Association between Serum Urate and Risk of Hypertension in Menopausal Women with XDH Gene

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Methods
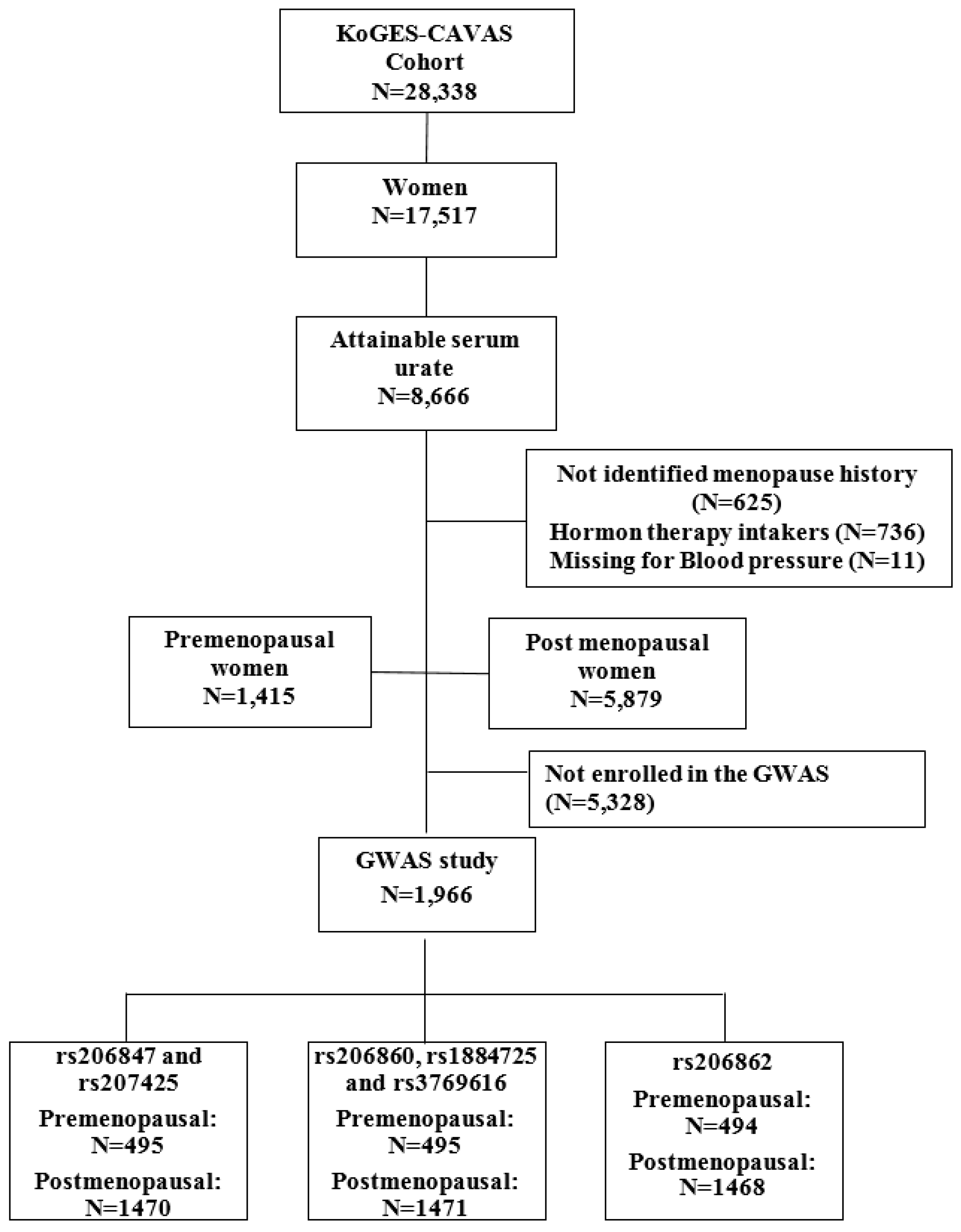
2.1. Study Population
2.2. Data Collection
2.3. Genome Wide Association Study Genotyping
2.4. Analysis of the XDH Genomic Polymorphism
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Anthropometric Characteristics of Premenopausal and Postmenopausal Women with Hypertension
3.3. Univariate and Multivariate Logistic Regression Analyses
3.4. Hypertension Risk of Participants according to Genotypes of Xanthine Dehydrogenase (XDH)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Chang, C.C.; Wu, C.H.; Liu, L.K.; Chou, R.H.; Kuo, C.S.; Huang, P.H.; Chen, L.K.; Lin, S.J. Association between serum uric acid and cardiovascular risk in nonhypertensive and nondiabetic individuals: The Taiwan I-Lan Longitudinal Aging Study. Sci. Rep. 2018, 8, 5234. [Google Scholar] [CrossRef]
- Orlando, A.; Cazzaniga, E.; Giussani, M.; Palestini, P.; Genovesi, S. Hypertension in Children: Role of Obesity, Simple Carbohydrates, and Uric Acid. Front. Public Health 2018, 6, 129. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, E.; Kwoh, C.K.; Schumacher, H.R.; Kuller, L. Hyperuricemia and incidence of hypertension among men without metabolic syndrome. Hypertension (Dallas Tex. 1979) 2007, 49, 298–303. [Google Scholar] [CrossRef]
- Jossa, F.; Farinaro, E.; Panico, S.; Krogh, V.; Celentano, E.; Galasso, R.; Mancini, M.; Trevisan, M. Serum uric acid and hypertension: The Olivetti heart study. J. Hum. Hypertens. 1994, 8, 677–681. [Google Scholar] [PubMed]
- Chen, Q.; Yin, Y.J.; Chen, W.Y.; Wu, J.N.; Huang, X. Assessment of the association between serum uric acid levels and the incidence of hypertension in nonmetabolic syndrome subjects: A prospective observational study. Medicine 2018, 97, e9765. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Sun, N.; Cai, C.; Feng, S.; Tian, J.; Shi, W.; Xu, W.; Wang, Y.; Yang, X.; Li, W.D. Associations between serum uric acid and the incidence of hypertension: A Chinese senior dynamic cohort study. J. Transl. Med. 2016, 14, 110. [Google Scholar] [CrossRef]
- Amos, C.I.; Wu, X.; Broderick, P.; Gorlov, I.P.; Gu, J.; Eisen, T.; Dong, Q.; Zhang, Q.; Gu, X.; Vijayakrishnan, J.; et al. Genome-wide association scan of tag SNPs identifies a susceptibility locus for lung cancer at 15q25.1. Nat. Genet. 2008, 40, 616–622. [Google Scholar] [CrossRef] [Green Version]
- Nieto, F.J.; Iribarren, C.; Gross, M.D.; Comstock, G.W.; Cutler, R.G. Uric acid and serum antioxidant capacity: A reaction to atherosclerosis? Atherosclerosis 2000, 148, 131–139. [Google Scholar] [CrossRef]
