1. Introduction
Asthma is the most common chronic lower respiratory disease in childhood throughout the world. Current guidelines are highly in favor of documenting reversible airflow obstruction as a cardinal characteristic of asthma, both for the diagnosis and the subsequent monitoring of asthma, preferably prior to controller treatment, in all age groups [
1]. The most widely used pulmonary function test is spirometry, which estimates lung volumes by rapid and maximal inspiratory and expiratory maneuvers that are often difficult to perform even in older children.
In contrast, the Forced Oscillation Technique (FOT) superimposes small air pressure perturbations on the natural breathing of a subject to measure the mechanical properties of the lungs [
2]. The Impulse Oscillometry System (IOS), based on the aforementioned technique, measures the resistance and reactance of the respiratory system, thus providing an indirect analysis of lung function through the use of short pulses (impulses) of acoustic waves—most commonly over a range of frequencies (5Hz to 20Hz)—applied at the mouth, during spontaneous, quiet breathing [
3]. IOS has been used to distinctively quantify the airflow limitation in the central and peripheral airways [
4,
5]. Low oscillation frequencies like 5 Hz can penetrate the periphery of the bronchial tree (diameter <2 mm) and, therefore, resistance of the respiratory system at 5 Hz (R5) reflects obstruction in both the peripheral and the central airways. On the contrary, higher frequencies cannot be transmitted distally. Thus, resistance of the respiratory system at 20 Hz (R20) reflects the proximal airways resistance. The change in resistance from low to high-frequency ranges (e.g., R5 minus R20, R(5−20)) has been identified as an index of the peripheral airways resistance only, and has been used as a potential marker of small airways obstruction [
6].
IOS has been developed as a patient-friendly lung function test that minimizes demands on the patient and requires only passive cooperation with normal breathing through the mouth. It has been successfully used for assessing lung function and asthma control in healthy and asthmatic children [
5,
6], including preschoolers, and in patients who recently underwent surgery or are unable to perform spirometry, both as an adjunct or even alternative to standard spirometry [
4,
7,
8].
Pediatric reference values and positive bronchodilation responses indicating peripheral air trapping have been standardized and published [
9]. R5 is the main parameter to assess bronchodilation. However, no consensus has been reached on the optimal cutoff values that could discriminate patients from healthy individuals. These values vary between 20 and 50% and have been used to diagnose and evaluate the severity of chronic respiratory diseases in childhood or compare to a number of techniques routinely used to assess lung function [
10,
11,
12,
13,
14]. Nevertheless, none of the studies has prospectively followed either baseline fluctuations of IOS parameters or fluctuations in the course of virus-induced wheeze episodes in preschool children.
In this prospective study, we aimed to longitudinally evaluate changes in airflow limitation and bronchodilator responsiveness by means of the main IOS resistance parameters, in steroid-naïve four- to six-year-old children during the course of a virus-induced wheezing episode. Moreover, IOS feasibility and reproducibility, in addition to the diagnostic properties of the main IOS resistance parameters were examined.
3. Results
All 98 consecutively examined children were able to perform an acceptable IOS effort and consent to be included in the study. Five of them were unable to achieve an acceptable spirometric maneuver with FET ≥0.5 s, even after three visits of continuous training efforts, and were excluded. All 93 finally recruited children (mean age 4.5 ± 0.4 years) were able to perform an IOS effort both at baseline and during the wheezing episodes. None of the children needed more than three demonstrations and an equal number of efforts during their initial visit to accomplish a technically correct IOS maneuver. Among them, 49 (52.7%) were able to perform a correct spirometric maneuver during the first visit, 32 (34.4%) needed two visits, and the remaining 12 (12.9%) needed three visits to be trained well enough to perform an acceptable and repeatable spirometric maneuver. Two out of these 12 were not able to perform spirometry and an acceptable IOS effort during their first wheezing episode.
Regular follow-up visits occurred every 40 ± 4 days. Four children were lost to follow-up. Among the remaining 89 children, 43 had at least one wheezing episode 0.6 ± 0.3 years after recruitment. This corresponds to a median of five visits for each patient. According to the study protocol, among these regular visits, the very last one was considered the baseline.
Following initial assessment at the beginning of an episode (day 0), the children were re-evaluated 10 ± 1 days (day 10) and 30 ± 3 days (day 30) later. None of the children reported wheezing unrelated to an apparent respiratory tract infection.
