat. Disord. 2017, 50, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Kamimura, M.; Koiwai, H.; Kato, H. Adequate nutrition status important for bone mineral density improvement in a patient with anorexia nervosa. Clin. Risk Manag. 2018, 14, 945–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.J.B.; Kruszka, B.; Delaney, J.A.C.; He, K.; Burke, G.L.; Alonso, A.; Bild, D.E.; Budoff, M.; Michos, E.D. Calcium Intake from Diet and Supplements and the Risk of Coronary Artery Calcification and its Progression Among Older Adults: 10-Year Follow-up of the Multi-Ethnic Study of Atherosclerosis (MESA). J. Am. Heart Assoc. Cardiovasc. Cereb. Dis. 2016, 5, e003815. [Google Scholar] [CrossRef] [PubMed]
- Giel, K.; Zipfel, S.; Hallschmid, M. Oxytocin and Eating Disorders: A Narrative Review on Emerging Findings and Perspectives. Curr. Neuropharmacol. 2018, 16, 1111–1121. [Google Scholar] [CrossRef] [PubMed]
- Zipfel, S.; Giel, K.E.; Bulik, C.M.; Hay, P.; Schmidt, U. Anorexia nervosa: Aetiology, assessment, and treatment. Lancet Psychiatry 2015, 2, 1099–1111. [Google Scholar] [CrossRef]
- Støving, R.K. Mechanisms in endocrinology: Anorexia nervosa and endocrinology: A clinical update. Eur. J. Endocrinol. 2019, 180, R9–R27. [Google Scholar] [CrossRef] [PubMed]
- Bargiacchi, A.; Clarke, J.; Paulsen, A.; Leger, J. Refeeding in anorexia nervosa. Eur. J. Pediatr. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.K.; Watson, H.J.; Harper, E.; McCormack, J.; Nguyen, T. Psychotropic drug prescribing in an Australian specialist child and adolescent eating disorder service: A retrospective study. J. Eat. Disord. 2013, 1, 27. [Google Scholar] [CrossRef] [PubMed]
- Mattar, L.; Huas, C.; Duclos, J.; Apfel, A.; Godart, N. Relationship between malnutrition and depression or anxiety in Anorexia Nervosa: A critical review of the literature. J. Affect. Disord. 2011, 132, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Himmerich, H.; Joaquim, M.; Bentley, J.; Kan, C.; Dornik, J.; Treasure, J.; Schmidt, U. Psychopharmacological options for adult patients with anorexia nervosa: The patients’ and carers’ perspectives. CNS Spectr. 2018, 23, 251–252. [Google Scholar] [CrossRef] [PubMed]
- Woodside, B.D.; Staab, R. Management of psychiatric comorbidity in anorexia nervosa and bulimia nervosa. CNS Drugs 2006, 20, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Treasure, J.; Stein, D.; Maguire, S. Has the time come for a staging model to map the course of eating disorders from high risk to severe enduring illness? An examination of the evidence. Early Interv. Psychiatry 2015, 9, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Wildes, J.E.; Marcus, M.D.; Crosby, R.D.; Ringham, R.M.; Dapelo, M.M.; Gaskill, J.A.; Forbush, K.T. The clinical utility of personality subtypes in patients with anorexia nervosa. J. Consult. Clin. Psychol. 2011, 79, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, S.; Jaussent, I.; Maimoun, L.; Ryst, A.; Seneque, M.; Villain, L.; Hamroun, D.; Lefebvre, P.; Renard, E.; Courtet, P. Associations between adverse childhood experiences and clinical characteristics of eating disorders. Sci. Rep. 2016, 6, 35761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dechartres, A.; Huas, C.; Godart, N.; Pousset, M.; Pham, A.; Divac, S.M.; Rouillon, F.; Falissard, B. Outcomes of empirical eating disorder phenotypes in a clinical female sample: Results from a latent class analysis. Psychopathology 2011, 44, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Wildes, J.E.; Forbush, K.T.; Markon, K.E. Characteristics and stability of empirically derived anorexia nervosa subtypes: Towards the identification of homogeneous low-weight eating disorder phenotypes. J. Abnorm. Psychol. 