1. Introduction
Intrahepatic cholangiocarcinoma represents the second most common primary liver cancer after hepatocellular carcinoma. The reported incidence has increased worldwide over the past few decades [
1]. Mortality from ICC is increasing in the US and UK and has tripled in Germany from 1998 to 2008 [
2,
3]. The five-year survival is below 5%, even for those patients who undergo tumor resection. Surgical resection is the only potentially curative therapy option for patients with ICC. However, only 20% are eligible for resection. The reason for the low resectability rate is disease spread and anatomic location, inadequate hepatic reserve or comorbidities [
2]. The median survival for patients with untreated unresectable ICC has been reported to be as low as 3–6 months [
4]. Systemic chemotherapy has a low survival benefit for patients with unresectable ICC, as the majority of patients have a chemorefractory course. For systemic chemotherapies like gemcitabine or gemcitabine and cisplatin, the previously reported survival rate is between 8.1 and 11.7 months, respectively [
5]. A recent post-hoc analysis of three large clinical trials just recently revealed improved survival rates of 16.7 months after 3 or 6 months of chemotherapy [
6]. Thus, the therapeutic options for patients suffering from advanced ICC are associated with poor response rates and severe side effects at the same time. To date, there is no consensus on the optimal treatment regime of unresectable and chemorefractory ICC [
7]. The goals of palliative therapy are clearly defined; in detail, these are control of local tumor growth, to relieve tumor induced symptoms, and to improve the quality of life.
There are a number of different local-ablative treatment options for unresectable and chemorefractory ICC, i.e., radiofrequency ablation (RFA), intra-arterial chemotherapy, transarterial chemoembolization (TACE), and radioembolization (TARE). Since the first reports,
90Y radioembolization has been shown to be an effective method for both primary liver cancer, especially HCC, as well as secondary liver cancer, with the most existing evidence in metastatic colorectal cancer [
8,
9]. There is an increasing number of reports on the use of
90Y radioembolization for intrahepatic cholangiocarcinoma, but the evidence of resin-based
90Y microspheres in the treatment of unresectable and chemorefractory ICC is still limited [
3,
10,
11,
12,
13,
14]. First results suggest that the median overall survival treating ICC with
90Y radioembolization is 13.9 months (9.5–18.3 months), thus being at least as high compared to systemic chemotherapy, but potentially reduced side effects [
3]. Most reported results confer to therapy-naïve patients when TARE is a first line therapy. In clinical practice, however, this is frequently not the case, and patients have undergone multiple therapies before presenting for
90Y-TARE.
We therefore aimed to further evaluate the safety and outcome of 90Y radioembolization for treatment of advanced intrahepatic cholangiocarcinoma in a retrospective multicenter cohort.
5. Discussion
Tumors of the biliary tree are associated with a poor prognosis [
5,
7,
15]. While surgical techniques have expanded in recent years, allowing for curative approaches even for advanced Klatskin tumors applying procedures such as associating liver partition and portal vein ligation (ALPPS) and portal vein embolization (PVE) with subsequent extended liver resection, intrahepatic cholangiocarcinoma can rarely be resected in a curative manner [
16,
17]. Moreover, biliary tract cancer shows poor response rates to systemic chemotherapy, with overall survival previously reported for gemcitabine monotherapy of 8.1 months and gemcitabine plus cisplatin of 11.7 months [
5]; 13.8 months for intrahepatic cholangiocarcinoma [
18] and 16.2 months for hepatocholangiocarcinoma [
19]. A recent post-hoc analysis of three large clinical trials on advanced ICC showed survival rates of 16.7 months following 3 to 6 months of chemotherapy, which likely reflects improved patient selection and improvements in chemotherapy regimens [
6]. Overall survival for traditional local ablative therapies such as TACE is similarly poor, with an overall survival after of 10–15 months [
20]. For radiofrequency ablation, survival rates of 23.6 months have been reported, with the caveat that radiofrequency ablation is limited to tumors with a small to moderate size, 1.8 cm in the cohort reported by Takahashi et al. [
21].