- Sciacqua, A.; Perticone, M.; Tassone, E.J.; Cimellaro, A.; Miceli, S.; Maio, R.; Sesti, G.; Perticone, F. Uric acid is an independent predictor of cardiovascular events in post-menopausal women. Int. J. Cardiol. 2015, 197, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Cheng, D.; Du, R.; Wu, X.Y.; Lin, L.; Peng, K.; Ma, L.N.; Xu, Y.; Xu, M.; Chen, Y.H.; Bi, Y.F.; et al. Serum Uric Acid is Associated with the Predicted Risk of Prevalent Cardiovascular Disease in a Community-dwelling Population without Diabetes. Biomed. Environ. Sci. 2018, 31, 106–114. [Google Scholar] [CrossRef]
- Kawamoto, R.; Ninomiya, D.; Senzaki, K.; Kumagi, T. Interaction between body mass index and serum uric acid in relation to blood pressure in community-dwelling Japanese men. Clin. Hypertens. 2018, 24, 1. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Yang, F.; Yang, I.; Yin, Y.; Luo, J.J.; Wang, H.; Yang, X.F. Uric acid, hyperuricemia and vascular diseases. Front. Biosci. (Landmark Ed.) 2012, 17, 656–669. [Google Scholar] [CrossRef]
- Corry, D.B.; Eslami, P.; Yamamoto, K.; Nyby, M.D.; Makino, H.; Tuck, M.L. Uric acid stimulates vascular smooth muscle cell proliferation and oxidative stress via the vascular renin-angiotensin system. J. Hypertens. 2008, 26, 269–275. [Google Scholar] [CrossRef]
- Kang, D.H.; Park, S.K.; Lee, I.K.; Johnson, R.J. Uric acid-induced C-reactive protein expression: Implication on cell proliferation and nitric oxide production of human vascular cells. J. Am. Soc. Nephrol. JASN 2005, 16, 3553–3562. [Google Scholar] [CrossRef]
- Mazzali, M.; Hughes, J.; Kim, Y.G.; Jefferson, J.A.; Kang, D.H.; Gordon, K.L.; Lan, H.Y.; Kivlighn, S.; Johnson, R.J. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension (Dallas Tex. 1979) 2001, 38, 1101–1106. [Google Scholar] [CrossRef]
- Wang, J.; Qin, T.; Chen, J.; Li, Y.; Wang, L.; Huang, H.; Li, J. Hyperuricemia and risk of incident hypertension: A systematic review and meta-analysis of observational studies. PLoS ONE 2014, 9, e114259. [Google Scholar] [CrossRef]
- Hak, A.E.; Choi, H.K. Menopause, postmenopausal hormone use and serum uric acid levels in US women--the Third National Health and Nutrition Examination Survey. Arthritis Res. Ther. 2008, 10, R116. [Google Scholar] [CrossRef] [PubMed]
- Sumino, H.; Ichikawa, S.; Kanda, T.; Nakamura, T.; Sakamaki, T. Reduction of serum uric acid by hormone replacement therapy in postmenopausal women with hyperuricaemia. Lancet (Lond. Engl.) 1999, 354, 650. [Google Scholar] [CrossRef]
