Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Material and Methods
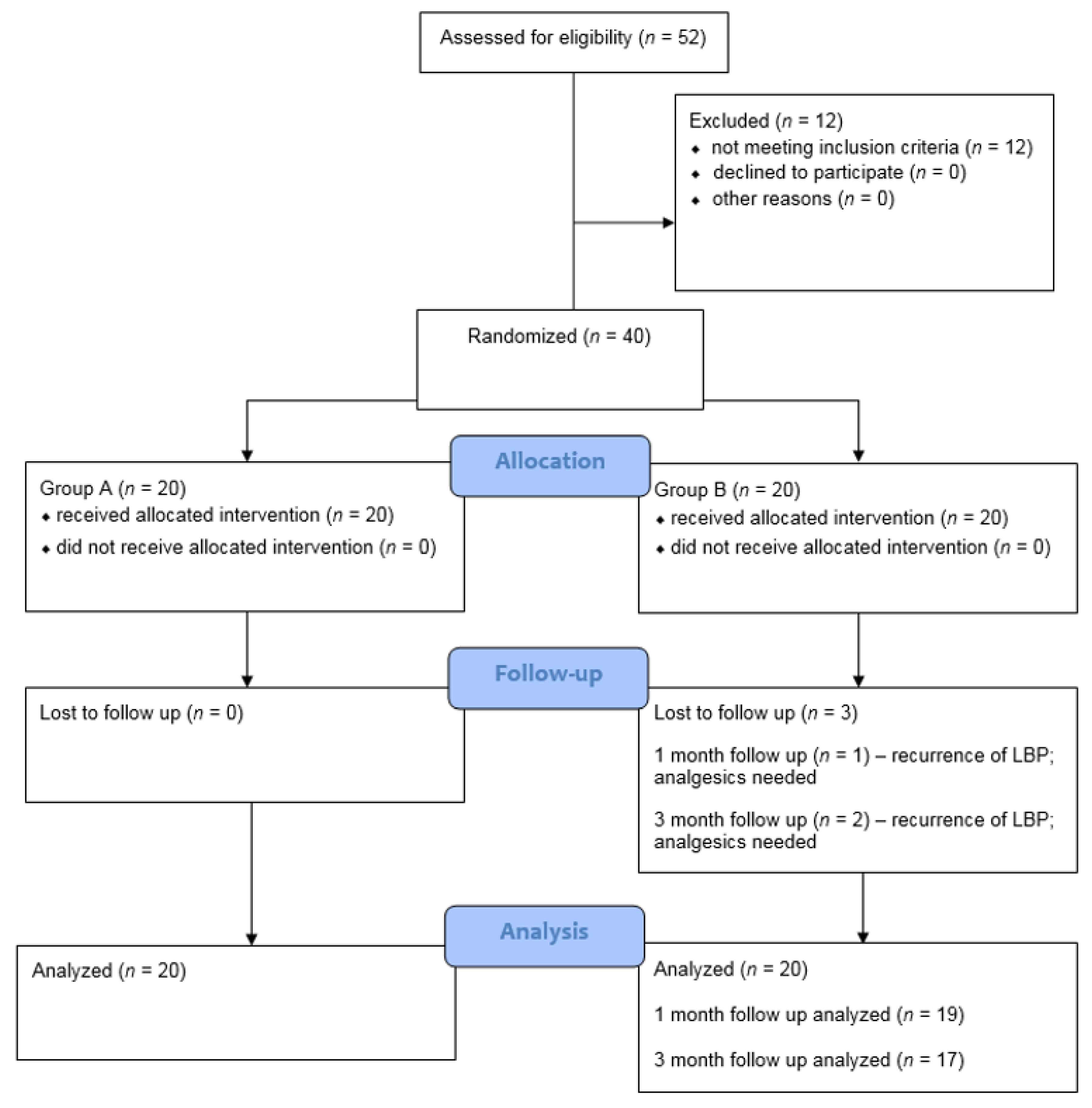
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Randomization and Blinding
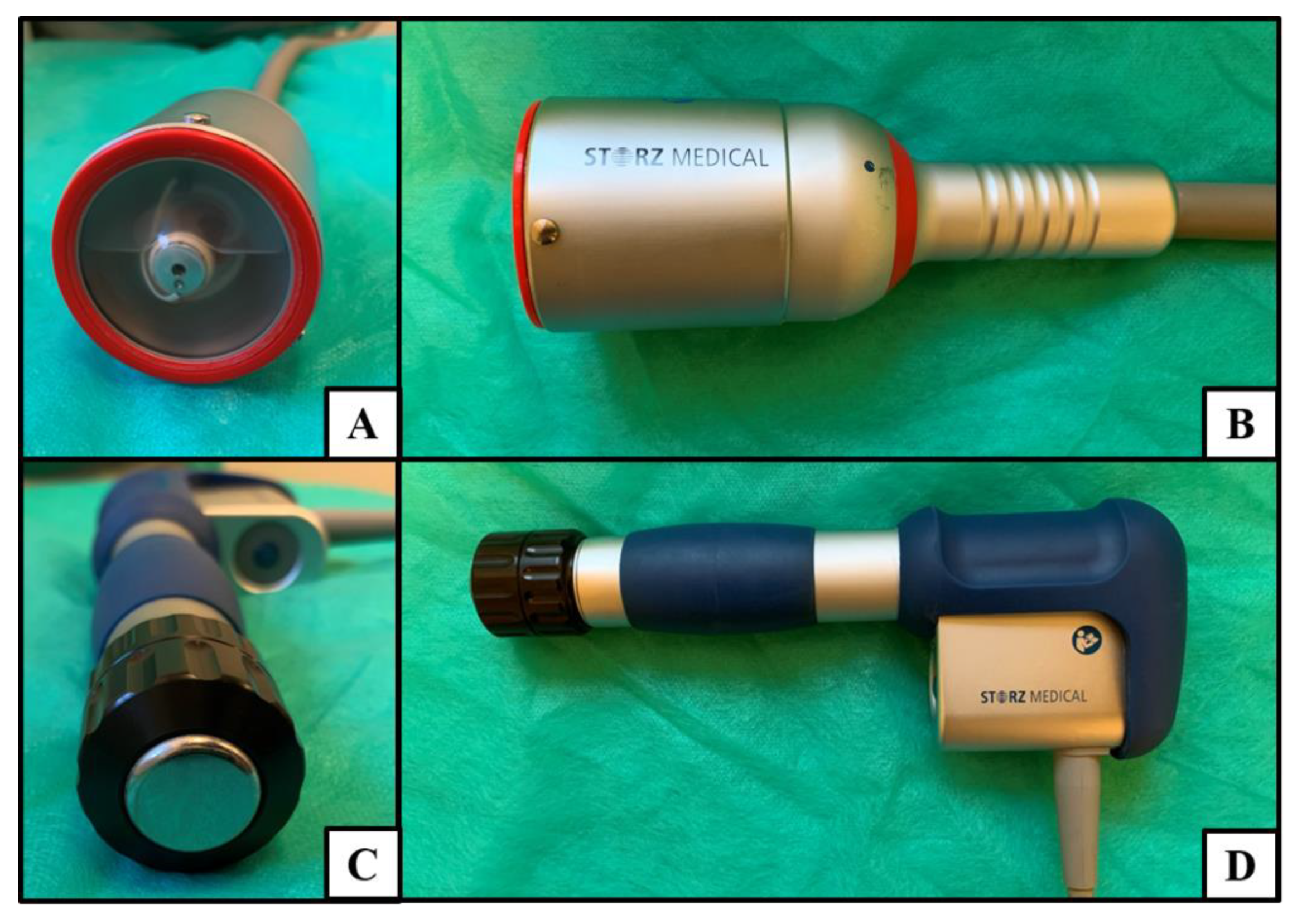
2.5. Interventions
2.6. Outcome Measurements
2.7. Statistical Analysis
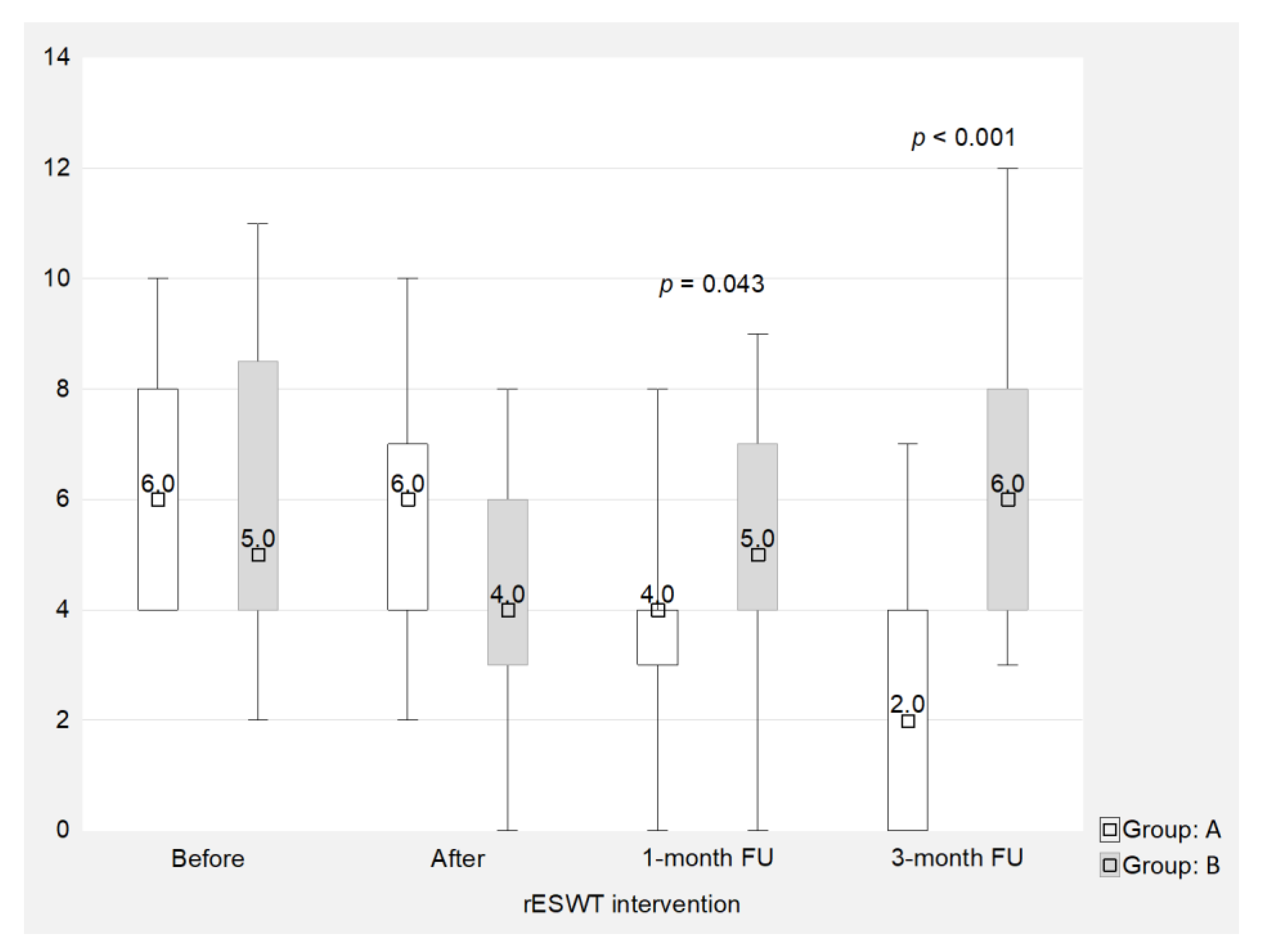
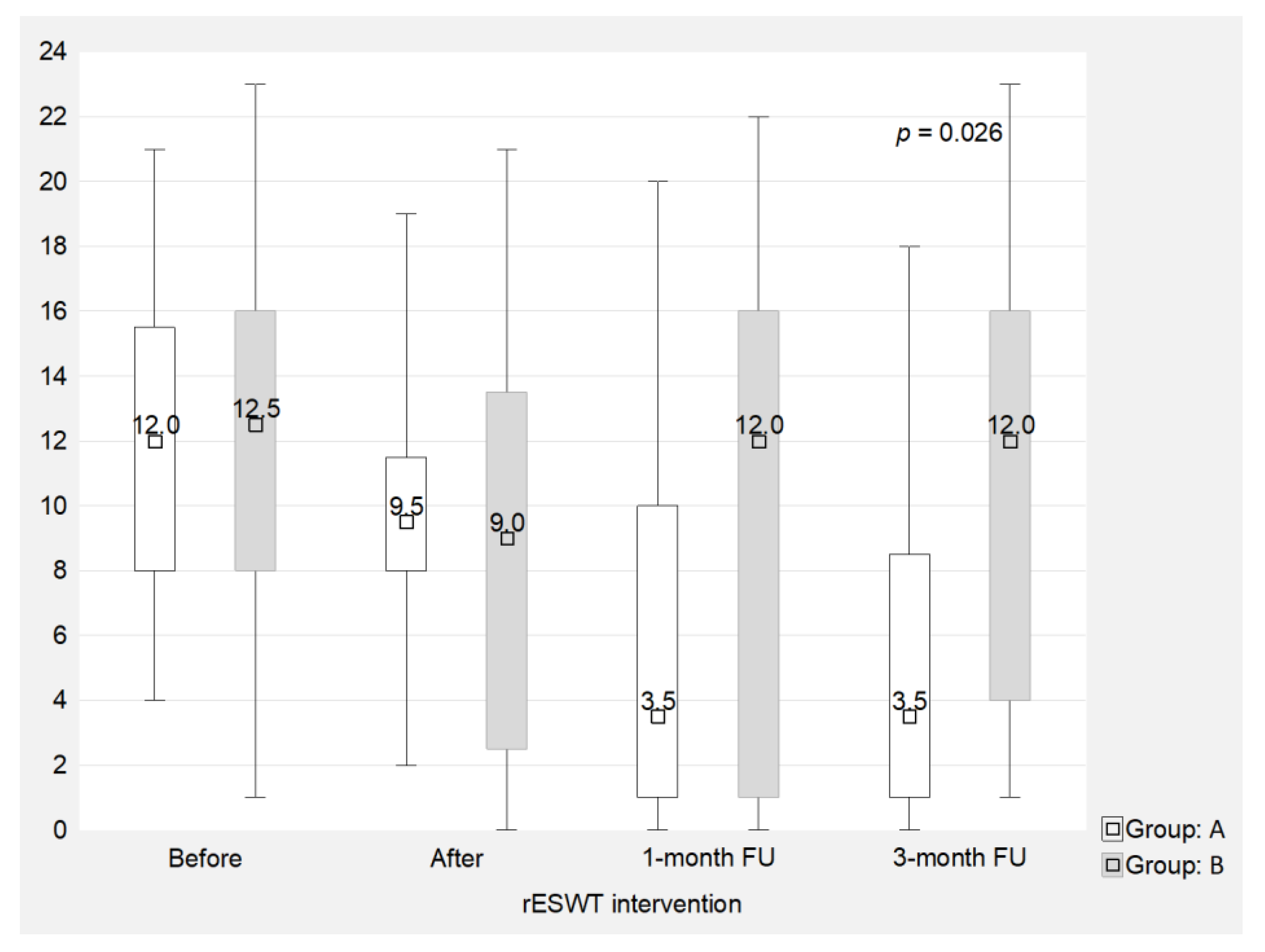
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Adogwa, O.; Davison, M.A.; Lilly, D.T.; Vuong, V.D.; Desai, S.A.; Moreno, J.; Cheng, J.; Bagley, C. A 2-year cost analysis of maximum nonoperative treatments in patients with symptomatic lumbar stenosis or spondylolisthesis that ultimately required surgery. Glob. Spine J. 2019, 9, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Buchbinder, R.; van Tulder, M.; Öberg, B.; Costa, L.M.; Woolf, A.; Schoene, M.; Croft, P. Lancet low back pain series working group low back pain: A call for action. Lancet 2018, 391, 2384–2388. [Google Scholar] [CrossRef]
- Foster, N.E.; Anema, J.R.; Cherkin, D.; Chou, R.; Cohen, S.P.; Gross, D.P.; Ferreira, P.H.; Fritz, J.M.; Koes, B.W.; Peul, W.; et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet 2018, 391, 2368–2383. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Colgrove, Y.M.; Gravino-Dunn, N.S.; Dinyer, S.C.; Sis, E.A.; Heier, A.C.; Sharma, N.K. Physical and physiological effects of yoga for an underserved population with chronic low back pain. Int. J. Yoga 