Association between Albumin-Bilirubin Grade and Non-Protein Respiratory Quotient in Patients with Chronic Liver Diseases

Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Measurement of npRQ by Indirect Calorimetry
2.3. SMI and ECW to TBW Ratio Using BIA
2.4. Statistical Considerations
3. Results
3.1. Patient Baseline Characteristics
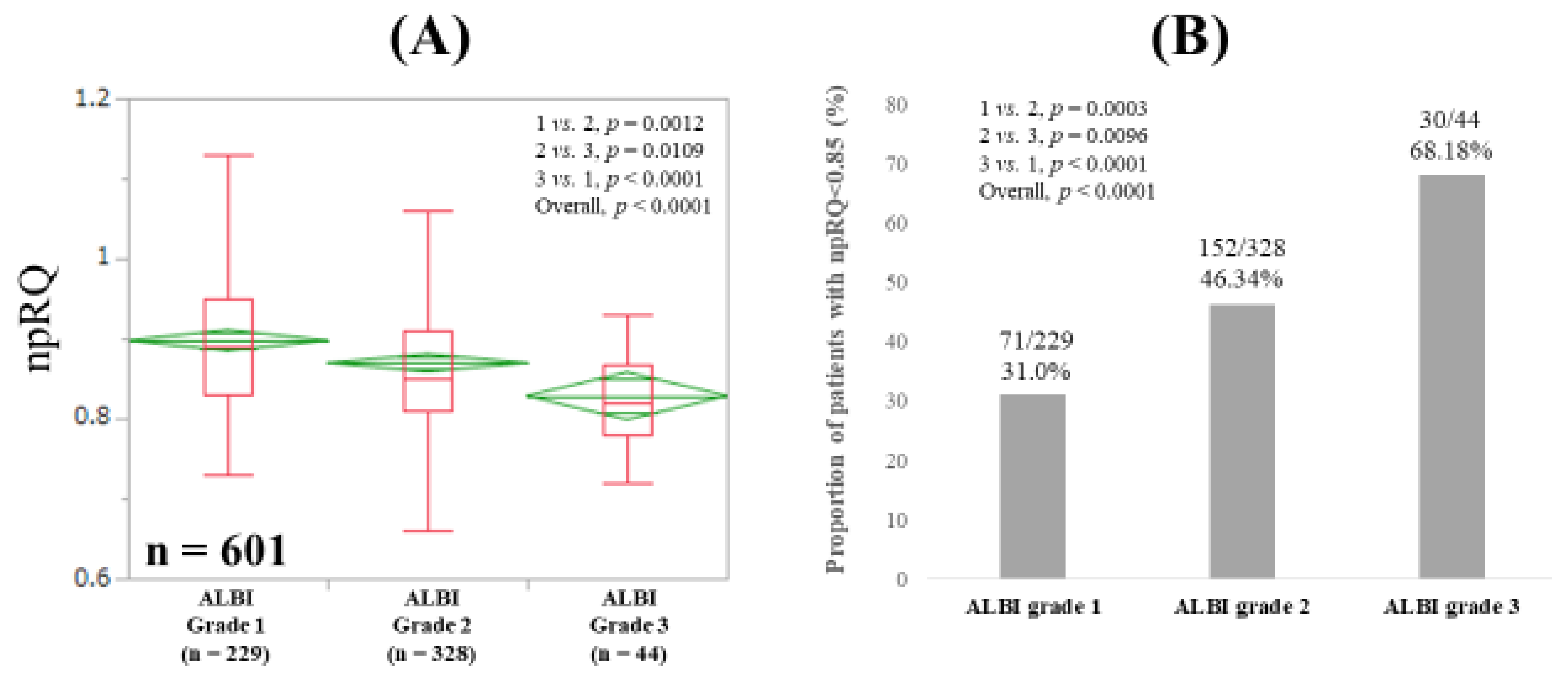
3.2. npRQ Level Among ALBI Grades 1, 2, and 3 for All Cases
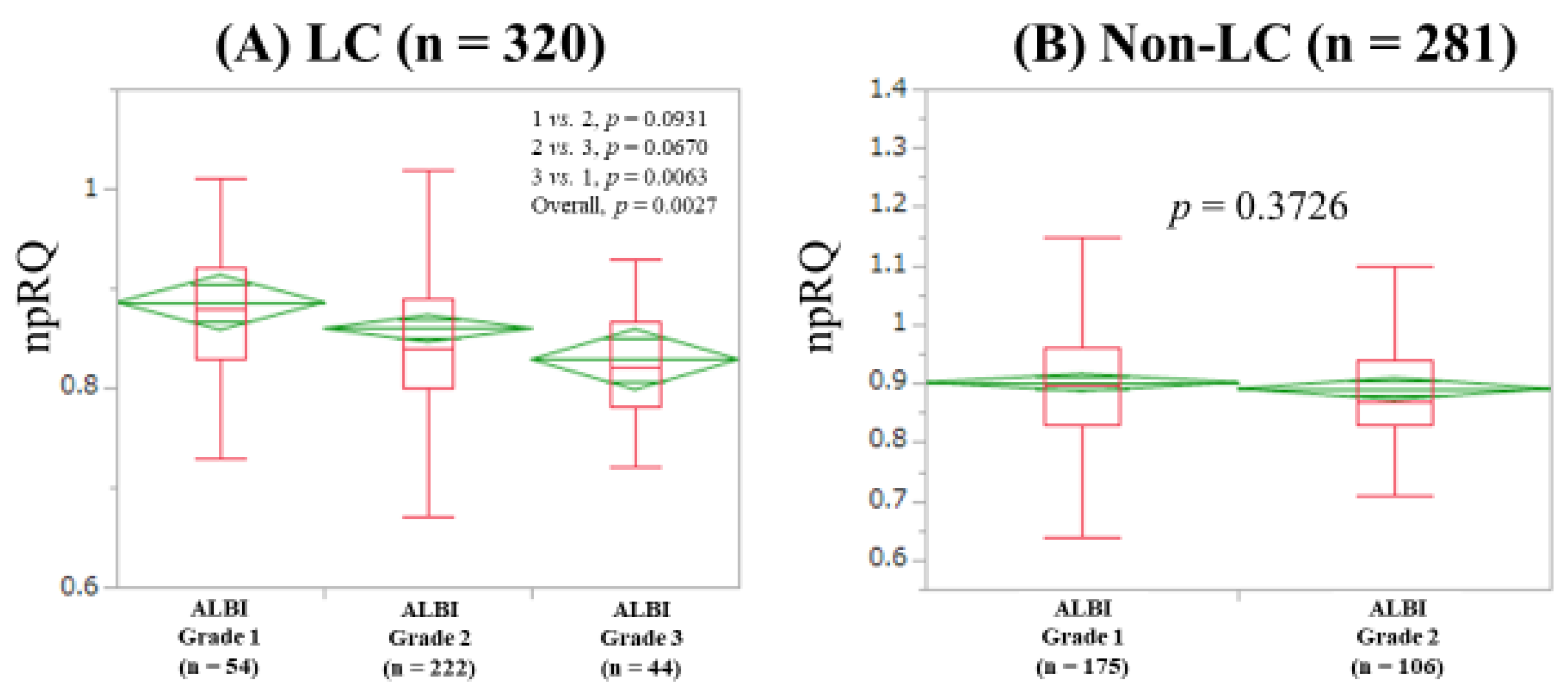
3.3. npRQ Level Among ALBI Grades 1, 2, and 3 According to the LC Status
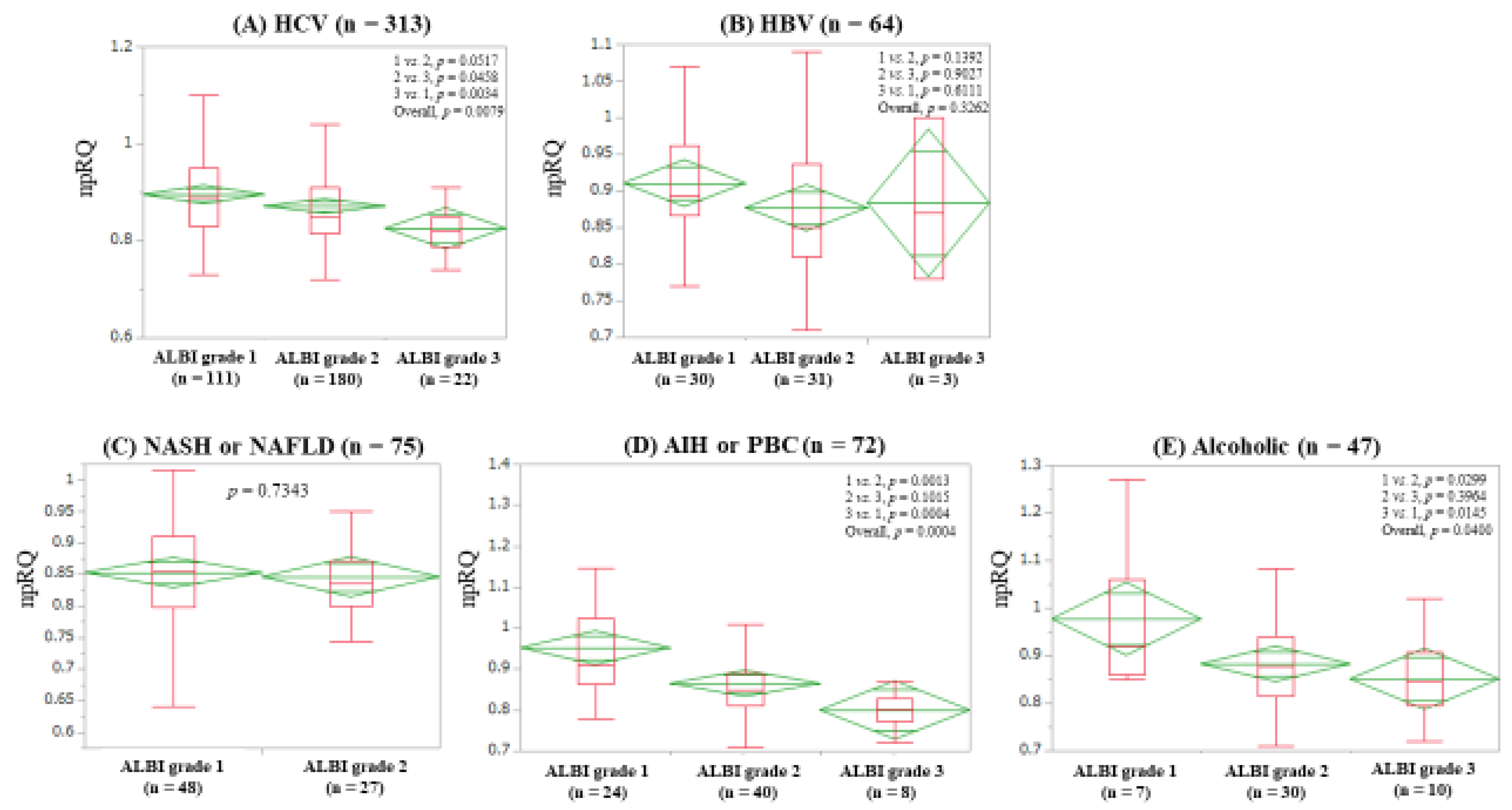
3.4. npRQ Level Among ALBI Grades 1, 2, and 3 According to Liver Disease Etiology
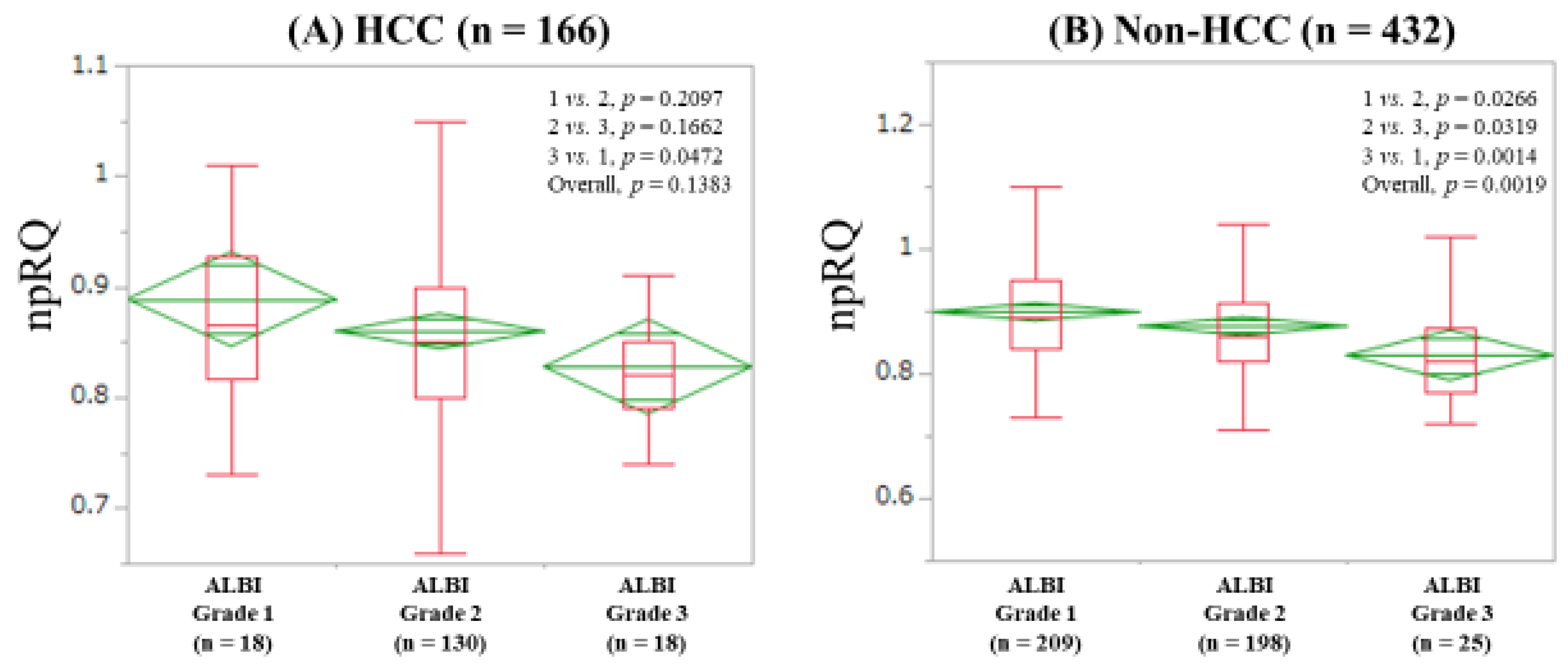
3.5. npRQ Level Among ALBI Grades 1, 2, and 3 According to the Presence of HCC
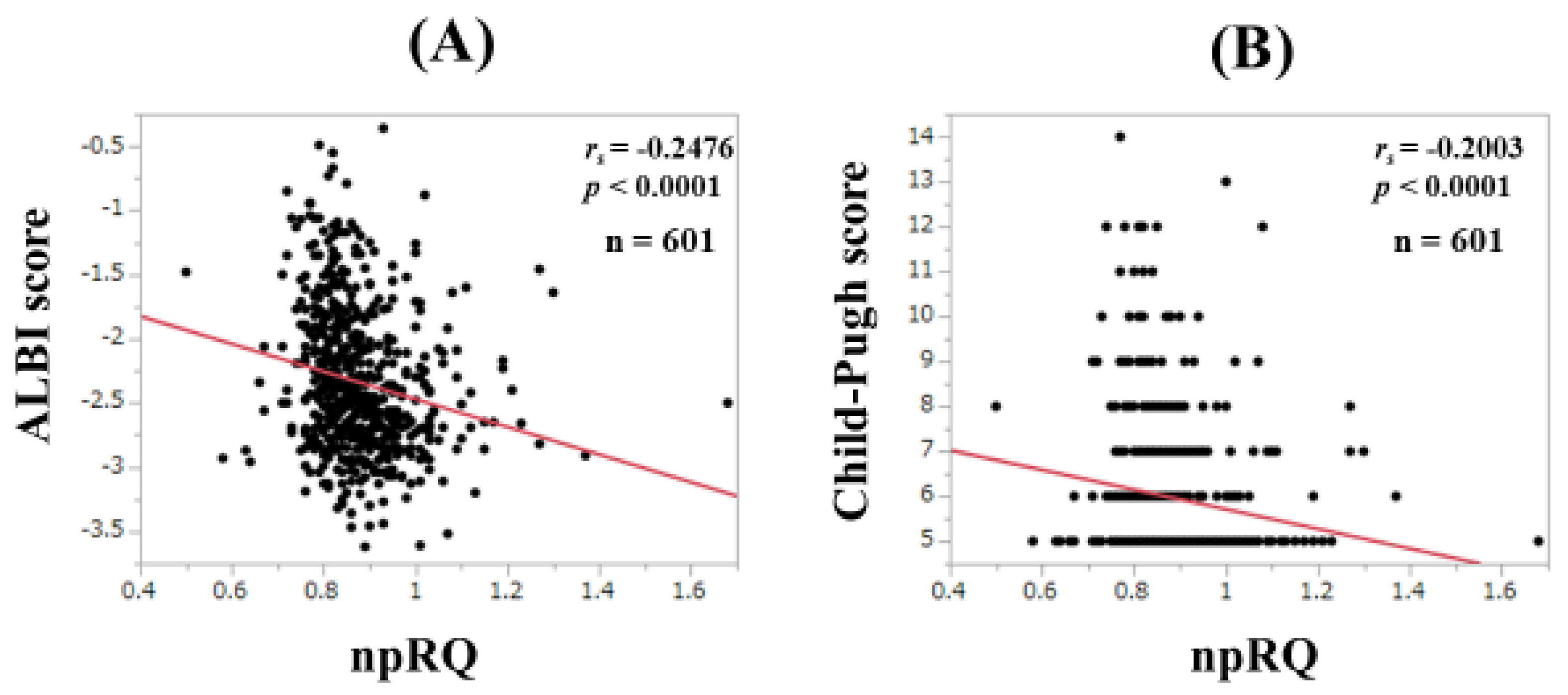
3.6. Correlation between npRQ and ALBI Score and Child-Pugh Score for All Cases
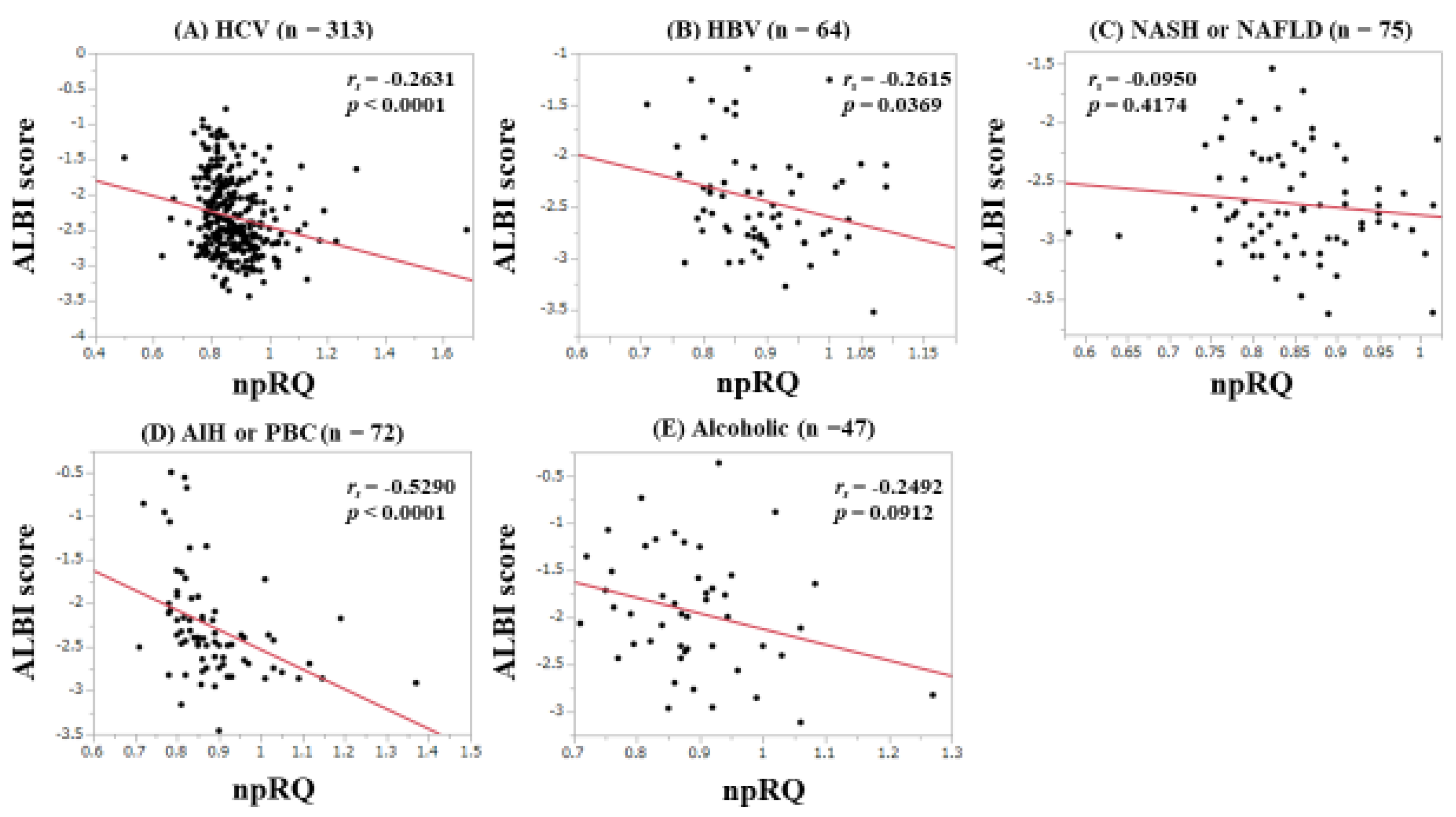
3.7. Correlation between npRQ and ALBI Score According to Liver Disease Etiology
3.8. Univariate and Multivariate Analyses of Factors Associated with npRQ < 0.85
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Moriwaki, H.; Miwa, Y.; Tajika, M.; Kato, M.; Fukushima, H.; Shiraki, M. Branched-chain amino acids as a protein- and energy-source in liver cirrhosis. Biochem. Biophys. Res. Commun. 2004, 313, 405–409. [Google Scholar] [CrossRef]
- Charlton, M.R. Branched-chain amino acid enriched supplements as therapy for liver disease. J. Nutr. 2006, 136, 295S–298S. [Google Scholar] [CrossRef]
