AMIC—Autologous Matrix-Induced Chondrogenesis Technique in Patellar Cartilage Defects Treatment: A Retrospective Study with a Mid-Term Follow-Up

 , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Patient Selection
2.2. Data Collection and Ethical Approval
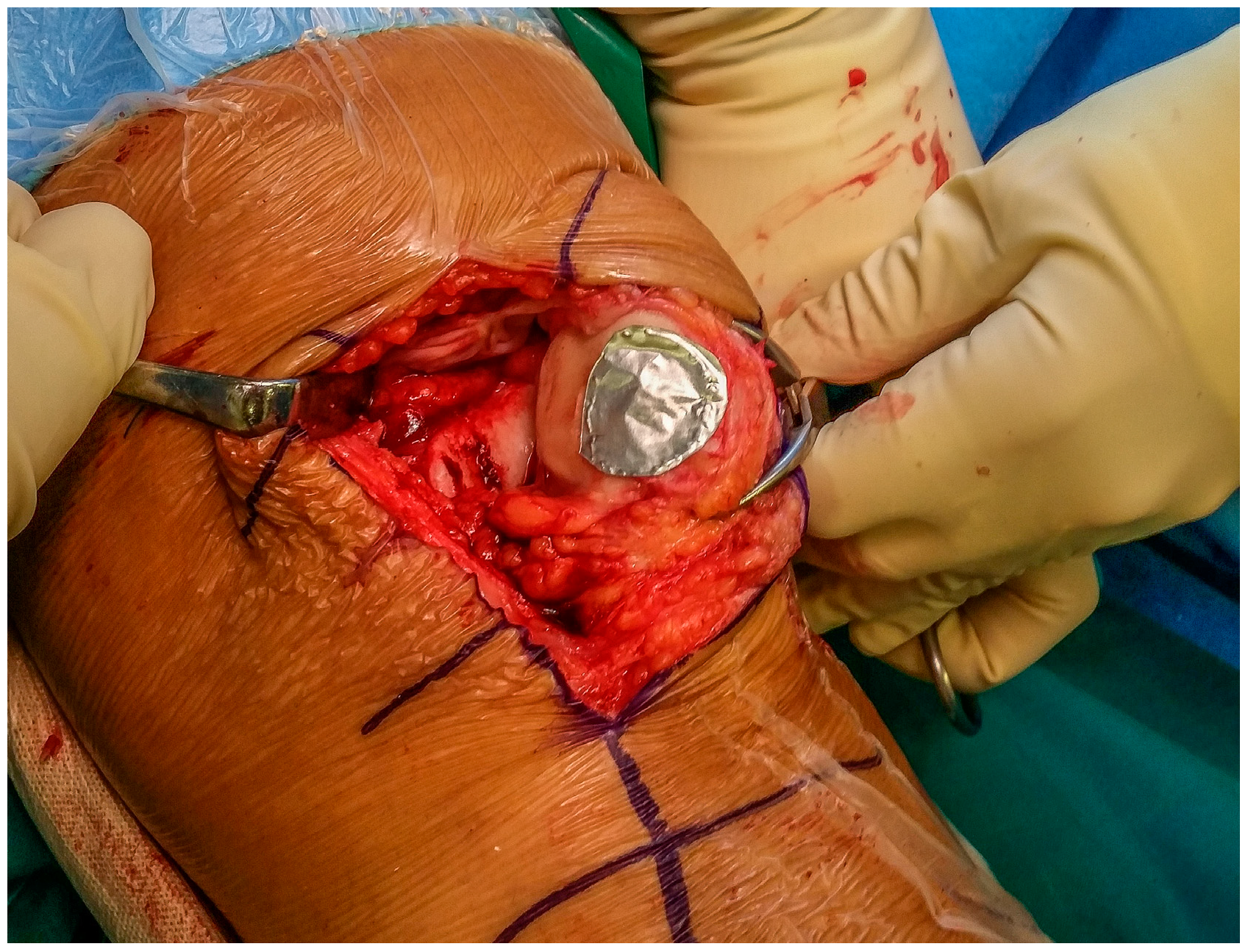
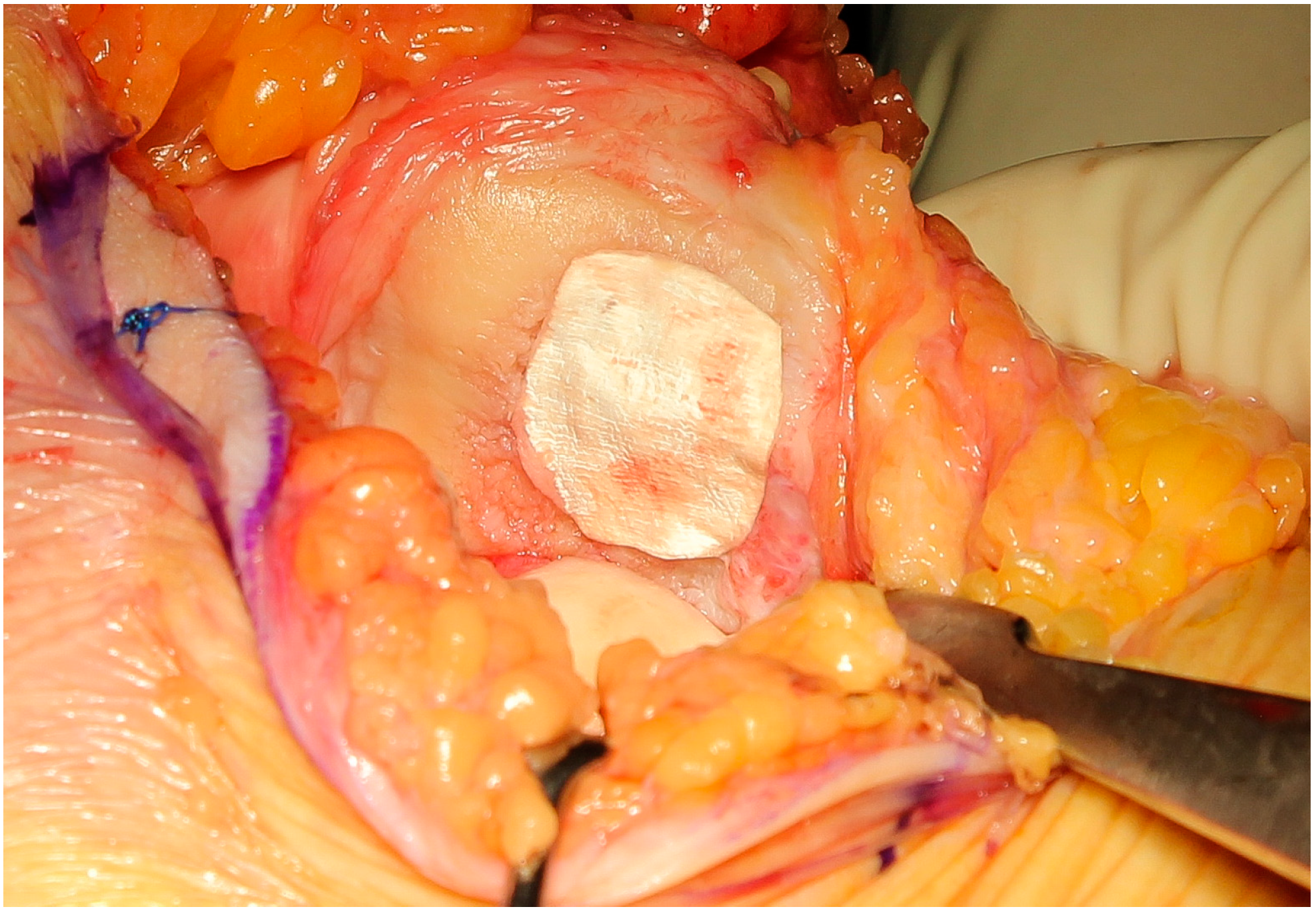
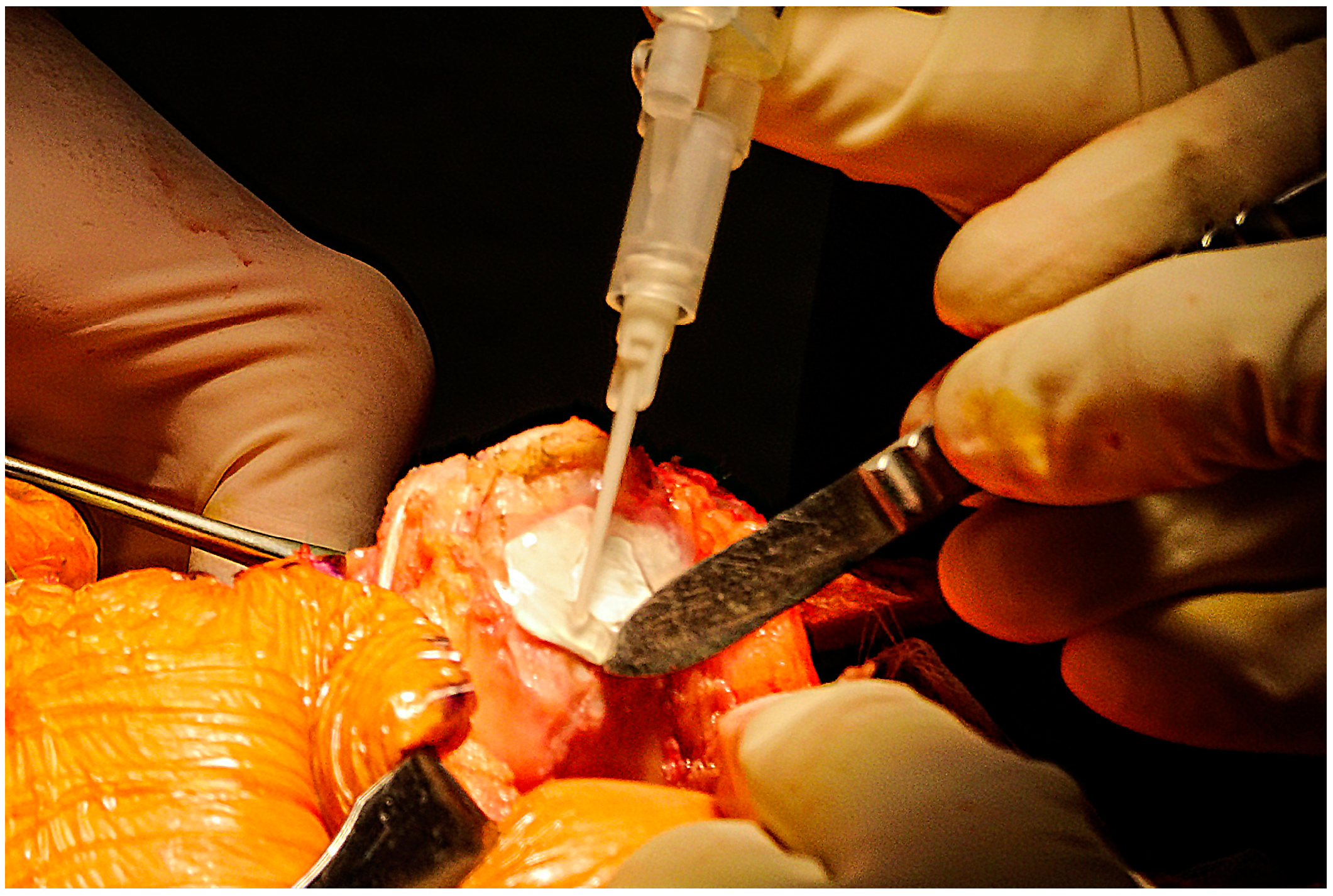
2.3. AMIC: Patient Evaluation, Indications, and Surgical Technique
2.4. Postoperative Management and Rehabilitation Protocol
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dhollander, A.; Moens, K.; Van der Maas, J.; Verdonk, P.; Almqvist, K.F.; Victor, J. Treatment of patellofemoral cartilage defects in the knee by autologous matrix-induced chondrogenesis (AMIC). Acta Orthop. Belg. 2014, 80, 251–259. [Google Scholar] [PubMed]
- Widuchowski, W.; Lukasik, P.; Kwiatkowski, G.; Faltus, R.; Szyluk, K.; Widuchowski, J.; Koczy, B. Isolated full thickness chondral injuries. Prevalance and outcome of treatment. A retrospective study of 5233 knee arthroscopies. Acta Chir. Orthop. Traumatol. Cechoslov. 2008, 75, 382–386. [Google Scholar]
- Flanigan, D.C.; Harris, J.D.; Trinh, T.Q.; Siston, R.A.; Brophy, R.H. Prevalence of chondral defects in athletes’ knees: A systematic review. Med. Sci. Sports Exerc. 2010, 42, 1795–1801. [Google Scholar] [CrossRef] [PubMed]
- Niemeyer, P.; Steinwachs, M.; Erggelet, C.; Kreuz, P.C.; Kraft, N.; Kostler, W.; Mehlhorn, A.; Sudkamp, N.P. Autologous chondrocyte implantation for the treatment of retropatellar cartilage defects: Clinical results referred to defect localisation. Arch. Orthop. Trauma Surg. 2008, 128, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Garrido, C.; Slabaugh, M.A.; L’Heureux, D.R.; Friel, N.A.; Cole, B.J. Recommendations and treatment outcomes for patellofemoral articular cartilage defects with autologous chondrocyte implantation: Prospective evaluation at average 4-year follow-up. Am. J. Sports Med. 2009, 37, 33S–41S. [Google Scholar] [CrossRef]