- Scheepers, L.E.; Wei, F.F.; Stolarz-Skrzypek, K.; Malyutina, S.; Tikhonoff, V.; Thijs, L.; Salvi, E.; Barlassina, C.; Filipovsky, J.; Casiglia, E.; et al. Xanthine oxidase gene variants and their association with blood pressure and incident hypertension: A population study. J. Hypertens. 2016, 34, 2147–2154. [Google Scholar] [CrossRef]
- Battelli, M.G.; Bolognesi, A.; Polito, L. Pathophysiology of circulating xanthine oxidoreductase: New emerging roles for a multi-tasking enzyme. Biochim. Biophys. Acta 2014, 1842, 1502–1517. [Google Scholar] [CrossRef] [Green Version]
- Wu, B.; Hao, Y.; Shi, J.; Geng, N.; Li, T.; Chen, Y.; Sun, Z.; Zheng, L.; Li, H.; Li, N.; et al. Association between xanthine dehydrogenase tag single nucleotide polymorphisms and essential hypertension. Mol. Med. Rep. 2015, 12, 5685–5690. [Google Scholar] [CrossRef]
- Verdecchia, P.; Schillaci, G.; Reboldi, G.; Santeusanio, F.; Porcellati, C.; Brunetti, P. Relation between serum uric acid and risk of cardiovascular disease in essential hypertension. The PIUMA study. Hypertension (Dallas Tex. 1979) 2000, 36, 1072–1078. [Google Scholar] [CrossRef]
- Choi, J.R.; Ahn, S.V.; Kim, J.Y.; Koh, S.B.; Choi, E.H.; Lee, G.Y.; Jang, Y.E. Comparison of various anthropometric indices for the identification of a predictor of incident hypertension: The ARIRANG study. J. Hum. Hypertens. 2018, 32, 294–300. [Google Scholar] [CrossRef]
- Kim, J.; Yoon, D.W.; Lee, S.K.; Lee, S.; Choi, K.M.; Robert, T.J.; Shin, C. Concurrent presence of inflammation and obstructive sleep apnea exacerbates the risk of metabolic syndrome: A KoGES 6-year follow-up study. Medicine 2017, 96, e4488. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.R.; Jang, Y.; Kim Yoon, S.; Park, J.K.; Sorn, S.R.; Park, M.Y.; Lee, M. The Impact of CDH13 Polymorphism and Statin Administration on TG/HDL Ratio in Cardiovascular Patients. Yonsei Med. J. 2015, 56, 1604–1612. [Google Scholar] [CrossRef] [PubMed]
- Bonora, E.; Capaldo, B.; Perin, P.C.; Del Prato, S.; De Mattia, G.; Frittitta, L.; Frontoni, S.; Leonetti, F.; Luzi, L.; Marchesini, G.; et al. Hyperinsulinemia and insulin resistance are independently associated with plasma lipids, uric acid and blood pressure in non-diabetic subjects. The GISIR database. Nutr. Metab. Cardiovasc. Dis. NMCD 2008, 18, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, T.; Kubo, M.; Doi, Y.; Yonemoto, K.; Tanizaki, Y.; Rahman, M.; Arima, H.; Tsuryuya, K.; Iida, M.; Kiyohara, Y. Impact of metabolic syndrome on the development of cardiovascular disease in a general Japanese population: The Hisayama study. Stroke 2007, 38, 2063–2069. [Google Scholar] [CrossRef]
- Kanellis, J.; Kang, D.H. Uric acid as a mediator of endothelial dysfunction, inflammation, and vascular disease. Semin. Nephrol. 2005, 25, 39–42. [Google Scholar] [CrossRef]
