Effects of Positive End-Expiratory Pressure on Pulmonary Oxygenation and Biventricular Function during One-Lung Ventilation: A Randomized Crossover Study


Abstract
:1. Introduction
2. Materials and Methods
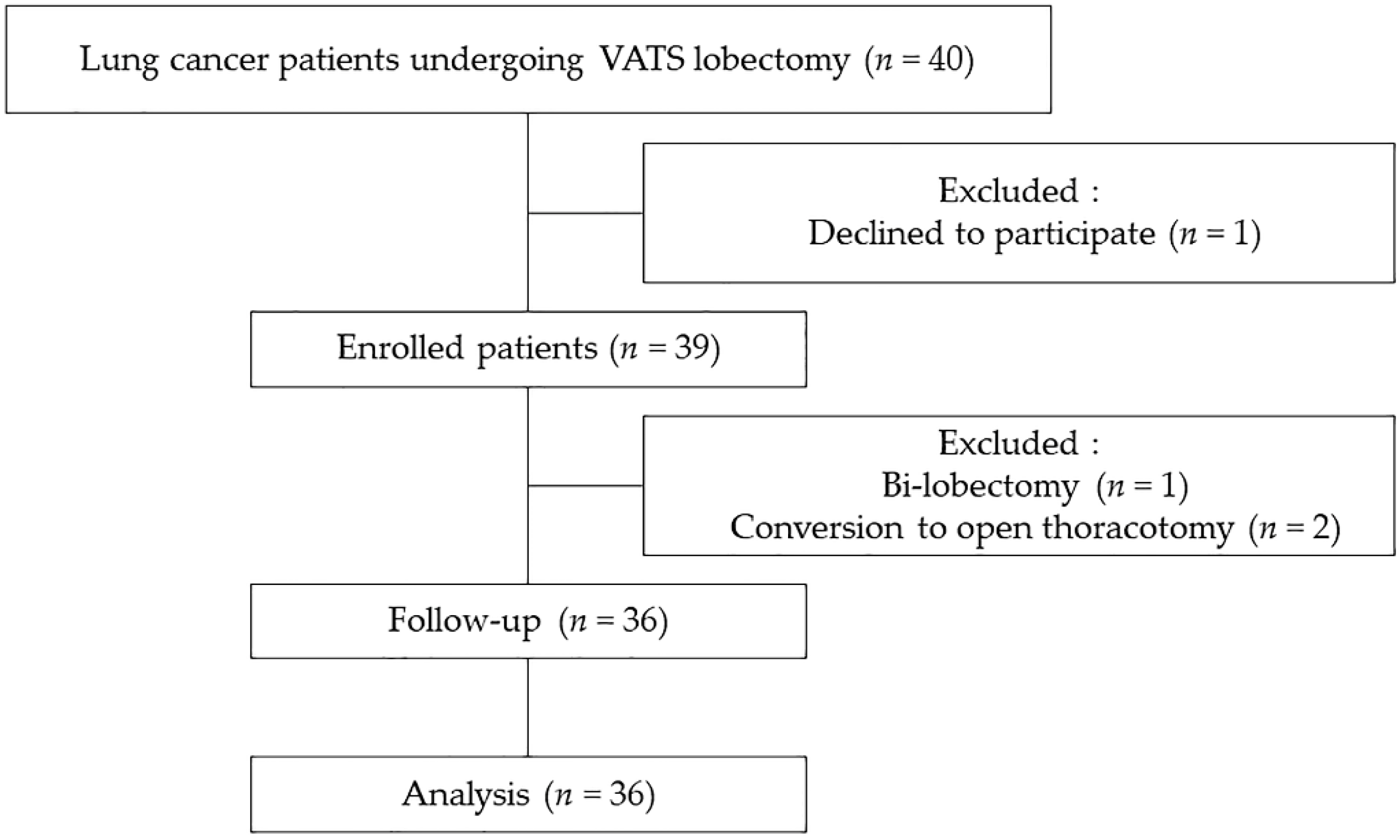
2.1. Patients
2.2. Anesthesia and Procedural Protocols
2.3. Study Design and Outcome Assessments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Karzai, W.; Schwarzkopf, K. Hypoxemia during one-lung ventilation: Prediction, prevention, and treatment. Anesthesiology 2009, 110, 1402–1411. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.A.; Laverne, R.G.; Fairley, H.B.; Thomas, A.N. Pulmonary oxygen exchange during endobronchial anesthesia: Effect of tidal volume and peep. Anesthesiology 1982, 56, 164–171. [Google Scholar] [CrossRef]
- Ishikawa, S.; Lohser, J. One-lung ventilation and arterial oxygenation. Curr. Opin. Anaesthesiol. 2011, 24, 24–31. [Google Scholar] [CrossRef]
- Yang, M.; Ahn, H.J.; Kim, K.; Kim, J.A.; Yi, C.A.; Kim, M.J.; Kim, H.J. Does a protective ventilation strategy reduce the risk of pulmonary complications after lung cancer surgery? A randomized controlled trial. Chest 2011, 139, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, C.; Mugarra, A.; Gutierrez, A.; Carbonell, J.A.; Garcia, M.; Soro, M.; Tusman, G.; Belda, F.J. Setting individualized positive end-expiratory pressure level with a positive end-expiratory pressure decrement trial after a recruitment maneuver improves oxygenation and lung mechanics during one-lung ventilation. Anesth. Analg. 2014, 118, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Huemer, G.; Kolev, N.; Kurz, A.; Zimpfer, M. Influence of positive end-expiratory pressure on right and left ventricular performance assessed by doppler two-dimensional echocardiography. Chest 1994, 106, 67–73. [Google Scholar] [CrossRef]
- Hardman, J.G.; Aitkenhead, A.R. Estimating alveolar dead space from the arterial to end-tidal co(2) gradient: A modeling analysis. Anesth. Analg. 2003, 97, 1846–1851. [Google Scholar] [CrossRef]
