The Clinical Significance of Programmed Death-1, Regulatory T Cells and Myeloid Derived Suppressor Cells in Patients with Nontuberculous Mycobacteria-Lung Disease

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Patient Enrollment
2.2. Isolation of Peripheral Blood Mononuclear Cells (PBMCs)
2.3. Flow Cytometry of PBMCs
2.4. NTM Species Identification
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. The Demographics of All Participants
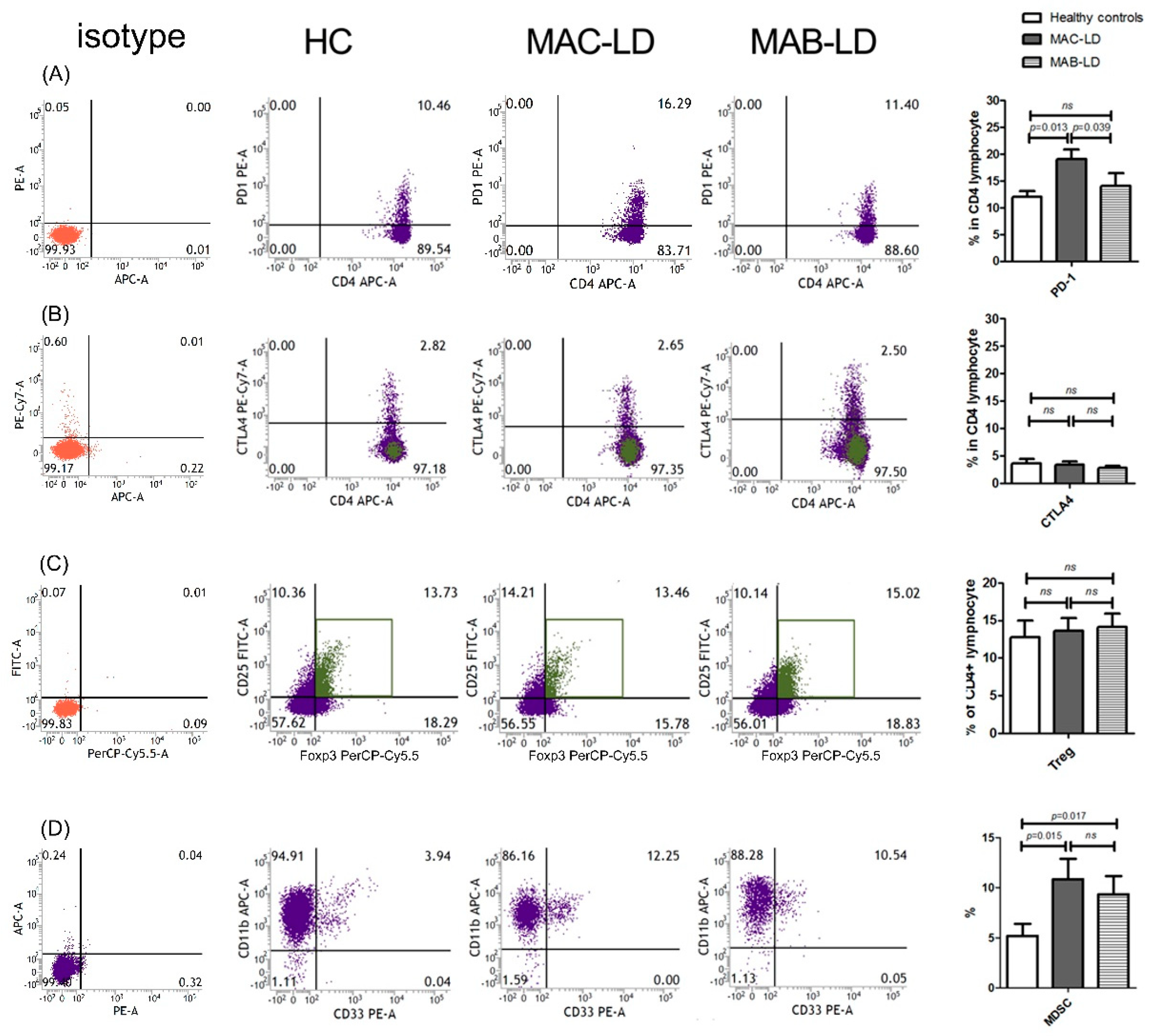
3.2. PD-1+CD4+ Lymphocytes, Treg Cells, and MDSCs in All Participants
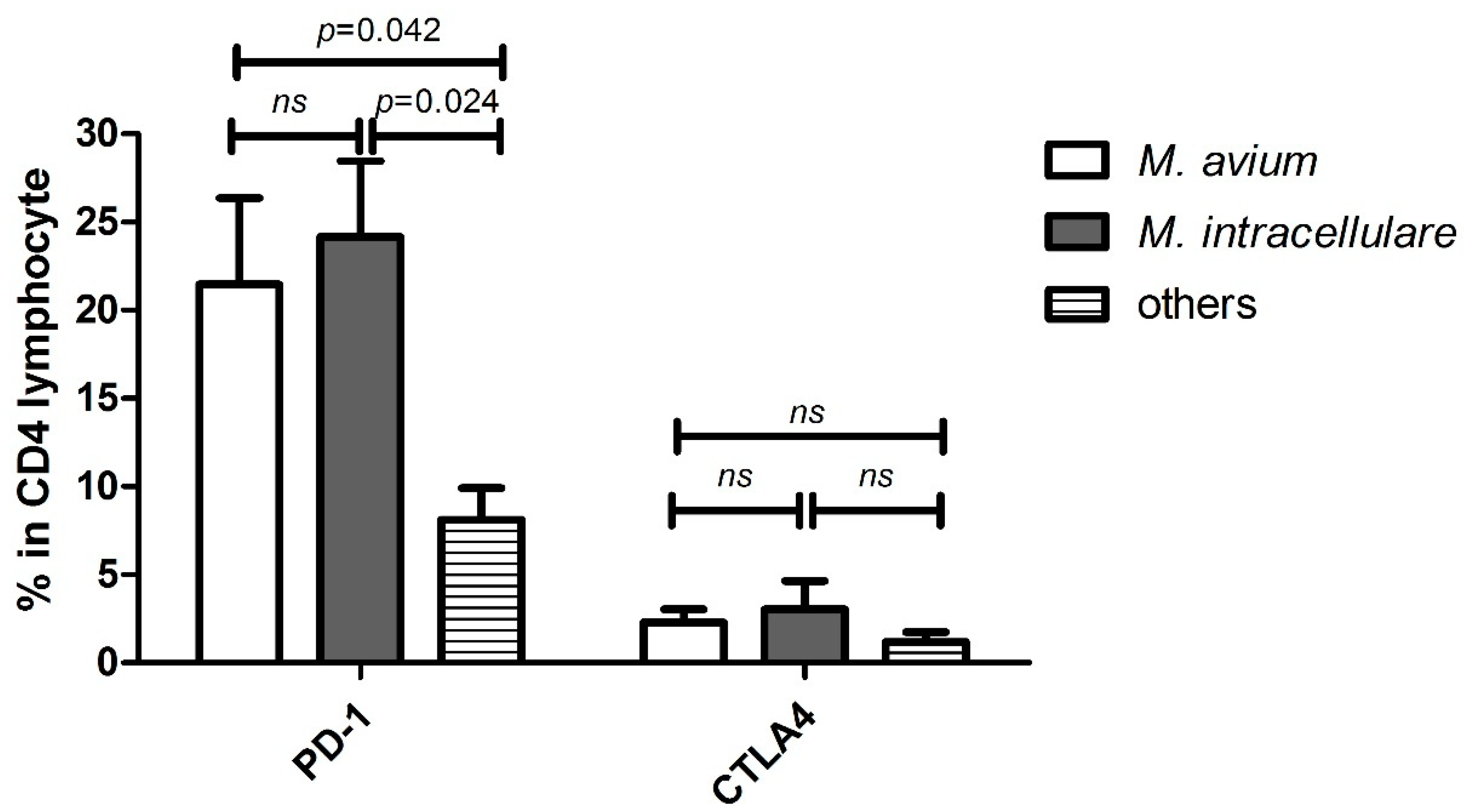
3.3. Differences among Different MAC Subspecies
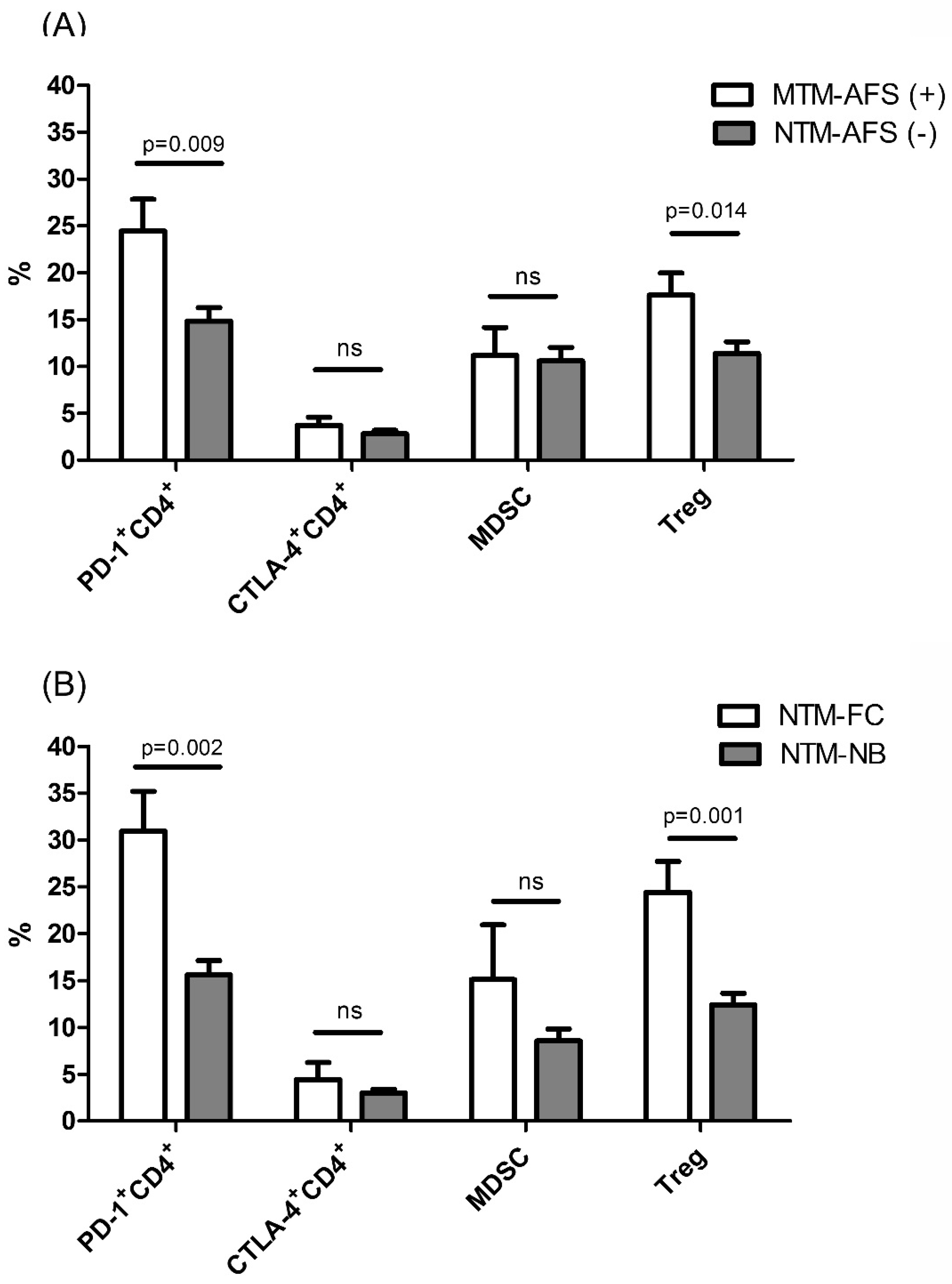
3.4. The Influence of Mycobacteria Load on Immune Exhaustion
3.5. Differences between Initial Radiographic Patterns
3.6. Radiographic Progression in NTM-LD and The Predictors
3.7. Follow-up Immune Regulatory Cells for Radiographic Progression in NTM-LD
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
Consent for Publication
Availability of Data and Material
References
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef] [PubMed]
- Menzies, D.; Nahid, P. Update in tuberculosis and nontuberculous mycobacterial disease 2012. Am. J. Respir. Crit. Care Med. 2013, 188, 923–927. [Google Scholar] [CrossRef]
- Prevots, D.R.; Shaw, P.A.; Strickland, D.; Jackson, L.A.; Raebel, M.A.; Blosky, M.A.; Montes de Oca, R.; Shea, Y.R.; Seitz, A.E.; Holland, S.M.; et al. Nontuberculous Mycobacterial Lung Disease Prevalence at Four Integrated Healthcare Delivery Systems. Am. J. Respir. Crit. Care Med. 2010, 182, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Tan, C.K.; Chou, C.H.; Hsu, H.L.; Liao, C.H.; Huang, Y.T.; Yang, P.C.; Luh, K.T.; Hsueh, P.R. Increasing incidence of nontuberculous mycobacteria, Taiwan, 2000-2008. Emerg. Infect. Dis. 2010, 16, 294–296. [Google Scholar] [CrossRef]
