Cigarette Smoking and Root Filled Teeth Extraction: Systematic Review and Meta-Analysis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Question
- Population: Adults patients with root-filled teeth.
- Intervention: Presence of smoking habits, smoker.
- Comparison: Absence of smoking habits, non-smoker.
- Outcome: Extraction of root-filled teeth.
2.2. Inclusion and Exclusion Criteria
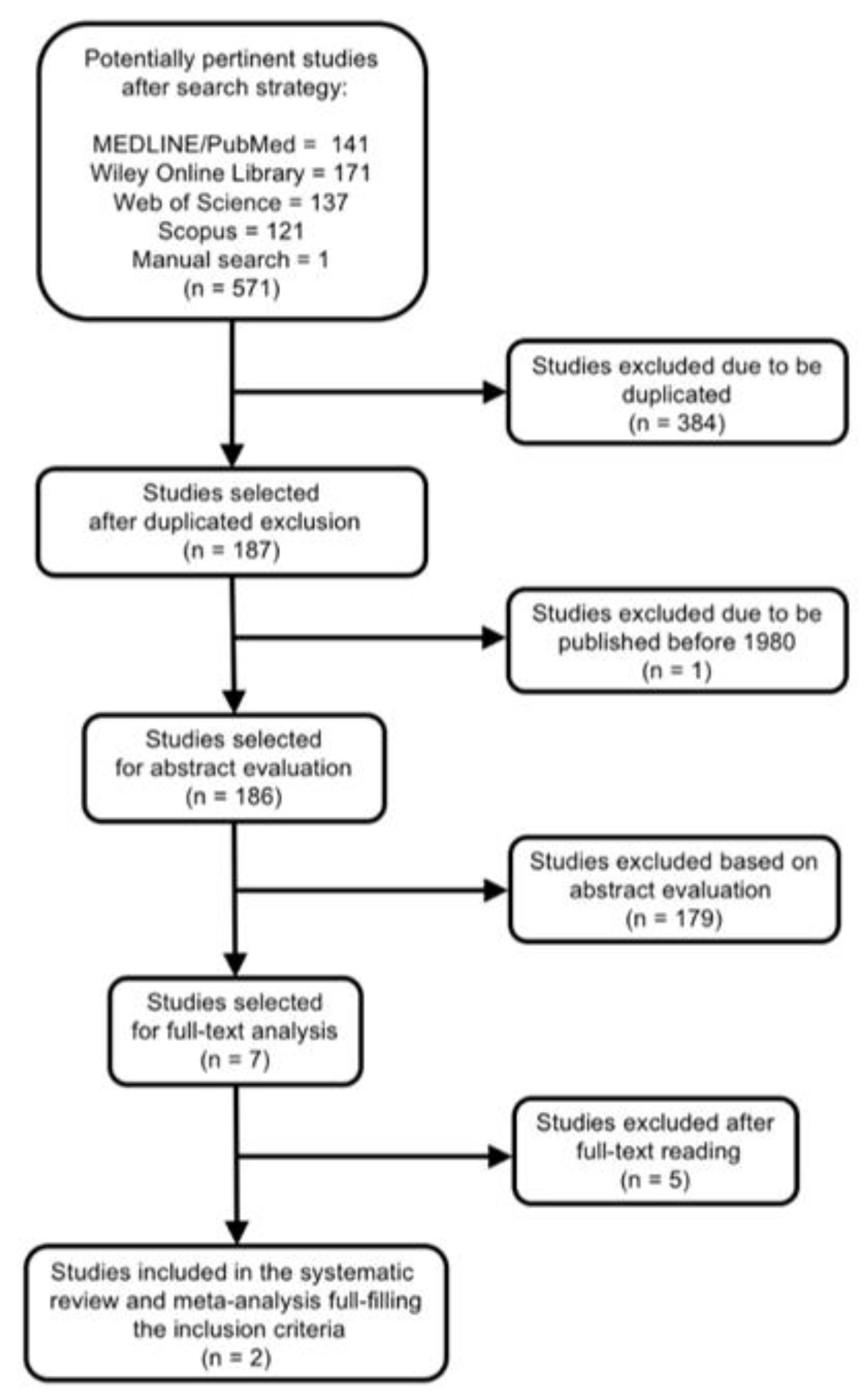
2.3. Literature Search
2.4. Data Extraction
2.5. Outcome Variables and Statistical Analysis
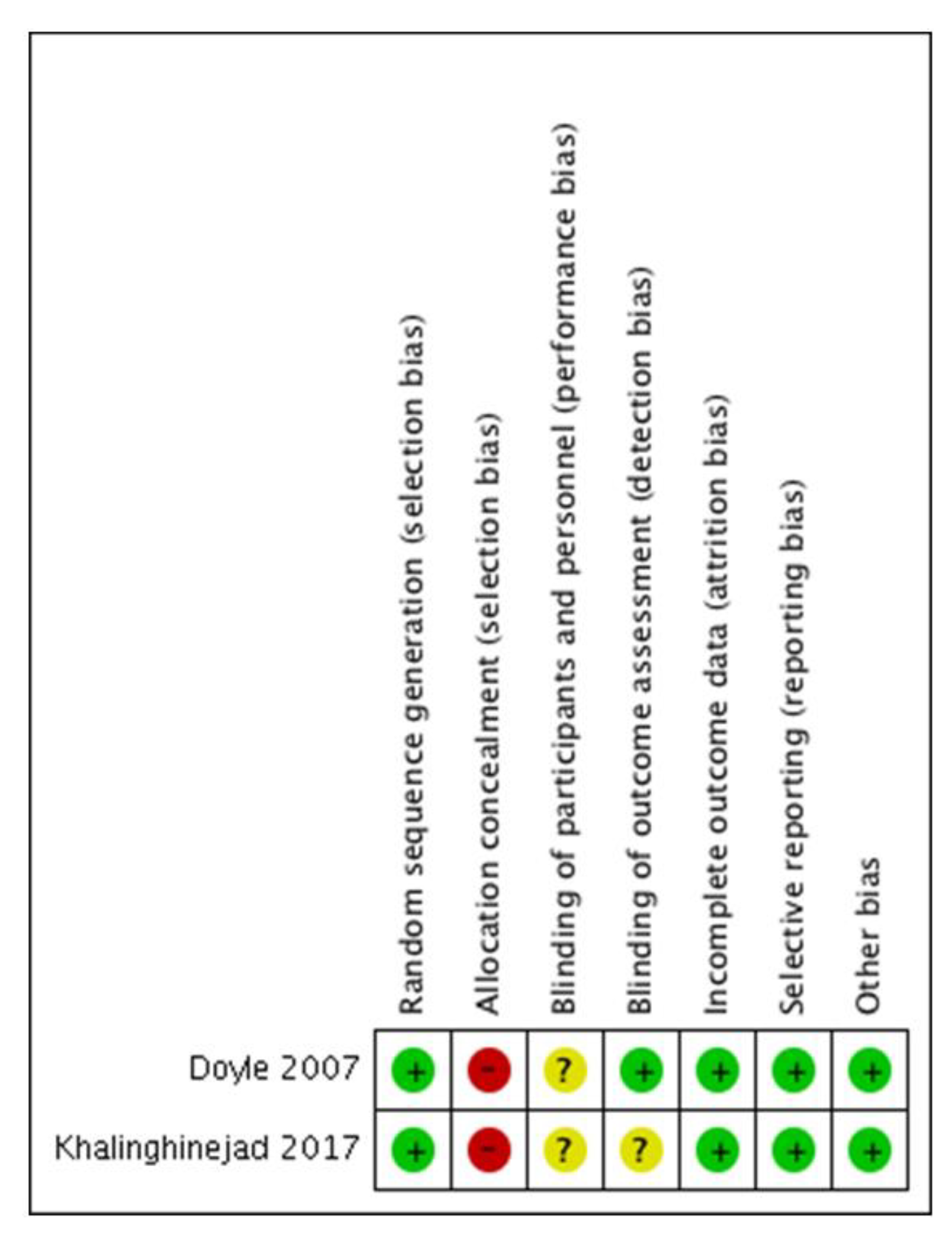
2.6. Quality Evidence Assessment and Risk of Bias in Individual Studies
3. Results
3.1. Study Characteristics
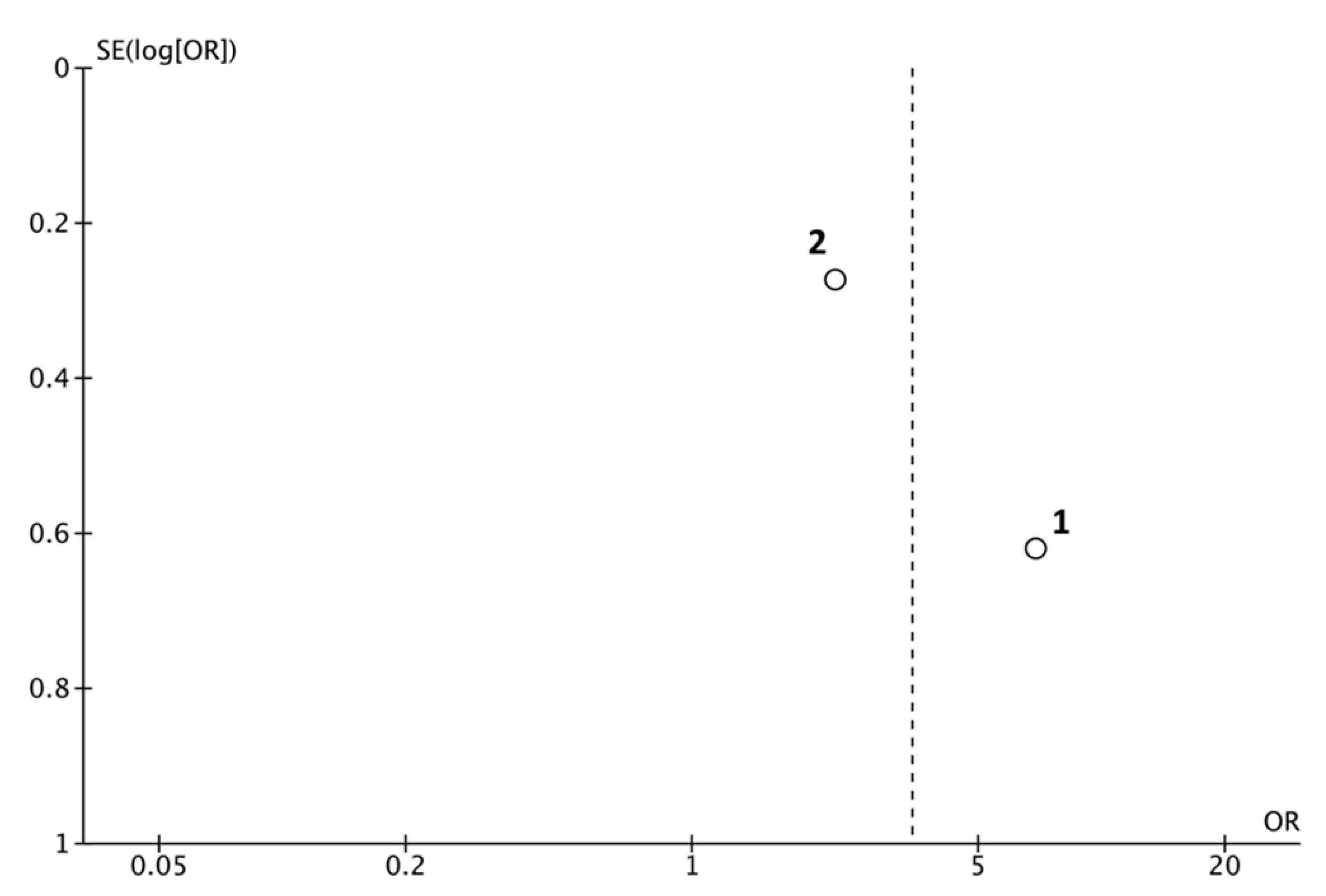
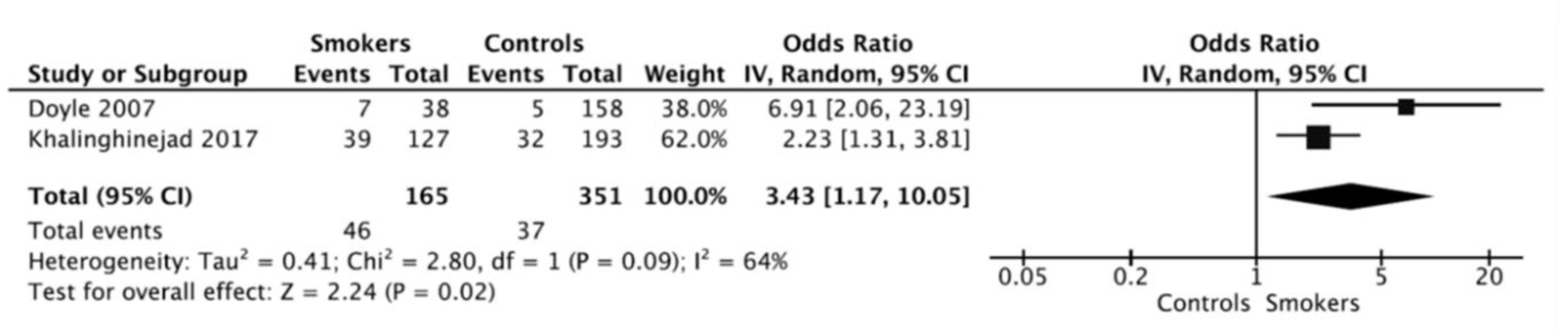
3.2. Meta-Analysis
3.3. Interpretation and Assessment of the Included Studies
3.4. Quality Evidence Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ricucci, D.; Siqueira, J.F. Biofilms and apical periodontitis: Study of prevalence and association with clinical and histopathologic findings. J. Endod. 2010, 36, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Ali, R.W.; Mudawi, A.M. Prevalence of apical periodontitis and frequency of root-filled teeth in an adult Sudanese population. Clin. Exp. Dent. Res. 2017, 3, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Kabak, Y.; Abbott, P.V. Prevalence of apical periodontitis and the quality of endodontic treatment in an adult Belarusian population. Int. Endod. J. 2005, 38, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Karabucak, B.; Bunes, A.; Chehoud, C.; Kohli, M.R.; Setzer, F. Prevalence of Apical Periodontitis in Endodontically Treated Premolars and Molars with Untreated Canal: A Cone-beam Computed Tomography Study. J. Endod. 2016, 42, 538–541. [Google Scholar] [CrossRef]
- Ricucci, D.; Lin, L.M.; Spångberg, L.S.W. Wound healing of apical tissues after root canal therapy: A long-term clinical, radiographic, and histopathologic observation study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 609–621. [Google Scholar] [CrossRef]