- Michelet, P.; Roch, A.; Brousse, D.; D’Journo, X.B.; Bregeon, F.; Lambert, D.; Perrin, G.; Papazian, L.; Thomas, P.; Carpentier, J.P.; et al. Effects of peep on oxygenation and respiratory mechanics during one-lung ventilation. Br. J. Anaesth. 2005, 95, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.H.; Lee, E.H.; Kim, W.J.; Choi, D.K.; Hahm, K.D.; Sim, J.Y.; Choi, I.C. Positive end-expiratory pressure aggravates left ventricular diastolic relaxation further in patients with pre-existing relaxation abnormality. Br. J. Anaesth. 2013, 111, 368–373. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Hedenstierna, G.; Edmark, L. The effects of anesthesia and muscle paralysis on the respiratory system. Intensive Care Med. 2005, 31, 1327–1335. [Google Scholar] [CrossRef]
- Tokics, L.; Hedenstierna, G.; Strandberg, A.; Brismar, B.; Lundquist, H. Lung collapse and gas exchange during general anesthesia: Effects of spontaneous breathing, muscle paralysis, and positive end-expiratory pressure. Anesthesiology 1987, 66, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Valenza, F.; Ronzoni, G.; Perrone, L.; Valsecchi, M.; Sibilla, S.; Nosotti, M.; Santambrogio, L.; Cesana, B.M.; Gattinoni, L. Positive end-expiratory pressure applied to the dependent lung during one-lung ventilation improves oxygenation and respiratory mechanics in patients with high fev1. Eur. J. Anaesthesiol. 2004, 21, 938–943. [Google Scholar] [CrossRef] [PubMed]
- Hoftman, N.; Canales, C.; Leduc, M.; Mahajan, A. Positive end expiratory pressure during one-lung ventilation: Selecting ideal patients and ventilator settings with the aim of improving arterial oxygenation. Ann. Card. Anaesth. 2011, 14, 183–187. [Google Scholar] [PubMed]