There was no significant seasonality for the wheezing episodes except the period from early May until late September (fewer episodes).
The variability of R5 and R20 among different visits was also estimated. Measurements at regular visits and during the course of a wheezing episode were examined. Pre- and post-bronchodilation R5 variability ranged from 2.9% to 33.7% (median: 15%, upper 95% percentile: 32.3%) and 1% to 27.7% (median 10.2%, upper 95% percentile 23.4%), respectively. Pre- and post-bronchodilation R20 variability ranged from 3% to 19.2% (median 8%, upper 95% percentile: 18.5%) and 1.7% to 25% (median 7%, upper 95% percentile: 16.5%).
The baseline demographic and somatometric characteristics and IOS measurements were similar between atopic children, non-atopic children, and children completing the study without any wheezing episode. Bronchodilation responses assessed by R5 and R20 did not differ either (
Table 1 and
Supplementary Table S1).
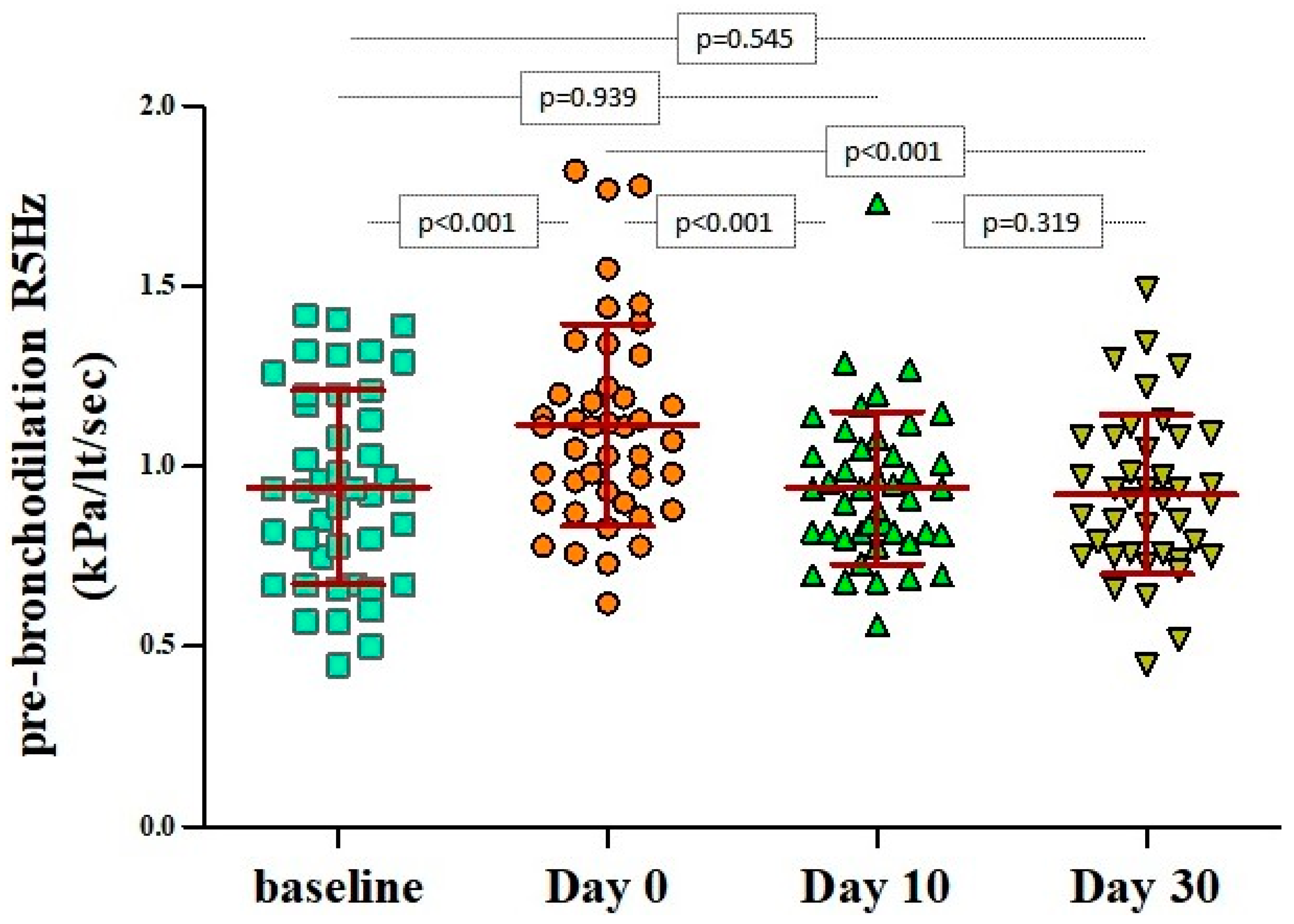
During the first 48 h from the beginning of a wheezing episode (day 0), pre-bronchodilation R5 values were significantly higher than their respective baseline values (1.114 ± 0.280 kPa/lt/sec vs 0.943 ± 0.269 kPa/lt/sec,
p < 0.001). The aforementioned measurements returned to baseline levels within 10 days from the initiation of the episode (
Figure 1). There were no significant differences in respect to the atopic status at all time points (
Supplementary Table S2).