- Hoefsloot, W.; van Ingen, J.; Andrejak, C.; Angeby, K.; Bauriaud, R.; Bemer, P.; Beylis, N.; Boeree, M.J.; Cacho, J.; Chihota, V.; et al. The geographic diversity of nontuberculous mycobacteria isolated from pulmonary samples: An NTM-NET collaborative study. Eur. Respir. J. 2013, 42, 1604–1613. [Google Scholar] [CrossRef]
- Koh, W.J.; Kwon, O.J.; Jeon, K.; Kim, T.S.; Lee, K.S.; Park, Y.K.; Bai, G.H. Clinical significance of nontuberculous mycobacteria isolated from respiratory specimens in Korea. Chest 2006, 129, 341–348. [Google Scholar] [CrossRef]
- van Ingen, J.; Bendien, S.A.; de Lange, W.C.; Hoefsloot, W.; Dekhuijzen, P.N.; Boeree, M.J.; van Soolingen, D. Clinical relevance of non-tuberculous mycobacteria isolated in the Nijmegen-Arnhem region, The Netherlands. Thorax 2009, 64, 502–506. [Google Scholar] [CrossRef] [Green Version]
- Chan, E.D.; Iseman, M.D. Underlying host risk factors for nontuberculous mycobacterial lung disease. Semin. Respir. Crit. Care Med. 2013, 34, 110–123. [Google Scholar]
- Vankayalapati, R.; Wizel, B.; Samten, B.; Griffith, D.E.; Shams, H.; Galland, M.R.; Von Reyn, C.F.; Girard, W.M.; Wallace, R.J., Jr.; Barnes, P.F. Cytokine profiles in immunocompetent persons infected with Mycobacterium avium complex. J. Infect. Dis. 2001, 183, 478–484. [Google Scholar] [CrossRef]