- Slinger, P.D.; Kruger, M.; McRae, K.; Winton, T. Relation of the static compliance curve and positive end-expiratory pressure to oxygenation during one-lung ventilation. Anesthesiology 2001, 95, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Blank, R.S.; Colquhoun, D.A.; Durieux, M.E.; Kozower, B.D.; McMurry, T.L.; Bender, S.P.; Naik, B.I. Management of one-lung ventilation: Impact of tidal volume on complications after thoracic surgery. Anesthesiology 2016, 124, 1286–1295. [Google Scholar] [CrossRef]
- Senturk, N.M.; Dilek, A.; Camci, E.; Senturk, E.; Orhan, M.; Tugrul, M.; Pembeci, K. Effects of positive end-expiratory pressure on ventilatory and oxygenation parameters during pressure-controlled one-lung ventilation. J. Cardiothorac. Vasc. Anesth. 2005, 19, 71–75. [Google Scholar] [CrossRef]
- Capan, L.M.; Turndorf, H.; Patel, C.; Ramanathan, S.; Acinapura, A.; Chalon, J. Optimization of arterial oxygenation during one-lung anesthesia. Anesth. Analg. 1980, 59, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Mascotto, G.; Bizzarri, M.; Messina, M.; Cerchierini, E.; Torri, G.; Carozzo, A.; Casati, A. Prospective, randomized, controlled evaluation of the preventive effects of positive end-expiratory pressure on patient oxygenation during one-lung ventilation. Eur. J. Anaesthesiol. 2003, 20, 704–710. [Google Scholar] [CrossRef]
- Tusman, G.; Bohm, S.H.; Sipmann, F.S.; Maisch, S. Lung recruitment improves the efficiency of ventilation and gas exchange during one-lung ventilation anesthesia. Anesth. Analg. 2004, 98, 1604–1609. [Google Scholar] [CrossRef]
- Park, S.H.; Jeon, Y.T.; Hwang, J.W.; Do, S.H.; Kim, J.H.; Park, H.P. A preemptive alveolar recruitment strategy before one-lung ventilation improves arterial oxygenation in patients undergoing thoracic surgery: A prospective randomised study. Eur. J. Anaesthesiol. 2011, 28, 298–302. [Google Scholar] [CrossRef]
- Della Rocca, G.; Coccia, C. Ventilatory management of one-lung ventilation. Minerva Anestesiol. 2011, 77, 534–536. [Google Scholar]