A similar fluctuation pattern, independent of the atopic status, was recorded for R(5−20) values, namely day 0 vs baseline: 0.314 ± 0.163 kPa/lt/sec vs 0.186 ± 0.115 kPa/lt/sec, respectively, p < 0.001. In respect to the R20, a small but significant increase was noted on day 0 compared to baseline, namely 0.801 ± 0.162 kPa/lt/sec vs 0.757 ± 0.191 kPa/lt/sec, respectively, p = 0.048.
R5 and R20 were not found to be significantly related to age, gender, and somatometric measures (cross-sectional logistic regression models at each time point and longitudinal GEE models). Gender and height, however, are used by the predicted equations to estimate the equipment’s default normal reference values. Pairwise correlation coefficients, although statistically significant, did not indicate strong correlations between reference/predicted values and actual values for both pre-bronchodilation R5 and R20 with Pearson’s correlation coefficients 0.522 vs 0.415 respectively,
p < 0.001 (
Supplementary Figures S1 and S2). The same applied for the post-bronchodilation values with Pearson’s correlation coefficients 0.496 and 0.308, respectively,
p < 0.001 (
Supplementary Figures S3 and S4). Independence of age, height and weight and suboptimal reference/predicted values suggested that, at least for the examined ages (four to six years of age), the personal best baseline measurement (lowest values) should be the reference values for each individual. Therefore, the reference/predicted values were not taken into consideration in any of the performed calculations. Additional information can be found in this article’s
supplementary data.
All post-bronchodilation values were significantly different in relation to the respective pre-bronchodilation at all time points for both R5 and R20 (
Table 2). Post-bronchodilation R5 values on day 0 were similar to the baseline pre-bronchodilation values, reflecting the reversible airway obstruction occurring at the beginning of a wheezing episode both in atopic and non-atopic children (
Table 2).
In particular, bronchodilation responses assessed by ΔR5 were significantly more pronounced only during the first 48 h from the initiation of the wheezing episode (day 0: −23.9% ± 12.1% versus baseline: −12% ± 13.5%,
p < 0.001), irrespectively of atopic status (
Table 2 and
Figure 2). The same applied for the ΔR(5−20), as depicted in
Figure 3. Bronchodilation responses measured with ΔR20 values on day 0 did not differ from the responses recorded at baseline or on days 10 and 30 (
Figure 4), therefore excluding any potential diagnostic value of ΔR20 to classify wheezing episodes correctly.
ΔR5 and ΔR(5−20) were additionally examined as potential diagnostic markers of clinically significant increase in peripheral resistance (assessed during a wheezing episode) in comparison with measures during asymptomatic periods (baseline, day 10, and day 30). For this reason, a ROC analysis was performed. The models examined were unadjusted since none of the other parameters was found to be significant.
The AUCs were 0.725 and 0.671 for ΔR5 and ΔR(5–20) (p = 0.118). Although the AUCs were not significantly different, the higher number for the ΔR5Hz and the simplicity of its calculation render it preferable.
In the ROC analysis, a value of ΔR5 ≤−46.4% accurately classified 80.6% of the wheezing episodes, while values ≤−35.1% correctly identified 77.3% of them (
Supplementary Figure S5). Selected cutoff values for ΔR5 and their respective sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), are presented in
Table 3.
4. Discussion
To our knowledge, this is the first study to prospectively assess IOS indices in virus-induced wheezing illnesses, suggesting that this method could be used in this age group, where spirometry might not be feasible for a substantial proportion of the children.