- Shu, C.C.; Wang, J.Y.; Wu, M.F.; Wu, C.T.; Lai, H.C.; Lee, L.N.; Chiang, B.L.; Yu, C.J. Attenuation of lymphocyte immune responses during Mycobacterium avium complex-induced lung disease due to increasing expression of programmed death-1 on lymphocytes. Sci. Rep. 2017, 7, 42004. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, T.; Chikuma, S.; Iwai, Y.; Fagarasan, S.; Honjo, T. A rheostat for immune responses: The unique properties of PD-1 and their advantages for clinical application. Nat. Immunol. 2013, 14, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Bluestone, J.A.; Abbas, A.K. Natural versus adaptive regulatory T cells. Nat. Rev. Immunol. 2003, 3, 253–257. [Google Scholar] [CrossRef]
- Murakami, M.; Sakamoto, A.; Bender, J.; Kappler, J.; Marrack, P. CD25+CD4+ T cells contribute to the control of memory CD8+ T cells. Proc. Natl. Acad. Sci. USA 2002, 99, 8832–8837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabrilovich, D.I.; Nagaraj, S. Myeloid-derived suppressor cells as regulators of the immune system. Nat. Rev. Immunol. 2009, 9, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Yang, C.Y.; Chang, K.P.; Keng, L.T.; Yen, D.H.; Wang, J.Y.; Wu, H.D.; Lee, L.N.; Yu, C.J. Factors associated with lung function decline in patients with non-tuberculous mycobacterial pulmonary disease. PLoS One 2013, 8, e58214. [Google Scholar] [CrossRef]
- Kitada, S.; Uenami, T.; Yoshimura, K.; Tateishi, Y.; Miki, K.; Miki, M.; Hashimoto, H.; Fujikawa, T.; Mori, M.; Matsuura, K.; et al. Long-term radiographic outcome of nodular bronchiectatic Mycobacterium avium complex pulmonary disease. Int. J. Tuberc. Lung Dis. 2012, 16, 660–664. [Google Scholar] [CrossRef]
- Shu, C.C.; Lee, C.H.; Hsu, C.L.; Wang, J.T.; Wang, J.Y.; Yu, C.J.; Lee, L.N. Clinical characteristics and prognosis of nontuberculous mycobacterial lung disease with different radiographic patterns. Lung 2011, 189, 467–474. [Google Scholar] [CrossRef]
