The Increase of Osteoporotic Hip Fractures and Associated One-Year Mortality in Poland: 2008–2015


Abstract
:1. Introduction
2. Materials and Methods
3. Results
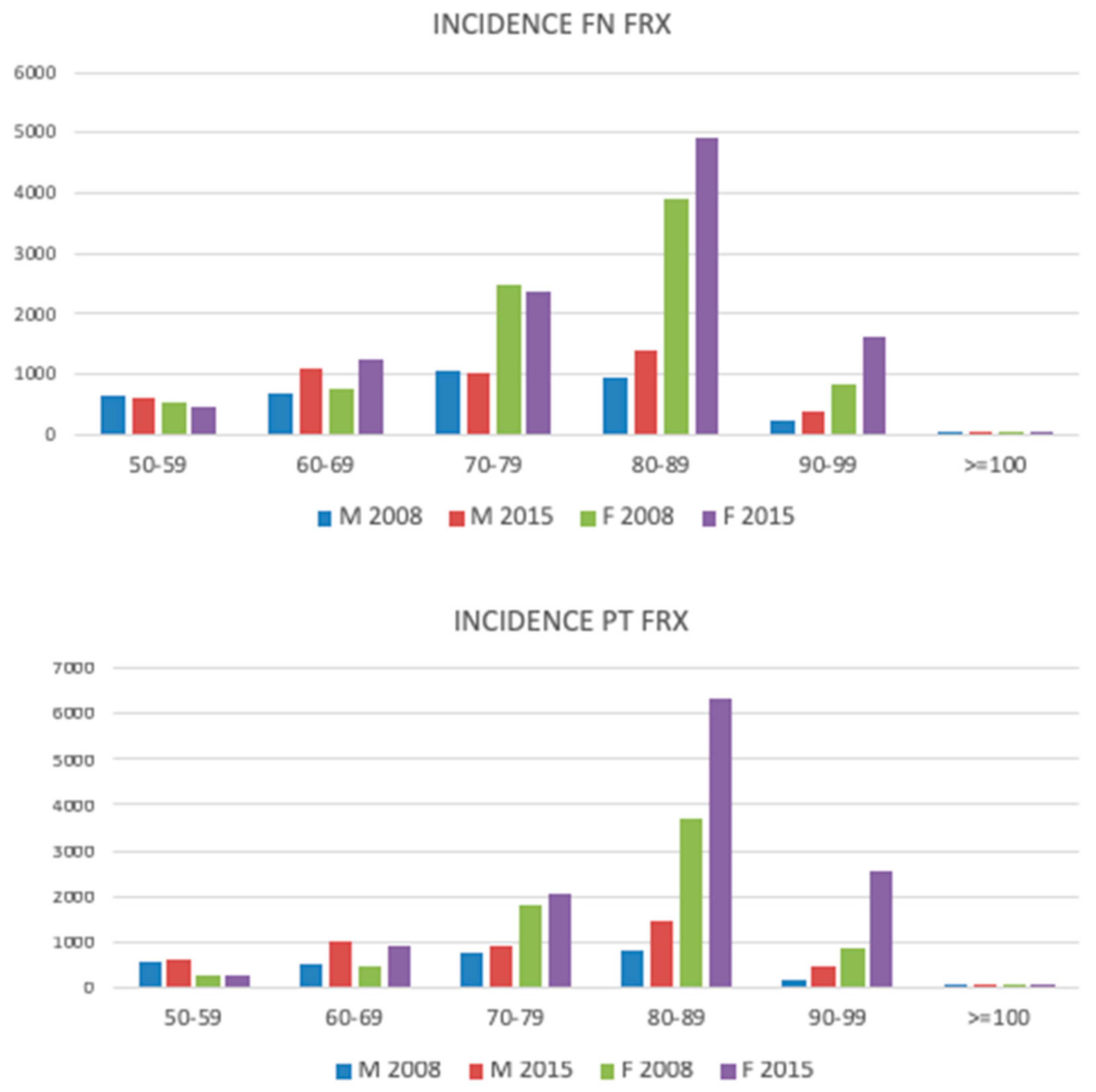
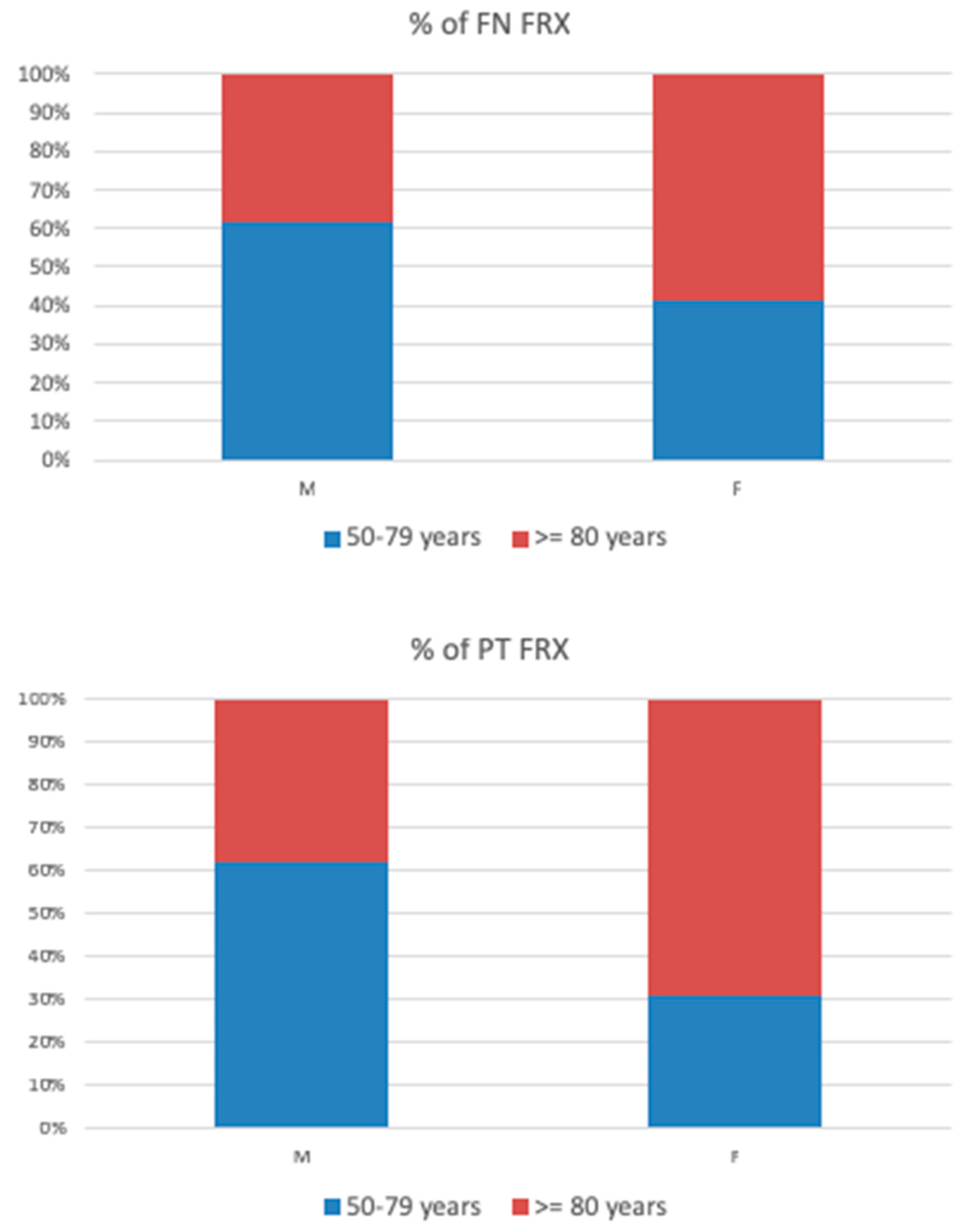
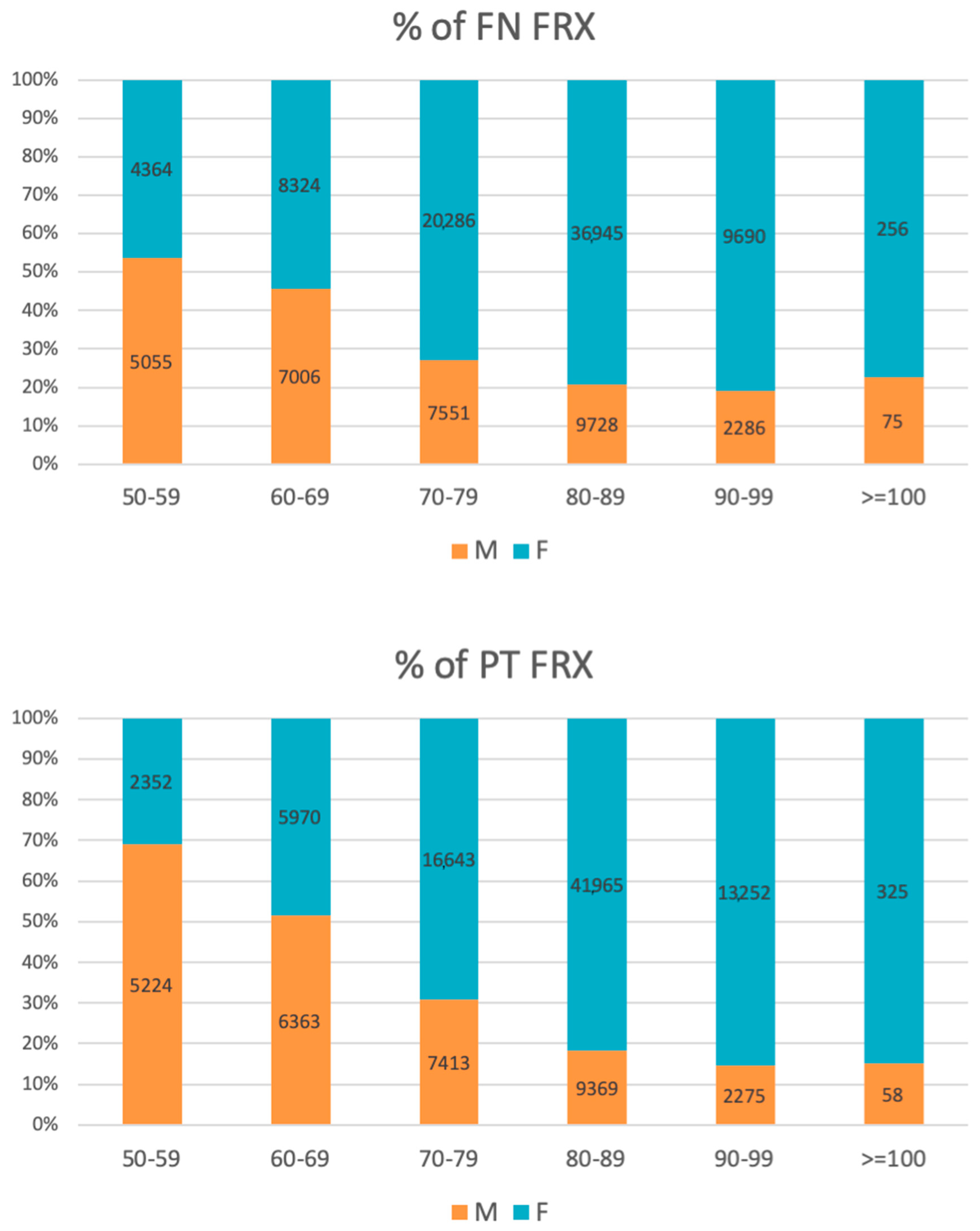
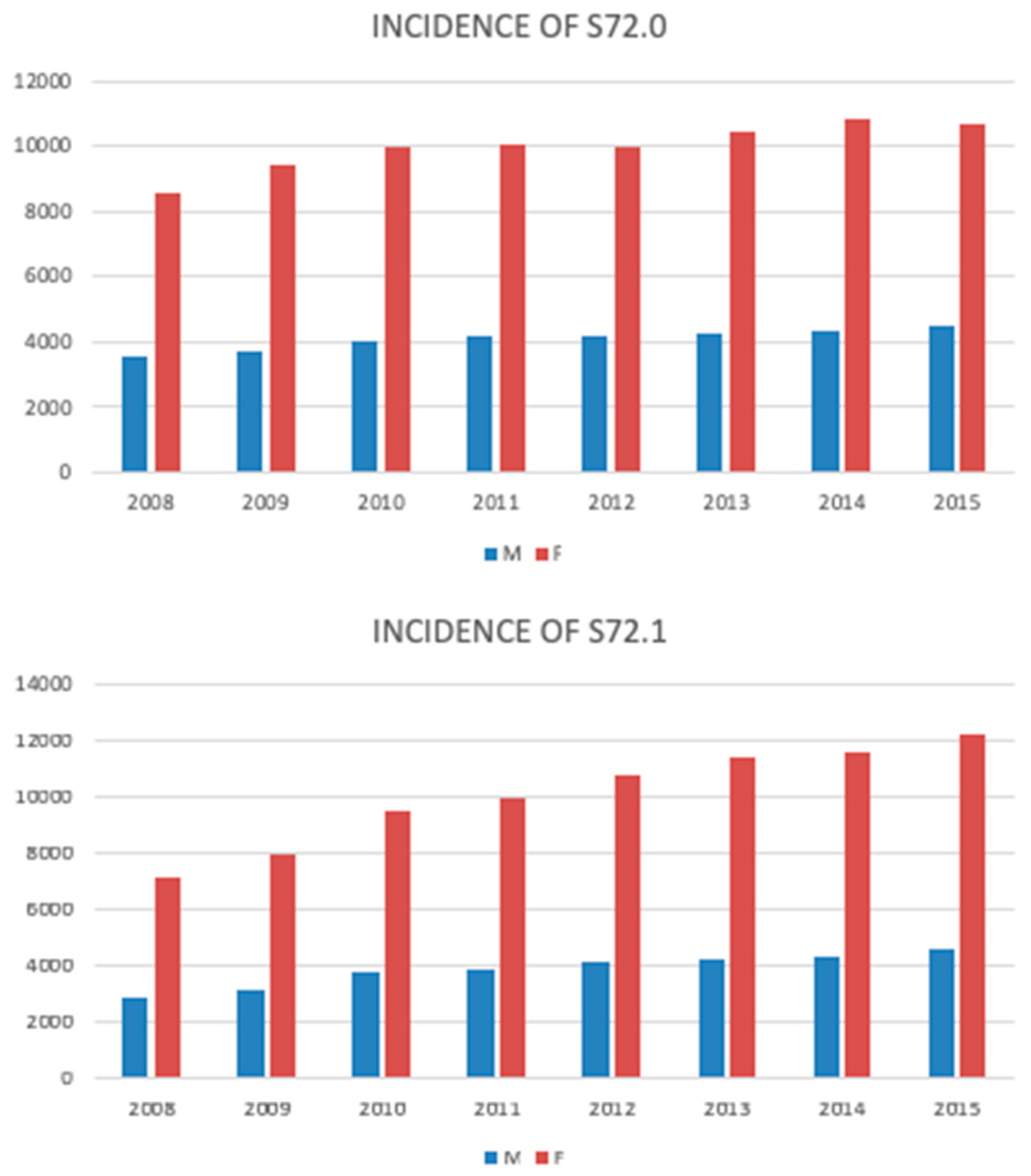
3.1. The Incidence of HFs
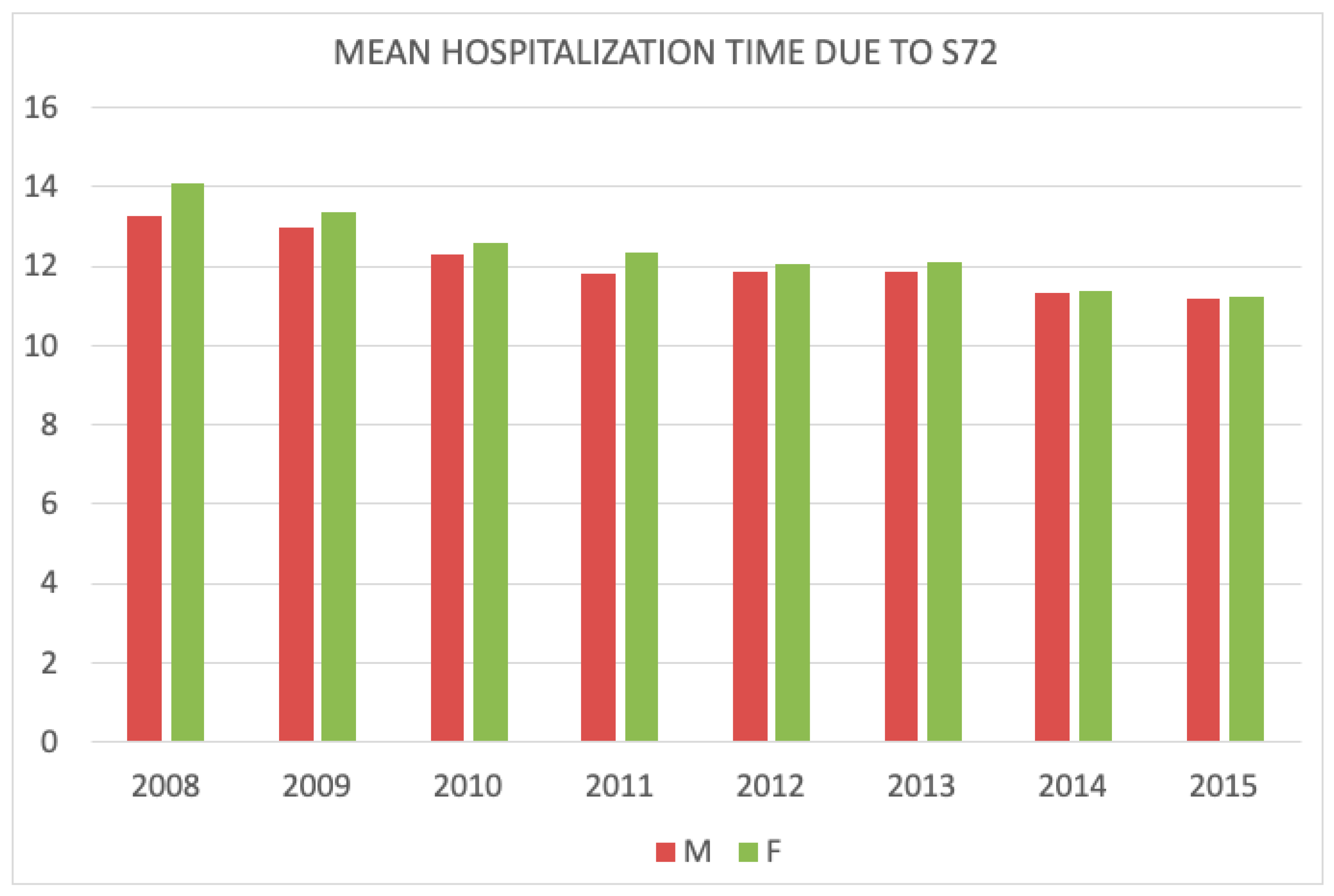
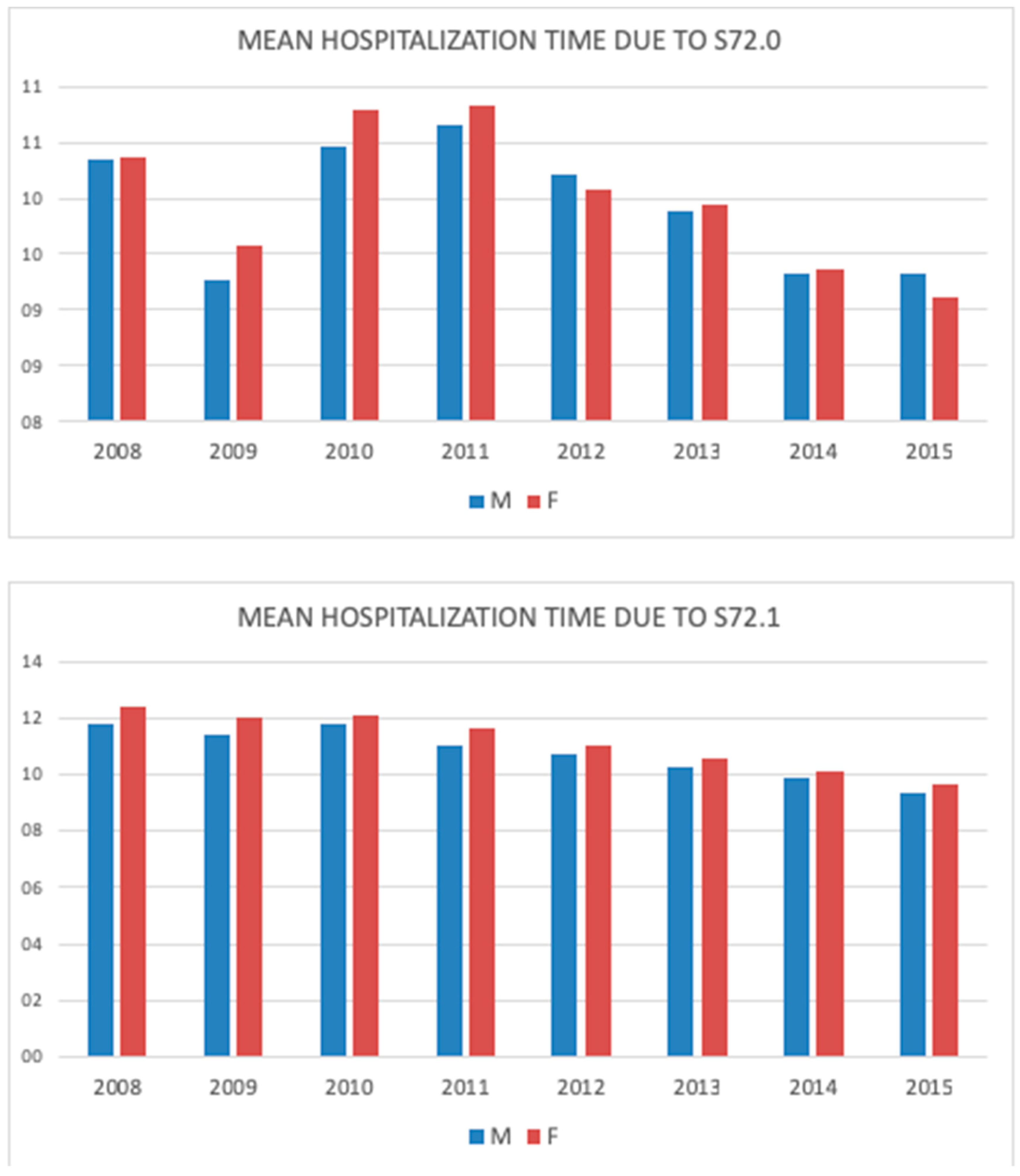
3.2. Hospitalization due to HFs
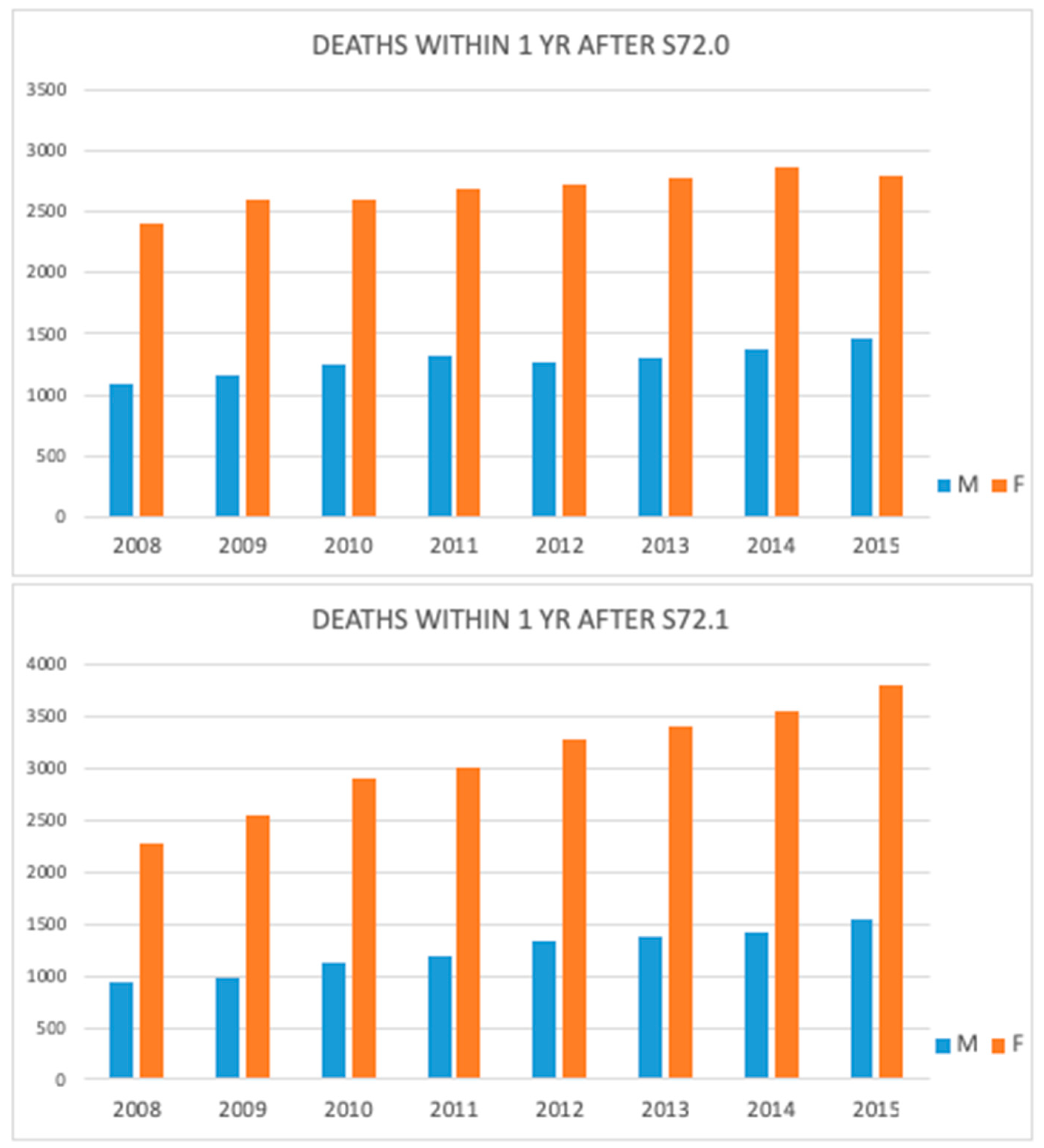
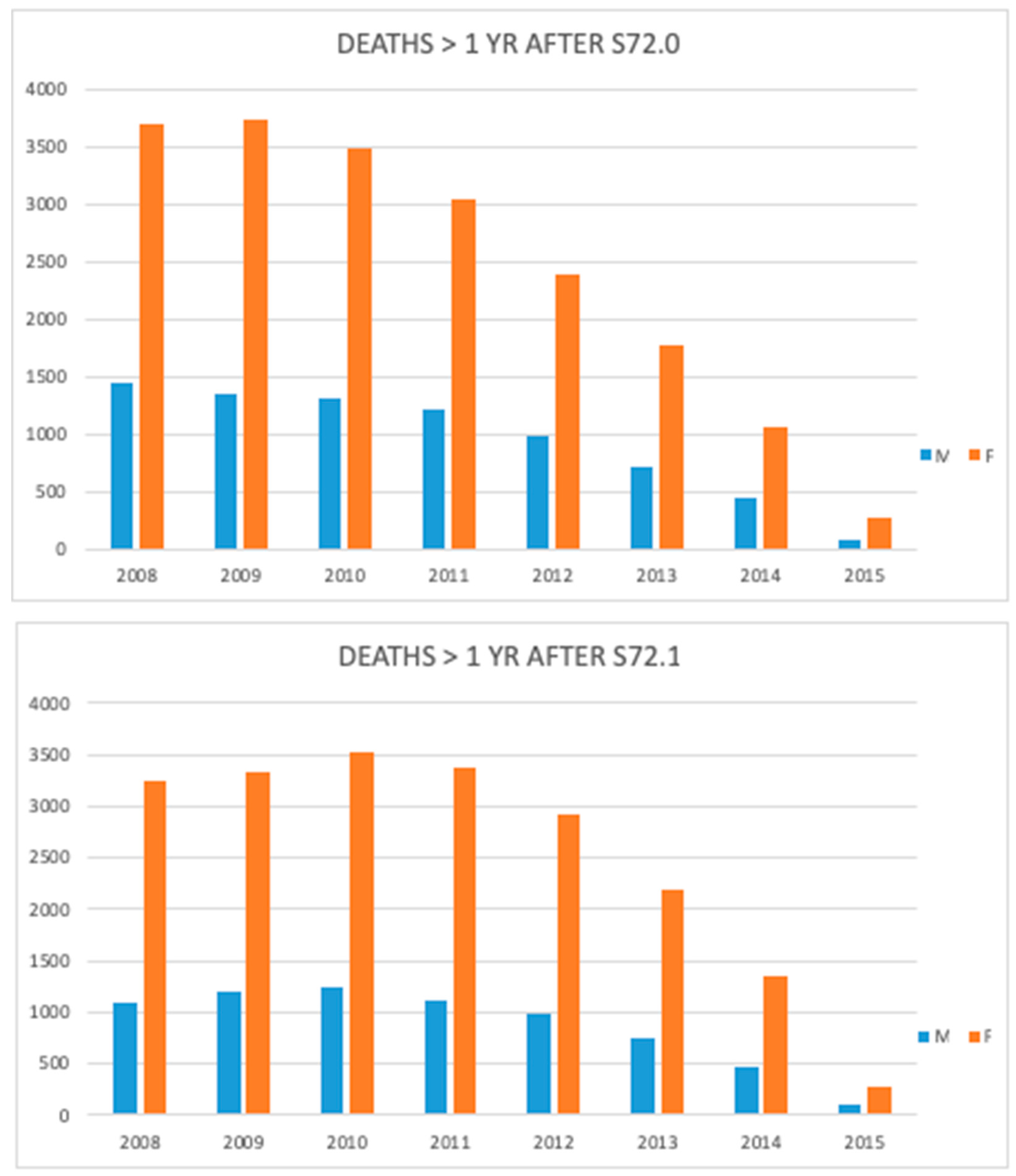
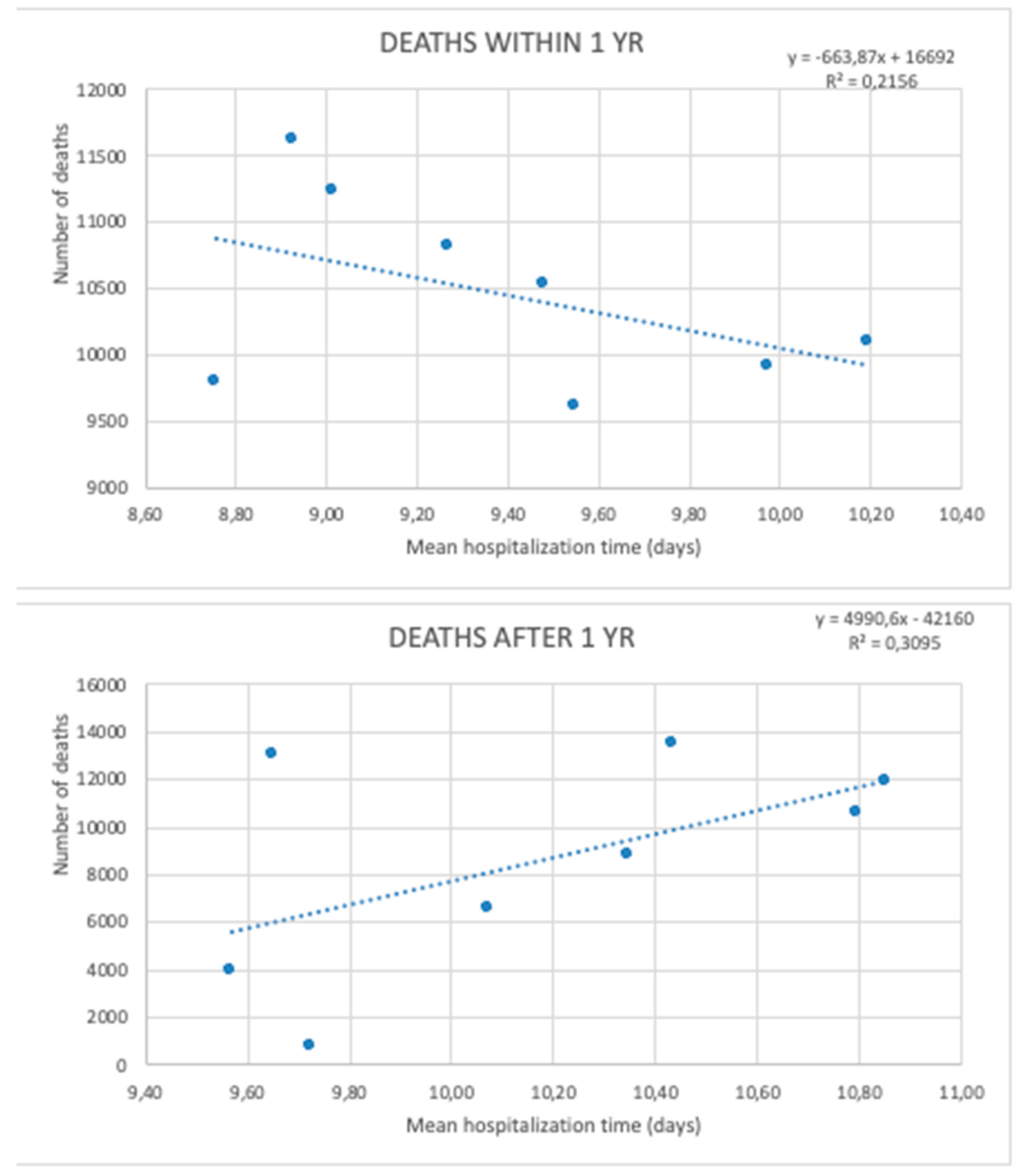
3.3. Mortality
