Expression of Immune System-Related Membrane Receptors CD40, RANK, BAFFR and LTβR is Associated with Clinical Outcome of Operated Non-Small-Cell Lung Cancer Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population, Tissue Specimens and Data Collection
2.2. Transcriptome Analyses of Public Datasets
2.3. Immunohistochemical Analysis
2.4. Evaluation of Immunohistochemistry
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Differences in CD40, BAFFR, RANK and LTβR Expression
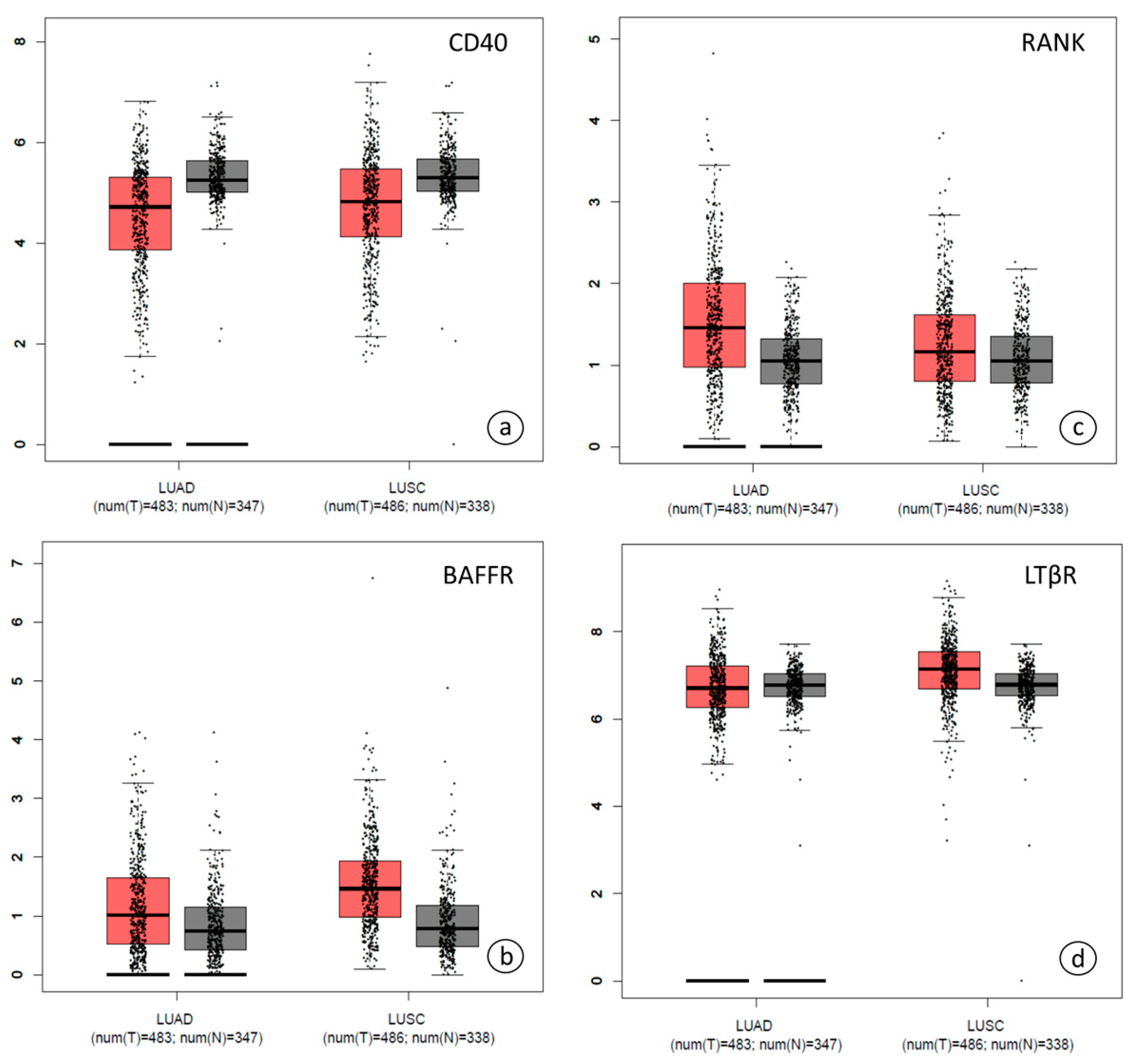
3.2.1. CD40, BAFFR, RANK and LTβR Gene Expression was Similar in Different Groups of Patients and in Different Tissues
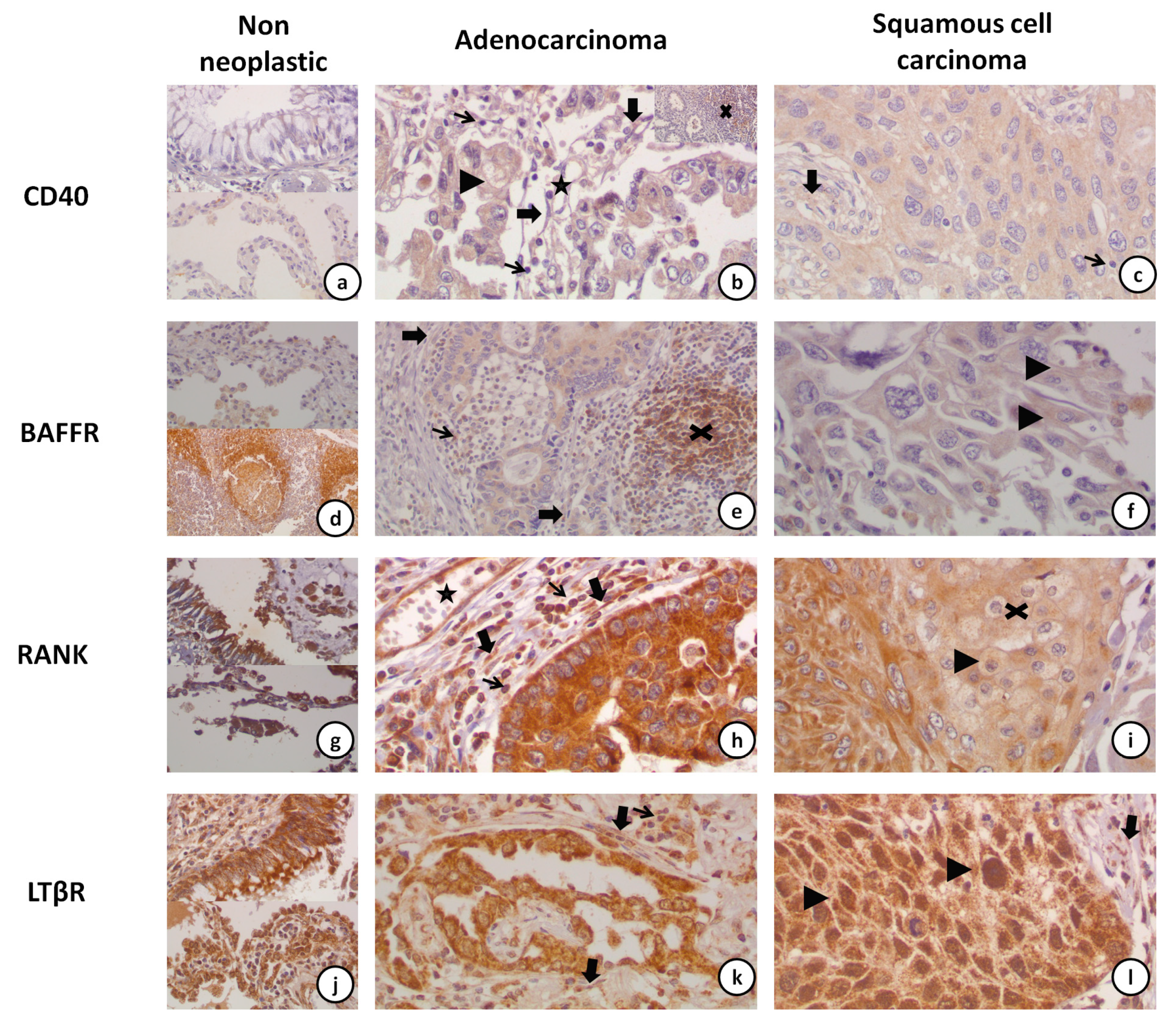
3.2.2. Subcellular Localization of CD40, RANK, BAFFR and LTβR
3.2.3. CD40 and BAFFR Protein Expression Was Lower in NSCLC
3.2.4. Correlation of CD40, BAFFR, RANK and LTβR Expression amongst the Cells of the Tumor Microenvironment (Tumor Cells and TILs/TAMs/CAFs)
3.3. Association of CD40, BAFFR, RANK and LTβR Expression with Clinical Outcome
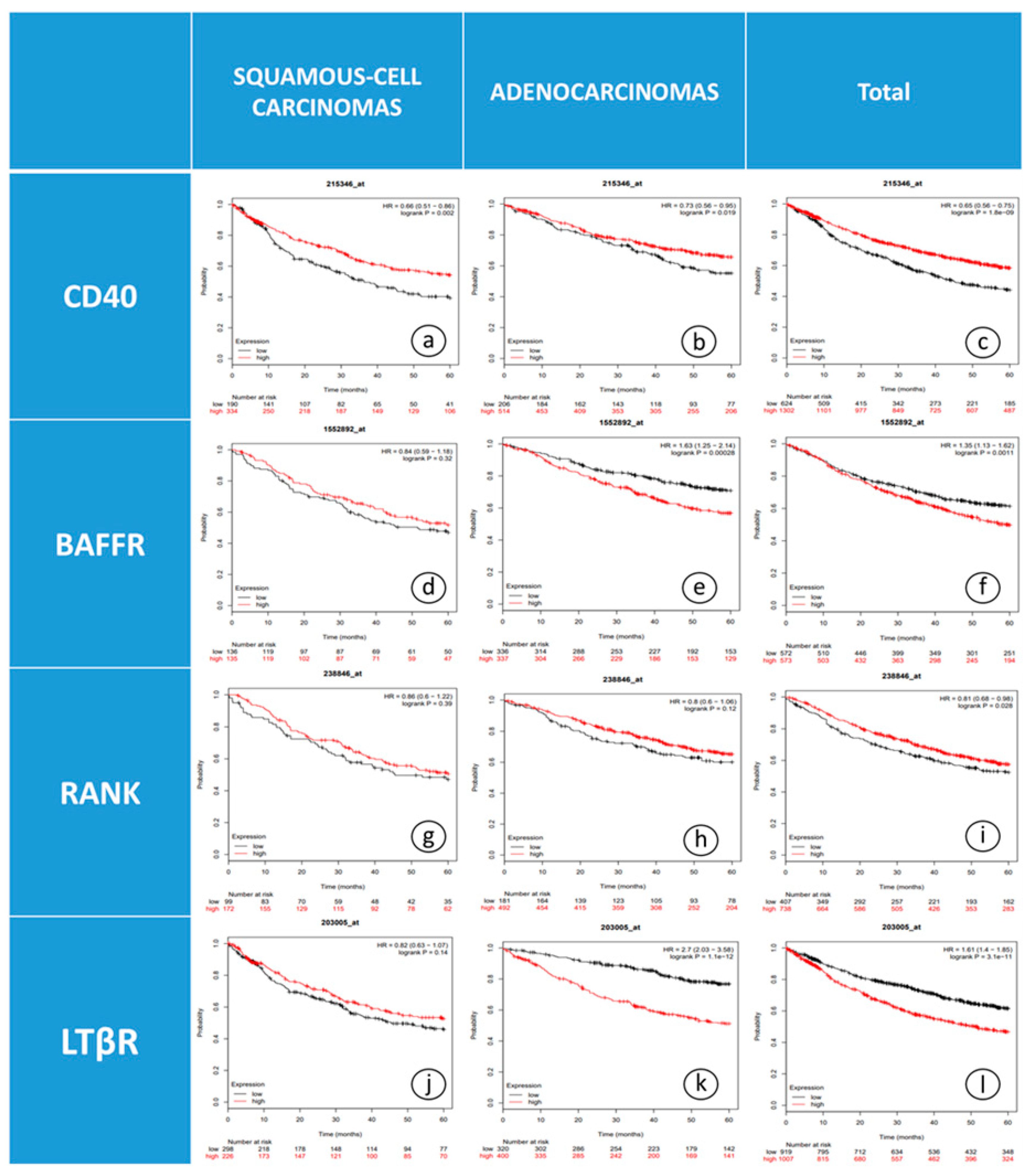
3.3.1. CD40, BAFFR and LTβR mRNA Levels were Associated with OS
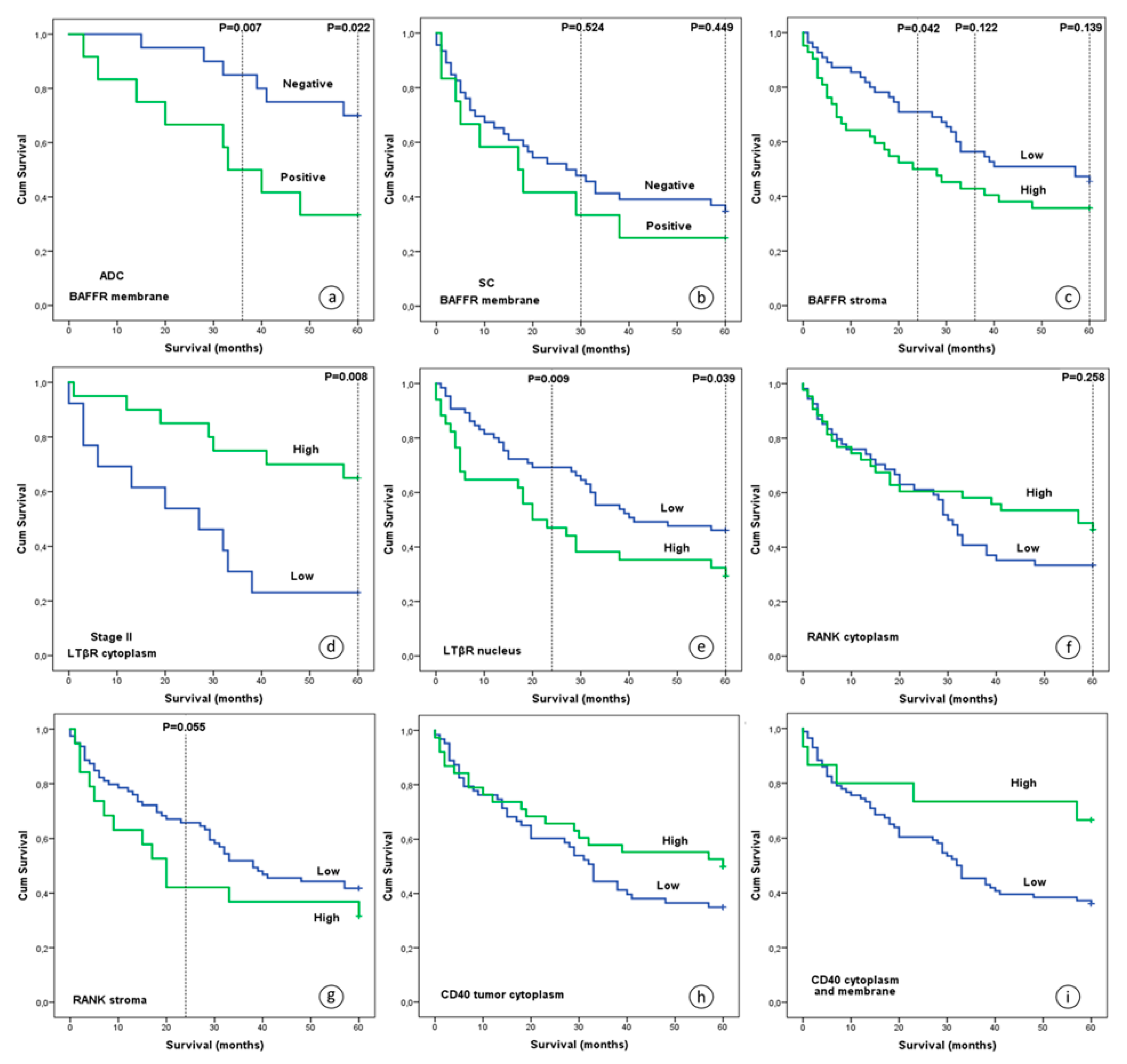
3.3.2. BAFFR, RANK and LTβR Protein Expression Were Associated with OS
3.3.3. CD40 and BAFFR Protein Expression Correlated with Development of Metastasis
3.4. Correlations between Protein Expression and Clinicopathological Characteristics
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Taniguchi, K.; Karin, M. NF-Kappab, Inflammation, Immunity and Cancer: Coming of Age. Nat. Rev. Immunol. 2018, 18, 309–324. [Google Scholar] [CrossRef]
- Godwin, P.; Baird, A.M.; Heavey, S.; Barr, M.P.; O’Byrne, K.J.; Gately, K. Targeting Nuclear Factor-Kappa B to Overcome Resistance to Chemotherapy. Front. Oncol. 2013, 3, 120. [Google Scholar] [CrossRef] [Green Version]
- Karin, M. Nuclear Factor-KappaB in Cancer Development and Progression. Nature 2006, 441, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Tchou-Wong, K.M.; Rom, W.N. NF-KappaB in Lung Tumorigenesis. Cancers 2011, 3, 4258–4268. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhang, L.; Joo, D.; Sun, S.-C. NF-κB Signaling in Inflammation. Signal Transduct. Target. Ther. 2017, 2, 17023. [Google Scholar] [CrossRef] [PubMed]
- Dimitrakopoulos, F.I.; Antonacopoulou, A.G.; Kottorou, A.; Marousi, S.; Koukourikou, I.; Kalofonou, M.; Panagopoulos, N.; Scopa, C.; Dougenis, D.; Papadaki, H.; et al. Variant of BCL3 Gene is Strongly Associated with Five-Year Survival of Non-Small-Cell Lung Cancer Patients. Lung Cancer 2015, 89, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Dimitrakopoulos, F.I.; Kottorou, A.E.; Antonacopoulou, A.G.; Scopa, C.; Dougenis, D.; Papadaki, H.; Kalofonos, H. 701: The Alternative Pathway of NF-kB is Deregulated in NSCLC? Eur. J. Cancer 2014, 50, S169. [Google Scholar] [CrossRef]