2019, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Neto, M.; Lopes, J.M.; Conceição, C.S.; Araujo, A.; Brasileiro, A.; Sousa, C.; Carvalho, V.O.; Arcanjo, F.L. Stabilization exercise compared to general exercises or manual therapy for the management of low back pain: A systematic review and meta-analysis. Phys. Ther. Sport 2017, 23, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Satpute, K.; Hall, T.; Bisen, R.; Lokhande, P. The Effect of spinal mobilization with leg movement in patients with lumbar radiculopathy-a double-blind randomized controlled trial. Arch. Phys. Med. Rehabil. 2019, 100, 828–836. [Google Scholar] [CrossRef]
- Ozsoy, G.; Ilcin, N.; Ozsoy, I.; Gurpinar, B.; Buyukturan, O.; Buyukturan, B.; Kararti, C.; Sas, S. The effects of myofascial release technique combined with core stabilization exercise in elderly with non-specific low back pain: A randomized controlled, single-blind study. Clin. Interv. Aging 2019, 14, 1729–1740. [Google Scholar] [CrossRef] [Green Version]
- Rajfur, J.; Pasternok, M.; Rajfur, K.; Walewicz, K.; Fras, B.; Bolach, B.; Dymarek, R.; Rosinczuk, J.; Halski, T.; Taradaj, J. Efficacy of Selected electrical therapies on chronic low back pain: A comparative clinical pilot study. Med. Sci. Monit. 2017, 23, 85–100. [Google Scholar] [CrossRef] [Green Version]
- Taradaj, J.; Rajfur, K.; Shay, B.; Rajfur, J.; Ptaszkowski, K.; Walewicz, K.; Dymarek, R.; Sopel, M.; Rosińczuk, J. Photobiomodulation using high- or low-level laser irradiations in patients with lumbar disc degenerative changes: Disappointing outcomes and remarks. Clin. Interv. Aging 2018, 13, 1445–1455. [Google Scholar] [CrossRef] [Green Version]