- van Jonbergen, H.P.; Poolman, R.W.; van Kampen, A. Isolated patellofemoral osteoarthritis. Acta Orthop. 2010, 81, 199–205. [Google Scholar] [CrossRef]
- Mouzopoulos, G.; Borbon, C.; Siebold, R. Patellar chondral defects: A review of a challenging entity. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1990–2001. [Google Scholar] [CrossRef]
- Kreuz, P.C.; Steinwachs, M.R.; Erggelet, C.; Krause, S.J.; Konrad, G.; Uhl, M.; Sudkamp, N. Results after microfracture of full-thickness chondral defects in different compartments in the knee. Osteoarthritis Cartil. 2006, 14, 1119–1125. [Google Scholar] [CrossRef] [Green Version]
- De Luca, P.; Kouroupis, D.; Vigano, M.; Perucca-Orfei, C.; Kaplan, L.; Zagra, L.; de Girolamo, L.; Correa, D.; Colombini, A. Human diseased articular cartilage contains a mesenchymal stem cell-like population of chondroprogenitors with strong immunomodulatory responses. J. Clin. Med. 2019, 8, 423. [Google Scholar] [CrossRef] [Green Version]
- Mithoefer, K.; McAdams, T.; Williams, R.J.; Kreuz, P.C.; Mandelbaum, B.R. Clinical efficacy of the microfracture technique for articular cartilage repair in the knee: An evidence-based systematic analysis. Am. J. Sports Med. 2009, 37, 2053–2063. [Google Scholar] [CrossRef]
- Marmotti, A.; de Girolamo, L.; Bonasia, D.E.; Bruzzone, M.; Mattia, S.; Rossi, R.; Montaruli, A.; Dettoni, F.; Castoldi, F.; Peretti, G.; et al. Bone marrow derived stem cells in joint and bone diseases: A concise review. Int. Orthop. 2014, 38, 1787–1801. [Google Scholar] [CrossRef] [PubMed]
- Ambra, L.F.; de Girolamo, L.; Mosier, B.; Gomoll, A.H. Review: Interventions for cartilage disease: Current state-of-the-art and emerging technologies. Arthritis Rheumatol. 2017, 69, 1363–1373. [Google Scholar] [CrossRef]
- Dhollander, A.A.; De Neve, F.; Almqvist, K.F.; Verdonk, R.; Lambrecht, S.; Elewaut, D.; Verbruggen, G.; Verdonk, P.C. Autologous matrix-induced chondrogenesis combined with platelet-rich plasma gel: Technical description and a five pilot patients report. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 536–542. [Google Scholar] [CrossRef] [PubMed]