- Michelet, P.; D’Journo, X.B.; Roch, A.; Doddoli, C.; Marin, V.; Papazian, L.; Decamps, I.; Bregeon, F.; Thomas, P.; Auffray, J.P. Protective ventilation influences systemic inflammation after esophagectomy: A randomized controlled study. Anesthesiology 2006, 105, 911–919. [Google Scholar] [CrossRef]
- Luecke, T.; Pelosi, P. Clinical review: Positive end-expiratory pressure and cardiac output. Crit. Care 2005, 9, 607–621. [Google Scholar] [CrossRef] [Green Version]
- Luecke, T.; Roth, H.; Herrmann, P.; Joachim, A.; Weisser, G.; Pelosi, P.; Quintel, M. Assessment of cardiac preload and left ventricular function under increasing levels of positive end-expiratory pressure. Intensive Care Med. 2004, 30, 119–126. [Google Scholar] [CrossRef]
- Schmitt, J.M.; Vieillard-Baron, A.; Augarde, R.; Prin, S.; Page, B.; Jardin, F. Positive end-expiratory pressure titration in acute respiratory distress syndrome patients: Impact on right ventricular outflow impedance evaluated by pulmonary artery doppler flow velocity measurements. Crit. Care Med. 2001, 29, 1154–1158. [Google Scholar] [CrossRef]
- Yamada, T.; Takeda, J.; Satoh, M.; Koyama, K.; Hashiguchi, S.; Yokoi, M. Effect of positive end-expiratory pressure on left and right ventricular diastolic filling assessed by transoesophageal doppler echocardiography. Anaesth Intensive Care 1999, 27, 341–345. [Google Scholar] [CrossRef]
- Vieillard-Baron, A.; Loubieres, Y.; Schmitt, J.M.; Page, B.; Dubourg, O.; Jardin, F. Cyclic changes in right ventricular output impedance during mechanical ventilation. J. Appl. Physiol. 1999, 87, 1644–1650. [Google Scholar] [CrossRef]
- Diaper, J.; Ellenberger, C.; Villiger, Y.; Robert, J.; Inan, C.; Tschopp, J.M.; Licker, M. Comparison of cardiac output as assessed by transesophageal echo-doppler and transpulmonary thermodilution in patients undergoing thoracic surgery. J. Clin. Anesth. 2010, 22, 97–103. [Google Scholar] [CrossRef]