- Taradaj, J.; Ozon, M.; Dymarek, R.; Bolach, B.; Walewicz, K.; Rosińczuk, J. Impact of selected magnetic fields on the therapeutic effect in patients with lumbar discopathy: A prospective, randomized, single-blinded, and placebo-controlled clinical trial. Adv. Clin. Exp. Med. 2018, 27, 649–666. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.K. Kailash, null Shock wave treatment in medicine. J. Biosci. 2005, 30, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Speed, C. A systematic review of shockwave therapies in soft tissue conditions: Focusing on the evidence. Br. J. Sports Med. 2014, 48, 1538–1542. [Google Scholar] [CrossRef] [PubMed]
- Dymarek, R.; Halski, T.; Ptaszkowski, K.; Slupska, L.; Rosinczuk, J.; Taradaj, J. Extracorporeal shock wave therapy as an adjunct wound treatment: A systematic review of the literature. Ostomy Wound Manag. 2014, 60, 26–39. [Google Scholar]
- Dolibog, P.; Franek, A.; Brzezińska-Wcisło, L.; Dolibog, P.; Wróbel, B.; Arasiewicz, H.; Chmielewska, D. Shockwave therapy in selected soft tissue diseases: A literature review. J. Wound Care 2018, 27, 573–583. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT Group CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Dymarek, R.; Bidzińska, G.; Zwierzchowski, K.; Słupska, L.; Ptaszkowski, K.; Halski, T. Evaluation of the effectiveness of extracorporeal shock wave therapy in selected musculoskeletal system disorders of the inflammatory etiology—A critical review of the literature. Wiad. Lek. 2015, 68, 183–192. [Google Scholar]