- Kalathil, S.G.; Lugade, A.A.; Pradhan, V.; Miller, A.; Parameswaran, G.I.; Sethi, S.; Thanavala, Y. T-regulatory cells and programmed death 1+ T cells contribute to effector T-cell dysfunction in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2014, 190, 40–50. [Google Scholar] [CrossRef]
- Pan, S.W.; Shu, C.C.; Feng, J.Y.; Wang, J.Y.; Chan, Y.J.; Yu, C.J.; Su, W.J. Microbiological persistence in patients with Mycobacterium avium complex lung disease: The predictors and the impact on radiographic progression. Clin. Infect. Dis. 2017, 65, 927–934. [Google Scholar] [CrossRef]
- Koh, W.J.; Jeong, B.H.; Jeon, K.; Lee, N.Y.; Lee, K.S.; Woo, S.Y.; Shin, S.J.; Kwon, O.J. Clinical significance of the differentiation between Mycobacterium avium and Mycobacterium intracellulare in M avium complex lung disease. Chest 2012, 142, 1482–1488. [Google Scholar] [CrossRef]
- Snider, G.L.; Doctor, L.; Demas, T.A.; Shaw, A.R. Obstructive airway disease in patients with treated pulmonary tuberculosis. Am. Rev. Respir. Dis. 1971, 103, 625–640. [Google Scholar]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Ann. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef]
- Wherry, E.J. T cell exhaustion. Nat. Immunol. 2011, 12, 492–499. [Google Scholar] [CrossRef]
- Singh, A.; Mohan, A.; Dey, A.B.; Mitra, D.K. Programmed death-1+ T cells inhibit effector T cells at the pathological site of miliary tuberculosis. Clin. Exp. Immunol. 2017, 187, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Boyle, D.P.; Zembower, T.R.; Reddy, S.; Qi, C. Comparison of Clinical Features, Virulence, and Relapse among Mycobacterium avium Complex Species. Am. J. Respir. Crit. Care Med. 2015, 191, 1310–1317. [Google Scholar] [CrossRef]