- Xu, J.; Lloyd, D.J.; Hale, C.; Stanislaus, S.; Chen, M.; Sivits, G.; Vonderfecht, S.; Hecht, R.; Li, Y.S.; Lindberg, R.A.; et al. Fibroblast growth factor 21 reverses hepatic steatosis, increases energy expenditure, and improves insulin sensitivity in diet-induced obese mice. Diabetes 2009, 58, 250–259. [Google Scholar] [CrossRef]
- Techatraisak, K.; Kongkaew, T. The association of hyperuricemia and metabolic syndrome in Thai postmenopausal women. Climacteric J. Int. Menopause Soc. 2017, 20, 552–557. [Google Scholar] [CrossRef]
- Johnson, R.J.; Kang, D.H.; Feig, D.; Kivlighn, S.; Kanellis, J.; Watanabe, S.; Tuttle, K.R.; Rodriguez-Iturbe, B.; Herrera-Acosta, J.; Mazzali, M. Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension (Dallas Tex. 1979) 2003, 41, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.E.; Kawut, S.M.; Krowka, M.J.; Brown, R.S., Jr.; Trotter, J.F.; Shah, V.; Peter, I.; Tighiouart, H.; Mitra, N.; Handorf, E.; et al. Genetic risk factors for hepatopulmonary syndrome in patients with advanced liver disease. Gastroenterology 2010, 139, 130–139.e24. [Google Scholar] [CrossRef]
- Li, Y.; Tang, H.; Qi, H.; Shen, C.; Sun, L.; Li, J.; Xu, F.; Jiao, W.; Yang, X.; Shen, A. rs1800796 of the IL6 gene is associated with increased risk for anti-tuberculosis drug-induced hepatotoxicity in Chinese Han children. Tuberculosis 2018, 111, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Kamide, K.; Kokubo, Y.; Takiuchi, S.; Horio, T.; Matayoshi, T.; Yasuda, H.; Miwa, Y.; Yoshii, M.; Yoshihara, F.; et al. Associations of hypertension and its complications with variations in the xanthine dehydrogenase gene. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2008, 31, 931–940. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Serum Urate (sUA) | p-Value | Post-Hoc * | |||
|---|---|---|---|---|---|---|
| Quartile 1 (<3.7 mg/dL) | Quartile 2 (3.7 ≤ 4.3 mg/dL) | Quartile 3 (4.3 ≤ 5.0 mg/dL) | Quartile 4 (≥5.0 mg/dL) | |||
| Women | ||||||
| Premenopausal | 411 (24.3) | 385 (23.4) | 381 (20.0) | 238 (11.6) | <0.01 | |
| Postmenopausal | 1282 (75.7) | 1258 (76.6) | 1524 (80.0) | 1815 (88.4) | ||
| Age | 60.5 ± 10.6 | 60.2 ± 10.5 | 60.4 ± 10.3 | 62.6 ± 9.6 | <0.01 | a, b, c < d |
| Smoking status | ||||||
| Non, ex-smoker | 1039 (96.9) | 978 (96.4) | 1140 (96.9) | 1116 (35.1) | 0.2 | |
| Current smoker | 22 (3.1) | 36 (3.6) | 37 (3.1) | 58 (4.9) | ||
| Alcohol | ||||||
| Yes | 458 (27.1) | 447 (27.3) | 573 (30.1) | 602 (29.3) | 0.11 | |
| No | 1235 (72.9) | 1193 (72.7) | 1330 (69.9) | 1451 (70.7) | ||
| Weight (kg) | 54.6 ± 8.5 | 56.1 ± 8.2 | 57.4 ± 8.7 | 58.8 ± 9.5 | <0.01 | a < b < c < d |