- Krukowska, J.; Wrona, J.; Sienkiewicz, M.; Czernicki, J. A comparative analysis of analgesic efficacy of ultrasound and shock wave therapy in the treatment of patients with inflammation of the attachment of the plantar fascia in the course of calcaneal spurs. Arch. Orthop. Trauma Surg. 2016, 136, 1289–1296. [Google Scholar] [CrossRef]
- Koç, M.; Bayar, B.; Bayar, K. A Comparison of back pain functional scale with roland morris disability questionnaire, oswestry disability index, and short form 36-health survey. Spine 2018, 43, 877–882. [Google Scholar] [CrossRef]
- Rezvani, A.; Ergin, O.; Karacan, I.; Oncu, M. Validity and reliability of the metric measurements in the assessment of lumbar spine motion in patients with ankylosing spondylitis. Spine 2012, 37, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Stodółka, J.; Sobera, M. Symmetry of lower limb loading in healthy adults during normal and abnormal stance. Acta Bioeng. Biomech. 2017, 19, 93–100. [Google Scholar] [PubMed]
- Truszczyńska, A.; Dobrzyńska, M.; Trzaskoma, Z.; Drzał-Grabiec, J.; Tarnowski, A. Assessment of postural stability in patients with lumbar spine chronic disc disease. Acta Bioeng. Biomech. 2016, 18, 71–77. [Google Scholar] [PubMed]