2013, 122, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- Goldschmidt, A.B.; Wonderlich, S.A.; Crosby, R.D.; Cao, L.; Engel, S.G.; Lavender, J.M.; Mitchell, J.E.; Crow, S.J.; Peterson, C.B.; Le Grange, D. Latent profile analysis of eating episodes in anorexia nervosa. J. Psychiatr. Res. 2014, 53, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levinson, C.A.; Vanzhula, I.; Brosof, L.C. Longitudinal and personalized networks of eating disorder cognitions and behaviors: Targets for precision intervention a proof of concept study. Int. J. Eat. Disord. 2018, 51, 1233–1243. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, K.A.; Woodside, B.; Downar, J. Targeting Neural Endophenotypes of Eating Disorders with Non-invasive Brain Stimulation. Front. Neurosci. 2016, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Campbell, P.; Brunton, G.; Hunt, H.; Estcourt, L. Selecting and implementing overview methods: Implications from five exemplar overviews. Syst. Rev. 2017, 6, 145. [Google Scholar] [CrossRef] [PubMed]
- Ballard, M.; Montgomery, P. Risk of bias in overviews of reviews: A scoping review of methodological guidance and four-item checklist: Review of Methodological Guidance for Overviews of Reviews & Four-Item Checklist. Res. Synth. Methods 2017, 8, 92–108. [Google Scholar] [PubMed]


{kind=link}
| Recommendations |
|---|
| Medication for anorexia nervosa |
| 1.3.24 Do not offer medication as the sole treatment for anorexia nervosa. |
| Dietary advice for people with anorexia nervosa […] |
| 1.3.21 Encourage people with anorexia nervosa to take an age-appropriate oral multi-vitamin and multi-mineral supplement until their diet includes enough to meet their dietary reference values. |
| Comorbid mental health problems |
| 1.8.12 When deciding in which order to treat an eating disorder and a comorbid mental health condition (in parallel, as part of the same treatment plan or one after the other), take the following into account: |
| - The severity and complexity of the eating disorder and comorbidity. |
| - The person’s level of functioning. |
| - The preferences of the person with the eating disorder and (if appropriate) those of their family members or carers. |
| 1.8.13 Refer to the NICE guidelines on specific mental health problems for further guidance on treatment. |
| Medication risk management |
| 1.8.14 When prescribing medication for people with an eating disorder, and comorbid mental or physical health conditions, take into account the impact that malnutrition and compensatory behaviours can have on medication effectiveness and the risk of side effects. |
| 1.8.15 When prescribing for people with an eating disorder and comorbidity assess how the eating disorder will affect medication adherence (for example, for medication that can affect body weight). |
| 1.8.16 When prescribing for people with an eating disorder, take into account the risks of medication that can compromise physical health due to pre-existing medical complications. |
| 1.8.17 Offer electrocardiogram (ECG) monitoring for people with an eating disorder who are taking medication that could compromise cardiac functioning (including medication that could cause electrolyte imbalance, bradycardia below 40 beats per minute, hypokalaemia, or a prolonged QT interval). Substance or medication misuse 1.8.18 For people with an eating disorder, who are misusing substances, or over-the-counter or prescribed medication, provide treatment for the eating disorder unless the substance misuse is interfering with this treatment. 1.8.19 If substance misuse or medication is interfering with treatment, consider a multidisciplinary approach with substance misuse services. Growth and development 1.8.20 Seek specialist paediatric or endocrinology advice for delayed physical development or faltering growth in children and young people with an eating disorder. |
| Parameters | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Patients | - AN 1 (with or without the mention of the restrictive or binging/purging types) - Human studies - All ages | - BN 2, BED 3, other ED 4 - Mixed eating disorder samples (AN and any other ED) |