- Nishikawa, H.; Osaki, Y. Clinical significance of therapy using branched-chain amino acid granules in patients with liver cirrhosis and hepatocellular carcinoma. Hepatol. Res. 2014, 44, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Osaki, Y. Liver Cirrhosis: Evaluation, Nutritional Status, and Prognosis. Mediat. Inflamm. 2015, 2015, 872152. [Google Scholar] [CrossRef] [PubMed]
- Tajika, M.; Kato, M.; Mohri, H.; Miwa, Y.; Kato, T.; Ohnishi, H.; Moriwaki, H. Prognostic value of energy metabolism in patients with viral liver cirrhosis. Nutrition 2002, 18, 229–234. [Google Scholar] [CrossRef]
- Sakai, Y.; Iwata, Y.; Enomoto, H.; Saito, M.; Yoh, K.; Ishii, A.; Takashima, T.; Aizawa, N.; Ikeda, N.; Tanaka, H.; et al. Two randomized controlled studies comparing the nutritional benefits of branched-chain amino acid (BCAA) granules and a BCAA-enriched nutrient mixture for patients with esophageal varices after endoscopic treatment. J. Gastroenterol. 2015, 50, 109–118. [Google Scholar] [CrossRef]
- Shiraki, M.; Nishiguchi, S.; Saito, M.; Fukuzawa, Y.; Mizuta, T.; Kaibori, M.; Hanai, T.; Nishimura, K.; Shimizu, M.; Tsurumi, H.; et al. Nutritional status and quality of life in current patients with liver cirrhosis as assessed in 2007–2011. Hepatol. Res. 2013, 43, 106–112. [Google Scholar] [CrossRef]
- Peng, S.; Plank, L.D.; McCall, J.L.; Gillanders, L.K.; McIlroy, K.; Gane, E.J. Body composition, muscle function, and energy expenditure in patients with liver cirrhosis: A comprehensive study. Am. J. Clin. Nutr. 2007, 85, 1257–1266. [Google Scholar] [CrossRef]
- Terakura, Y.; Shiraki, M.; Nishimura, K.; Iwasa, J.; Nagaki, M.; Moriwaki, H. Indirect calorimetry and anthropometry to estimate energy metabolism in patients with liver cirrhosis. J. Nutr. Sci. Vitaminol. 