- de Girolamo, L.; Schonhuber, H.; Vigano, M.; Bait, C.; Quaglia, A.; Thiebat, G.; Volpi, P. Autologous matrix-induced chondrogenesis (amic) and amic enhanced by autologous concentrated bone marrow aspirate (bmac) allow for stable clinical and functional improvements at up to 9 years follow-up: Results from a randomized controlled study. J. Clin. Med. 2019, 8, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, M.; Zech, S. Matrix-associated stem cell transplantation (MAST) in chondral defects of foot and ankle is effective. Foot Ankle Surg. 2013, 19, 84–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brittberg, M.; Peterson, L. Introduction to an Articular Cartilage Classification; ICRS Newsletter: Zurich, Switzerland, 1998; pp. 5–8. [Google Scholar]
- Benthien, J.P.; Behrens, P. Autologous matrix-induced chondrogenesis (amic): Combining microfracturing and a collagen i/iii matrix for articular cartilage resurfacing. Cartilage 2010, 1, 65–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertho, P.; Pauvert, A.; Pouderoux, T.; Robert, H. Traumatology Society of Western, F. Treatment of large deep osteochondritis lesions of the knee by autologous matrix-induced chondrogenesis (AMIC): Preliminary results in 13 patients. Orthop. Traumatol. Surg. Res. 2018, 104, 695–700. [Google Scholar] [CrossRef]
- Fontana, A.; de Girolamo, L. Sustained five-year benefit of autologous matrix-induced chondrogenesis for femoral acetabular impingement-induced chondral lesions compared with microfracture treatment. Bone Jt. J. 2015, 97-B, 628–635. [Google Scholar] [CrossRef]
- Gille, J.; Behrens, P.; Volpi, P.; de Girolamo, L.; Reiss, E.; Zoch, W.; Anders, S. Outcome of autologous matrix induced chondrogenesis (AMIC) in cartilage knee surgery: Data of the AMIC Registry. Arch. Orthop. Trauma Surg. 2013, 133, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Gille, J.; Schuseil, E.; Wimmer, J.; Gellissen, J.; Schulz, A.P.; Behrens, P. Mid-term results of Autologous Matrix-Induced Chondrogenesis for treatment of focal cartilage defects in the knee. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 1456–1464. [Google Scholar] [CrossRef]