- Dimitrakopoulos, F.I.; Antonacopoulou, A.G.; Kottorou, A.; Vlotinou, H.; Panagopoulos, N.D.; Dougenis, D.; Scopa, C.; Papadaki, H.; Kalofonos, H.P. NSCLC and the Alternative Pathway of NF-KappaB: Uncovering an Unknown Relation. Virchows Arch. Int. J. Pathol. 2012, 460, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Dimitrakopoulos, F.-I.D.; Antonacopoulou, A.G.; Kottorou, A.E.; Kalofonou, F.; Scopa, C.D.; Papadaki, D.D.; Kalofonos, H. The Clinical Significance of NF-{kappa}B2, RelB, NIK, and BCL3 Expression in NSCLC. J. Clin. Oncol. 2015, 33, e18511. [Google Scholar]
- Dejardin, E. The Alternative NF-KappaB Pathway from Biochemistry to Biology: Pitfalls and Promises for Future Drug Development. Biochem. Pharmacol. 2006, 72, 1161–1179. [Google Scholar] [CrossRef]
- Beatty, G.L.; Li, Y.; Long, K.B. Cancer Immunotherapy: Activating Innate and Adaptive Immunity through CD40 Agonists. Expert Rev. Anticancer Ther. 2017, 17, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Rihacek, M.; Bienertova-Vasku, J.; Valik, D.; Sterba, J.; Pilatova, K.; Zdrazilova-Dubska, L. B-Cell Activating Factor as a Cancer Biomarker and Its Implications in Cancer-Related Cachexia. BioMed Res. Int. 2015, 2015, 792187. [Google Scholar] [CrossRef]
- Renema, N.; Navet, B.; Heymann, M.-F.; Lezot, F.; Heymann, D. RANK–RANKL Signalling in Cancer. Biosci. Rep. 2016, 36, e00366. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.J.; Seleznik, G.M.; Zeller, N.; Heikenwalder, M. The Unexpected Role of Lymphotoxin Beta Receptor Signaling in Carcinogenesis: From Lymphoid Tissue Formation to Liver and Prostate Cancer Development. Oncogene 2010, 29, 5006–5018. [Google Scholar] [CrossRef]
- Vonderheide, R.H. Prospect of Targeting the CD40 Pathway for Cancer Therapy. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2007, 13, 1083–1088. [Google Scholar] [CrossRef] [Green Version]
- Jellusova, J.; Miletic, A.V.; Cato, M.H.; Lin, W.W.; Hu, Y.; Bishop, G.A.; Shlomchik, M.J.; Rickert, R.C. Context-Specific BAFF-R Signaling by the NF-KappaB and PI3K Pathways. Cell Rep. 2013, 5, 1022–1035. [Google Scholar] [CrossRef] [PubMed]
- Remouchamps, C.; Boutaffala, L.; Ganeff, C.; Dejardin, E. Biology and Signal Transduction Pathways of the Lymphotoxin-Alphabeta/LTbetaR System. Cytokine Growth Factor Rev. 2011, 22, 301–310. [Google Scholar] [CrossRef] [PubMed]
- World Medical, A. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- World Health Organization. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus, and Heart; Travis, W.D., Brambilla, E., Müller-Hermelink, H.K., Harris, C.C., Eds.; IARC Press: Lyon, France, 2004; p. 344. [Google Scholar]