- Siqueira, J.F. Aetiology of root canal treatment failure: Why well-treated teeth can fail. Int. Endod. J. 2001, 34, 1–10. [Google Scholar] [CrossRef]
- Vire, D.E. Failure of endodontically treated teeth: Classification and evaluation. J. Endod. 1991, 17, 338–342. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Gulabivala, K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: Part 2: Tooth survival. Int. Endod. J. 2011, 44, 610–625. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F.; Bate, A.L.; Pitt Ford, T.R. Histologic Investigation of Root Canal–treated Teeth with Apical Periodontitis: A Retrospective Study from Twenty-four Patients. J. Endod. 2009, 35, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Ricucci, D.; Siqueira, J.F. Infection in a complex network of apical ramifications as the cause of persistent apical periodontitis: A case report. J. Endod. 2013, 39, 1179–1184. [Google Scholar] [CrossRef]
- Costa, F.F.N.P.; Pacheco-Yanes, J.; Siqueira, J.F.; Oliveira, A.C.S.; Gazzaneo, I.; Amorim, C.A.; Santos, P.H.B.; Alves, F.R.F. Association between missed canals and apical periodontitis. Int. Endod. J. 2019, 52, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Danesh, N.; Ljunggren, A.C.; Wolf, E.; Fransson, H. Development of criteria for investigation of periapical tissue from root-filled teeth. Acta Odontol. Scand. 2019, 77, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Avila, G.; Galindo-Moreno, P.; Soehren, S.; Misch, C.E.; Morelli, T.; Wang, H.-L. A Novel Decision-Making Process for Tooth Retention or Extraction. J. Periodontol. 2009, 80, 476–491. [Google Scholar] [CrossRef] [PubMed]
- Chatzopoulos, G.S.; Koidou, V.P.; Lunos, S.; Wolff, L.F. Implant and root canal treatment: Survival rates and factors associated with treatment outcome. J. Dent. 2018, 71, 61–66. [Google Scholar] [CrossRef]
- Segura-Egea, J.J.; Martín-González, J.; Castellanos-Cosano, L. Endodontic medicine: Connections between apical periodontitis and systemic diseases. Int. Endod. J. 2015, 48, 933–951. [Google Scholar] [CrossRef]
