Efficacy and Safety of Combined Extracts of Cornus officinalis and Ribes fasciculatum for Body Fat Reduction in Overweight Women

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Treatment Material
2.3. Study Design
2.4. Efficacy Evaluation
2.5. Safety Assessment
2.6. Statistical Analysis
3. Results
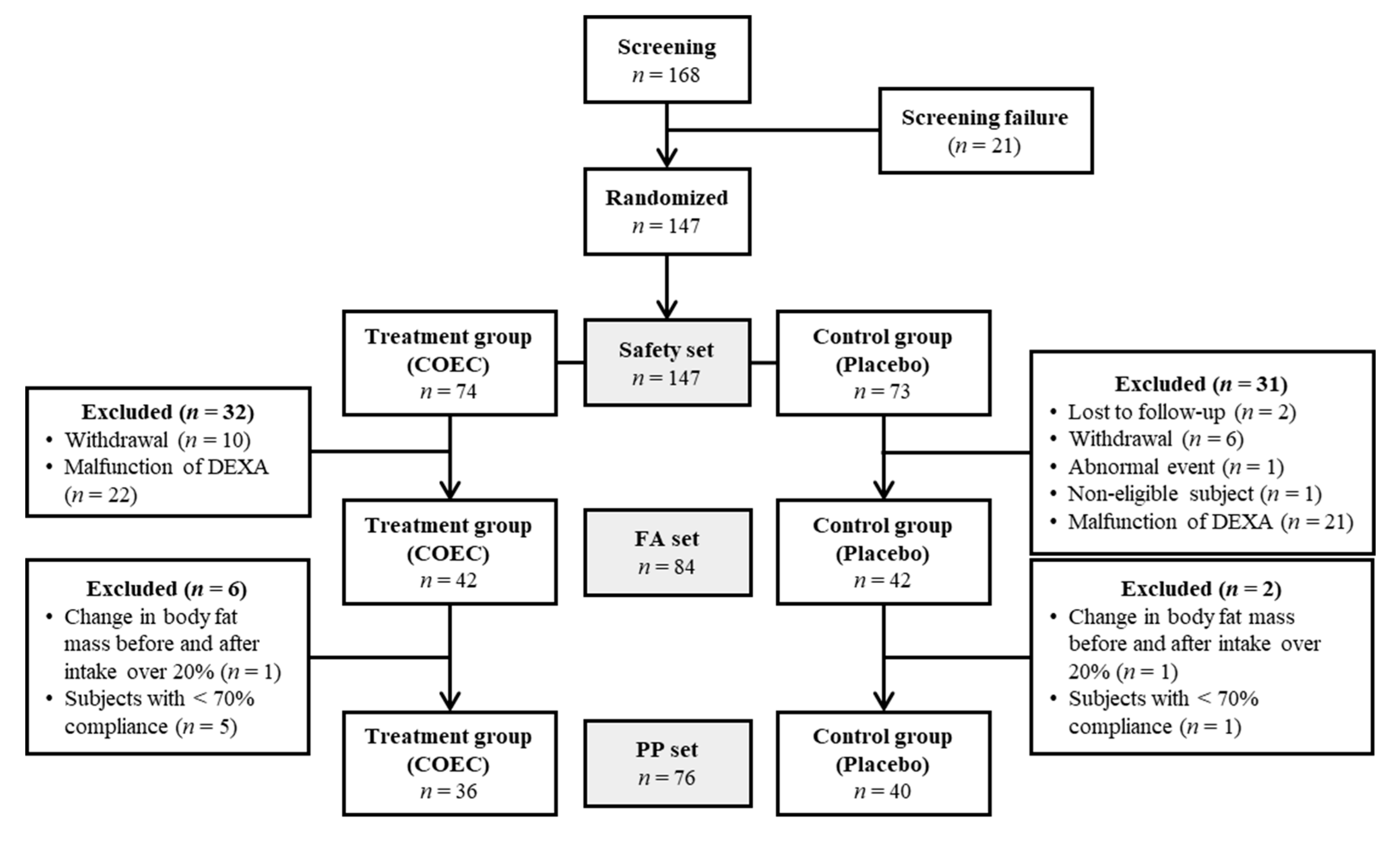
3.1. Inclusion and Exclusion of Participants and Baseline Characteristics
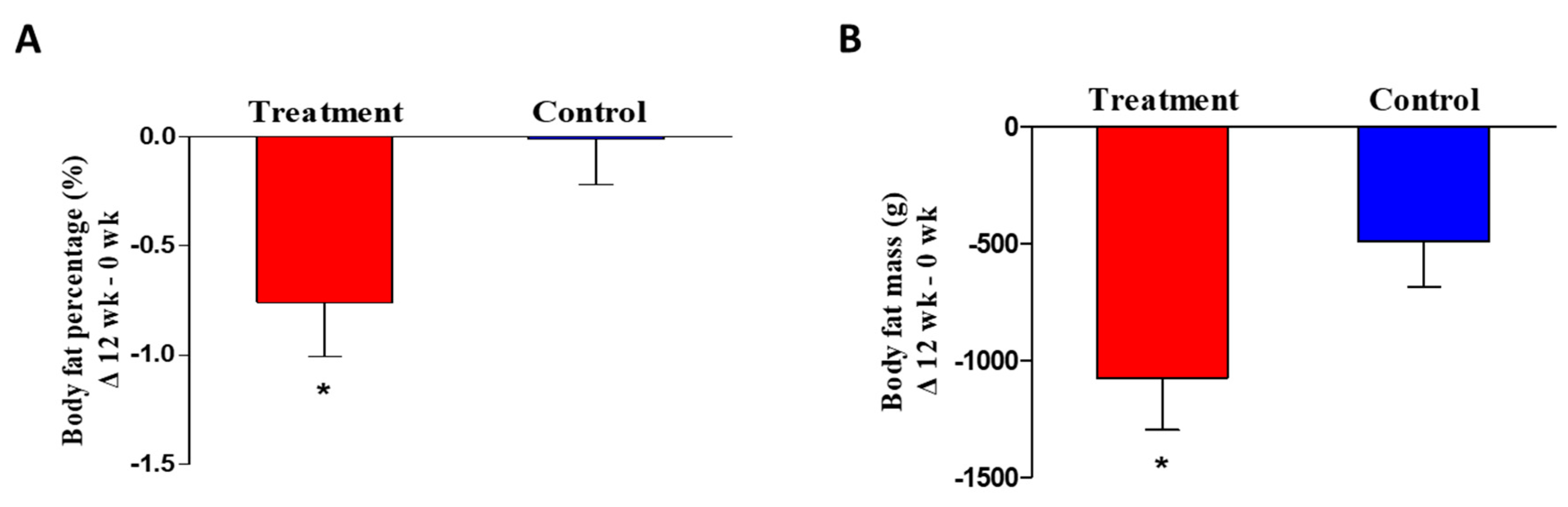
3.2. Efficacy Assessment
3.3. Safety Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pi-Sunyer, X. The Medical Risks of Obesity. Postgrad. Med. 2009, 121, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Hudda, M.T.; Nightingale, C.M.; Donin, A.S.; Owen, C.G.; Rudnicka, A.R.; Wells, J.C.K.; Rutter, H.; Cook, D.G.; Whincup, P.H. Patterns of childhood body mass index (BMI), overweight and obesity in South Asian and black participants in the English National child measurement programme: Effect of applying BMI adjustments standardising for ethnic differences in BMI-body fatness associations. Int. J. Obes. 2018, 42, 662–670. [Google Scholar] [CrossRef] [Green Version]
- Chiolero, A. Why causality, and not prediction, should guide obesity prevention policy. Lancet Public Health 2018, 3, e461–e462. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, T.I.A. From fat cells through an obesity theory. Eur. J. Clin. Nutr. 2018, 72, 1329–1335. [Google Scholar] [CrossRef]
- Longo, M.; Zatterale, F.; Naderi, J.; Parrillo, L.; Formisano, P.; Raciti, G.A.; Beguinot, F.; Miele, C. Adipose Tissue Dysfunction as Determinant of Obesity-Associated Metabolic Complications. Int. J. Mol. Sci. 2019, 20, 2358. [Google Scholar] [CrossRef] [Green Version]
- Hall, K.D.; Kahan, S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef]
- Kang, J.G.; Park, C.-Y. Anti-Obesity Drugs: A Review about Their Effects and Safety. Diabetes Metab. J. 2012, 36, 13–25. [Google Scholar] [CrossRef] [Green Version]
- Bray, G.A. Use and Abuse of Appetite-Suppressant Drugs in the Treatment of Obesity. Ann. Intern. Med. 1993, 119, 707–713. [Google Scholar] [CrossRef]
- Hensrud, N.D. Pharmacotherapy for Obesity. Med. Clin. N. Am. 2000, 84, 463–476. [Google Scholar] [CrossRef]
- Kim, M.K.; Lee, W.Y.; Kang, J.H.; Kang, J.H.; Kim, B.T.; Kim, S.M.; Kim, E.M.; Suh, S.H.; Shin, H.J.; Lee, K.R.; et al. 2014 clinical practice guidelines for overweight and obesity in Korea. Endocrinol. Metab. 2014, 29, 405–409. [Google Scholar] [CrossRef] [Green Version]