- Tang, Z.; Li, C.; Kang, B.; Gao, G.; Li, C.; Zhang, Z. GEPIA: A Web Server for Cancer and Normal Gene Expression Profiling and Interactive Analyses. Nucl. Acids Res. 2017, 45, W98–W102. [Google Scholar] [CrossRef] [PubMed]
- Tzelepi, V.; Karlou, M.; Wen, S.; Hoang, A.; Logothetis, C.; Troncoso, P.; Efstathiou, E. Expression of Hedgehog Pathway Components in Prostate Carcinoma Microenvironment: Shifting the Balance towards Autocrine Signalling. Histopathology 2011, 58, 1037–1047. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-Tile: A New Bio-Informatics Tool for Biomarker Assessment and Outcome-Based Cut-Point Optimization. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef]
- Ishikawa, K.; Miyamoto, M.; Yoshioka, T.; Kato, T.; Kaji, M.; Ohbuchi, T.; Hirano, S.; Itoh, T.; Dosaka-Akita, H.; Kondo, S. Up-Regulation of CD40 with Juxtacrine Activity in Human Nonsmall Lung Cancer Cells Correlates with Poor Prognosis. Cancer 2008, 113, 530–541. [Google Scholar] [CrossRef] [PubMed]
- Sabel, M.S.; Yamada, M.; Kawaguchi, Y.; Chen, F.A.; Takita, H.; Bankert, R.B. CD40 Expression on Human Lung Cancer Correlates with Metastatic Spread. Cancer Immunol. Immunother. CII 2000, 49, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Van Den Oord, J.J.; Maes, A.; Stas, M.; Nuyts, J.; Battocchio, S.; Kasran, A.; Garmyn, M.; De Wever, I.; De Wolf-Peeters, C. CD40 is a Prognostic Marker in Primary Cutaneous Malignant Melanoma. Am. J. Pathol. 1996, 149, 1953–1961. [Google Scholar] [PubMed]
- Sugimoto, K.; Shiraki, K.; Ito, T.; Fujikawa, K.; Takase, K.; Tameda, Y.; Moriyama, M.; Nakano, T. Expression of Functional CD40 in Human Hepatocellular Carcinoma. Hepatology 1999, 30, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Costello, A.; Rey-Hipolito, C.; Patel, A.; Oakley, K.; Vasco, V.; Calabria, C.; Tuttle, R.M.; Francis, G.L. Thyroid Cancers Express CD-40 and CD-40 Ligand: Cancers that Express CD-40 Ligand may Have a Greater Risk of Recurrence in Young Patients. Thyr. Off. J. Am. Thyr. Assoc. 2005, 15, 105–113. [Google Scholar] [CrossRef]
- Cooke, P.W.; James, N.D.; Ganesan, R.; Wallace, M.; Burton, A.; Young, L.S. CD40 Expression in Bladder Cancer. J. Pathol. 1999, 188, 38–43. [Google Scholar] [CrossRef]
- Pang, X.; Zhang, L.; Wu, J.; Ma, C.; Mu, C.; Zhang, G.; Chen, W. Expression of CD40/CD40L in Colon Cancer, and Its Effect on Proliferation and Apoptosis of SW48 Colon Cancer Cells. J. BUON 2017, 22, 894–899. [Google Scholar]