Radioembolization has been proposed as a potential alternative for irresectable ICC, particularly because TARE especially in hypovascular liver tumors is considered more suitable than other transarterial embolization therapies, as the chemotherapeutic agents might not adequately reach the target in poorly perfused lesions [
3,
22]. Several studies have reported a potential benefit for TARE in ICC, but most confer to patients with limited disease or naïve to other anticancer treatments [
3,
12]; in some, TARE was able to even achieve a disease reduction allowing for subsequent surgical resection [
14]. A recent pooled analysis of
90Y TARE in unresectable ICC summarizing 12 cohort studies revealed a median survival of 14.3 months, similarly indicating that most TARE studies included patients with a limited disease extent [
23]. A small study of 23 patients investigated differences in response to TARE in therapy-naïve ICC patients compared to patients with previous therapy and showed that survival is substantially increased in therapy-naïve patients undergoing Y-90 TARE [
22].
Therefore, the primary aim of the presenting study was to investigate TARE in the treatment of more advanced stages of disease. Patients either refractory to previous anticancer therapy or, if therapy-naïve, with at least a tumor burden of 25% of the entire liver volume were included. In the presented patient cohort with an advanced disease stage, median survival was 9.5 months. At 3 months post TARE, 50% patients achieved local tumor control with partial remission or stable disease and 28% patients suffering from progressive disease. These results confirm the previous findings of Mosconi et al., who described survival rates of 16 months in 19 patients with advanced disease stage having undergone previous anticancer therapy, compared to 52 months in
n = 4 therapy-naïve ICC patients [
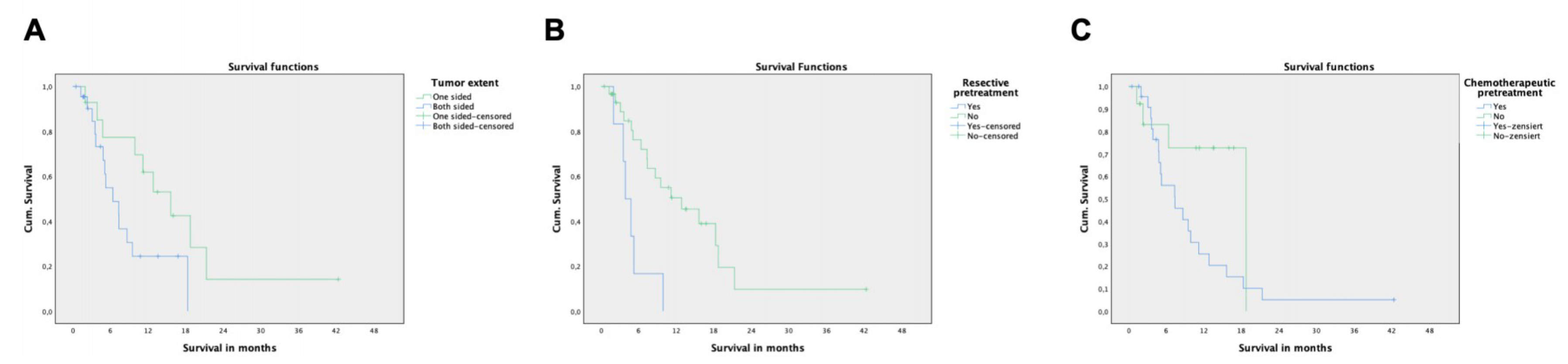
22]. In the analysis of prognostic factors for decreased survival, patients having undergone previous surgical resection for ICC had especially low survival rates of four months only after TARE. This does not necessarily mean that TARE is not indicated in those patients, but the limited benefit needs to be balanced carefully with associated risks. Additionally, previous surgical therapy can rather be seen as a surrogate marker for relapse or progressive disease, rather than a real prognostic factor for survival. Interestingly, a predictive model based on 405 patients with biliary tract cancer revealed improved survival of patients who had undergone surgical resection of the primary tumor [
24]. However, it has to be noted that this cohort included patients with various biliary tract cancers, including extrahepatic manifestation, in whom an R0 resection can be achieved much more frequently. Moreover, this patient cohort potentially suffered from a less aggressive form of disease, whereas our cohort was focused on advanced stages of intrahepatic cholangiocarcinoma only.