- El-Ishaq, A.; Alshawsh, M.A.; Chik, Z. Evaluating the oestrogenic activities of aqueous root extract of Asparagus africanus Lam in female Sprague-Dawley rats and its phytochemical screening using Gas Chromatography-Mass Spectrometry (GC/MS). PeerJ 2019, 7, e7254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teiten, M.-H.; Gaascht, F.; Dicato, M.; Diederich, M. Anticancer bioactivity of compounds from medicinal plants used in European medieval traditions. Biochem. Pharmacol. 2013, 86, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Che, C.-T.; Zhang, H. Plant Natural Products for Human Health. Int. J. Mol. Sci. 2019, 20, 830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iriti, M.; Varoni, E.M.; Vitalini, S. Healthy Diets and Modifiable Risk Factors for Non-Communicable Diseases—The European Perspective. Foods 2020, 9, 940. [Google Scholar] [CrossRef]
- Saito, M.; Yoneshiro, T.; Matsushita, M. Food Ingredients as Anti-Obesity Agents. Trends Endocrinol. Metab. 2015, 26, 585–587. [Google Scholar] [CrossRef]
- Sun, N.-N.; Wu, T.-Y.; Chau, C.-F. Natural Dietary and Herbal Products in Anti-Obesity Treatment. Molecules 2016, 21, 1351. [Google Scholar] [CrossRef]
- Lee, N.-H.; Seo, C.-S.; Lee, H.-Y.; Jung, D.-Y.; Lee, J.-K.; Lee, J.-A.; Song, K.Y.; Shin, H.-K.; Lee, M.-Y.; Seo, Y.B.; et al. Hepatoprotective and Antioxidative Activities of Cornus officinalis against Acetaminophen-Induced Hepatotoxicity in Mice. Evid. Based Complement. Altern. Med. 2011, 2012, 804924. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Kim, Y.-K.; Choi, M.K.; Oh, J.; Kwak, H.B.; Kim, J.-J. Effect of Cornus Officinalis on Receptor Activator of Nuclear Factor-kappaB Ligand (RANKL)-induced Osteoclast Differentiation. J. Bone Metab. 2012, 19, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Tian, W.; Zhao, J.; Lee, J.H.; Akanda, R.; Cho, J.H.; Kim, S.-K.; Choi, Y.-J.; Park, B.-Y. Neuroprotective Effects of Cornus officinalis on Stress-Induced Hippocampal Deficits in Rats and H2O2-Induced Neurotoxicity in SH-SY5Y Neuroblastoma Cells. Antioxidants 2019, 9, 27. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.K.; Im, J.S.; Kim, B.S.; Cha, D.S.; Kwon, J.; Oh, C.H.; Ma, S.Y.; Yu, J.H.; Nam, J.I.; Jeon, H. Anti-nociceptive Properties of Ribes fasciculatum. Nat. Prod. Sci. 2013, 19, 311–315. [Google Scholar]