- Matsumura, Y.; Hiraoka, K.; Ishikawa, K.; Shoji, Y.; Noji, T.; Hontani, K.; Itoh, T.; Nakamura, T.; Tsuchikawa, T.; Shichinohe, T.; et al. CD40 Expression in Human Esophageal Squamous Cell Carcinoma is Associated with Tumor Progression and Lymph Node Metastasis. Anticancer Res. 2016, 36, 4467–4475. [Google Scholar] [CrossRef]
- Hakkarainen, T.; Hemminki, A.; Pereboev, A.V.; Barker, S.D.; Asiedu, C.K.; Strong, T.V.; Kanerva, A.; Wahlfors, J.; Curiel, D.T. CD40 is Expressed on Ovarian Cancer Cells and Can be Utilized for Targeting Adenoviruses. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2003, 9, 619–624. [Google Scholar]
- Li, R.; Chen, W.C.; Pang, X.Q.; Hua, C.; Li, L.; Zhang, X.G. Expression of CD40 and CD40L in Gastric Cancer Tissue and Its Clinical Significance. Int. J. Mol. Sci. 2009, 10, 3900–3917. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.C.; Youde, S.J.; Man, S.; Teale, G.R.; Baxendale, A.J.; Hislop, A.; Davies, C.C.; Luesley, D.M.; Blom, A.M.; Rickinson, A.B.; et al. Activation of CD40 in Cervical Carcinoma Cells Facilitates CTL Responses and Augments Chemotherapy-Induced Apoptosis. J. Immunol. 2005, 174, 41–50. [Google Scholar] [CrossRef]
- He, S.; Zhao, H.; Fei, M.; Wu, Y.; Wang, L.; Zhu, X.; Li, D. Expression of the Co-Signaling Molecules CD40-CD40L and Their Growth Inhibitory Effect on Pancreatic Cancer in Vitro. Oncol. Rep. 2012, 28, 262–268. [Google Scholar] [CrossRef]
- Song, G.; Ni, H.; Zou, L.; Wang, S.; Tian, F.; Liu, H.; Cho, W.C. Expression of CD40 is a Positive Prognostic Factor of Diffuse Large B-cell Lymphoma Treated with R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone). OncoTargets Ther. 2016, 9, 3799–3805. [Google Scholar] [CrossRef]
- Troeger, A.; Glouchkova, L.; Ackermann, B.; Escherich, G.; Meisel, R.; Hanenberg, H.; Den Boer, M.L.; Pieters, R.; Janka-Schaub, G.E.; Goebel, U.; et al. High Expression of CD40 on B-Cell Precursor Acute Lymphoblastic Leukemia Blasts is an Independent Risk Factor Associated with Improved Survival and Enhanced Capacity to Up-Regulate the Death Receptor CD95. Blood 2008, 112, 1028–1034. [Google Scholar] [CrossRef]
- Rodig, S.J.; Shahsafaei, A.; Li, B.; Mackay, C.R.; Dorfman, D.M. BAFF-R, the Major B Cell-Activating Factor Receptor, is Expressed on Most Mature B Cells and B-Cell Lymphoproliferative Disorders. Hum. Pathol. 2005, 36, 1113–1119. [Google Scholar] [CrossRef]
- Li, Y.-J.; Jiang, W.-Q.; Rao, H.-L.; Huang, J.-J.; Xia, Y.; Huang, H.-Q.; Lin, T.-Y.; Xia, Z.-J.; Li, S.; Li, Z.-M. Expression of BAFF and BAFF-R in Follicular Lymphoma: Correlation with Clinicopathologic Characteristics and Survival Outcomes. PLoS ONE 2012, 7, e50936. [Google Scholar] [CrossRef] [PubMed]
- Novak, A.J.; Bram, R.J.; Kay, N.E.; Jelinek, D.F. Aberrant Expression of B-Lymphocyte Stimulator by B Chronic Lymphocytic Leukemia Cells: A Mechanism for Survival. Blood 2002, 100, 2973–2979. [Google Scholar] [CrossRef]