2010, 56, 372–379. [Google Scholar] [CrossRef]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Naiki, T.; Moriwaki, H. Free fatty acid as a marker of energy malnutrition in liver cirrhosis. Hepatol. Res. 2014, 44, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Zhong, J.H.; Su, Z.Y.; Huang, J.F.; Lu, S.D.; Xiang, B.D.; Ma, L.; Qi, L.N.; Ou, B.N.; Li, L.Q. Albumin-bilirubin versus Child-Pugh score as a predictor of outcome after liver resection for hepatocellular carcinoma. Br. J. Surg. 2016, 103, 725–734. [Google Scholar] [CrossRef]
- Toyoda, H.; Lai, P.B.; O’Beirne, J.; Chong, C.C.; Berhane, S.; Reeves, H.; Manas, D.; Fox, R.P.; Yeo, W.; Mo, F.; et al. Long-term impact of liver function on curative therapy for hepatocellular carcinoma: Application of the ALBI grade. Br. J. Cancer 2016, 114, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Toyoda, H.; Tada, T.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2016, 31, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Edeline, J.; Blanc, J.F.; Johnson, P.; Campillo-Gimenez, B.; Ross, P.; Ma, Y.T.; King, J.; Hubner, R.A.; Sumpter, K.; Darby, S.; et al. A multicentre comparison between Child Pugh and Albumin-Bilirubin scores in patients treated with sorafenib for Hepatocellular Carcinoma. Liver Int. 2016, 36, 1821–1828. [Google Scholar] [CrossRef] [Green Version]
- Fujita, K.; Oura, K.; Yoneyama, H.; Shi, T.; Takuma, K.; Nakahara, M.; Tadokoro, T.; Nomura, T.; Morishita, A.; Tsutsui, K.; et al. Albumin-bilirubin score indicates liver fibrosis staging and prognosis in chronic hepatitis C patients. Hepatol. Res. 2019. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, Z.; Yan, X.; Li, M.; Xia, J.; Liu, Y.; Chen, Y.; Jia, B.; Zhu, L.; Zhu, C.; et al. Albumin-Bilirubin (ALBI) as an accurate and simple prognostic score for chronic hepatitis B-related liver cirrhosis. Dig. Liver Dis. 2019. [Google Scholar] [CrossRef]