- Roze, H.; Lafargue, M.; Perez, P.; Tafer, N.; Batoz, H.; Germain, C.; Janvier, G.; Ouattara, A. Reducing tidal volume and increasing positive end-expiratory pressure with constant plateau pressure during one-lung ventilation: Effect on oxygenation. Br. J. Anaesth. 2012, 108, 1022–1027. [Google Scholar] [CrossRef]
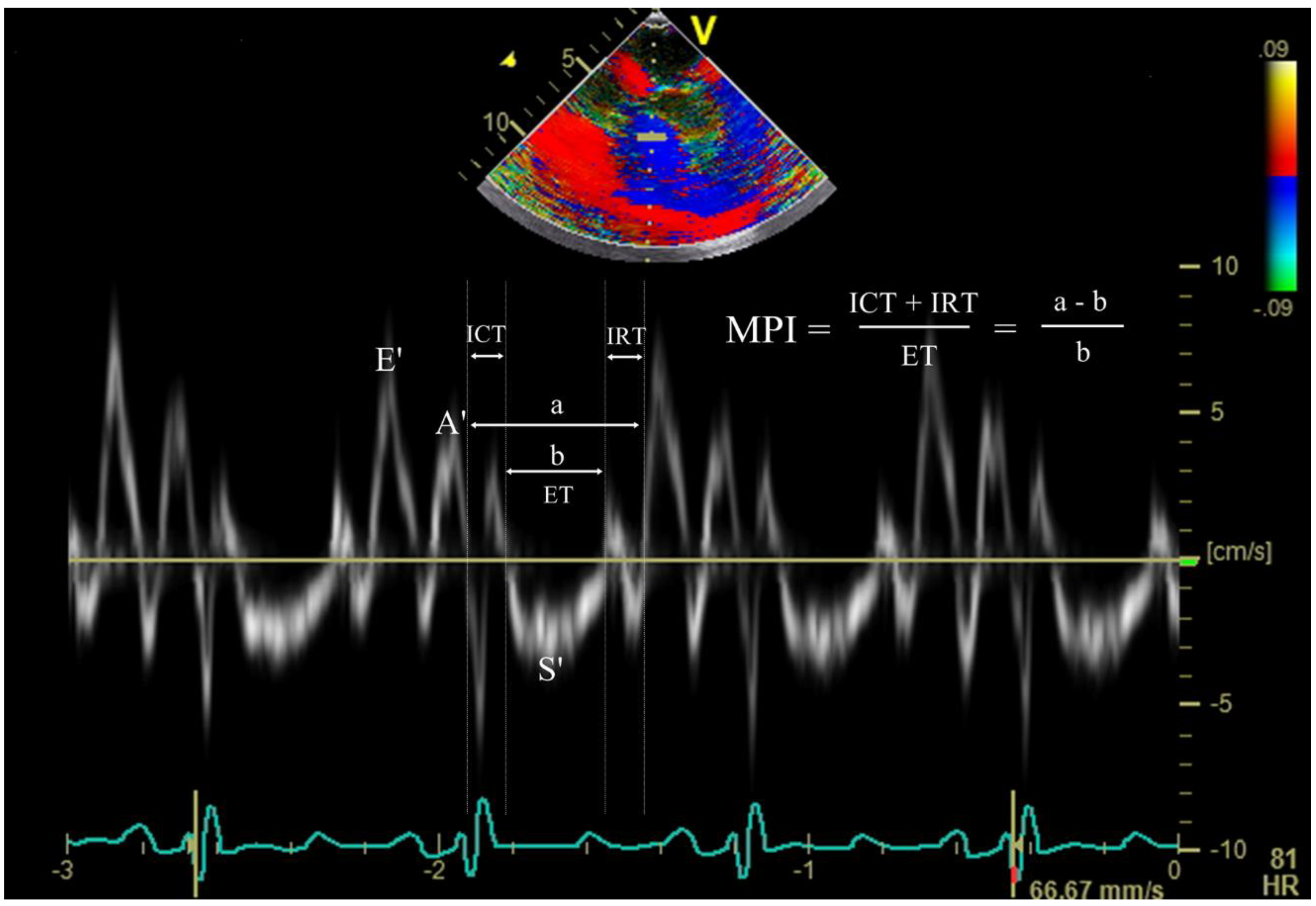
- Skubas, N. Intraoperative doppler tissue imaging is a valuable addition to cardiac anesthesiologists’ armamentarium: A core review. Anesth. Analg. 2009, 108, 48–66. [Google Scholar] [CrossRef]
- Tei, C.; Ling, L.H.; Hodge, D.O.; Bailey, K.R.; Oh, J.K.; Rodeheffer, R.J.; Tajik, A.J.; Seward, J.B. New index of combined systolic and diastolic myocardial performance: A simple and reproducible measure of cardiac function--a study in normals and dilated cardiomyopathy. J. Cardiol. 1995, 26, 357–366. [Google Scholar]
- Yu, C.M.; Sanderson, J.E.; Marwick, T.H.; Oh, J.K. Tissue doppler imaging a new prognosticator for cardiovascular diseases. J. Am. Coll. Cardiol. 2007, 49, 1903–1914. [Google Scholar] [CrossRef] [PubMed]
- Tei, C.; Dujardin, K.S.; Hodge, D.O.; Bailey, K.R.; McGoon, M.D.; Tajik, A.J.; Seward, S.B. Doppler echocardiographic index for assessment of global right ventricular function. J. Am. Soc. Echocardiogr. 1996, 9, 838–847. [Google Scholar] [CrossRef]
- Schaefer, A.; Meyer, G.P.; Hilfiker-Kleiner, D.; Brand, B.; Drexler, H.; Klein, G. Evaluation of tissue doppler tei index for global left ventricular function in mice after myocardial infarction: Comparison with pulsed doppler tei index. Eur. J. Echocardiogr. 2005, 6, 367–375. [Google Scholar] [CrossRef]
- Haddad, F.; Denault, A.Y.; Couture, P.; Cartier, R.; Pellerin, M.; Levesque, S.; Lambert, J.; Tardif, J.C. Right ventricular myocardial performance index predicts perioperative mortality or circulatory failure in high-risk valvular surgery. J. Am. Soc. Echocardiogr. 