- Segura-Egea, J.J.; Cabanillas-Balsera, D.; Jiménez-Sánchez, M.C.; Martín-González, J. Endodontics and diabetes: Association versus causation. Int. Endod. J. 2019, 52, 790–802. [Google Scholar] [CrossRef]
- Marending, M.; Peters, O.A.; Zehnder, M. Factors affecting the outcome of orthograde root canal therapy in a general dentistry hospital practice. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 119–124. [Google Scholar] [CrossRef]
- Cabanillas-Balsera, D.; Martín-González, J.; Montero-Miralles, P.; Sánchez-Domínguez, B.; Jiménez-Sánchez, M.C.; Segura-Egea, J.J. Association between diabetes and nonretention of root filled teeth: A systematic review and meta-analysis. Int. Endod. J. 2019, 52, 297–306. [Google Scholar] [CrossRef]
- Duncan, H.F.; Pitt Ford, T.R. The potential association between smoking and endodontic disease. Int. Endod. J. 2006, 39, 843–854. [Google Scholar] [CrossRef]
- Doyle, S.L.; Hodges, J.S.; Pesun, I.J.; Law, A.S.; Bowles, W.R. Retrospective cross sectional comparison of initial nonsurgical endodontic treatment and single-tooth implants. Compend. Contin. Educ. Dent. 2007, 28, 296–301. [Google Scholar] [CrossRef]
- Ghattas Ayoub, C.; Aminoshariae, A.; Bakkar, M.; Ghosh, S.; Bonfield, T.; Demko, C.; Montagnese, T.A.; Mickel, A.K. Comparison of IL-1β, TNF-α, hBD-2, and hBD-3 Expression in the Dental Pulp of Smokers Versus Nonsmokers. J. Endod. 2017, 43, 2009–2013. [Google Scholar] [CrossRef] [PubMed]
- Haverstock, B.D.; Mandracchia, V.J. Cigarette smoking and bone healing: Implications in foot and ankle surgery. J. Foot Ankle Surg. 1998, 37, 69–74. [Google Scholar] [CrossRef]
- Pinto, K.P.; Ferreira, C.M.; Maia, L.C.; Sassone, L.M.; Fidalgo, T.K.S.; Silva, E.J.N.L. Does tobacco smoking predispose to apical periodontitis and endodontic treatment need? A systematic review and meta-analysis. Int. Endod. J. 2020, 53, 1068–1083. [Google Scholar] [CrossRef]