- Kim, S.J.; Choi, S.M.; Lee, J.; Lee, C.H.; Han, S.K.; Yim, J.J. Characteristics associated with progression in patients with of nontuberculous mycobacterial lung disease: A prospective cohort study. BMC Pulm. Med. 2017, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Belkaid, Y.; Rouse, B.T. Natural regulatory T cells in infectious disease. Nat. Immunol. 2005, 6, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Bronte, V.; Serafini, P.; Mazzoni, A.; Segal, D.M.; Zanovello, P. L-arginine metabolism in myeloid cells controls T-lymphocyte functions. Trends Immunol. 2003, 24, 302–306. [Google Scholar] [CrossRef]
- Srivastava, M.K.; Sinha, P.; Clements, V.K.; Rodriguez, P.; Ostrand-Rosenberg, S. Myeloid-derived suppressor cells inhibit T-cell activation by depleting cystine and cysteine. Cancer Res. 2010, 70, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Law, J.P.; Hirschkorn, D.F.; Owen, R.E.; Biswas, H.H.; Norris, P.J.; Lanteri, M.C. The importance of Foxp3 antibody and fixation/permeabilization buffer combinations in identifying CD4+CD25+Foxp3+ regulatory T cells. Cytometry A 2009, 75, 1040–1050. [Google Scholar] [CrossRef] [PubMed]
- Di Ianni, M.; Del Papa, B.; Cecchini, D.; Bonifacio, E.; Moretti, L.; Zei, T.; Ostini, R.I.; Falzetti, F.; Fontana, L.; Tagliapietra, G.; et al. Immunomagnetic isolation of CD4+CD25+FoxP3+ natural T regulatory lymphocytes for clinical applications. Clin. Exp. Immunol. 2009, 156, 246–1253. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MAC-LD n = 46 | MAB-LD n = 23 | Healthy Subjects n = 27 | |
|---|---|---|---|
| Age (years) | 64.5 (15.4) | 62.1 (14.0) | 55.5 (14.1) * |
| Male sex | 20 (44%) | 8 (35%) | 15 (56%) |
| Current smoker | 1 (2%) | 0 | 2 (7%) |