- Jeon, H.; Cha, D.S. Anti-aging properties of Ribes fasciculatum in Caenorhabditis elegans. Chin. J. Nat. Med. 2016, 14, 335–342. [Google Scholar] [PubMed]
- Shah, S.A.A.; Akhter, N.; Auckloo, B.N.; Khan, I.; Lu, Y.; Wang, K.; Wu, B.; Guo, Y. Structural Diversity, Biological Properties and Applications of Natural Products from Cyanobacteria. A Review. Mar. Drugs 2017, 15, 354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, S.; Hoskins, C. Drug development: Lessons from nature. Biomed. Rep. 2017, 6, 612–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulrich-Merzenich, G.; Panek, D.; Zeitler, H.; Wagner, H.; Vetter, H. New perspectives for synergy research with the “omic”-technologies. Phytomedicine 2009, 16, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Rejhova, A.; Opattová, A.; Čumová, A.; Slíva, D.; Vodička, P. Natural compounds and combination therapy in colorectal cancer treatment. Eur. J. Med. Chem. 2018, 144, 582–594. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Lim, E.; Yeo, S.; Yong, Y.; Yang, J.; Jeong, S.-Y. Anti-Menopausal Effects of Cornus officinalis and Ribes fasciculatum Extract In Vitro and In Vivo. Nutrients 2020, 12, 369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, E.; Lee, C.G.; Jeong, H.; Yeo, S.; Kim, J.A.; Jeong, S.-Y. Antiadipogenic Effects of Mixtures of Cornus officinalis and Ribes fasciculatum Extracts on 3T3-L1 Preadipocytes and High-Fat Diet-Induced Mice. Molecules 2020, 25, 2350. [Google Scholar] [CrossRef]
- Fu, C.; Jiang, Y.; Guo, J.; Su, Z. Natural Products with Anti-obesity Effects and Different Mechanisms of Action. J. Agric. Food Chem. 2016, 64, 9571–9585. [Google Scholar] [CrossRef]
- Qian, D.S.; Zhu, Y.F.; Zhu, Q. Effect of alcohol extract of Cornus officinalis Sieb. et Zucc on GLUT4 expression in skeletal muscle in type 2 (non-insulin-dependent) diabetic mellitus rats. China J. Chin. Mater. Med. 2001, 26, 859–862. [Google Scholar]
- Chauhan, A.; Sharma, P.; Srivastava, P.; Kumar, N.; Dudhe, R. Plants Having Potential Antidiabetic Activity: A Review. Der Pharm. Lett. 2009, 2, 369–387. [Google Scholar]