- Hsieh, Y.C.; Lee, K.C.; Wang, Y.W.; Yang, Y.Y.; Hou, M.C.; Huo, T.I.; Lin, H.C. Correlation and prognostic accuracy between noninvasive liver fibrosismarkers and portal pressure in cirrhosis: Role of ALBI score. PLoS ONE 2018, 13, e0208903. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Combined Albumin-Bilirubin Grade and Skeletal Muscle Mass as a Predictor in Liver Cirrhosis. J. Clin. Med. 2019, 8, 782. [Google Scholar] [CrossRef]
- Antkowiak, M.; Gabr, A.; Das, A.; Ali, R.; Kulik, L.; Ganger, D.; Moore, C.; Abecassis, M.; Katariya, N.; Mouli, S.; et al. Prognostic Role of Albumin, Bilirubin, and ALBI Scores: Analysis of 1000 Patients with Hepatocellular Carcinoma Undergoing Radioembolization. Cancers 2019, 11, 879. [Google Scholar] [CrossRef] [PubMed]
- Honmyo, N.; Kobayashi, T.; Hamaoka, M.; Kohashi, T.; Abe, T.; Oishi, K.; Tazawa, H.; Imaoka, Y.; Akita, T.; Tanaka, J.; et al. Hiroshima Surgical study group of Clinical Oncology (HiSCO). Comparison of new prognostic systems for patients with resectable hepatocellular carcinoma: Albumin-Bilirubin grade and Albumin-Indocyanine green Evaluation grade. Hepatol. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Iwata, Y.; Kishino, K.; Shimono, Y.; Hasegawa, K.; Nakano, C.; Takata, R.; Ishii, A.; Nishimura, T.; et al. Prognostic significance of nonprotein respiratory quotient in patients with liver cirrhosis. Medicine 2017, 96, e5800. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Hasegawa, K.; Nakano, C.; Takata, R.; Kishino, K.; Shimono, Y.; Sakai, Y.; et al. Serum hyaluronic acid predicts protein-energy malnutrition in chronic hepatitis C. Medicine 2016, 95, e3920. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, R.N.; Tidwell, A.C.; Minard, G.; Croce, M.A.; Brown, R.O. Predicting total urinary nitrogen excretion from urinary urea nitrogen excretion in multiple-trauma patients receiving specialized nutritional support. Nutrition 2005, 21, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- McManus, M.L.; Churchwell, K.B.; Strange, K. Regulation of cell volume in health and disease. N. Engl. J. Med. 1995, 333, 1260–1266. [Google Scholar] [CrossRef]
- Saito, M.; Yano, Y.; Minami, A.; Hirano, H.; Momose, K.; Sugimoto, M.; Yoshida, M.; Azuma, T. Branched-chain amino acid granules improve the non-protein respiratory quotient after radiofrequency ablation. Intern. Med. 2014, 53, 1469–1475. [Google Scholar] [CrossRef]
- Rohm, M.; Zeigerer, A.; Machado, J.; Herzig, S. Energy metabolism in cachexia. EMBO Rep. 2019, 20, e47258. [Google Scholar] [CrossRef]
- Ren, M.; Li, J.; Xue, R.; Wang, Z.; Coll, S.L.; Meng, Q. Liver function and energy metabolism in hepatocellular carcinoma developed in patients with hepatitis B-related cirrhosis. Medicine 2019, 98, e15528. [Google Scholar] [CrossRef]
- Saito, M.; Seo, Y.; Yano, Y.; Miki, A.; Yoshida, M.; Azuma, T. Short-term reductions in non-protein respiratory quotient and prealbumin can be associated with the long-term deterioration of liver function after transcatheter arterial chemoembolization in patients with hepatocellular carcinoma. J. Gastroenterol. 2012, 47, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Wu, L.C.; Hsia, C.Y.; Yin, P.H.; Chi, C.W.; Yeh, T.S.; Lee, H.C. Energy metabolism determines the sensitivity of human hepatocellular carcinoma cells to mitochondrial inhibitors and biguanide drugs. Oncol. Rep. 2015, 34, 1620–1628. [Google Scholar] [CrossRef] [PubMed]