| Interventions | - Medication for AN (psychotropic or somatic or nutritional) | - Medication for refeeding complications |
| Comparators | - All comparison groups (placebo or active drug or treatment as usual) | |
| Outcomes | - All criteria linked to ED symptoms, psychiatric -and somatic symptoms, and nutritional aspects, as appropriate | |
| Study design | - Meta-analyses and systematic reviews with a detailed methodology, including RCTs 5 and/or open trials | - Narrative or qualitative reviews - Overviews - Reviews of unpublished data |
| Period considered | - Papers published between September 2011 (since the publication of The World Federation of Societies of Biological Psychiatry Guidelines for the Pharmacological Treatment of Eating Disorders) [6] and 30th January 2019 | |
| Language | - English and French |
| Author | Year | Method | Database | Type of Study | Participant Age | Review Period from | Review Period to | Medication |
|---|---|---|---|---|---|---|---|---|
| Aigner, M. et al. [6] | 2011 | Systematic review | MEDLINE | 45 studies = 19 open or case studies 26 RCTs | All | 1977 | 2011 | Antidepressants; Antipsychotics (typical and atypical); Prokinetic agents; Cannabinoids; Antihistaminics; Naltrexone; Clonidine; Tube feeding; Lithium; Growth Hormone; Zinc |
| Flament, M. et al. [37] | 2012 | Systematic review | MEDLINE; PsycINFO | 11 RCTs; if none were available (e.g. for paediatric EDs) open trials or case reports suggesting benefits; systemic reviews; meta-analyses; and guidelines | All | 1960 | May 2010 | Antidepressants; Antipsychotics (typical and atypical); Mood stabilizers and anticonvulsivants; Prokinetic agents; Opiate agonists; Appetite enhancers |
| Kishi, T. et al. [27] | 2012 | Meta-analysis | PubMed; PsycINFO; Cochrane | 8 RCTs | All | No limitation | March 2012 | Antipsychotics (typical and atypical) |
| Lebow et al. [38] | 2013 | Meta-analysis | Cochrane; MEDLINE; Embase; Scopus; Web of Science; PsychINFO | 8 RCTs on atypical antipsychotics (in any form, used for at least 4 weeks) compared to any control intervention on BMI, eating disorder, and psychiatric symptoms in adolescents and adults with AN Eligible studies assessed BMI before, during, and/or after treatment. We excluded studies that enrolled patients who had a primary psychotic disorder. | All | 1998 | November 2011 | Atypical antipsychotics |
| Lebow, J. et al. [39] | 2013 | Systematic review | Not reported | 10 studies = 8 RCTs, 2 prospective cohort studies | 11–42.5 years | Not reported | Not reported | Estrogen therapies |
| Watson, T. et al. [40] | 2013 | Systematic review | MEDLINE; PsycINFO; The Cumulative Index to Nursing and Applied Health; Educational Resources Information Center; National Agricultural OnLine; Embase Scopus Access; Cochrane Collaboration libraries | 32 RCTs | All | 1960 | October 2011 | Antidepressants; Antipsychotics; Cyproheptadine; Recombinant human growth hormone (rhGH); Risedronate; Testosterone; Nasogastric tube |
| De Vos et al. [41] | 2014 | Meta-analysis | PubMed; PsycINFO; Embase; Cochrane Library | 18 studies = (a) RCTs and (b) comparing pharmacotherapy with a placebo controlled condition and reported on (c) patients with Anorexia Nervosa and an age minimum of 12 years. Outcome was measured in (d) terms of weight gain | All | No limitation | October 2012 | Antidepressants; Antipsychotics; Hormonal therapy |
| Rocks, T. et al. [42] | 2014 | Systematic review | PubMed; Scopus; Web of Science | 7 observational studies | ≤19 years | No limitation | May 2012 | Nutrition therapy |
| Dold et al. [43] | 2015 | Meta-analysis | ClinicalTrials.gov; Clinicaltrialsregister.eu; Cochrane Central Register of Controlled Trials (CENTRAL); Embase; PubMed/MEDLINE; PsycINFO | 7 RCTs second generation antipsychotics efficacy, acceptability, and tolerability in comparison to placebo/no treatment, even unpublished studies | All | No limitation | August 2014 | Atypical antipsychotics |