- Jung, J.W.; Kim, S.J.; Ahn, E.M.; Oh, S.R.; Lee, H.J.; Jeong, J.A.; Lee, J.Y. Ribes fasciculatum var. chinense attenuated allergic inflammation in vivo and in vitro. Biomol. Ther. 2014, 22, 547–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, J.W. Possible anti-obesity therapeutics from nature—A review. Phytochemistry 2010, 71, 1625–1641. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Luo, N.; Klein, R.L.; Garvey, W.T. Adiponectin promotes adipocyte differentiation, insulin sensitivity, and lipid accumulation. J. Lipid Res. 2005, 46, 1369–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of Overweight and Obesity in the United States, 1999–2004. JAMA 2006, 295, 1549–1555. [Google Scholar] [CrossRef]
- Yang, L.; Colditz, G.A. Prevalence of Overweight and Obesity in the United States, 2007–2012. JAMA Intern. Med. 2015, 175, 1412–1413. [Google Scholar] [CrossRef] [Green Version]
- Morselli, E.; Santos, R.D.S.; Gao, S.; Ávalos, Y.; Criollo, A.; Palmer, B.F.; Clegg, D.J. Impact of estrogens and estrogen receptor-α in brain lipid metabolism. Am. J. Physiol. Metab. 2018, 315, E7–E14. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.-H.; Chun, H.; Kwon, J.-W. Gender Differences in the Effect of Obesity on Chronic Diseases among the Elderly Koreans. J. Korean Med. Sci. 2011, 26, 250–257. [Google Scholar] [CrossRef]
- Foong, K.W.; Bolton, H. Obesity and ovarian cancer risk: A systematic review. Post Reprod. Health 2017, 23, 183–198. [Google Scholar] [CrossRef]
- Engin, A. Obesity-associated Breast Cancer: Analysis of risk factors. Adv. Exp. Med. Biol. 2017, 960, 571–606. [Google Scholar] [CrossRef]
- Kushner, R.F. Clinical Assessment and Management of Adult Obesity. Circulation 2012, 126, 2870–2877. [Google Scholar] [CrossRef] [Green Version]
- Heymsfield, S.B.; Cefalu, W.T. Does Body Mass Index Adequately Convey a Patient’s Mortality Risk? JAMA 2013, 309, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Goss, A.M.; Gower, B.; Soleymani, T.; Stewart, M.; Pendergrass, M.; Lockhart, M.; Krantz, O.; Dowla, S.; Bush, N.; Barry, V.G.; et al. Effects of weight loss during a very low carbohydrate diet on specific adipose tissue depots and insulin sensitivity in older adults with obesity: A randomized clinical trial. Nutr. Metab. 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, A.; Mousavi, S.M.; Mokhtari, T.; Parohan, M.; Milajerdi, A. Metformin Therapy Reduces Obesity Indices in Children and Adolescents: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Child. Obes. 2020, 16, 174–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattsson, S.; Vano, E. ICRP perspective on criteria of acceptability for medical radiological equipment. Radiat. Prot. Dosim. 