- Pelekanou, V.; Kampa, M.; Kafousi, M.; Darivianaki, K.; Sanidas, E.; Tsiftsis, D.D.; Stathopoulos, E.N.; Tsapis, A.; Castanas, E. Expression of TNF-Superfamily Members BAFF and APRIL in Breast Cancer: Immunohistochemical Study in 52 Invasive Ductal Breast Carcinomas. BMC Cancer 2008, 8, 76. [Google Scholar] [CrossRef]
- Pelekanou, V.; Notas, G.; Theodoropoulou, K.; Kampa, M.; Takos, D.; Alexaki, V.I.; Radojicic, J.; Sofras, F.; Tsapis, A.; Stathopoulos, E.N.; et al. Detection of the TNFSF Members BAFF, APRIL, TWEAK and Their Receptors in Normal Kidney and Renal Cell Carcinomas. Anal. Cell. Pathol. 2011, 34, 49–60. [Google Scholar] [CrossRef]
- Pelekanou, V.; Notas, G.; Kampa, M.; Tsentelierou, E.; Stathopoulos, E.N.; Tsapis, A.; Castanas, E. BAFF, APRIL, TWEAK, BCMA, TACI and Fn14 Proteins are Related to Human Glioma Tumor Grade: Immunohistochemistry and Public Microarray Data Meta-Analysis. PLoS ONE 2013, 8, e83250. [Google Scholar] [CrossRef]
- Kohno, T.; Daa, T.; Otani, H.; Shimokawa, I.; Yokoyama, S.; Matsuyama, T. Aberrant Expression of BAFF Receptor, a Member of the Tumor Necrosis Factor Receptor Family, in Malignant Cells of Nonhematopoietic Origins. Genes Cells Devoted Mol. Cell. Mech. 2008, 13, 1061–1073. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, M.; Hiasa, Y.; Kumagi, T.; Yamanishi, H.; Azemoto, N.; Kobata, T.; Matsuura, B.; Abe, M.; Onji, M. Increased B Cell-Activating Factor Promotes Tumor Invasion and Metastasis in Human Pancreatic Cancer. PLoS ONE 2013, 8, e71367. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; He, X.; Zhu, Y.; Yan, T.; Ma, H.; Zhang, X. Abnormally High Expression of BAFF on T Lymphocytes from Lung Cancer-Associated Pleural Effusions and Its Potent Anti-Tumor Effect. Acta Biochim. Biophys. Sin. 2007, 39, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Guo, W.; Ren, T.; Lou, Z.; Lu, X.; Zhang, S.; Lu, Q.; Sun, Y. Differential Expression of the RANKL/RANK/OPG System is Associated with Bone Metastasis in Human Non-Small Cell Lung Cancer. PLoS ONE 2013, 8, e58361. [Google Scholar] [CrossRef]
- Sisay, M.; Mengistu, G.; Edessa, D. The RANK/RANKL/OPG System in Tumorigenesis and Metastasis of Cancer Stem Cell: Potential Targets for Anticancer Therapy. OncoTargets Ther. 2017, 10, 3801–3810. [Google Scholar] [CrossRef]
- Palafox, M.; Ferrer, I.; Pellegrini, P.; Vila, S.; Hernandez-Ortega, S.; Urruticoechea, A.; Climent, F.; Soler, M.T.; Munoz, P.; Vinals, F.; et al. RANK Induces Epithelial-Mesenchymal Transition and Stemness in Human Mammary Epithelial Cells and Promotes Tumorigenesis and Metastasis. Cancer Res. 2012, 72, 2879–2888. [Google Scholar] [CrossRef]