2007, 20, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Matyal, R.; Mahmood, F.; Hess, P.; Zhao, X.; Mitchell, J.; Maslow, A.; Gangadharan, S.; Decamp, M. Right ventricular echocardiographic predictors of postoperative supraventricular arrhythmias after thoracic surgery: A pilot study. Ann. Thorac. Surg. 2010, 90, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the american society of echocardiography endorsed by the european association of echocardiography, a registered branch of the european society of cardiology, and the canadian society of echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713; quiz 786–788. [Google Scholar]
- Lee, S.H.; Kim, N.; Kim, H.I.; Oh, Y.J. Echocardiographic evaluation of pulmonary venous blood flow and cardiac function changes during one-lung ventilation. Int. J. Clin. Exp. Med. 2015, 8, 13099–13108. [Google Scholar]
- Karbing, D.S.; Kjaergaard, S.; Smith, B.W.; Espersen, K.; Allerod, C.; Andreassen, S.; Rees, S.E. Variation in the pao2/fio2 ratio with fio2: Mathematical and experimental description, and clinical relevance. Crit. Care 2007, 11, R118. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (n = 36) | |
|---|---|
| Age (years) | 68.2 ± 7.9 |
| Sex (male/female), n (%) | 19 (53)/17 (47) |
| Body surface area (m2) | 1.7 ± 0.2 |
| Body mass index (kg/m2) | 24.7 ± 2.9 |
| Smoking history, (None n (%)/Ex n (%)/Current n (%)) | 23 (64)/13 (36)/0 (0) |
| Height (cm) | 161.4 ± 8.0 |
| Weight (Kg) | 64.5 ± 9.8 |
| Lesion, n (%) | |
| Right upper/middle/lower lobe | 13 (36)/5 (14)/6 (17) |
| Left upper/lower lobe | 6 (17)/6 (17) |
| Type of lung cancer, n (%) | |
| Adenocarcinoma/squamous cell carcinoma | 26 (72)/10 (28) |
| TNM stage, n (%) | |
| T1N0M0/T2N0M0/T1N1M0 | 19 (53)/10 (28)/2 (6) |
| T2N1M0/T2N2M0/T3N0M0 | 3 (8)/1 (3)/1 (3) |
| Preoperative pulmonary function test | |
| FVC (L) | 3.0 ± 0.6 |
| FVC (%, predicted) | 97.3 ± 16.8 |
| FEV1 (L) | 2.2 ± 0.4 |
| FEV1 (%, predicted) | 102.6 ± 15.0 |
| FEV1/FVC ratio (%) | 74.4 ± 6.3 |
| DLCO (mL/mmHg/min) | 16.4 ± 3.3 |