- Krall, E.A.; Sosa, C.A.; Garcia, C.; Nunn, M.E.; Caplan, D.J.; Garcia, R.I. Cigarette Smoking Increases the Risk of Root Canal Treatment. J. Dent. Res. 2006, 85, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Walter, C.; Rodriguez, F.R.; Taner, B.; Hecker, H.; Weiger, R. Association of tobacco use and periapical pathosis—A systematic review. Int. Endod. J. 2012, 45, 1065–1073. [Google Scholar] [CrossRef]
- López-López, J.; Castellanos-Cosano, L.; Estrugo-Devesa, A.; Gómez-Vaquero, C.; Velasco-Ortega, E.; Segura-Egea, J.J. Radiolucent periapical lesions and bone mineral density in post-menopausal women. Gerodontology 2015, 32, 195–201. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Bader, J.D. Systematic reviews and their implications for dental practice. Tex. Dent. J. 2004, 121, 380–387. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Lewis, S.; Clarke, M. Forest plots: Trying to see the wood and the trees. BMJ 2001, 322, 1479–1480. [Google Scholar] [CrossRef] [PubMed]
- The Cochrane Collaboration. Review Manager (RevMan); Computer program, Version 5.4; The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Oxford Centre for Evidence-Based Medicine. Levels of Evidence—CEBM; Oxford Centre for Evidence-Based Medicine: Oxford, UK, 2020. [Google Scholar]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence—Study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355. [Google Scholar] [CrossRef]
- Zadik, Y.; Sandler, V.; Bechor, R.; Salehrabi, R. Analysis of factors related to extraction of endodontically treated teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 106, 31–35. [Google Scholar] [CrossRef]
- Zhong, Y.; Garcia, R.; Kaye, E.K.; Cai, J.; Kaufman, J.S.; Trope, M.; Wilcosky, T.; Caplan, D.J. Association of endodontic involvement with tooth loss in the veterans affairs dental longitudinal study. J. Endod. 2010, 36, 1943–1949. [Google Scholar] [CrossRef]
- Touré, B.; Faye, B.; Kane, A.W.; Lo, C.M.; Niang, B.; Boucher, Y. Analysis of Reasons for Extraction of Endodontically Treated Teeth: A Prospective Study. J. Endod. 2011, 37, 1512–1515. [Google Scholar] [CrossRef]
- Olcay, K.; Ataoglu, H.; Belli, S. Evaluation of Related Factors in the Failure of Endodontically Treated Teeth: A Cross-sectional Study. J. Endod. 2018, 44, 38–45. [Google Scholar] [CrossRef]