The IOS technique is easy to perform in preschoolers. All recruited children were trained within a few minutes, and more importantly, none of them experienced difficulties in cooperating during the episode. On the contrary, during the recruitment period, 44 out of 93 children (47.3%) needed more than a regular (according to the study protocol) visit to be properly trained in order to perform a correct spirometric effort, while two of them did not achieve a technically acceptable spirometric maneuver during the episode. Taking into consideration the fact that measurements were performed in a research setting, it is rather self-explanatory that, in everyday clinical practice, spirometry might be quite time-consuming for the medical personnel, thus indisputably supporting the IOS’s superiority in this age group. Since there is an unmet need for objective measures in preschoolers with asthma-related symptoms, seeing that the documentation of reversibility using spirometry is often problematic due to effort dependency, IOS merits the consideration of being included in the diagnostic and therapeutic algorithm.
In particular, we showed that, in preschool children with virus-induced wheeze, IOS indices mainly reflecting peripheral airways, such as R5, are indicative of airflow limitation during an asthma-associated episode. R5 values increased significantly, while bronchodilation responses were more pronounced upon the initiation of the wheezing illness than at baseline. Fluctuations of the IOS resistance parameters resemble the correspondent fluctuations of symptoms (noisy breathing, cough, and shortness of breath), airway inflammation (FeNO) and spirometric parameters (such as FEV
0.5)—as shown in our previously published study, indicating that these episodes share common characteristics with the well-defined asthma exacerbations in older children [
18].
In general, the within- and between-visit variability of R5 and R20 is estimated to be up to 10%. This variability indicates acceptable repeatability among multiple efforts performed by the same subject [
22]. In children, this variability is expected to be higher and has been estimated to be up to 16% for measurements within the same day or up to 30% among several weeks [
7,
10,
19,
23,
24]. When assessing post-bronchodilation values, their variability is expected to vary even more, with coefficients of variation twice the amount of these reported for measurements before bronchodilation [
19]. This was also the case in our cohort. The median variability ranged from 7% to 15% after taking into consideration pre- and post- bronchodilation measurements for R5 and R20 at regular visits and during the course of a wheezing episode. The variability did not differ significantly before and after bronchodilation and, on both occasions, it was within the acceptable extent, suggesting excellent repeatability and reliability in recorded measurements at different time points.
In our cohort, moderate to low correlations (ranging from 0.308 to 0.522) were found between predicted and recorded values for both R5 and R20, before and after bronchodilation. Moreover, neither pre- nor post-bronchodilation R5 and R20 values were found to be correlated with either age, gender, or somatometric parameters. Predicted values for R5 and R20 were based on gender- and height-adjusted existing reference values from a Swedish and a Polish study, as recommended by the manufacturer [
20,
21]. In the Swedish study by Denker et al. [
20], 350 children, 2.1 to 11.1 years old with height 90–160 cm were examined. The investigators found significant correlations with height but weak with weight for both R5 and R20. No significant gender-related difference was found for respiratory resistance. The investigators stated that there were more observations in the height interval 130–145 cm (vs. 107–121 cm in our study population). They do not provide information about the number of children between the 4–6 year of age but based on the height information, it is clear that the predicted equations are weighted for older and higher children and are not representative for preschoolers. In the Polish study by Nowowiejska et al. [
21], 626 children, 3.1–18.9 years old (mean age for boys 10.6 years and for girls 10.9 years), with height 95–193 cm (mean height for boys 144.8 cm and for girls 141.9 cm) were examined. Similar correlations with the Swedish study were found for both R5 and R20. Again, the predicted equations were weighted over older and higher children.
In general, young children exhibit higher pulmonary resistance than older children and adults, and, therefore, airway resistance is inversely proportional to age, especially at lower frequencies [
25]. In a recent meta-analysis, a correlation with anthropometric variables has been suggested too [
26]. The lack of similar correlations in our study could be explained by the narrow range of height and weight in the sample of 4- to 6-year-old children examined. The Polish and Swedish studies provide predicted equations with anthropometric data based mainly on older and higher children, with values over a wide spectrum. Thus, extrapolating data in younger and smaller children appears to provide suboptimal reference values. Additionally, it should be underscored that the differences in ethnicity might also influence the estimated reference values which do not seem to be appropriate at least for the Greek children.
Nevertheless, based on the low variability and excellent repeatability in our study, measures up to six months apart (based on this study average observational period until a wheezing episode occurred), even during different seasons, could be considered stable and independent of known confounders like gender, height or weight. For these reasons, at least in this age-group, reference values are not recommended, until appropriate studies are conducted. An individualized approach using the personal best value, recorded either when the child is asymptomatic or at least 10 days after a mild wheezing episode occurs, is recommended. These values can be used up to at least six months apart to follow-up mild wheezers.