- Schiavone Panni, A.; Del Regno, C.; Mazzitelli, G.; D’Apolito, R.; Corona, K.; Vasso, M. Good clinical results with autologous matrix-induced chondrogenesis (Amic) technique in large knee chondral defects. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Usuelli, F.G.; Grassi, M.; Manzi, L.; Guarrella, V.; Boga, M.; Girolamo, L. Treatment of osteochondral lesions of the talus with autologous collagen-induced chondrogenesis: Clinical and magnetic resonance evaluation at one-year follow-up. Joints 2016, 4, 80–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volz, M.; Schaumburger, J.; Frick, H.; Grifka, J.; Anders, S. A randomized controlled trial demonstrating sustained benefit of Autologous Matrix-Induced Chondrogenesis over microfracture at five years. Int. Orthop. 2017, 41, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinwachs, M.R.; Gille, J.; Volz, M.; Anders, S.; Jakob, R.; De Girolamo, L.; Volpi, P.; Schiavone-Panni, A.; Scheffler, S.; Reiss, E.; et al. Systematic review and meta-analysis of the clinical evidence on the use of autologous matrix-induced chondrogenesis in the knee. Cartilage 2019. [Google Scholar] [CrossRef] [Green Version]
- Astur, D.C.; Lopes, J.C.; Santos, M.A.; Kaleka, C.C.; Amaro, J.T.; Cohen, M. Surgical treatment of chondral knee defects using a collagen membrane—Autologus matrix-induced chondrogenesis. Rev. Bras. Ortop. 2018, 53, 733–739. [Google Scholar] [CrossRef]
- Kusano, T.; Jakob, R.P.; Gautier, E.; Magnussen, R.A.; Hoogewoud, H.; Jacobi, M. Treatment of isolated chondral and osteochondral defects in the knee by autologous matrix-induced chondrogenesis (AMIC). Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2109–2115. [Google Scholar] [CrossRef]
- Iwano, T.; Kurosawa, H.; Tokuyama, H.; Hoshikawa, Y. Roentgenographic and clinical findings of patellofemoral osteoarthrosis. With special reference to its relationship to femorotibial osteoarthrosis and etiologic factors. Clin. Orthop. Relat. Res. 1990, 252, 190–197. [Google Scholar]