| El Ghoch, M. et al. [44] | 2016 | Systematic review | PubMed | 19 studies = 11 prospective non-controlled, 4 prospective controlled, 4 retrospective non-controlled | 11–19 years | No limitation | No limitation | Weight gain and restoration |
| Frank, G.K. et al. [45] | 2016 | Systematic review | National Center for Biotechnology Information database | 66 studies = 25 double-blind, placebo-controlled studies; 7 double-blind, placebo-controlled crossover studies; 5 single-blind, placebo-controlled studies; 23 open-label studies; and 6 retrospective systematic chart reviews | All | No limitation | 2014 | Antidepressants; Antipsychotics (typical and atypical); Mood Stabilizers: Zinc; Opiates and Cannabinoids; Benzodiazepines and Alpha 2 Adrenergics; D-Cyclocerine; Amantadine; DHEA; Ghrelin; Growth Hormone; Testosterone; Estrogen |
| Garber, A.K. et al. [46] | 2016 | Systematic review | PubMed; Scopus; PsycINFO; Clinical trials database | 27 studies = 1 RCT, 6 prospective, 14 retrospective, 6 observational | 13–38 years | 1960 | 15 March 2015 | Refeeding approaches |
| Kells, M. et al. [47] | 2016 | Systematic review (integrative) | PubMed; Embase; Cochrane CINAHL | 18 studies = 2 RCTs, 6 retrospective, 5 cohort, 1 observational, 4 case reports | 11–57 years | No limitation | May 2016 | Tube feeding |
| Miniati, M. et al. [48] | 2016 | Systematic review | MEDLINE; PsycINFO | 41 studies = 17 RCTs, 9 open trials, 12 case series and case reports, 2 retrospective observations, 1 single-blind RCT | Adults | January 1966 | January 2014 | Antidepressants; Antipsychotics (typical and atypical); Lithium; Clonidine; Cyproheptadine |
| Misra, M. et al. [49] | 2016 | Systematic review | PubMed | 20 studies = 10 RCTs, 8 prospective observational studies, 1 retrospective cohort study, 1 prospective study | 11–45 years | 1995 | 2015 | Weight gain and restoration, Estrogen replacement therapy, recombinant h-GH, recombinant h-IgF1, DHEA, Biphosphonates, Teriparatide |
| Robinson, L. et al. [50] | 2017 | Systematic review | MEDLINE; PsychINFO; Embase; Cochrane Database | 19 studies =10 double-blind RCTs, 2 prospective observational studies, 1 retrospective cohort study, 1 case-control study and 5 non-randomised control trials | All | No limitation | 3 March 2017 | DHEA, various OC (EE or EE/levonorgestrel or EE/progestin or EE/Norgestimate), various oestrogen replacement treatments (transdermal 17ßPE/progesterone or oral EE/progesterone), Teriparatide (TPt), Alendronate, rhIgF1, Menatetrenone (MED) (vitamin K2), risedronate, transdermal testosterone |
| Brockmeyer, T. et al. [51] | 2018 | Systematic review | PubMed; Scopus; Web of Science | 6 RCTs on medication (including one unpublished study) | All | October 2011 (post Watson 2012) | 31 December 2016 | Antipsychotics; Dronabinol; Tube feeding |
| Hale, M.D. et al. [52] | 2018 | Systematic review | PubMed; PsycINFO; CINAHL; Web of Science; Cochrane Library; Dissertations and Theses (ProQuest); Google Scholar | 19 open, prospective RCTs, non-randomized controlled trials, prospective cohort studies, retrospective chart reviews | All | No limitation | September 2017 | Tube feeding |
| Rizzo, S.M. et al. [53] | 2018 | Systematic review | PubMed; Scopus;Web of Science; PsycINFO | 10 studies = 1 RCT, 1 prospective cohort study, 8 retrospective cohort studies | 10–57 years | No limitation | May 2018 | Enteral Nutrition via Nasogastric Tube |
| Author | Study | Treatment Group | Daily Medication Dose | Length of Treatment | N | Mean Age ± SD (Years) | Results |
|---|---|---|---|---|---|---|---|
| Vandereycken and Pierloot, [77] 1982 | Double-blind placebo controlled crossover | pimozide placebo | 4 to 6 mg | 6 weeks | 18 | Non reported | Non-significant on weight gain |
| Vandereycken, [78] 1984 | Double-blind placebo controlled crossover | sulpiride /placebo sequence placebo /sulpiride sequence | 300 or 400 mg | 2–3 weeks | 99 | 23.2 ± 6.5 23.7 ± 9.6 | Non-significant on weight gain |