Atopy does not seem to affect the resistance baseline measurements or the bronchodilation responses either when these parameters are assessed cross-sectionally or longitudinally. This finding has also been shown in spirometry and FE
NO in preschoolers [
18]. This independence could be explained by the intermittent, short-lasting inflammatory responses during mild wheezing episodes in our cases. It remains to be shown [
27] whether the probably new, atopy-related inflammation could predispose patients to a more chronic inflammatory process since multiple relapses could lead to alterations in the peripheral resistance measures and bronchodilation responses in atopics.
R5 and R(5−20) values, as indicators of bronchial obstruction, increased significantly during wheezing episodes and spontaneously returned to baseline within 10 days. Post-bronchodilation R5 values on day 0 were similar to the pre-bronchodilation baseline values, reflecting a reversible airway obstruction at the beginning of a wheezing episode, independently of atopic status as has previously been shown for FEV
0.5 [
18].
Mean bronchodilation responses were significantly higher at the beginning of the episode compared to the respective changes at baseline or on day 10 and 30 for ΔR5 (representing the total airway resistance) and ΔR(5−20) (representing peripheral resistance) but not for ΔR20 (representing the resistance of the large airways). Considering the resistance that each of these variables reflects, this is to be expected. In particular, the bronchodilation responses assessed by ΔR5 were more pronounced within the first 48 h from the initiation of the wheezing episode than the responses assessed by ΔR(5−20). When both ΔR5 and ΔR(5−20) were examined for their potential diagnostic value in discriminating clinically significant increase in peripheral resistance during the first days of a wheezing episode (day 0, day 10 and day 30), compared to measurements during asymptomatic periods (baseline) their AUCs were not significantly different (0.725 vs 0.671, respectively). Nevertheless, the higher absolute magnitude of AUCΔR5 renders this parameter preferable for analyzing performance characteristics with a ROC analysis.
Indeed, the ROC analysis provided specific diagnostic cutoff values. Based on the analysis of this cohort, the optimal cutoff point with the highest sensitivity and specificity was found to be −20.5% (
Table 3). Taking into account that the cutoff values have been calculated in patients using measurements even during a wheezing episode, the bronchodilation magnitude is expected to be overestimated in healthy individuals of similar age, and, hence, the proposed cutoff values are expected to be of greater diagnostic value.
The major strength of this study is the steroid-naïve cohort that has been longitudinally examined, providing robust data. To our knowledge, this is the first study to assess airflow limitation in preschool children experiencing wheezing episodes with such study design, that is, by utilizing the IOS technique, and it is also the first time cutoff values have been calculated based on longitudinal measures during and outside an episode for a short period, to adjust for intra- and inter-variability. Considering the fact that the two most likely sources to rely on for the calculation of cutoffs are either population surveys—using only non-wheezers—or studies comparing wheezers with non-wheezers during asymptomatic periods, the data of this study are expected to be more reliable.
A weakness of the study is the lack of a healthy control group because of ethical considerations regarding salbutamol administration to healthy children [
28]. This issue has been overcome by assessing the value of a personalized approach and proving that the personal best value is reliable enough to follow up with such patients. Moreover, the sample was small, although the multiple measurements per studied child provided robust longitudinal analyses. Last but not least, it is not known if the inferences could be applied in children with severe viral-induced wheezing episodes.
In summary, we have shown that IOS is an easy, highly reproducible, and sensitive technique that can be successfully performed to assess airflow limitation objectively in preschool children with virus-induced wheezing illnesses. The study design supports the superiority of the longitudinal approach of such data, suggesting, that reference or predicted values, although necessary, are suboptimal, and that an individualized approach utilizing the personal best values as the personal reference is useful and reliable. Among the commonly measured parameters, the R5 seems to be the best to assess clinically significant fluctuations and bronchodilation responses suggestive of airflow limitation. Cutoff values do have diagnostic properties that can help identify significant bronchodilation responses. Considering the difficulties in examining preschoolers using spirometry and the time required to train them and perform an acceptable spirometric maneuver, IOS could be suggested as the future gold standard to examine airflow limitation in children even in everyday clinical practice. Further studies with similar design are needed for children with persistent or moderate to severe symptoms.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}