| Body mass index, kg/m2 | 20.0 (3.2) | 22.6 (3.7) ǂ | 23.1 (2.8) * |
| Diabetes mellitus | 2 (4%) | 1 (4%) | 2 (7%) |
| Autoimmune diseases | 1 (2%) | 1 (4%) | 0 |
| Prior TB history | 5 (11%) | 1 (4%) | 0 |
| Symptoms | |||
| Cough | 13 (28%) | 10 (44%) | - |
| Dyspnea | 22 (48%) | 14 (61%) | - |
| Hemoptysis | 15 (33%) | 8 (35%) | - |
| Sputum study within 1 year | |||
| Max. positive AFS | 1.1 (1.4) | 0.4 (1.1) ǂ | - |
| No. of positive cultures | 3.5 (3.0) | 3.0 (1.9) | - |
| Radiological finding | |||
| CXR score # | 4.5 (2.2) | 3.0 (2.2) ǂ | - |
| FC pattern | 8 (17%) | 2 (9%) | - |
| NB pattern | 32 (70%) | 16 (70%) | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shu, C.-C.; Pan, S.-W.; Feng, J.-Y.; Wang, J.-Y.; Chan, Y.-J.; Yu, C.-J.; Su, W.-J. The Clinical Significance of Programmed Death-1, Regulatory T Cells and Myeloid Derived Suppressor Cells in Patients with Nontuberculous Mycobacteria-Lung Disease. J. Clin. Med. 2019, 8, 736. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050736
Shu C-C, Pan S-W, Feng J-Y, Wang J-Y, Chan Y-J, Yu C-J, Su W-J. The Clinical Significance of Programmed Death-1, Regulatory T Cells and Myeloid Derived Suppressor Cells in Patients with Nontuberculous Mycobacteria-Lung Disease. Journal of Clinical Medicine. 2019; 8(5):736. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050736
Chicago/Turabian StyleShu, Chin-Chung, Sheng-Wei Pan, Jia-Yih Feng, Jann-Yuan Wang, Yu-Jiun Chan, Chong-Jen Yu, and Wei-Juin Su. 2019. "The Clinical Significance of Programmed Death-1, Regulatory T Cells and Myeloid Derived Suppressor Cells in Patients with Nontuberculous Mycobacteria-Lung Disease" Journal of Clinical Medicine 8, no. 5: 736. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050736