2012, 153, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, J.M.; Carbajo, M.-A.; Lopez, M.; Castro, M.-J.; Ruiz-Tovar, J.; Garcia, S.; Castro-Alija, M.J. Changes in Lipid Profile, Body Weight Variables and Cardiovascular Risk in Obese Patients Undergoing One-Anastomosis Gastric Bypass. Int. J. Environ. Res. Public Health 2020, 17, 5858. [Google Scholar] [CrossRef]
- Ravelli, A.C.J.; Van Der Meulen, J.H.P.; Osmond, C.; Barker, D.J.P.; Bleker, O.P. Infant feeding and adult glucose tolerance, lipid profile, blood pressure, and obesity. Arch. Dis. Child. 2000, 82, 248–252. [Google Scholar] [CrossRef] [Green Version]
- New, M.I.; Roberts, T.N.; Bierman, E.L.; Reader, G.G. The Significance of Blood Lipid Alterations in Diabetes Mellitus. Diabetes 1963, 12, 208–212. [Google Scholar] [CrossRef]
- Frantz, I.D.; Dawson, E.A.; Ashman, P.L.; Gatewood, L.C.; Bartsch, G.E.; Kuba, K.; Brewer, E.R. Test of effect of lipid lowering by diet on cardiovascular risk. The Minnesota Coronary Survey. Arter. Off. J. Am. Hear. Assoc. Inc. 1989, 9, 129–135. [Google Scholar] [CrossRef] [Green Version]
- Ooi, G.J.; Doyle, L.; Tie, T.; Wentworth, J.M.; Laurie, C.; Earnest, A.; Cowley, M.A.; Sikaris, K.A.; Le Roux, C.W.; Burton, P.R.; et al. Weight loss after laparoscopic adjustable gastric band and resolution of the metabolic syndrome and its components. Int. J. Obes. 2017, 41, 902–908. [Google Scholar] [CrossRef]
- Cunha, F.M.; Oliveira, J.A.G.; Preto, J.; Saavedra, A.; Costa, M.M.; Magalhães, D.; Lau, E.; Bettencourt-Silva, R.; Freitas, P.; Varela, A.; et al. The Effect of Bariatric Surgery Type on Lipid Profile: An Age, Sex, Body Mass Index and Excess Weight Loss Matched Study. Obes. Surg. 2015, 26, 1041–1047. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Treatment Group (n = 36) | Control Group (n = 40) | Total (n = 76) | p-Value | |
|---|---|---|---|---|
| Age | ||||
| Mean ± SD | 48.25 ± 9.66 | 48.60 ± 10.40 | 48.43 ± 9.99 | 0.816 * |
| Min, max | 23.00, 61.00 | 20.00, 64.00 | 20.00, 64.00 | |
| Smoking, n (%) | ||||
| Non-smokers | 34 (94.44) | 39 (97.50) | 73 (96.05) | 0.600 ‡ |
| Former smokers | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Current smokers | 2 (5.56) | 1 (2.50) | 3 (3.95) | |