- Beyoğlu, D.; Imbeaud, S.; Maurhofer, O.; Bioulac-Sage, P.; Zucman-Rossi, J.; Dufour, J.F.; Idle, J.R. Tissue metabolomics of hepatocellular carcinoma: Tumor energy metabolism and the role of transcriptomic classification. Hepatology 2013, 58, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.G.; Santos, L.F.; Anastácio, L.R.; Lima, A.S.; Correia, M.I. Resting energy expenditure, body composition, and dietary intake: A longitudinal study before and after liver transplantation. Transplantation 2013, 96, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Yoh, K.; Enomoto, H.; Ishii, N.; Iwata, Y.; Nakano, C.; Takata, R.; Nishimura, T.; Aizawa, N.; Sakai, Y.; et al. Extracellular Water to Total Body Water Ratio in Viral Liver Diseases: A Study Using Bioimpedance Analysis. Nutrients 2018, 10, 1072. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number or Median (Interquartile Range (IQR)) |
|---|---|
| Age (years) | 63 (54, 71) |
| Gender, male/female | 301/300 |
| Body mass index (kg/m2) | 22.2 (20.2, 24.9) |
| Presence of LC, yes/no | 320/281 |
| Child-Pugh classification, A/B/C | 447/131/23 |
| Presence of HCC, yes/no/unknown | 166/432/3 |
| Skeletal muscle mass index (kg/m2), male | 7.3 (6.8, 8.0) |
| Skeletal muscle mass index (kg/m2), female | 5.8 (5.3, 6.3) |
| ECW to TBW ratio | 0.385 (0.376, 0.393) |
| Causes of liver disease | 64/313/47/75/72/30 |
| Hepatitis B/Hepatitis C/alcohol/NAFLD or NASH/AIH or PBC/others | |
| Liver histology | |
| F0/F1/F2/F3/F4 | 12/117/77/75/320 |