- Khalighinejad, N.; Aminoshariae, A.; Kulild, J.C.; Wang, J.; Mickel, A. The Influence of Periodontal Status on Endodontically Treated Teeth: 9-year Survival Analysis. J. Endod. 2017, 43, 1781–1785. [Google Scholar] [CrossRef]
- Doyle, S.L.; Hodges, J.S.; Pesun, I.J.; Baisden, M.K.; Bowles, W.R. Factors affecting outcomes for single-tooth implants and endodontic restorations. J. Endod. 2007, 33, 399–402. [Google Scholar] [CrossRef]
- Costa, T.H.R.; de Figueiredo Neto, J.A.; de Oliveira, A.E.F.; de Figueierdo Lopes e Maia, M.; de Almeida, A.L. Association between chronic apical periodontitis and coronary artery disease. J. Endod. 2014, 40, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Sánchez, M.; Cabanillas-Balsera, D.; Areal-Quecuty, V.; Velasco-Ortega, E.; Martín-González, J.; Segura-Egea, J. Cardiovascular diseases and apical periodontitis: Association not always implies causality. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e652–e659. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Segura-Egea, J.J.; Fouad, A.F.; Pulikkotil, S.J.; Dummer, P.M.H. Association between diabetes and the outcome of root canal treatment in adults: An umbrella review. Int. Endod. J. 2020, 53, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Segura-Egea, J.J.; Martín-González, J.; Cabanillas-Balsera, D.; Fouad, A.F.; Velasco-Ortega, E.; López-López, J. Association between diabetes and the prevalence of radiolucent periapical lesions in root-filled teeth: Systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 1133–1141. [Google Scholar] [CrossRef]
- Mindiola, M.J.; Mickel, A.K.; Sami, C.; Jones, J.J.; Lalumandier, J.A.; Nelson, S.S. Endodontic treatment in an American Indian population: A 10-year retrospective study. J. Endod. 2006, 32, 828–832. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Dietrich, T.; Bornstein, M.M.; Casals Peidró, E.; Preshaw, P.M.; Walter, C.; Wennström, J.L.; Bergström, J. Oral health risks of tobacco use and effects of cessation. Int. Dent. J. 2010, 60, 7–30. [Google Scholar] [CrossRef]