| Alcohol consumption, n (%) | ||||
| Non-drinker | 25 (69.44) | 21 (52.50) | 46 (60.53) | 0.281 ‡ |
| Former drinker | 0 (0.00) | 0 (0.00) | 0 (0.00) | |
| Current drinker | 11 (30.56) | 19 (47.50) | 30 (39.47) | |
| Height (cm) | ||||
| Mean ± SD | 158.70 ± 4.56 | 157.57 ± 5.83 | 158.11 ± 5.26 | 0.445 * |
| Min, max | 148.30, 168.90 | 144.90, 170.00 | 144.90, 170.00 | |
| Energy intake (Kcal/day) | ||||
| Mean ± SD | 1574.48 ± 498.84 | 1530 ± 406.79 | 0.353 * | |
| Energy expenditure (Kcal/day) | ||||
| Mean ± SD | 154.62 ± 150.17 | 141.32 ± 160.70 | 0.556 * |
| Treatment Group (n = 36) | Control Group (n = 40) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 Week | 12 Weeks | Change from Baseline (12 Week–0 Week) | p-Value ** | 0 Week | 12 Weeks | Change from Baseline (12 Week–0 Week) | p-Value ** | p-Value $ | |
| (12 Week) | |||||||||
| DEXA measurement | |||||||||
| Body fat percentage (%) | 39.21 ± 4.58 | 38.45 ± 4.33 | −0.76 ± 1.48 | 0.004 | 39.67 ± 3.66 | 39.66 ± 3.73 | −0.01 ± 1.33 | 0.971 | 0.014 |
| Body fat mass (g) | 25,608.97 ± 4466.42 | 24,536.19 ± 4177.00 | −1072.78 ± 1339.04 | 0.001 | 25,992.23 ± 3845.81 | 25,501.30 ± 3949.28 | -490.93 ± 1206.69 | 0.014 | 0.037 |
| Lean body mass (g) | 39,469.53 ± 3821.07 | 39,062.69 ± 3880.21 | −406.83 ± 1067.27 | 0.028 | 39,429.78 ± 4265.47 | 38,658.10 ± 4125.28 | −771.68 ± 985.55 | 0.001 | 0.120 |
| CT measurement | |||||||||
| Visceral fat area (cm2) | 123.72 ± 42.98 | 110.96 ± 45.79 | −12.76 ± 18.51 | 0.001 | 119.32 ± 40.04 | 112.38 ± 36.05 | −6.94 ± 15.51 | 0.007 | 0.162 |
| Subcutaneous fat area (cm2) | 230.36 ± 60.73 | 223.33 ± 50.88 | −7.03 ± 32.82 | 0.207 | 223.83 ± 56.75 | 225.40 ± 51.88 | 1.58 ± 32.54 | 0.761 | 0.304 |
| Total abdominal fat area (cm2) | 354.08 ± 81.86 | 334.29 ± 70.41 | −19.79 ± 41.14 | 0.006 | 343.15 ± 77.04 | 337.78 ± 67.62 | −5.37 ± 40.72 | 0.409 | 0.162 |
| Visceral- to-subcutaneous fat ratio | 0.57 ± 0.25 | 0.53 ± 0.28 | −0.04 ± 0.11 | 0.029 | 0.55 ± 0.19 | 0.52 ± 0.19 | −0.03 ± 0.09 | 0.021 | 0.817 |
| Treatment Group (n = 36) | Control Group (n = 40) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 Week | 12 Weeks | Change from Baseline (12 Week–0 Week) | p-Value ** | 0 Week | 12 Weeks | Change from Baseline (12 Week–0 Week) | p-Value ** | p-Value $ (12 Week) | |
| Anthropometric | |||||||||