| ALBI grade, 1/2/3 | 229/328/44 |
| npRQ | 0.86 (0.81, 0.925) |
| Total bilirubin (mg/dL) | 0.9 (0.7, 1.3) |
| Serum albumin (g/dL) | 3.8 (3.3, 4.1) |
| Prothrombin time (%) | 86.0 (71.9, 95.5) |
| Platelets (×104/mm3) | 12.4 (7.8, 19.0) |
| Total cholesterol (mg/dL) | 160 (134.75, 188) |
| AST (IU/L) | 40 (28.5, 62) |
| ALT (IU/L) | 35 (23, 61.5) |
| HbA1c (NGSP) | 5.2 (4.9, 5.7) |
| Branched-chain amino acid to tyrosine ratio | 5.04 (3.725, 6.335) |
| Ascites, yes/no/unknown | 54/544/3 |
| Variables | npRQ ≥ 0.85 (n = 348) | npRQ < 0.85 (n = 253) | p Value |
|---|---|---|---|
| Age (years) | 62 (51,70) | 66 (56,73) | 0.0042 |
| Gender, male/female | 178/170 | 123/130 | 0.5635 |
| HBV/HCV/alcohol/NAFLD or NASH/AIH or PBC/others | 43/177/32/37/43/16 | 21/136/15/38/29/14 | 0.2124 |
| Body mass index (kg/m2) | 21.9 (20.1, 24.4) | 22.8 (20.2, 25.6) | 0.0259 |
| Presence of LC, yes/no | 154/194 | 166/87 | <0.0001 |
| Presence of HCC, yes/no | 81/266 | 85/166 | 0.0055 |
| ALBI grade, 1/2/3 | 158/176/14 | 71/152/30 | <0.0001 |
| Prothrombin time (%) | 89.6 (76.1, 98.1) | 78.9 (67.6, 91.0) | <0.0001 |
| Platelet count (×104/mm3) | 14.2 (8.7, 19.8) | 9.8 (7.2, 17.2) | 0.0003 |
| AST (IU/L) | 36 (27,57) | 44 (30, 65) | 0.0506 |
| ALT (IU/L) | 35 (23, 62.75) | 35 (24, 60) | 0.9233 |
| Total cholesterol (mg/dL) | 166 (136, 193.25) | 153 (129.25, 180) | 0.0044 |
| HbA1c (NGSP) | 5.2 (5.0, 5.6) | 5.2 (4.7, 5.7) | 0.1438 |
| BTR | 5.34 (4.08, 6.42) | 4.605 (3.28, 6.0325) | 0.0009 |
| ECW to TBW ratio | 0.384 (0.375, 0.392) | 0.386 (0.377, 0.394) | 0.0643 |
| SMI (kg/m2), male | 7.3 (6.8, 7.85) | 7.35 (6.9, 8.0) | 0.3515 |
| SMI (kg/m2), female | 5.7 (5.3, 6.3) | 5.9 (5.2, 6.4) | 0.1723 |
| Multivariate Analysis | |||