- Topalidou, A.; Tzagarakis, G.; Souvatzis, X.; Kontakis, G.; Katonis, P. Evaluation of the reliability of a new non-invasive method for assessing the functionality and mobility of the spine. Acta Bioeng. Biomech. 2014, 16, 117–124. [Google Scholar]
- Ciesielska, J.; Lisiński, P.; Bandosz, A.; Huber, J.; Kulczyk, A.; Lipiec, J. Hip strategy alterations in patients with history of low disc herniation and non-specific low back pain measured by surface electromyography and balance platform. Acta Bioeng. Biomech. 2015, 17, 103–108. [Google Scholar]
- Tomska, N.; Turoń-Skrzypińska, A.; Szylińska, A.; Rył, A.; Lubińska-Gruszka, A.; Mosiejczuk, H.; Rotter, I. Deep electromagnetic stimulation and radial shock wave therapy in back pain. Ortop. Traumatol. Rehabil. 2018, 20, 189–195. [Google Scholar] [CrossRef]
- Han, H.; Lee, D.; Lee, S.; Jeon, C.; Kim, T. The effects of extracorporeal shock wave therapy on pain, disability, and depression of chronic low back pain patients. J. Phys. Ther. Sci. 2015, 27, 397–399. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lee, D.; Park, J. Effects of extracorporeal shockwave therapy on patients with chronic low back pain and their dynamic balance ability. J. Phys. Ther. Sci. 2014, 26, 7–10. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Parameters | ||||
|---|---|---|---|---|---|
| n | SD | p-Value | |||
| Age (years) | A | 20 | 51.1 | 8.4 | 0.105 |
| B | 20 | 55.8 | 9.3 | ||
| Height (cm) | A | 20 | 165.7 | 7.8 | 0.465 |
| B | 20 | 165.0 | 7.7 | ||