| Height (cm) | 152.0 ± 6.2 | 152.6 ± 6.2 | 152.5 ± 5.9 | 152.1 ± 6.0 | 0.02 | |
| BMI (kg/) | 23.6 ± 3.2 | 24.1 ± 3.0 | 24.7 ± 3.2 | 25.3 ± 3.4 | <0.01 | a < b < c < d |
| WC (cm) | 81.0 ± 9.0 | 81.9 ± 8.8 | 83.4 ± 9.0 | 85.2 ± 8.9 | <0.01 | a < b < c < d |
| HC (cm) | 91.7 ± 6.3 | 92.5 ± 6.2 | 93.3 ± 6.8 | 94.0 ± 6.9 | <0.01 | a < b < c < d |
| Creatinine (mg/dL) | 0.8 ± 0.1 | 0.8 ± 0.1 | 0.9 ± 0.1 | 0.9 ± 0.3 | <0.01 | a < b < c < d |
| HDL-C (mg/dL) | 47.9 ± 11.2 | 46.9 ± 10.9 | 45.8 ± 11.2 | 43.7 ± 10.4 | <0.01 | a, b > c > d |
| Fasting glucose (mg/dL) | 97.9 ± 24.5 | 95.9 ± 19.3 | 98.0 ± 19.2 | 100.4 ± 21.1 | <0.01 | a < d, b < c < d |
| Total cholesterol (mg/dL) | 199.0 ± 36.0 | 200.6 ± 34.7 | 203.7 ± 36.2 | 208.8 ± 38.6 | <0.01 | a < c < d, b < d |
| Triglycerides (mg/dL) | 126.4 ± 67.2 | 130.7 ± 72.2 | 146.1 ± 83.4 | 171.8 ± 104.0 | <0.01 | a, b < c < d |
| Total protein (g/dL) | 7.3 ± 0.4 | 7.3 ± 0.4 | 7.4 ± 0.4 | 7.5 ± 0.4 | <0.01 | a < c < d, b < d |
| Albumin (g/dL) | 4.4 ± 0.2 | 4.4 ± 0.2 | 4.5 ± 0.2 | 4.5 ± 0.2 | <0.01 | a, b < c, d |
| GGT (I/U) | 17.2 ± 15.7 | 17.8 ± 21.7 | 20.4 ± 28.2 | 24.8 ± 30.8 | <0.01 | a, b < c < d |
| SBP (mmHg) | 122.3 ± 18.1 | 122.3 ± 17.7 | 123.6 ± 18.4 | 126.4 ± 18.0 | <0.01 | a, b, c < d |
| DBP (mmHg) | 75.8 ± 10.3 | 75.9 ± 10.4 | 76.5 ± 10.4 | 77.7 ± 10.4 | <0.01 | a, b, c < d |
| Hypertension | 545 (32.2) | 569 (34.6) | 748 (39.3) | 1103 (53.7) | <0.01 | a, b < c < d |
| Variables | Premenopausal Women (N = 1415) | Postmenopausal Women (N = 5879) | ||||
|---|---|---|---|---|---|---|
| Without Hypertension (N = 1142) | With Hypertension (N = 273) | p * | Without Hypertension (N = 3187) | With Hypertension (N = 2692) | p * | |
| sUA (mg/dL) | 4.08 ± 0.87 | 4.42 ± 1.06 | <0.01 | 4.35 ± 1.03 | 4.72 ± 1.25 | <0.01 |
| Age (year) | 46.65 ± 3.98 | 48.57 ± 4.27 | <0.01 | 63.08 ± 8.44 | 65.84 ± 7.82 | <0.01 |
| BMI (kg/m2) | 24.10 ± 2.96 | 26.19 ± 3.55 | <0.01 | 23.94 ± 3.15 | 25.06 ± 3.33 | <0.01 |
| WC (cm) | 79.25 ± 8.18 | 84.26 ± 8.65 | <0.01 | 82.35 ± 8.96 | 85.25 ± 8.98 | <0.01 |
| HC (cm) | 93.45 ± 6.31 | 96.14 ± 6.39 | <0.01 | 92.06 ± 6.48 | 93.54 ± 6.83 | <0.01 |
| SBP (mmHg) | 111.00 ± 11.22 | 136.00 ± 16.44 | <0.01 | 116.30 ± 12.00 | 136.90 ± 17.92 | <0.01 |
| DBP (mmHg) | 72.43 ± 8.41 | 88.61 ± 9.81 | <0.01 | 73.14 ± 7.97 | 81.14 ± 11.08 | <0.01 |
| TC (mg/dL) | 190.40 ± 32.36 | 197.40 ± 33.90 | 0.002 | 205.48 ± 36.26 | 206.94 ± 37.99 | 0.14 |
| TG (mg/dL) | 114.80 ± 70.17 | 146.30 ± 94.17 | <0.01 | 141.50 ± 78.67 | 162.50 ± 95.14 | <0.01 |
| HDL (mg/dL) | 47.55 ± 11.10 | 46.49 ± 11.40 | 0.16 | 46.48 ± 11.10 | 44.55 ± 10.74 | <0.01 |