| Body weight (kg) | 68.09 ± 5.99 | 66.87 ± 6.13 | −1.22 ± 2.14 | 0.001 | 68.45 ± 6.54 | 67.50 ± 6.77 | −0.94 ± 1.59 | 0.001 | 0.516 |
| Waist circumference (cm) | 91.05 ± 5.73 | 89.00 ± 5.35 | −2.05 ± 2.89 | 0.001 | 91.68 ± 6.04 | 89.70 ± 5.60 | −1.98 ± 2.22 | 0.001 | 0.752 |
| Hip circumference (cm) | 100.18 ± 4.54 | 98.79 ± 4.01 | −1.39 ± 1.94 | 0.001 | 101.59 ± 4.15 | 100.45 ± 4.27 | −1.14 ± 1.61 | 0.001 | 0.281 |
| Waist-to-hip ratio | 0.91 ± 0.04 | 0.90 ± 0.04 | −0.01 ± 0.02 | 0.046 | 0.90 ± 0.05 | 0.89 ± 0.05 | −0.01 ± 0.02 | 0.010 | 0.687 |
| BMI (kg/m2) | 27.01 ± 1.55 | 26.52 ± 1.73 | −0.49 ± 0.83 | 0.001 | 27.51 ± 1.30 | 27.12 ± 1.45 | −0.39 ± 0.64 | 0.001 | 0.537 |
| Blood chemistry | |||||||||
| Total cholesterol (mg/dL) | 205.42 ± 32.69 | 208.86 ± 30.61 | 3.44 ± 22.84 | 0.371 | 203.48 ± 33.21 | 212.63 ± 34.91 | 9.15 ± 23.58 | 0.018 | 0.302 |
| HDL-Cholesterol (mg/dL) | 56.19 ± 9.80 | 56.83 ± 11.47 | 0.64 ± 7.63 | 0.618 | 55.83 ± 13.25 | 55.43 ± 10.47 | −0.40 ± 8.32 | 0.762 | 0.492 |
| LDL-Cholesterol (mg/dL) | 125.50 ± 28.16 | 131.14 ± 26.64 | 5.64 ± 19.82 | 0.096 | 119.68 ± 30.68 | 131.35 ± 32.50 | 11.68 ± 27.37 | 0.010 | 0.421 |
| Triglyceride (mg/dL) | 118.44 ± 82.06 | 104.47 ± 51.37 | −13.97 ± 50.40 | 0.105 | 139.83 ± 101.64 | 129.08 ± 99.05 | −10.75 ± 103.16 | 0.513 | 0.357 |
| Adiponectin (μg/mL) | 8.10 ± 3.47 | 8.33 ± 2.90 | 0.23 ± 2.80 | 0.619 | 7.84 ± 3.26 | 7.89 ± 2.82 | 0.05 ± 1.61 | 0.852 | 0.527 |
| Treatment Group (n = 36) | Control Group (n = 40) | ||||||
|---|---|---|---|---|---|---|---|
| 0 Week | 12 Weeks | Change from Baseline | 0 Week | 12 Weeks | Change from Baseline | p-Value ** | |
| (12 Week–0 Week) | (12 Week–0 Week) | ||||||
| AST (IU/L) | 24.28 ± 6.53 | 23.19 ± 4.49 | −1.44 ± 6.06 | 24.62 ± 6.83 | 23.19 ± 4.91 | −1.57 ± 5.59 | 0.880 |
| ALT (IU/L) | 20.66 ± 10.46 | 17.55 ± 6.66 | −3.42 ± 8.58 | 21.82 ± 11.46 | 19.83 ± 9.49 | −2.44 ± 8.32 | 0.454 |
| Total protein (g/dL) | 7.48 ± 0.39 | 7.46 ± 0.39 | −0.01 ± 0.42 | 7.50 ± 0.39 | 7.50 ± 0.35 | 0.01 ± 0.31 | 0.566 |
| Albumin (g/dL) | 4.42 ± 0.22 | 4.40 ± 0.24 | −0.02 ± 0.25 | 4.46 ± 0.24 | 4.46 ± 0.24 | 0.00 ± 0.19 | 0.678 |
| Glucose (mg/dL) | 93.82 ± 7.90 | 90.77 ± 6.88 | −3.00 ± 9.30 | 94.21 ± 9.63 | 93.32 ± 11.84 | −1.32 ± 12.28 | 0.548 |
| Total bilirubin (mg/dL) | 0.69 ± 0.25 | 0.69 ± 0.24 | −0.01 ± 0.27 | 0.61 ± 0.23 | 0.64 ± 0.23 | 0.03 ± 0.21 | 0.445 |