- Mai, X.; Wactawski-Wende, J.; Hovey, K.M.; LaMonte, M.J.; Chen, C.; Tezal, M.; Genco, R.J. Associations between smoking and tooth loss according to the reason for tooth loss: The Buffalo OsteoPerio Study. J. Am. Dent. Assoc. 2013, 144, 252–265. [Google Scholar] [CrossRef]
- Leite, F.R.M.; Nascimento, G.G.; Scheutz, F.; López, R. Effect of Smoking on Periodontitis: A Systematic Review and Meta-regression. Am. J. Prev. Med. 2018, 54, 831–841. [Google Scholar] [CrossRef]
- Graetz, C.; Plaumann, A.; Schlattmann, P.; Kahl, M.; Springer, C.; Sälzer, S.; Gomer, K.; Dörfer, C.; Schwendicke, F. Long-term tooth retention in chronic periodontitis—Results after 18 years of a conservative periodontal treatment regimen in a university setting. J. Clin. Periodontol. 2017, 44, 169–177. [Google Scholar] [CrossRef]
- De Maat, M.P.M.; Kluft, C. The association between inflammation markers, coronary artery disease and smoking. Vascul. Pharmacol. 2002, 39, 137–139. [Google Scholar] [CrossRef]
- Johnson, G.K.; Guthmiller, J.M. The impact of cigarette smoking on periodontal disease and treatment. Periodontol. 2000 2007, 44, 178–194. [Google Scholar] [CrossRef] [PubMed]
- Trowbridge, H.O. Immunological aspects of chronic inflammation and repair. J. Endod. 1990, 16, 54–61. [Google Scholar] [CrossRef]
- Holt, P.G. Immune and inflammatory function in cigarette smokers. Thorax 1987, 42, 241–249. [Google Scholar] [CrossRef]
- Tappia, P.S.; Troughton, K.L.; Langley-Evans, S.C.; Grimble, R.F. Cigarette smoking influences cytokine production and antioxidant defences. Clin. Sci. 1995, 88, 485–489. [Google Scholar] [CrossRef]
- Bazdyrev, E.D.; Polikutina, O.M.; Kalichenko, N.A.; Slepynina, Y.S.; Uchasova, E.G.; Pavlova, V.Y.; Barbarash, O.L. Relationship between smoking and indicators of systemic inflammation in patients with coronary heart disease. Klin. Med. (Mosk). 2017, 95, 264–271. [Google Scholar]