| Total protein (g/dL) | 7.34 ± 0.38 | 7.43 ± 0.42 | 0.01 | 7.35 ± 0.40 | 7.42 ± 0.42 | <0.01 |
| Albumin (g/dL) | 4.42 ± 0.22 | 4.44 ± 0.26 | 0.22 | 4.43 ± 0.23 | 4.48 ± 0.24 | <0.01 |
| GGT (I/U) | 18.34 ± 27.48 | 22.56 ± 27.39 | 0.03 | 19.06 ± 20.14 | 22.38 ± 29.59 | <0.01 |
| Fasting glucose (mg/dL) | 92.93 ± 15.41 | 98.30 ± 23.20 | <0.01 | 97.10 ± 20.58 | 101.70 ± 23.00 | <0.01 |
| Creatinine (mg/dL) | 0.85 ± 0.08 | 0.85 ± 0.11 | 0.88 | 0.86 ± 0.10 | 0.90 ± 0.25 | <0.01 |
| Current smoking (%) | 7 (1.2) | 2 (1.4) | 0.93 | 90 (2.8) | 66 (2.5) | 0.53 |
| Current drinker (%) | 448 (39.2) | 108 (39.6) | 0.89 | 886 (27.8) | 638 (23.7) | 0.001 |
| Regular exercise (%) | 459 (40.2) | 107 (39.2) | 0.76 | 849 (26.6) | 785 (29.2) | 0.11 |
| Variables | Crude Odds Ratio (95% CI) | Adjusted Odds Ratio (95% CI) | ||
|---|---|---|---|---|
| Premenopausal (N = 1415) | Postmenopausal (N = 5879) | Premenopausal (N = 1415) | Postmenopausal (N = 5879) | |
| Drinking status sUA † | ||||
| Never, past drinker and sUA < 5 mg/dL | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Current drinker and sUA < 5 mg/dL | 0.95 (0.69–1.30) | 0.82 (0.71–0.95) | 0.92 (0.60–1.42) | 0.79 (0.66–0.95) |
| Never, past drinker and sUA ≥ 5 mg/dL | 2.16 (1.44–3.24) | 1.96 (1.71–2.23) | 1.57 (0.88–2.77) | 1.91 (1.62–2.25) |
| Current drinker and sUA ≥ 5 mg/dL | 2.66 (1.67–4.23) | 1.42 (1.17–1.71) | 2.09 (1.10–4.00) | 1.44 (1.14–1.81) |
| BMI urate ‡ | ||||
| Normal and sUA < 5 mg/dL | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Obesity and sUA < 5 mg/dL | 3.11 (2.27–4.25) | 1.85 (1.63–2.11) | 1.15 (0.69–1.92) | 1.61 (1.33–1.94) |
| Normal and sUA ≥ 5 mg/dL | 2.32 (1.34–4.00) | 1.82 (1.56–2.12) | 1.93 (0.92–4.06) | 1.86 (1.53–2.25) |
| Obesity and sUA ≥ 5 mg/dL | 5.20 (3.48–7.78) | 3.13 (2.67–3.66) | 2.13 (1.14–3.99) | 3.18 (2.54–3.96) |
| Waist circumference urate † | ||||
| Normal and sUA < 5 mg/dL | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Abdominal obesity and sUA < 5 mg/dL | 2.58 (1.87–3.56) | 1.60 (1.41–1.82) | 0.77 (0.43–1.27) | 0.86 (0.71–1.03) |
| Normal and sUA ≥ 5 mg/dL | 2.27 (1.46–3.53) | 1.87 (1.59–2.18) | 1.97 (1.08–3.60) | 1.84 (1.51–2.24) |
| Abdominal obesity and sUA ≥ 5 mg/dL | 4.59 (2.98–7.06) | 2.74 (2.35–3.20) | 1.27 (0.64–2.52) | 1.62 (1.30–2.01) |
| Triglyceride sUA † | ||||
| Normal and sUA < 5 mg/dL | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Hypertriglyceridemia and sUA < 5 mg/dL | 2.03 (1.43–2.88) | 1.50 (1.32–1.72) | 1.26 (0.78–2.06) | 1.14 (0.96–1.34) |
| Normal and sUA ≥ 5 mg/dL | 2.19 (1.45–3.31) | 1.78 (1.53–2.07) | 1.65 (0.92–2.96) | 1.82 (1.51–2.20) |