| DLCO (%, predicted) | 94.8 ± 24.2 |
| Intra-operative data | |
| Duration of anesthesia (min) | 190 ± 46 |
| Duration of surgery (min) | 133 ± 40 |
| Duration of OLV (min) | 111 ± 37 |
| Intake fluid (mL) | 1,061 ± 320 |
| Urine output (mL) | 246 ± 200 |
| Estimated blood loss (mL) | 79 ± 55 |
| TLV | OLV | p-Value | |||
|---|---|---|---|---|---|
| PEEP_0 | PEEP_5 | PEEP_10 | |||
| pH | 7.36 ± 0.04 | 7.35 ± 0.04 | 7.35 ± 0.05 | 7.35 ± 0.04 | 0.357 |
| Hb (g/dl) | 12.0 ± 1.2 | 11.7 ± 1.6 | 11.9 ± 1.7 | 11.8 ± 1.7 | 0.926 |
| FiO2 | 0.6 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.989 |
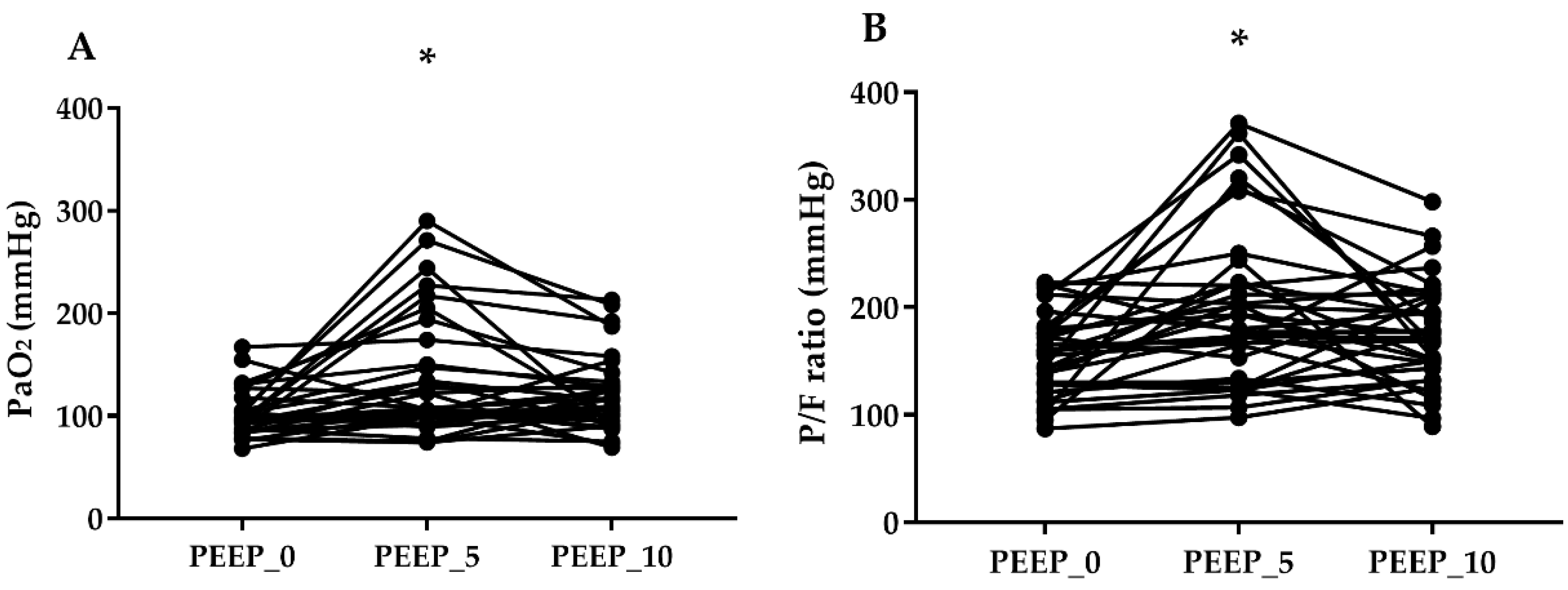
| PaO2 (mmHg) | 208.2 ± 62.4 | 95.6 ± 27.3 | 126.6 ± 71.0 * | 119.6 ± 59.2 | 0.012 |
| PaCO2 (mmHg) | 45.1 ± 4.8 | 47.4 ± 5.6 | 47.3 ± 6.1 | 47.9 ± 6.1 | 0.377 |
| EtCO2 (mmHg) | 40.2 ± 4.2 | 39.0 ± 2.7 | 39.7 ± 3.3 | 40.4 ± 3.7 | 0.188 |
| P/F ratio (mmHg) | 327.6 ± 129.8 | 145.1 ± 53.4 | 184.0 ± 77.8 * | 176.1 ± 77.0 | 0.010 |
| Ppeak (cmH2O) | 12.3 ± 3.0 | 17.8 ± 3.1 | 19.9 ± 2.8 * | 22.9 ± 2.4 *,† | <0.001 |
| Dynamic compliance (mL/cmH2O) | 32.3 ± 10.4 | 20.9 ± 5.2 | 24.6 ± 7.3 * | 27.5 ± 7.2 *,† | <0.001 |
| VD/VT (%) | 14.9 ± 7.3 | 18.0 ± 8.0 | 18.1 ± 8.4 | 18.8 ± 9.8 | 0.902 |
| TLV | OLV | p-Value | ||||
|---|---|---|---|---|---|---|
| PEEP_0 | PEEP_5 | PEEP_10 | ||||
| HR (beats/min) | 72 ± 13 | 75 ± 13 | 73 ± 11 | 73 ± 12 | 0.365 | |
| MAP (mmHg) | 84 ± 15 | 84 ± 15 | 86 ± 12 | 86 ± 15 | 0.673 | |
| CVP (mmHg) | 10 ± 3 | 12 ± 5 | 13 ± 4 | 13 ± 3 | 0.461 | |
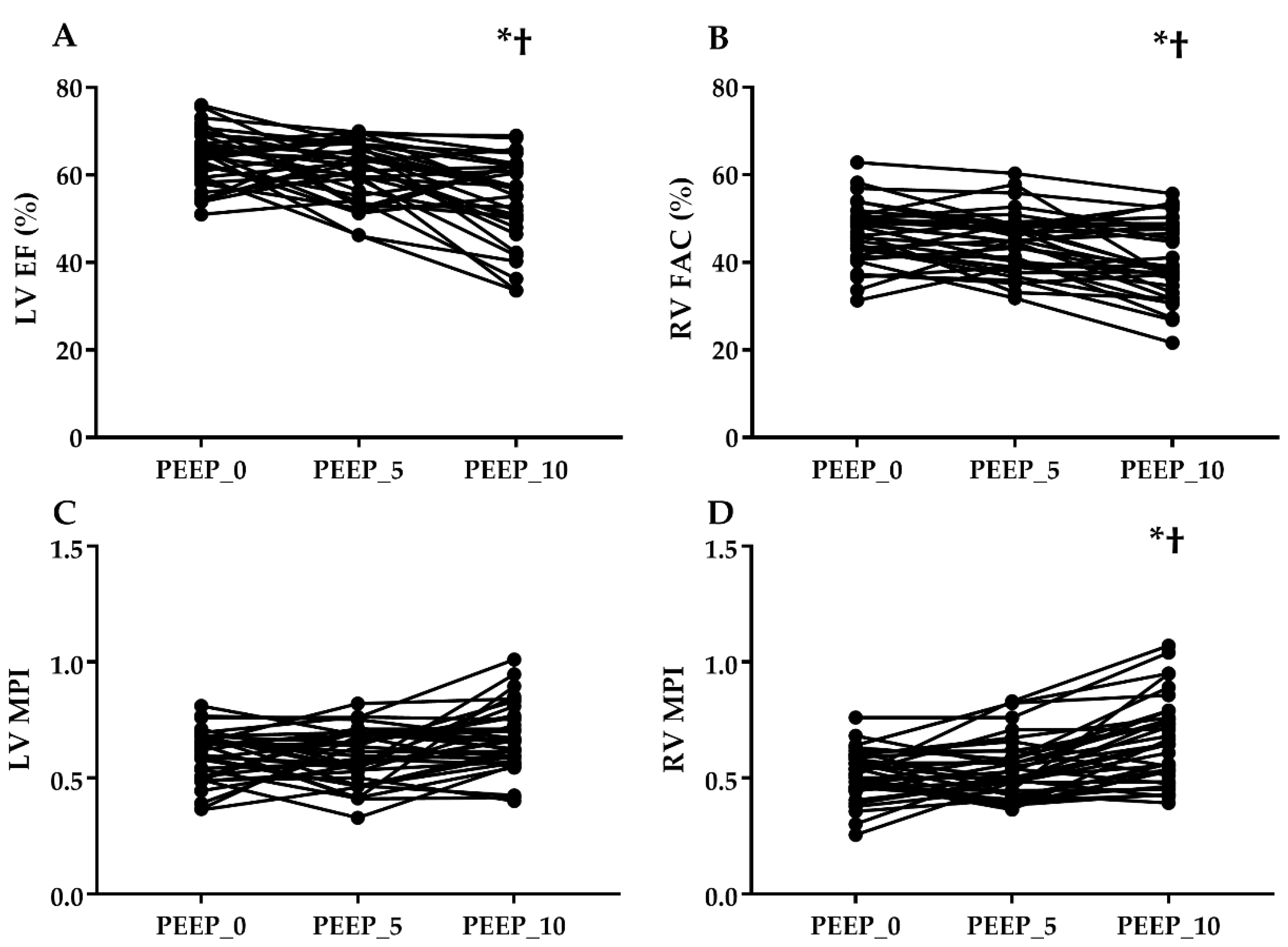
| LV | EF (%) | 58 ± 9 | 63 ± 9 | 61 ± 7 | 55 ± 10 *,† | <0.001 |
| MV E’ (cm/s) | 5.3 ± 1.5 | 5.8 ± 1.6 | 5.6 ± 1.4 | 5.5 ± 1.1 | 0.553 | |
| MV A’ (cm/s) | 4.9 ± 1.4 | 5.9 ± 2.4 | 5.6 ± 1.7 | 5.2 ± 1.8 | 0.067 | |
| MV S’ (cm/s) | 4.0 ± 0.9 | 3.9 ± 1.2 | 3.9 ± 1.1 | 3.7 ± 0.9 | 0.473 | |
| LV E/E’ | 12.3 ± 3.3 | 12.3 ± 3.1 | 12.9 ± 3.6 | 13.6 ± 3.1 | 0.051 | |