- Walch, G.; Dejour, H. Radiology in femoro-patellar pathology. Acta Orthop. Belg. 1989, 55, 371–380. [Google Scholar]
- Hefti, F.; Muller, W.; Jakob, R.P.; Staubli, H.U. Evaluation of knee ligament injuries with the IKDC form. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 226–234. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual analog scale for pain (VAS pain), numeric rating scale for pain (NRS pain), mcgill pain questionnaire (MPQ), short-form mcgill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form-36 bodily pain scale (SF-36 BPS), and measure of intermittent and constant osteoarthritis pain (ICOAP). Arthritis Care Res. Hoboken 2011, 63, S240–S252. [Google Scholar]
- Cerciello, S.; Corona, K.; Morris, B.J.; Visona, E.; Maccauro, G.; Maffulli, N.; Ronga, M. Cross-cultural adaptation and validation of the Italian versions of the Kujala, Larsen, Lysholm and Fulkerson scores in patients with patellofemoral disorders. J. Orthop. Traumatol. 2018, 19, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tegner, Y.; Lysholm, J. Rating systems in the evaluation of knee ligament injuries. Clin. Orthop. Relat. Res. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- Crosby, E.B.; Insall, J. Recurrent dislocation of the patella. Relation of treatment to osteoarthritis. J. Bone Jt. Surg. Am. 1976, 58, 9–13. [Google Scholar] [CrossRef]
- Beighton, P.; Solomon, L.; Soskolne, C.L. Articular mobility in an African population. Ann. Rheum. Dis. 1973, 32, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Dejour, H.; Walch, G.; Nove-Josserand, L.; Guier, C. Factors of patellar instability: An anatomic radiographic study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef]
- Sadlik, B.; Puszkarz, M.; Kosmalska, L.; Wiewiorski, M. All–Arthroscopic autologous matrix-induced chondrogenesis-aided repair of a patellar cartilage defect using dry arthroscopy and a retraction system. J. Knee Surg. 2017, 30, 925–929. [Google Scholar]