- Lau, T.S.; Chung, T.K.; Cheung, T.H.; Chan, L.K.; Cheung, L.W.; Yim, S.F.; Siu, N.S.; Lo, K.W.; Yu, M.M.; Kulbe, H.; et al. Cancer Cell-Derived Lymphotoxin Mediates Reciprocal Tumour-Stromal Interactions in Human Ovarian Cancer by Inducing CXCL11 in Fibroblasts. J. Pathol. 2014, 232, 43–56. [Google Scholar] [CrossRef]
- Lukashev, M.; LePage, D.; Wilson, C.; Bailly, V.; Garber, E.; Lukashin, A.; Ngam-ek, A.; Zeng, W.; Allaire, N.; Perrin, S.; et al. Targeting the Lymphotoxin-Beta Receptor with Agonist Antibodies as a Potential Cancer Therapy. Cancer Res. 2006, 66, 9617–9624. [Google Scholar] [CrossRef]
- Dhawan, P.; Su, Y.; Thu, Y.M.; Yu, Y.; Baugher, P.; Ellis, D.L.; Sobolik-Delmaire, T.; Kelley, M.; Cheung, T.C.; Ware, C.F.; et al. The Lymphotoxin-Beta Receptor is an Upstream Activator of NF-KappaB-Mediated Transcription in Melanoma Cells. J. Biol. Chem. 2008, 283, 15399–15408. [Google Scholar] [CrossRef]
- Ganeff, C.; Remouchamps, C.; Boutaffala, L.; Benezech, C.; Galopin, G.; Vandepaer, S.; Bouillenne, F.; Ormenese, S.; Chariot, A.; Schneider, P.; et al. Induction of the Alternative NF-KappaB Pathway by Lymphotoxin Alphabeta (LTalphabeta) Relies on Internalization of LTbeta Receptor. Mol. Cell. Biol. 2011, 31, 4319–4334. [Google Scholar] [CrossRef]
- Force, W.R.; Glass, A.A.; Benedict, C.A.; Cheung, T.C.; Lama, J.; Ware, C.F. Discrete Signaling Regions in the Lymphotoxin-Beta Receptor for Tumor Necrosis Factor Receptor-Associated Factor Binding, Subcellular Localization, and Activation of Cell Death and NF-KappaB Pathways. J. Biol. Chem. 2000, 275, 11121–11129. [Google Scholar] [CrossRef] [PubMed]
- Kubokura, H.; Koizumi, K.; Harada, A.; Yoshino, N.; Okada, D.; Hirata, T.; Kawamoto, M.; Shimizu, K. The Relationship between CD40 and Lymph Node Metastasis on Lung Adenocarcinomas by Using Immuno Histochemical Staining. Cancer Res. 2008, 68, 2158. [Google Scholar]
- Ingersoll, S.B.; Langer, F.; Walker, J.M.; Meyer, T.; Robson, T.; Amaya, M.; Desai, H.; Francis, J.L.; Amirkhosravi, A. Deficiencies in the CD40 and CD154 Receptor-Ligand System Reduce Experimental Lung Metastasis. Clin. Exp. Metastasis 2009, 26, 829–837. [Google Scholar] [CrossRef]
- Amirkhosravi, A.; Ingersoll, S.B.; Robson, T.; Langer, F.; Walker, J.; Francis, J.L. Blood-Borne, but Not Endothelial CD40 Promotes Experimental Lung Metastasis. Blood 2006, 108, 1092. [Google Scholar]
- Brouty-Boye, D.; Pottin-Clemenceau, C.; Doucet, C.; Jasmin, C.; Azzarone, B. Chemokines and CD40 Expression in Human Fibroblasts. Eur. J. Immunol. 2000, 30, 914–919. [Google Scholar] [CrossRef]
- Wang, L.; Cao, L.; Wang, H.; Liu, B.; Zhang, Q.; Meng, Z.; Wu, X.; Zhou, Q.; Xu, K. Cancer-Associated Fibroblasts Enhance Metastatic Potential of Lung Cancer Cells through IL-6/STAT3 Signaling Pathway. Oncotarget 2017, 8, 76116–76128. [Google Scholar] [CrossRef]