| LV MPI | 0.58 ± 0.14 | 0.60 ± 0.11 | 0.60 ± 0.15 | 0.66 ± 0.15 | 0.054 | |
| RV | FAC (%) | 44 ± 7 | 46 ± 10 | 45 ± 7 | 41 ± 9 *,† | 0.001 |
| TV E’ (cm/s) | 4.3 ± 1.4 | 4.9 ± 1.8 | 4.4 ± 1.6 | 4.2 ± 2.0 | 0.129 | |
| TV A’ (cm/s) | 6.3 ± 2.5 | 6.3 ± 2.3 | 5.6 ± 2.2 | 5.4 ± 2.2 | 0.067 | |
| TV S’ (cm/s) | 4.7 ± 1.7 | 4.9 ± 1.8 | 4.8 ± 1.6 | 4.3 ± 1.4 | 0.054 | |
| RV E/E’ | 10.1 ± 4.0 | 9.0 ± 3.3 | 9.7 ± 3.2 | 10.2 ± 3.0 * | 0.048 | |
| TAPSE (mm) | 15.8 ± 2.4 | 15.9 ± 1.8 | 15.7 ± 2.2 | 14.9 ± 1.8 | 0.087 | |
| RV MPI | 0.54 ± 0.13 | 0.52 ± 0.12 | 0.54 ± 0.16 | 0.64 ± 0.21 *,† | <0.001 | |
| Within 1st Investigator | Between 2nd Investigator | p-Value | |
|---|---|---|---|
| E’ | 0.977 (0.970–0.983) | 0.956 (0.941–0.966) | <0.001 |
| A’ | 0.987 (0.984–0.990) | 0.970(0.960–0.977) | <0.001 |
| S’ | 0.982 (0.976–0.986) | 0.966 (0.944–0.978) | <0.001 |
| E/E’ | 0.936 (0.916–0.951) | 0.920 (0.895–0.939) | <0.001 |
| MPI | 0.944 (0.927–0.957) | 0.924 (0.901–0.942) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, N.; Lee, S.H.; Choi, K.W.; Lee, H.; Oh, Y.J. Effects of Positive End-Expiratory Pressure on Pulmonary Oxygenation and Biventricular Function during One-Lung Ventilation: A Randomized Crossover Study. J. Clin. Med. 2019, 8, 740. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050740
Kim N, Lee SH, Choi KW, Lee H, Oh YJ. Effects of Positive End-Expiratory Pressure on Pulmonary Oxygenation and Biventricular Function during One-Lung Ventilation: A Randomized Crossover Study. Journal of Clinical Medicine. 2019; 8(5):740. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050740
Chicago/Turabian StyleKim, Namo, Su Hyun Lee, Kwan Woong Choi, Haeyeon Lee, and Young Jun Oh. 2019. "Effects of Positive End-Expiratory Pressure on Pulmonary Oxygenation and Biventricular Function during One-Lung Ventilation: A Randomized Crossover Study" Journal of Clinical Medicine 8, no. 5: 740. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050740