- Norland, R.; Muchnick, M.; Harmon, Z.; Chin, T.; Kakar, R.S. Opportunities for regenerative rehabilitation and advanced technologies in physical therapy: Perspective from academia. Phys. Ther. 2016, 96, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Thompson, W.R.; Scott, A.; Loghmani, M.T.; Ward, S.R.; Warden, S.J. Understanding mechanobiology: Physical therapists as a force in mechanotherapy and musculoskeletal regenerative rehabilitation. Phys. Ther. 2016, 96, 560–569. [Google Scholar] [CrossRef]
- Khan, K.M.; Scott, A. Mechanotherapy: How physical therapists’ prescription of exercise promotes tissue repair. Br. J. Sports Med. 2009, 43, 247–252. [Google Scholar] [CrossRef]
- Huang, C.; Holfeld, J.; Schaden, W.; Orgill, D.; Ogawa, R. Mechanotherapy: Revisiting physical therapy and recruiting mechanobiology for a new era in medicine. Trends Mol. Med. 2013, 19, 555–564. [Google Scholar] [CrossRef]
- Dunn, S.L.; Olmedo, M.L. Mechanotransduction: Relevance to physical therapist practice-understanding our ability to affect genetic expression through mechanical forces. Phys. Ther. 2016, 96, 712–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingber, D.E. Cellular mechanotransduction: Putting all the pieces together again. FASEB J. 2006, 20, 811–827. [Google Scholar] [CrossRef] [PubMed]
- Matthews, B.D.; Overby, D.R.; Mannix, R.; Ingber, D.E. Cellular adaptation to mechanical stress: Role of integrins, Rho, cytoskeletal tension and mechanosensitive ion channels. J. Cell Sci. 2006, 119, 508–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, M.A. Integrins and extracellular matrix in mechanotransduction. Cold Spring Harb. Perspect. Biol. 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Schatti, O.; Grad, S.; Goldhahn, J.; Salzmann, G.; Li, Z.; Alini, M.; Stoddart, M.J. A combination of shear and dynamic compression leads to mechanically induced chondrogenesis of human mesenchymal stem cells. Eur. Cell Mater. 2011, 22, 214–225. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F. Knee biomechanics of the dynamic squat exercise. Med. Sci. Sports Exerc. 2001, 33, 127–141. [Google Scholar] [CrossRef]