| Body weight (kg) | A | 20 | 77.2 | 17.3 | 0.394 |
| B | 20 | 80.4 | 15.2 | ||
| Duration of symptoms (years) | A | 20 | 9.8 | 5.1 | 0.725 |
| B | 20 | 9.0 | 4.1 | ||
| Modic classification (o) | A | 20 | 3.1 | 0.2 | 0.797 |
| B | 20 | 3.1 | 0.3 | ||
| Sex (n/%) | A | Women n = 14 (70%) Men n = 6 (30%) | 0.723 | ||
| B | Women n = 15 (75%) Men n = 5 (25%) | ||||
| Group A | |||||
| n | SD | p-Value (Main Effect) * | p-Value (Multiple Comparisons) ** | ||
| Before | 20 | 236 | 52.52 | p = 0.024 | Before: After p = 0.257 Before: 1-month FU p = 0.008 Before: 3-month FU p = 0.003 After: 1-month FU p = 0.041 After: 3-month FU p = 0.032 1-month: 3-month p = 0.837 |
| After | 20 | 224 | 44.28 | ||
| 1-month FU | 20 | 199 | 32 | ||
| 3-month FU | 20 | 195 | 34.24 | ||
| Group B | |||||
| n | SD | p-Value (Main Effect) * | p-Value (Multiple Comparisons) ** | ||
| Before | 20 | 232 | 62.22 | p = 0.334 | Before: After p = 0.512 Before: 1-month FU p = 0.839 Before: 3-month FU p = 0.897 After: 1-month FU p = 0.730 After: 3-month FU p = 0.722 1-month FU: 3-month FU p = 0.925 |
| After | 20 | 223 | 57.22 | ||
| 1-month FU | 19 | 233 | 60 | ||
| 3-month FU | 17 | 234 | 64.76 | ||
| Group A | |||||
| n | SD | p-Value (Main Effect) * | p-Value (Multiple Comparisons) ** | ||
| Before | 20 | 318 | 57.95 | p = 0.041 | Before: After p = 0.310 Before: 1-month FU p = 0.018 Before: 3-month FU p = 0.026 After: 1-month FU p = 0.048 After: 3-month FU p = 0.079 1-month FU: 3-month FU p = 0.637 |