| Ruggiero et al., [65] 2001 | Open-label | clomipramine fluoxetine amisulpride | Mean= 57.7 ± 25.8 mg Mean = 26.0 ± 10.3 mg Mean= 50.0 ± 0.0 mg | 3 months | 10 13 12 | 23.7 ± 4.6 4.5 ± 5.1 24.3 ± 5.8 | No significant difference between groups in term of weight gain significant increase for fluoxetine and amisulpride groups |
| Cassano et al., [79] 2003 | Open label | haloperidol | Months 1–3 Mean = 1.2 ± 0.4 mg; Months 4–6 Mean = 1.1 ± 0.2 mg | 6 months | 13 | 22.8 ± 4.2 | BMI increased significantly in chronic and treatment-resistant patients |
| Mondraty et al., [80] 2005 | Double-blind placebo controlled | olanzapine chlorpromazine | 10 mg 50 mg | Mean = 46 ± 31 days Mean = 53 ± 26 days | 87 10 | 25.3 ± 7.42 5.3 ± 7.3 | No significant difference in weight gain |
| Brambilla et al., [81] 2007a | Double-blind placebo controlled | olanzapine and cognitive behaviour therapy and nutritional rehabilitation placebo and cognitive behavioural therapy and nutritional rehabilitation | 2.5 mg for 1 month; 5 mg for 2 months | 3 months | 10 | 23 ± 4.8 | No difference for weight gain |
| Brambilla et al., [82] 2007b | Double-blind placebo controlled | olanzapine and cognitive behavioural therapy placebo and cognitive behavioural therapy | 2.5 mg for 1 month; 5 mg for 2 months | 3 months | 15 15 | 23.7 ± 4.8 26.3 ± 8.5 | No difference for weight gain between groups greater improvement on the Eating Disorder Inventory ineffectiveness and maturity fear scores in the olanzapine group |
| Bissada et al., [83] 2008 | Double-blind placebo controlled | olanzapine placebo | Start = 2.5 mg; Max = 10 mg – flexible dose regimen | 10 weeks | 16 18 | 23.6 ± 6.5 29.7 ± 11.6 | Olanzapine: greater weight increase and faster achievement of weight goals |
| Attia et al., [84] 2011 | Double-blind placebo controlled | olanzapine placebo | Start = 2.5 mg; Last 4 Weeks = 10 mg | 8 weeks | 11 12 | 27.7 ± 9.1 | Olanzapine was associated with a small but significant increase in BMI compared to placebo |
| Kafantaris et al., [85] 2011 | Double-blind placebo controlled | olanzapine and psychotherapy placebo and psychotherapy | Start = 2.5 mg; week 4 target = 10 mg | 10 weeks | 10 10 | 16.4 ± 2.2 18.1 ± 2.0 | No significant difference in weight gain between groups |
| Hagman et al., [86] 2011 | Double-blind placebo controlled | risperidone placebo | Mean = 2.5 ± 1.2 mg Mean = 3.0 ± 1.0 mg | 17 weeks | 182 2 | 16.2 ± 2.5 15.8 ± 2.3 | No significant difference in weight gain between groups; the risperidone group showed greater reduction in drive for thinness over the first half of the study, but this was not sustained |
| Powers et al., [87] 2012 | Double-blind placebo controlled | quetiapine placebo | Mean = 177.7 ± 90.8 mg | 8 weeks | 46 | 34 ± 14.5 | No difference between quetiapine and placebo on weight, eating disorders, anxiety and depressive symptoms |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanchet, C.; Guillaume, S.; Bat-Pitault, F.; Carles, M.-E.; Clarke, J.; Dodin, V.; Duriez, P.; Gerardin, P.; Hanachi-Guidoum, M.; Iceta, S.; et al. Medication in AN: A Multidisciplinary Overview of Meta-Analyses and Systematic Reviews. J. Clin. Med. 2019, 8, 278. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020278
Blanchet C, Guillaume S, Bat-Pitault F, Carles M-E, Clarke J, Dodin V, Duriez P, Gerardin P, Hanachi-Guidoum M, Iceta S, et al. Medication in AN: A Multidisciplinary Overview of Meta-Analyses and Systematic Reviews. Journal of Clinical Medicine. 2019; 8(2):278. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020278
Chicago/Turabian StyleBlanchet, Corinne, Sébastien Guillaume, Flora Bat-Pitault, Marie-Emilie Carles, Julia Clarke, Vincent Dodin, Philibert Duriez, Priscille Gerardin, Mouna Hanachi-Guidoum, Sylvain Iceta, and et al. 2019. "Medication in AN: A Multidisciplinary Overview of Meta-Analyses and Systematic Reviews" Journal of Clinical Medicine 8, no. 2: 278. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020278