| ALP (IU/L) | 62.45 ± 16.47 | 63.53 ± 16.09 | 1.14 ± 7.16 | 61.48 ± 16.70 | 61.87 ± 14.94 | 0.24 ± 6.90 | 0.499 |
| Na+ (mmol/L) | 138.43 ± 2.18 | 139.03 ± 1.83 | 0.72 ± 1.94 | 138.77 ± 1.72 | 139.10 ± 1.67 | 0.27 ± 2.14 | 0.222 |
| K+ (mmol/L) | 4.22 ± 0.37 | 4.17 ± 0.43 | −0.07 ± 0.52 | 4.28 ± 0.38 | 4.28 ± 0.49 | 0.03 ± 0.53 | 0.433 |
| Cl− (mmol/L) | 103.70 ± 1.80 | 104.23 ± 2.01 | 0.53 ± 1.98 | 103.86 ± 1.67 | 104.32 ± 1.77 | 0.41 ± 2.04 | 0.844 |
| Ca2+ (mmol/L) | 9.06 ± 0.37 | 9.15 ± 0.34 | 0.10 ± 0.45 | 9.14 ± 0.38 | 9.23 ± 0.34 | 0.09 ± 0.36 | 0.817 |
| CK (mg/dL) | 118.68 ± 163.52 | 100.30 ± 35.13 | −25.31 ± 171.08 | 109.08 ± 56.49 | 113.68 ± 48.07 | 6.05 ± 48.72 | 0.178 |
| Creatinine (mg/dL) | 0.65 ± 0.09 | 0.67 ± 0.09 | 0.02 ± 0.07 | 0.66 ± 0.10 | 0.69 ± 0.10 | 0.03 ± 0.06 | 0.435 |
| BUN (mg/dL) | 13.09 ± 3.59 | 13.59 ± 3.78 | 0.38 ± 3.36 | 13.40 ± 4.11 | 13.63 ± 4.95 | 0.19 ± 4.17 | 0.853 |
| Uric acid (mg/dL) | 4.71 ± 1.06 | 4.79 ± 1.02 | 0.06 ± 0.73 | 4.66 ± 0.91 | 4.77 ± 0.91 | 0.11 ± 0.53 | 0.598 |
| γ-GTP (IU/L) | 18.59 ± 9.60 | 16.30 ± 6.60 | −2.25 ± 5.23 | 21.40 ± 20.71 | 21.62 ± 21.52 | −0.60 ± 8.88 | 0.255 |
| Treatment Group (n = 74) | Control Group (n = 73) | Total (n = 147) | p-Value ‡ | ||||
|---|---|---|---|---|---|---|---|
| N | Incidence (%) | N | Incidence (%) | N | Incidence (%) | ||
| Mild | 31 | 100 | 31 | 100 | 62 | 100 | - |
| Moderate | 0 | 0 | 0 | 0 | 0 | 0 | |
| Severe | 0 | 0 | 0 | 0 | 0 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, E.; Lee, C.G.; Kim, J.; Kang, J.-H.; Cho, Y.G.; Jeong, S.-Y. Efficacy and Safety of Combined Extracts of Cornus officinalis and Ribes fasciculatum for Body Fat Reduction in Overweight Women. J. Clin. Med. 2020, 9, 3629. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113629
Park E, Lee CG, Kim J, Kang J-H, Cho YG, Jeong S-Y. Efficacy and Safety of Combined Extracts of Cornus officinalis and Ribes fasciculatum for Body Fat Reduction in Overweight Women. Journal of Clinical Medicine. 2020; 9(11):3629. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113629
Chicago/Turabian StylePark, Eunkuk, Chang Gun Lee, Jeonghyun Kim, Jae-Heon Kang, Young Gyu Cho, and Seon-Yong Jeong. 2020. "Efficacy and Safety of Combined Extracts of Cornus officinalis and Ribes fasciculatum for Body Fat Reduction in Overweight Women" Journal of Clinical Medicine 9, no. 11: 3629. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113629