| After | 20 | 312 | 56.44 | ||
| 1-month FU | 20 | 302 | 58.45 | ||
| 3-month FU | 20 | 309 | 50.24 | ||
| Group B | |||||
| n | SD | p-Value (Main Effect) * | p-Value (Multiple Comparisons) ** | ||
| Before | 20 | 320 | 73.10 | p = 0.424 | Before: After p = 0.312 Before: 1-month FU p = 0.479 Before: 3-month FU p = 0.510 After: 1-month FU p = 0.880 After: 3-month FU p = 0.712 1-month FU: 3-month FU p = 0.725 |
| After | 20 | 315 | 65.50 | ||
| 1-month FU | 19 | 316 | 66.24 | ||
| 3-month FU | 17 | 319 | 70.76 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walewicz, K.; Taradaj, J.; Dobrzyński, M.; Sopel, M.; Kowal, M.; Ptaszkowski, K.; Dymarek, R. Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial. J. Clin. Med. 2020, 9, 568. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9020568
Walewicz K, Taradaj J, Dobrzyński M, Sopel M, Kowal M, Ptaszkowski K, Dymarek R. Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial. Journal of Clinical Medicine. 2020; 9(2):568. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9020568
Chicago/Turabian StyleWalewicz, Karolina, Jakub Taradaj, Maciej Dobrzyński, Mirosław Sopel, Mateusz Kowal, Kuba Ptaszkowski, and Robert Dymarek. 2020. "Effect of Radial Extracorporeal Shock Wave Therapy on Pain Intensity, Functional Efficiency, and Postural Control Parameters in Patients with Chronic Low Back Pain: A Randomized Clinical Trial" Journal of Clinical Medicine 9, no. 2: 568. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9020568