- Fröhlich, M.; Sund, M.; Löwel, H.; Imhof, A.; Hoffmeister, A.; Koenig, W. Independent association of various smoking characteristics with markers of systemic inflammation in men. Results from a representative sample of the general population (MONICA Augsburg Survey 1994/95). Eur. Heart J. 2003, 24, 1365–1372. [Google Scholar] [CrossRef]
- Ijzerman, R.G.; Serne, E.H.; Van Weissenbruch, M.H.; De Jongh, R.T.; Stehouwer, C.D.A. Cigarette smoking is associated with an acute impairment of microvascular function in humans. Clin. Sci. 2003, 104, 247–252. [Google Scholar] [CrossRef]
- Wong, L.S.; Green, H.M.; Feugate, J.E.; Yadav, M.; Nothnagel, E.A.; Martins-Green, M. Effects of second-hand smoke on structure and function of fibroblasts, cells that are critical for tissue repair and remodeling. BMC Cell Biol. 2004, 5. [Google Scholar] [CrossRef]
- Eder, A.; Koegl, E.; Von Duvillard, S.P.; Sinzinger, H.; Berent, R. Influence of cigarette smoking on synthesis of eicosanoids, isoprostanes and lipoxygenase metabolites in apical periodontitis. Arch. Oral Biol. 2012, 57, 1133–1140. [Google Scholar] [CrossRef]
- Bergstrom, J.; Babcan, J.; Eliasson, S. Tobacco smoking and dental periapical condition. Eur. J. Oral Sci. 2004, 112, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Balto, H.A.; Alabdulaaly, L.; Bahammam, S.; Al-Ekrish, A.A. Comparative analysis of prevalence of apical periodontitis in smokers and non-smokers using cone-beam computed tomography. Saudi Dent. J. 2019, 31, 52–57. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Excluded Reason | Authors | Year |
|---|---|---|
| Not provide necessary data to meta-analysis (absence initial n° RFT) | 1. Zadik et al. | 2008 [38] |
| 2. Zhong et al. | 2010 [39] | |
| 3. Touré et al. | 2011 [40] | |
| 4. Olcay et al. | 2018 [41] | |
| Not provide necessary data to meta-analysis (absence n° RFT extracted) | 5. Marending et al. | 2005 [17] |
| Authors | Year | Study Design | RCT | Association Diab.-Extr.RFT | Evidence Level [34] |
|---|---|---|---|---|---|
| 1. Doyle et al. | 2007 [20] | Retrospective chart review (follow up 1 years) | Controls: 158 Smokers: 38 | YES; p = 0.0004 | 3b |
| 2. Khalinghinejad et al. | 2017 [42] | Longitudinal (retrospective 9 years) | Controls: 193 Smokers: 127 | YES; p = 0.003 | 3b |