| Hypertriglyceridemia and sUA ≥ 5 mg/dL | 3.88 (2.49–6.04) | 2.63 (2.25–3.08) | 2.38 (1.28–4.43) | 2.08 (1.72–2.53) |
| SNP | Crude | p | Model 1 | p | Model 2 | p | |
|---|---|---|---|---|---|---|---|
| Number | Type | ||||||
| rs206847 | AA | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | |||
| AC | 2.467 (0.677–8.997) | 0.17 | 2.519 (0.690–9.202) | 0.16 | 3.174 (0.807–12.491) | 0.1 | |
| CC | 3.631 (0.863–15.287) | 0.08 | 3.755 (0.887–15.900) | 0.07 | 5.076 (1.044–24.682) | 0.04 | |
| rs206860 | AA | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | |||
| AG | 0.287 (0.091–0.905) | 0.03 | 0.282 (0.089–0.893) | 0.03 | 0.263 (0.078–0.888) | 0.03 | |
| GG | 0.661 (0.183–2.386) | 0.53 | 0.646 (0.178–2.342) | 0.51 | 0.451 (0.109–1.866) | 0.27 | |
| rs207425 | GG | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | |||
| GA | 2.065 (0.770–5.537) | 0.15 | 2.044 (0.758–5.509) | 0.16 | 3.160 (1.015–9.841) | 0.05 | |
| AA | - | 0.99 | - | 0.99 | - | 0.99 | |
| rs1884725 | GG | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | |||
| GA | 1.052 (0.338–3.279) | 0.93 | 1.011 (0.323–3.162) | 0.99 | 0.957 (0.282–3.244) | 0.94 | |
| AA | 3.668 (0.805–16.725) | 0.09 | 3.935 (0.854–18.127) | 0.08 | 11.162 (1.525–81.706) | 0.02 | |
| rs3769616 | GG | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | |||
| GA | - | 0.99 | - | 0.99 | - | 0.99 | |
| AA | 1.580 (0.207–12.037) | 0.66 | 1.562 (0.203–12.013) | 0.67 | 9.732 (0.972–97.400) | 0.05 | |
| rs206826 | AA | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | |||
| AC | 0.351 (0.110–1.123) | 0.08 | 0.355 (0.110–1.139) | 0.08 | 0.282 (0.081–0.979) | 0.05 | |
| CC | 0.907 (0.283–2.913) | 0.87 | 0.905 (0.280–2.918) | 0.87 | 0.588 (0.158–2.180) | 0.43 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Go, T.H.; Lee, S.-H.; Kim, J.; Huh, J.H.; Kim, J.Y.; Kang, D.R.; Jeong, S.; Koh, S.-B.; Choi, J.R. Association between Serum Urate and Risk of Hypertension in Menopausal Women with XDH Gene. J. Clin. Med. 2019, 8, 738. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050738
Lee J-H, Go TH, Lee S-H, Kim J, Huh JH, Kim JY, Kang DR, Jeong S, Koh S-B, Choi JR. Association between Serum Urate and Risk of Hypertension in Menopausal Women with XDH Gene. Journal of Clinical Medicine. 2019; 8(5):738. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050738
Chicago/Turabian StyleLee, Jong-Han, Tae Hwa Go, San-Hui Lee, Juwon Kim, Ji Hye Huh, Jang Young Kim, Dae Ryong Kang, Seongmun Jeong, Sang-Baek Koh, and Jung Ran Choi. 2019. "Association between Serum Urate and Risk of Hypertension in Menopausal Women with XDH Gene" Journal of Clinical Medicine 8, no. 5: 738. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050738