- Tada, S.; Yasui, T.; Nakatsuji, Y.; Okuno, T.; Koda, T.; Mochizuki, H.; Sakoda, S.; Kikutani, H. BAFF Controls Neural Cell Survival through BAFF Receptor. PLoS ONE 2013, 8, e70924. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Lin-Lee, Y.C.; Pham, L.V.; Tamayo, A.T.; Yoshimura, L.C.; Ford, R.J. BAFF-R Promotes Cell Proliferation and Survival through Interaction with IKKbeta and NF-KappaB/c-Rel in the Nucleus of Normal and Neoplastic B-Lymphoid Cells. Blood 2009, 113, 4627–4636. [Google Scholar] [CrossRef]
- Tiwari, N.; Gheldof, A.; Tatari, M.; Christofori, G. EMT as the Ultimate Survival Mechanism of Cancer Cells. Sem. Cancer Biol. 2012, 22, 194–207. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Y.J.; Jiang, W.Q.; Rao, H.L.; Huang, J.J.; Xia, Y.; Bi, X.; Sun, P.; Huang, H.Q.; Lin, T.Y.; et al. Expression of BAFF-R, but not BAFF, is an Independent Prognostic Factor in Diffuse Large B-Cell Lymphoma Patients Treated with R-CHOP. Ann. Hematol. 2015, 94, 1865–1873. [Google Scholar] [CrossRef]
- Fernandes, M.T.; Dejardin, E.; Dos Santos, N.R. Context-Dependent Roles for Lymphotoxin-Beta Receptor Signaling in Cancer Development. Biochim. Biophys. Acta 2016, 1865, 204–219. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Clonality/Source | Company | Catalogue number | Clone | Dilution | Antigen Retrieval Conditions | Incubation Time |
|---|---|---|---|---|---|---|---|
| RANK | M/mouse | R&D systems Minneapolis, MN, USA | MAB6831 | 80707 | 1:300 | 1.2 mM EDTA, pH 8.0 | Overnight 4 °C |
| LTβR | P/rabbit | Abcam Cambridge, UK | Ab193449 | - | 1:750 | 8 mM sodium citrate, pH 6.0 | Overnight 4 °C |
| CD40 | M/mouse | SANTA CRUZ, Biotechnology Dallas, TX, USA | Sc-13528 | LOB-11 | 1:20 | 1.2 mM EDTA, pH 8.0 | Overnight 4 °C |
| BAFFR | M/mouse | SANTA CRUZ, Biotechnology Dallas, TX, USA | Sc-32774 | 11C1 | 1:20 | 1.2 mM EDTA, pH 8.0 | Overnight 4 °C |
| Clinicopathological Characteristics | Cases n (%) |
|---|---|
| Total | 119 (100) |
| Age (years) Median (range) | 66 (42–84) |
| Gender | |
| Total | 119 (100) |
| Male | 112 (94.1) |
| Female | 7 (5.9) |
| Smoking (pack-years) | |
| Total | 119 (100) |
| Cases (%) | 49 (41.2) |
| Mean (range) | 90.31 (20–165) |
| NA | 90 (58.8) |
| Primary location | |
| Total | 119 (100) |
| Left lung | 45 (37.8) |
| Right lung | 74 (62.2) |
| NA | - |
| Histology | |
| Total | 119 (100) |
| Squamous | 67 (56.3) |
| Adenocarcinoma | 42 (35.3) |
| Large carcinoma | 10 (8.4) |
| NA | - |
| Stage | |
| Total | 119 (100) |
| I | 43 (36.1) |
| II | 37 (31.1) |
| III | 39 (32.8) |
| NA | - |
| Grade | |