- Kreuz, P.C.; Steinwachs, M.; Erggelet, C.; Lahm, A.; Krause, S.; Ossendorf, C.; Meier, D.; Ghanem, N.; Uhl, M. Importance of sports in cartilage regeneration after autologous chondrocyte implantation: A prospective study with a 3-year follow-up. Am. J. Sports Med. 2007, 35, 1261–1268. [Google Scholar] [CrossRef]
- Gobbi, A.; Karnatzikos, G.; Sankineani, S.R. One-step surgery with multipotent stem cells for the treatment of large full-thickness chondral defects of the knee. Am. J. Sports Med. 2014, 42, 648–657. [Google Scholar] [CrossRef]
- Buda, R.; Vannini, F.; Cavallo, M.; Baldassarri, M.; Luciani, D.; Mazzotti, A.; Pungetti, C.; Olivieri, A.; Giannini, S. One-step arthroscopic technique for the treatment of osteochondral lesions of the knee with bone-marrow-derived cells: Three years results. Musculoskelet Surg. 2013, 97, 145–151. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tradati, D.; De Luca, P.; Maione, A.; Uboldi, F.M.; Volpi, P.; de Girolamo, L.; Berruto, M. AMIC—Autologous Matrix-Induced Chondrogenesis Technique in Patellar Cartilage Defects Treatment: A Retrospective Study with a Mid-Term Follow-Up. J. Clin. Med. 2020, 9, 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041184
Tradati D, De Luca P, Maione A, Uboldi FM, Volpi P, de Girolamo L, Berruto M. AMIC—Autologous Matrix-Induced Chondrogenesis Technique in Patellar Cartilage Defects Treatment: A Retrospective Study with a Mid-Term Follow-Up. Journal of Clinical Medicine. 2020; 9(4):1184. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041184
Chicago/Turabian StyleTradati, Daniele, Paola De Luca, Alessio Maione, Francesco Mattia Uboldi, Piero Volpi, Laura de Girolamo, and Massimo Berruto. 2020. "AMIC—Autologous Matrix-Induced Chondrogenesis Technique in Patellar Cartilage Defects Treatment: A Retrospective Study with a Mid-Term Follow-Up" Journal of Clinical Medicine 9, no. 4: 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041184