| Authors | Year | Number of RFT | Non-Smoker Controls | Smoker Patients | OR (95% C.I.) | p | ||
|---|---|---|---|---|---|---|---|---|
| Extracted*RFT/Total RFT | Extracted*RFT (%) | Extracted*RFT/Total RFT | Extracted*RFT (%) | |||||
| Doyle et al. | 2007 [20] | 196 | 5/158 | 3.2% | 7/38 | 18.4% | 6.9 (2.1–23.2) | 0.0004 |
| Khalinghinejad et al. | 2017 [42] | 320 | 32/193 | 16.6% | 39/127 | 30.7% | 2.2 (1.31–3.81) | 0.003 |
| OVERALL | 516 | 37/351 | 10.5% | 46/165 | 27.9% | 3.43 (1.2–10.1) * | 0.002 | |
| Certainty Assessment | Certainty | Importance | ||||||
|---|---|---|---|---|---|---|---|---|
| Number of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | ||
| Extracted root filled teeth | ||||||||
| 2 | Observational studies | serious a | serious b | not serious | not serious | strong association all plausible residual confounding would reduce the demonstrated effect | ⊕⊕○○ Low | IMPORTANT |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabanillas-Balsera, D.; Segura-Egea, J.J.; Jiménez-Sánchez, M.C.; Areal-Quecuty, V.; Sánchez-Domínguez, B.; Montero-Miralles, P.; Saúco-Márquez, J.J.; Martín-González, J. Cigarette Smoking and Root Filled Teeth Extraction: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 3179. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103179
Cabanillas-Balsera D, Segura-Egea JJ, Jiménez-Sánchez MC, Areal-Quecuty V, Sánchez-Domínguez B, Montero-Miralles P, Saúco-Márquez JJ, Martín-González J. Cigarette Smoking and Root Filled Teeth Extraction: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(10):3179. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103179
Chicago/Turabian StyleCabanillas-Balsera, Daniel, Juan J. Segura-Egea, María C. Jiménez-Sánchez, Victoria Areal-Quecuty, Benito Sánchez-Domínguez, Paloma Montero-Miralles, Juan J. Saúco-Márquez, and Jenifer Martín-González. 2020. "Cigarette Smoking and Root Filled Teeth Extraction: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 10: 3179. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103179