4. Discussion
4.1. Incidence
4.2. Hospitalization
4.3. Mortality
Author Contributions
Funding
Conflicts of Interest
References
- Papadimitriou, N.; Tsilidis, K.K.; Orfanos, P.; Benetou, V.; E Ntzani, E.; Soerjomataram, I.; Künn-Nelen, A.; Pettersson-Kymmer, U.; Eriksson, S.; Brenner, H.; et al. Burden of hip fracture using disability-adjusted life-years: A pooled analysis of prospective cohorts in the CHANCES consortium. Lancet Public Health 2017, 2, e239–e246. [Google Scholar] [CrossRef]
- Klop, C.; Welsing, P.M.; Cooper, C.; Harvey, N.C.; Elders, P.J.; Bijlsma, J.W.; Leufkens, H.G.; De Vries, F. Mortality in British hip fracture patients, 2000–2010: A population-based retrospective cohort study. Bone 2014, 66, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Z.; Xiao, W. Risk factors for mortality in elderly patients with hip fractures: A meta-analysis of 18 studies. Aging Clin. Exp. Res. 2018, 30, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Wilk, R.; Skrzypek, M.; Kowalska, M.; Kusz, D.; Koczy, B.; Zagorski, P.; Pluskiewicz, W. The 13-year observation of hip fracture in Poland-worrying trend and prognosis for the future. Aging Clin. Exp. Res. 2018, 30, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Czerwinski, E.; Kanis, J.A.; Trybulec, B.; Johansson, H.; Borowy, P.; Osieleniec, J. The incidence and risk of hip fracture in Poland. Osteoporos. Int. 2009, 20, 1363–1367. [Google Scholar] [CrossRef]
- Kanis, J.A.; Oden, A.; McCloskey, E.V.; Johansson, H.; Wahl, D.A.; Cooper, C.A. systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos. Int. 2012, 23, 2239–2256. [Google Scholar] [CrossRef]
- Yoon, B.-H.; Lee, Y.-K.; Kim, S.-C.; Kim, S.-H.; Ha, Y.-C.; Koo, K.-H. Epidemiology of proximal femoral fractures in South Korea. Arch. Osteoporos. 2013, 8, 157. [Google Scholar] [CrossRef]
- Cordey, J.; Schneider, M.; Bühler, M. The epidemiology of fractures of the proximal femur. Injury 2000, 31, 56–93. [Google Scholar] [CrossRef]
- Sadat-Ali, M.; Al-Dakheel, D.A.; Azam, M.Q.; Al-Bluwi, M.T.; Al-Farhan, M.F.; AlAmer, H.A.; Al-Meer, Z.; Al-Mohimeed, A.; Tabash, I.K.; Karry, M.O.; et al. Reassessment of osteoporosis-related femoral fractures and economic burden in Saudi Arabia. Arch. Osteoporos 2015, 10, 37. [Google Scholar] [CrossRef]
- Xia, W.B.; He, S.L.; Xu, L.; Liu, A.M.; Jiang, Y.; Li, M.; Wang, O.; Xing, X.P.; Sun, Y.; Cummings, S.R. Rapidly increasing rates of hip fracture in Beijing, China. J. Bone Miner. Res. 2012, 27, 125–129. [Google Scholar] [CrossRef]
- Emaus, N.; Olsen, L.R.; Ahmed, L.A.; Balteskard, L.; Jacobsen, B.K.; Magnus, T.; Ytterstad, B. Hip fractures in a city in Northern Norway over 15 years: Time trends, seasonal variation and mortality: The Harstad Injury Prevention Study. Osteoporos. Int. 2011, 22, 2603–2610. [Google Scholar] [CrossRef] [PubMed]
- Statistics Poland. Basic Statistics. Available online: https://stat.gov.pl/download/gfx/portalinformacyjny/pl/defaultaktualnosci/5515/2/18/1/rocznik_statystyczny_rzeczypospolitej_polskiej_2018_.pdf (accessed on 31 December 2018).