|---|---|---|---|
| Hazard Ratio | 95% CI | p Value | |
| Age | 1.593 | 0.488–5.201 | 0.4407 |
| Platelet count | 0.729 | 0.0963–5.515 | 0.7593 |
| Body mass index | 0.309 | 0.0808–1.181 | 0.0861 |
| Total cholesterol | 0.636 | 0.185–2.185 | 0.4721 |
| BTR | 0.159 | 0.0159–1.578 | 0.1162 |
| Prothrombin time | 0.118 | 0.0215–0.647 | 0.0139 |
| Presence of HCC | 1.016 | 0.649–1.593 | 0.9428 |
| Presence of LC | 1.646 | 0.987–2.743 | 0.0560 |
| ALBI | |||
| ALBI grade 1 | 1.000 | Reference | |
| ALBI grade 2 | 1.465 | 0.930–2.309 | 0.1000 |
| ALBI grade 3 | 3.242 | 1.333–7.886 | 0.0095 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takata, R.; Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; et al. Association between Albumin-Bilirubin Grade and Non-Protein Respiratory Quotient in Patients with Chronic Liver Diseases. J. Clin. Med. 2019, 8, 1485. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091485
Takata R, Nishikawa H, Enomoto H, Yoh K, Iwata Y, Sakai Y, Kishino K, Ikeda N, Takashima T, Aizawa N, et al. Association between Albumin-Bilirubin Grade and Non-Protein Respiratory Quotient in Patients with Chronic Liver Diseases. Journal of Clinical Medicine. 2019; 8(9):1485. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091485
Chicago/Turabian StyleTakata, Ryo, Hiroki Nishikawa, Hirayuki Enomoto, Kazunori Yoh, Yoshinori Iwata, Yoshiyuki Sakai, Kyohei Kishino, Naoto Ikeda, Tomoyuki Takashima, Nobuhiro Aizawa, and et al. 2019. "Association between Albumin-Bilirubin Grade and Non-Protein Respiratory Quotient in Patients with Chronic Liver Diseases" Journal of Clinical Medicine 8, no. 9: 1485. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091485