| Total | 119 (100) |
| I | 5 (4.2) |
| II | 55 (46.2) |
| III | 52 (43.7) |
| NA | 7 (5.9) |
| Maximum diameter (cm) | |
| Total | 119 (100) |
| Cases (%) | 108 (99.2) |
| Mean (range) | 5.35 (1.10–21.00) |
| NA | 1 (0.8) |
| Lymph node infiltration | |
| Total | 119 (100) |
| No | 63 (52.9) |
| Yes | 52 (43.7) |
| NA | 4 (3.4) |
| Metastasis (adrenals) | |
| Total | 119 (100) |
| No | 24 (20.2) |
| Yes | 3 (2.5) |
| NA | 92 (77.3) |
| Metastasis (liver) | |
| Total | 119 (100) |
| No | 25 (21.0) |
| Yes | 4 (3.4) |
| NA | 90 (75.6) |
| Metastasis (brain) | |
| Total | 119 (100) |
| No | 24 (20.2) |
| Yes | 7 (5.9) |
| NA | 88 (73.9) |
| Metastasis (bone) | |
| Total | 119 (100) |
| No | 19 (16.0) |
| Yes | 14 (11.8) |
| NA | 86 (72.3) |
| Metastasis (adrenals-liver-brain-bone) | |
| Total | 119 (100) |
| No | 8 (6.7) |
| Yes | 28 (23.5) |
| NA | 83 (69.7) |
| Survival (two years) | |
| Total | 119 (100) |
| Dead | 46 (38.7) |
| Alive | 71 (59.7) |
| NA | 2 (1.7) |
| Survival (three years) | |
| Total | 119 (100) |
| Dead | 59 (49.6) |
| Alive | 56 (47.1) |
| NA | 4 (3.4) |
| Survival (five years) | |
| Total | 119 (100) |
| Dead | 70 (58.8) |
| Alive | 45 (37.8) |
| NA | 4 (3.4) |
| Relapse | |
| Total | 119 (100) |
| No | 14 (11.8) |
| Yes | 16 (13.4) |
| NA | 89 (74.8) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimitrakopoulos, F.-I.D.; Kottorou, A.E.; Antonacopoulou, A.G.; Panagopoulos, N.; Scopa, C.; Kalofonou, M.; Dougenis, D.; Koutras, A.; Makatsoris, T.; Tzelepi, V.; et al. Expression of Immune System-Related Membrane Receptors CD40, RANK, BAFFR and LTβR is Associated with Clinical Outcome of Operated Non-Small-Cell Lung Cancer Patients. J. Clin. Med. 2019, 8, 741. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050741
Dimitrakopoulos F-ID, Kottorou AE, Antonacopoulou AG, Panagopoulos N, Scopa C, Kalofonou M, Dougenis D, Koutras A, Makatsoris T, Tzelepi V, et al. Expression of Immune System-Related Membrane Receptors CD40, RANK, BAFFR and LTβR is Associated with Clinical Outcome of Operated Non-Small-Cell Lung Cancer Patients. Journal of Clinical Medicine. 2019; 8(5):741. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050741
Chicago/Turabian StyleDimitrakopoulos, Foteinos-Ioannis D., Anastasia E. Kottorou, Anna G. Antonacopoulou, Nikolaos Panagopoulos, Chrisoula Scopa, Melpomeni Kalofonou, Dimitrios Dougenis, Angelos Koutras, Thomas Makatsoris, Vassiliki Tzelepi, and et al. 2019. "Expression of Immune System-Related Membrane Receptors CD40, RANK, BAFFR and LTβR is Associated with Clinical Outcome of Operated Non-Small-Cell Lung Cancer Patients" Journal of Clinical Medicine 8, no. 5: 741. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8050741