- Wilk, R.; Skrzypek, M.; Kowalska, M.; Kusz, D.; Wielgórecki, A.; Horyniecki, M.; Śliwiak, J.; Piejczyk, S.; Pluskiewicz, W. Standardized incidence and trend of osteoporotic hip fracture in Polish women and men: A nine year observation. Maturitas 2014, 77, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Johnell, O.; De Laet, C.; Jonsson, B.; Odén, A.; Ogelsby, A.K. International Variations in Hip Fracture Probabilities: Implications for Risk Assessment. J. Bone Miner. Res. 2002, 17, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Johnel, O.; Gullberg, B.; Allander, E.; Kanis, J.A. The MEDOS Study Group The apparent incidence of hip fracture in Europe: A study of national register sources. Osteoporos. Int. 1992, 2, 298–302. [Google Scholar] [CrossRef]
- Roszkowska, H.; Goryński, P.; Wojtyniak, B. Hospitalization due to hip fracture in Poland in 1979–1995 by sex, age and place of residence. [pol.]. Postępy Osteoartrologii 1998, 10, 150–156. [Google Scholar]
- Jaworski, M.; Lorenc, R.S. Risk of hip fracture in Poland. Med. Sci. Monit. 2007, 13, CR206–CR210. [Google Scholar] [PubMed]
- Elffors, I.; Allander, E.; Kanis, J.A.; Gullberg, B.; Johnell, O.; Dequeker, J.; Dilsen, G.; Gennari, C.; Vaz, A.A.L.; Lyritis, G.; et al. The variable incidence of hip fracture in Southern Europe: The MEDOS study. Osteoporos. Int. 1994, 4, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Van Staa, T.; Dennison, E.; Leufkens, H.; Cooper, C.; Van Staa, T. Epidemiology of fractures in England and Wales. Bone 2001, 29, 517–522. [Google Scholar] [CrossRef] [Green Version]
- Ratti, C.; Vulcano, E.; La Barbera, G.; Canton, G.; Murena, L.; Cherubino, P. The incidence of fragility fractures in Italy. Aging Clin. Exp. Res. 2013, 25, 13–14. [Google Scholar] [CrossRef] [PubMed]
- Rapp, K.; Buchele, G.; Dreinhofer, K.; Bucking, B.; Becker, C.; Benzinger, P. Epidemiology of hip fractures: Systematic literature review of German data and an overview of the international literature. Z. Gerontol. Geriatr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Mann, E.; Meyer, G.; Haastert, B.; Icks, A. Comparison of hip fracture incidence and trends between Germany and Austria 1995–2004: An epidemiological study. BMC Public Health 2010, 10, 46. [Google Scholar] [CrossRef]
- Sund, R.; Riihimäki, J.; Mäkelä, M.; Vehtari, A.; Lüthje, P.; Huusko, T.; Häkkinen, U. Modeling the length of the care episode after hip fracture: Does the type of fracture matter? Scand. J. Surg. 2009, 98, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Medin, E.; Goude, F.; Melberg, H.O.; Tediosi, F.; Belicza, É.; Peltola, M. on behalf of the EuroHOPE study group European Regional Differences in All-Cause Mortality and Length of Stay for Patients with Hip Fracture. Health Econ. 2015, 24, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Fenton, J.J.; Jerant, A.F.; Bertakis, K.D.; Franks, P. The cost of satisfaction: A national study of patient satisfaction, health care utilization, expenditures, and mortality. Arch. Intern. Med. 2012, 172, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Currie, C. Hip fracture audit: Creating a ‘critical mass of expertise and enthusiasm for hip fracture care’? Injury 2018, 49, 1418–1423. [Google Scholar] [CrossRef]
- Johansen, A.; Golding, D.; Brent, L.; Close, J.; Gjertsen, J.-E.; Holt, G.; Hommel, A.; Pedersen, A.B.; Röck, N.D.; Thorngren, K.-G. Using national hip fracture registries and audit databases to develop an international perspective. Injury 2017, 48, 2174–2179. [Google Scholar] [CrossRef] [PubMed]
- Cundall-Curry, D.J.; Lawrence, J.E.; Fountain, D.M.; Gooding, C.R. Data errors in the National Hip Fracture Database: A local validation study. Bone Joint J. 2016, 98, 1406–1409. [Google Scholar] [CrossRef]
- Voeten, S.; Krijnen, P.; Voeten, D.; Hegeman, J.; Wouters, M.; Schipper, I. Quality indicators for hip fracture care, a systematic review. Osteoporos. Int. 2018, 29, 1963–1985. [Google Scholar] [CrossRef] [Green Version]
- Voeten, S.C.; Arends, A.J.; Wouters, M.W.J.M.; Blom, B.J.; Heetveld, M.J.; Slee-Valentijn, M.S.; Krijnen, P.; Schipper, I.B.; Hegeman, J.H.; Arends, A.J. The Dutch Hip Fracture Audit: Evaluation of the quality of multidisciplinary hip fracture care in the Netherlands. Arch. Osteoporos. 2019, 14, 28. [Google Scholar] [CrossRef]
- Macdonald, V.; Maher, A.B.; Mainz, H.; Meehan, A.J.; Brent, L.; Hommel, A.; Hertz, K.; Taylor, A.; Sheehan, K.J. Developing and Testing an International Audit of Nursing Quality Indicators for Older Adults With Fragility Hip Fracture. Orthop. Nurs. 2018, 37, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Mattisson, L.; Bojan, A.; Enocson, A. Epidemiology, treatment and mortality of trochanteric and subtrochanteric hip fractures: Data from the Swedish fracture register. BMC Musculoskelet. Disord. 2018, 19, 369. [Google Scholar] [CrossRef] [PubMed]
- Iacovino, J.R. Mortality outcomes after osteoporotic fractures in men and women. J. Insur. Med. 2001, 33, 316–320. [Google Scholar] [PubMed]
- Ftouh, S.; Morga, A.; Swift, C. Management of hip fracture in adults: Summary of NICE guidance. BMJ 2011, 342, d3304. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Gustafson, Y.; Michaëlsson, K.; Nordström, A. Length of hospital stay after hip fracture and short term risk of death after discharge: A total cohort study in Sweden. BMJ 2015, 350, h696. [Google Scholar] [CrossRef] [PubMed]
- Nikkel, L.E.; Kates, S.L.; Schreck, M.; Maceroli, M.; Mahmood, B.; Elfar, J.C. Length of hospital stay after hip fracture and risk of early mortality after discharge in New York state: Retrospective cohort study. BMJ 2015, 351, h6246. [Google Scholar] [CrossRef]