Previous systemic therapies just missed statistical significance as a prognostic factor in our study (
p = 0.054), which is attributed to the limited sample size and, therefore, a decreased statistical power. However, there is a clear trend that previous systemic therapy is associated with decreased survival (7.3 vs. 13.1 months in our study), which has been confirmed by other studies [
22]. Similarly as above, however, previous systemic therapy can be rather considered as a surrogate marker for progressive disease. Moreover, a bilobar tumor extent was associated with decreased survival rates compared to unilobar disease only, while mere tumor volume interestingly did not show to be a prognostic factor for survival after TARE in advanced ICC. Similar, the presence of extrahepatic disease had no impact on survival, indicating that the intrahepatic tumor spread remains the major determining factor for survival. This also suggests that TARE may be indicated in patients with limited metastasis and with liver-dominant disease, which has to evaluated in further studies. Serum levels of liver function such as albumin and bilirubin as well as the tumor markers did not correlate with survival in our study. Of note, only a minority of patients had impaired liver function in our cohort reflected by normal bilirubin levels in most patients. Interestingly, Edeline et al. found carcinoembryogenic antigen (CEA) to be a prognostic factor in advanced ICC undergoing combined radioembolization and chemotherapy [
25].
To date, there is no evidence that the choice of glass versus resin microspheres has a significant impact on tumor response or survival [
3,
10,
11,
22]. However, Levillain et al. showed that the efficacy of TARE in unresectable ICC significantly depends on the delivered tumor radiation dose. Mean tumoral radiation dose was higher with the partition model applied compared to the body-surface area model, suggesting that a personalized radiation activity regime should be performed for each patient [
13].
While in the present study,
90Y TARE was applied as a salvage therapy option for ICC, when other anticancer treatments including surgery had failed or disease relapse occurred,
90Y TARE might be combined with other anticancer treatments in a multimodality setting earlier in the course of the disease. A recent phase Ib trial of combined gemcitabine chemotherapy and
90Y TARE has proven an acceptable safety profile for gemcitabine doses up to 600 mg/m
2, with all patients experiencing grade 1 toxicity, 37.5% grade 2, and 12.5% grade 3 toxicities [
26]. Survival data of the study are still pending. These multimodal therapy regimes, including
90Y TARE, have the potential to improve survival and reduce side effects compared to sole chemotherapeutic approaches using high dose regimens. Furthermore, the advent of new chemotherapy regimens with improved survival rates [
6], immunotherapies, as well as improved patient selection, promise novel multimodal treatment options when combined with
90Y TARE for the treatment of ICC [
27,
28,
29]. The first prospective trial combining radioembolization and chemotherapy (again with cisplatin and gemcitabine), which was recently published, reported a median overall survival of 22 months following combined treatment [
25]. The improved survival rates in this study compared to our cohort is attributed again to the much-advanced tumor stages and similarly increased morbidity in our cohort, having undergone already multiple therapies, while the study cohort of Edeline et al. were all therapy-naïve when included in the protocol. A remarkable result of the study by Edeline et al. was that 9/41 patients (previously not suited for surgical resection) were able to undergo curative surgery following downstaging with combined radioembolization and chemotherapy.
This study is limited by its retrospective character, including a significant amount of loss to follow-up at 12 months, and additionally by the limited sample size of 47 patients. To overcome this problem, data were pooled from three collaborating tertiary care cancer centers to increase the size of the analyzed cohort. Nonetheless, the collected patient cohort was still heterogenic, especially with regard to previous therapies, limiting the ability to perform adequate subgroup analyses according to specific pre-treatments. The presented sample size limits the power of the analysis of potential prognostic factors, and interpretation of the retrieved results has to be performed with caution. Previous surgical as well as systemic therapies in patients with advanced ICC, moreover, have to be rather interpreted as surrogate markers of progressive disease, which was present in the patients with radioembolization being performed following previous therapies. Further studies with higher patient numbers and subsequently increased power are expected to reveal further prognostic factors, such as previous systemic therapies, which missed statistical significance in our cohort and which were identified as relevant in other cohorts. Additionally, is has to be emphasized that n = 3 patients received a repeated radioembolization within the observation period, which induces a certain bias.
The poor overall survival in the presented study cohort raises the question of whether TARE in patients with progressive disease or disease relapse after previous therapy has substantial benefit compared to best supportive care alone. This question, however, can only be answered through prospective randomized trials and, as already discussed, embedding radioembolization in a multimodal therapy regimen in patients with advanced ICC has to be further explored in subsequent research.

 ,
, 

{kind=link}