- Dubljanin-Raspopović, E.; Marković-Denić, L.; Marinkovic, J.; Nedeljković, U.; Bumbaširević, M. Does Early Functional Outcome Predict 1-year Mortality in Elderly Patients With Hip Fracture? Clin. Orthop. Relat. Res. 2013, 471, 2703–2710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyes, G.J.; Tucker, A.; Marley, D.; Foster, A. Predictors for Readmission up to 1 Year Following Hip Fracture. Arch. Trauma Res. 2015, 4. [Google Scholar] [CrossRef]
- Kanis, J.; Oden, A.; Johnell, O.; De Laet, C.; Jonsson, B.; Oglesby, A. The components of excess mortality after hip fracture. Bone 2003, 32, 468–473. [Google Scholar] [CrossRef]
- Karampampa, K.; Ahlbom, A.; Michaëlsson, K.; Andersson, T.; Drefahl, S.; Modig, K. Declining incidence trends for hip fractures have not been accompanied by improvements in lifetime risk or post-fracture survival—A nationwide study of the Swedish population 60years and older. Bone 2015, 78, 55–61. [Google Scholar] [CrossRef]
- Cooper, C.; Atkinson, E.J.; Jacobsen, S.J.; O’Fallon, W.M.; Melton, L.J., 3rd. Population-based study of survival after osteoporotic fractures. Am. J. Epidemiol. 1993, 137, 1001–1005. [Google Scholar] [CrossRef]
- Leibson, C.L.; Tosteson, A.N.A.; Gabriel, S.E.; Ransom, J.E.; Melton, L.J. Mortality, Disability, and Nursing Home Use for Persons with and without Hip Fracture: A Population-Based Study. J. Am. Geriatr. Soc. 2002, 50, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Keene, G.S.; Parker, M.J.; Pryor, G.A. Mortality and morbidity after hip fractures. BMJ 1993, 307, 1248–1250. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.; Pelpola, K.; Ball, M.; Ong, A.; Myint, P.K. Pre-operative indicators for mortality following hip fracture surgery: A systematic review and meta-analysis. Age Ageing 2014, 43, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Söderqvist, A.; Ekström, W.; Ponzer, S.; Pettersson, H.; Cederholm, T.; Dalén, N.; Hedström, M.; Tidermark, J. Prediction of Mortality in Elderly Patients with Hip Fractures: A Two-Year Prospective Study of 1944 Patients. Gerontology 2009, 55, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Pioli, G.; Barone, A.; Giusti, A.; Oliveri, M.; Pizzonia, M.; Razzano, M.; Palummeri, E. Predictors of mortality after hip fracture: Results from 1-year follow-up. Aging Clin. Exp. Res. 2006, 18, 381–387. [Google Scholar] [CrossRef]
- Magaziner, J.; Simonsick, E.M.; Kashner, T.M.; Hebel, J.R.; Kenzora, J.E. Predictors of Functional Recovery One Year Following Hospital Discharge for Hip Fracture: A Prospective Study. J. Gerontol. 1990, 45, 101–107. [Google Scholar] [CrossRef]
- Riggs, B.L.; Melton, L.J., 3rd. The worldwide problem of osteoporosis: Insights afforded by epidemiology. Bone 1995, 17, 505S–511S. [Google Scholar] [CrossRef]
- Haentjens, P.; Autier, P.; Barette, M.; Venken, K.; Vanderschueren, D.; Boonen, S. Survival and functional outcome according to hip fracture type: A one-year prospective cohort study in elderly women with an intertrochanteric or femoral neck fracture. Bone 2007, 41, 958–964. [Google Scholar] [CrossRef]
- Haentjens, P.; Autier, P.; Barette, M.; Boonen, S.; Autier, P. Predictors of functional outcome following intracapsular hip fracture in elderly women. Injury 2005, 36, 842–850. [Google Scholar] [CrossRef]
- Barette, M.; Vanderschueren, D.; Lips, P.; Haentjens, P.; Boonen, S.; Autier, P. Functional outcome and quality of life following hip fracture in elderly women: A prospective controlled study. Osteoporos. Int. 2004, 15, 87–94. [Google Scholar] [CrossRef]
- Wilk, R.; Skrzypek, M.; Kowalska, M.; Kusz, D.; Koczy, B.; Zagorski, P.; Pluskiewicz, W. Do we need orthogeriatrics in Poland? Changes in the age structure and location of hip fractures. Aging Clin. Exp. Res. 2017, 29, 737–743. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Total Incidence/100,000 | Incidence in Men/100,000 | Incidence in Women/100,000 | |
|---|---|---|---|---|
| Femoral Neck FRX | 2008 | 119 | 67 | 167 |
| 2009 | 146 | 75 | 212 | |
| 2010 | 113 | 62 | 161 | |
| 2011 | 124 | 68 | 176 | |
| 2012 | 147 | 78 | 211 | |
| 2013 | 205 | 108 | 295 | |
| 2014 | 220 | 117 | 317 | |
| 2015 | 207 | 125 | 283 | |
| Pertrochanteric FRX | 2008 | 73 | 42 | 102 |
| 2009 | 104 | 53 | 152 | |
| 2010 | 98 | 52 | 141 | |
| 2011 | 115 | 63 | 163 | |
| 2012 | 143 | 82 | 201 | |
| 2013 | 212 | 108 | 309 | |
| 2014 | 225 | 114 | 329 | |
| 2015 | 237 | 121 | 346 |
| Proximal Femur Fracture | Total Incidence/100,000 | Incidence in Men/100,000 | Incidence in Women/100,000 |
|---|---|---|---|
| 2008 | 56 | 32 | 78 |
| 2009 | 73 | 37 | 106 |
| 2010 | 61 | 33 | 88 |
| 2011 | 69 | 38 | 98 |
| 2012 | 84 | 46 | 119 |
| 2013 | 121 | 63 | 175 |
| 2014 | 129 | 67 | 187 |
| 2015 | 129 | 71 | 183 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glinkowski, W.; Narloch, J.; Krasuski, K.; Śliwczyński, A. The Increase of Osteoporotic Hip Fractures and Associated One-Year Mortality in Poland: 2008–2015. J. Clin. Med. 2019, 8, 1487. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091487
Glinkowski W, Narloch J, Krasuski K, Śliwczyński A. The Increase of Osteoporotic Hip Fractures and Associated One-Year Mortality in Poland: 2008–2015. Journal of Clinical Medicine. 2019; 8(9):1487. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091487
Chicago/Turabian StyleGlinkowski, Wojciech, Jerzy Narloch, Krzysztof Krasuski, and Andrzej Śliwczyński. 2019. "The Increase of Osteoporotic Hip Fractures and Associated One-Year Mortality in Poland: 2008–2015" Journal of Clinical Medicine 8, no. 9: 1487. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8091487