Herbal Medicine for the Treatment of Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of Randomized Controlled Trials



Abstract
:1. Introduction
2. Methods
2.1. Study Registration
2.2. Search Strategy
- English databases: PubMed, Embase, Allied and Complementary Medicine Database (AMED) and Cochrane Register of Controlled Trials (CENTRAL).
- Chinese databases: Chinese National Knowledge Infrastructure Database (CNKI), Chinese Science and Technique Journals Database (VIP), Chinese Biomedical Literature Database (CBM) and the Wanfang Database.
- Korean databases: Korean Association of Medical Journal database (KoreaMed), Korean Medical database (KMBase), Research Information Service System (RISS), and OASIS database.
2.3. Eligibility Criteria
2.3.1. Types of Studies
2.3.2. Participants
2.3.3. Intervention Groups
2.3.4. Comparison Groups
2.3.5. Outcome Measures
2.4. Study Selection and Data Extraction
2.5. Assessment of Risk of Bias
2.6. Data Analysis
3. Results
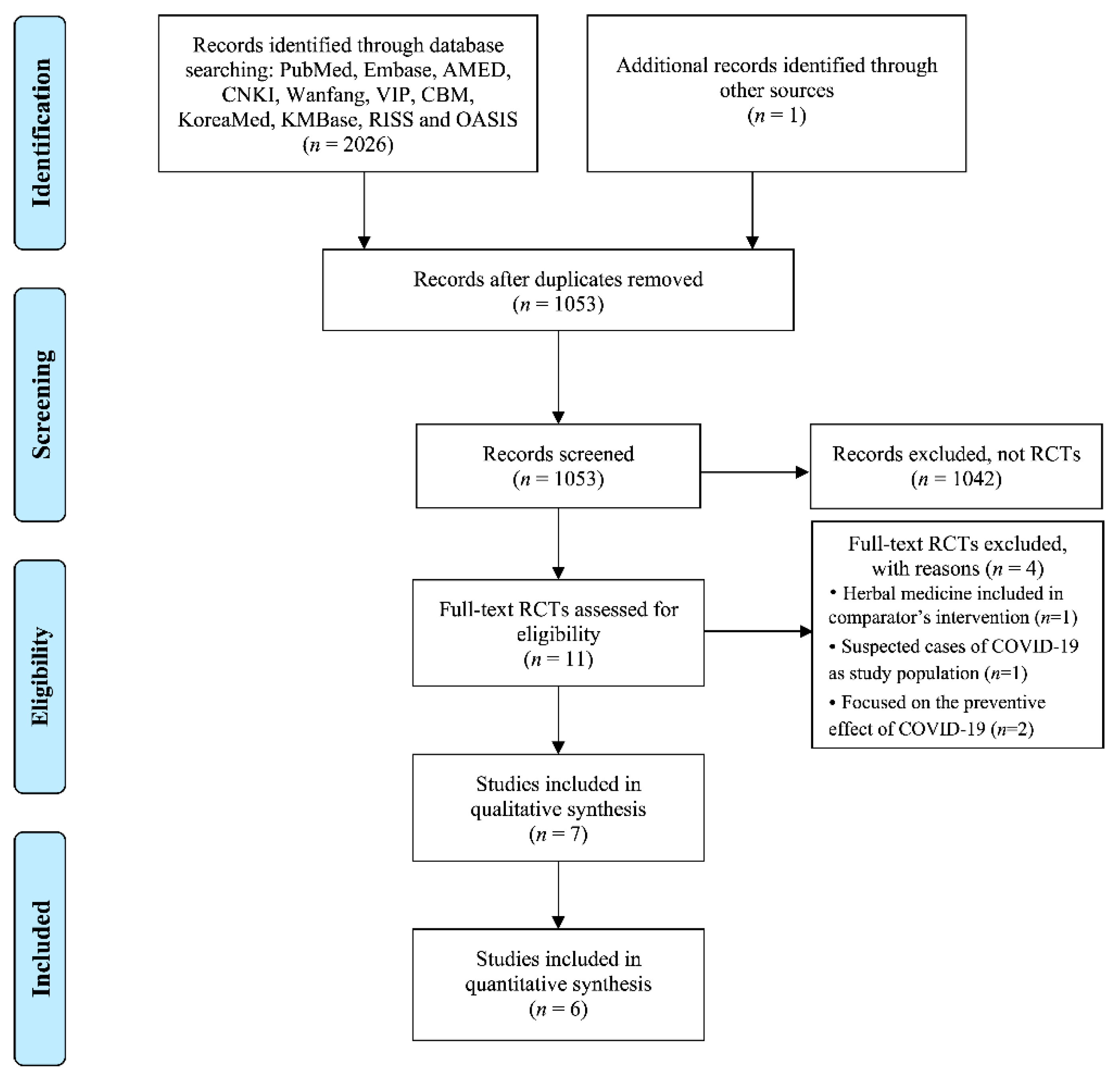
3.1. Literature Search
3.2. Study Characteristics
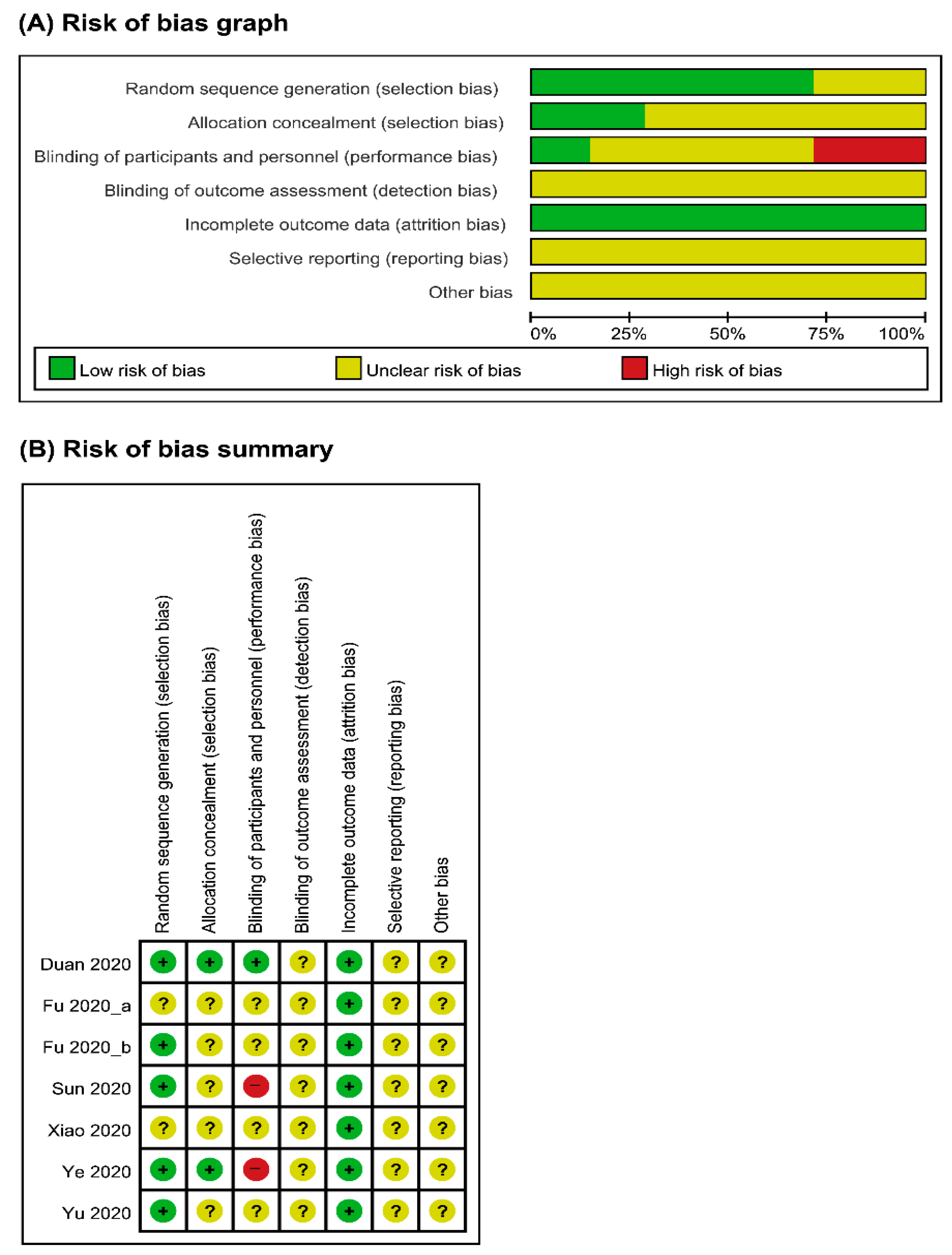
3.3. Risk of Bias Assessment
3.4. Effect of Intervention on Primary Outcomes
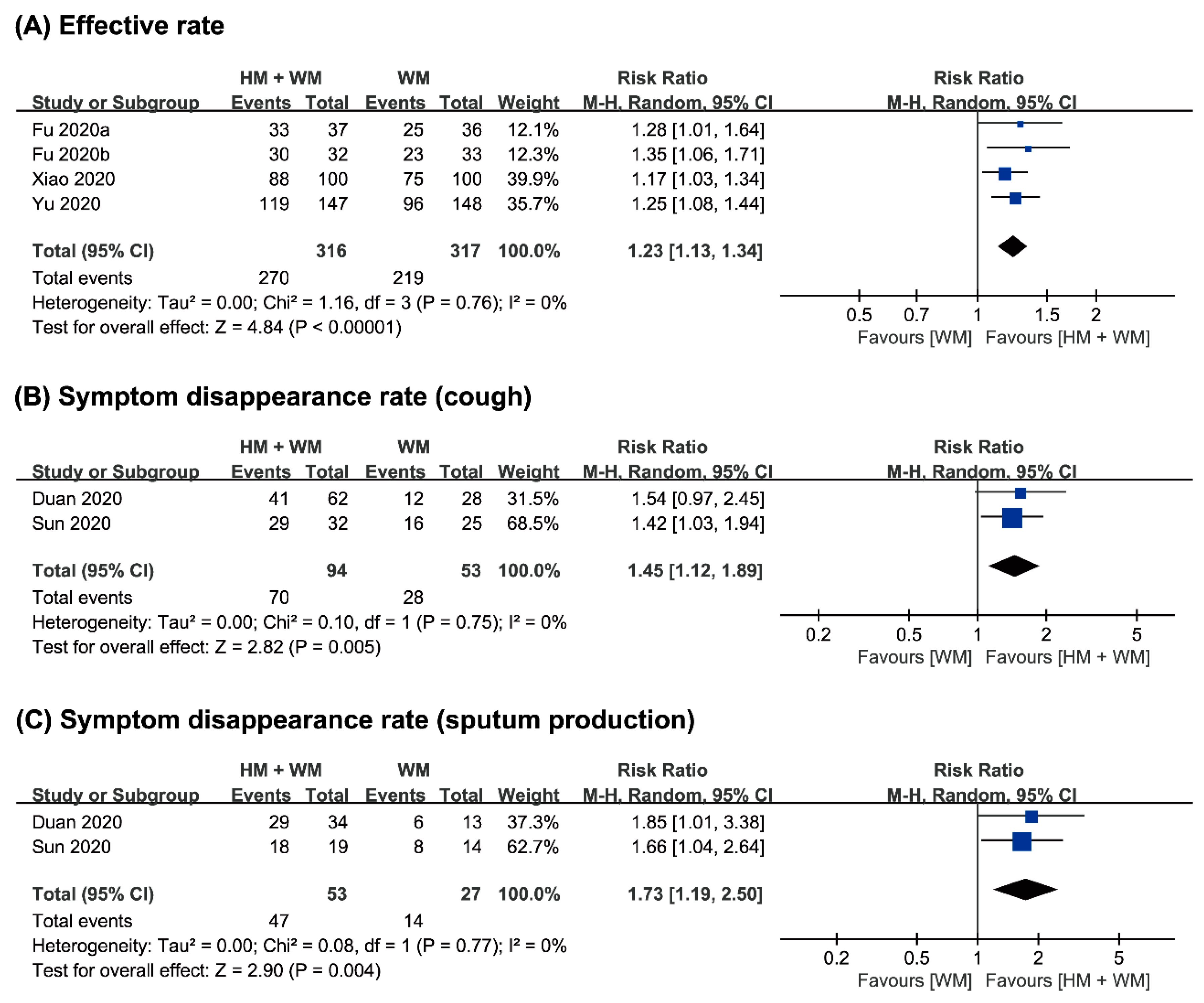
3.4.1. Primary Outcomes
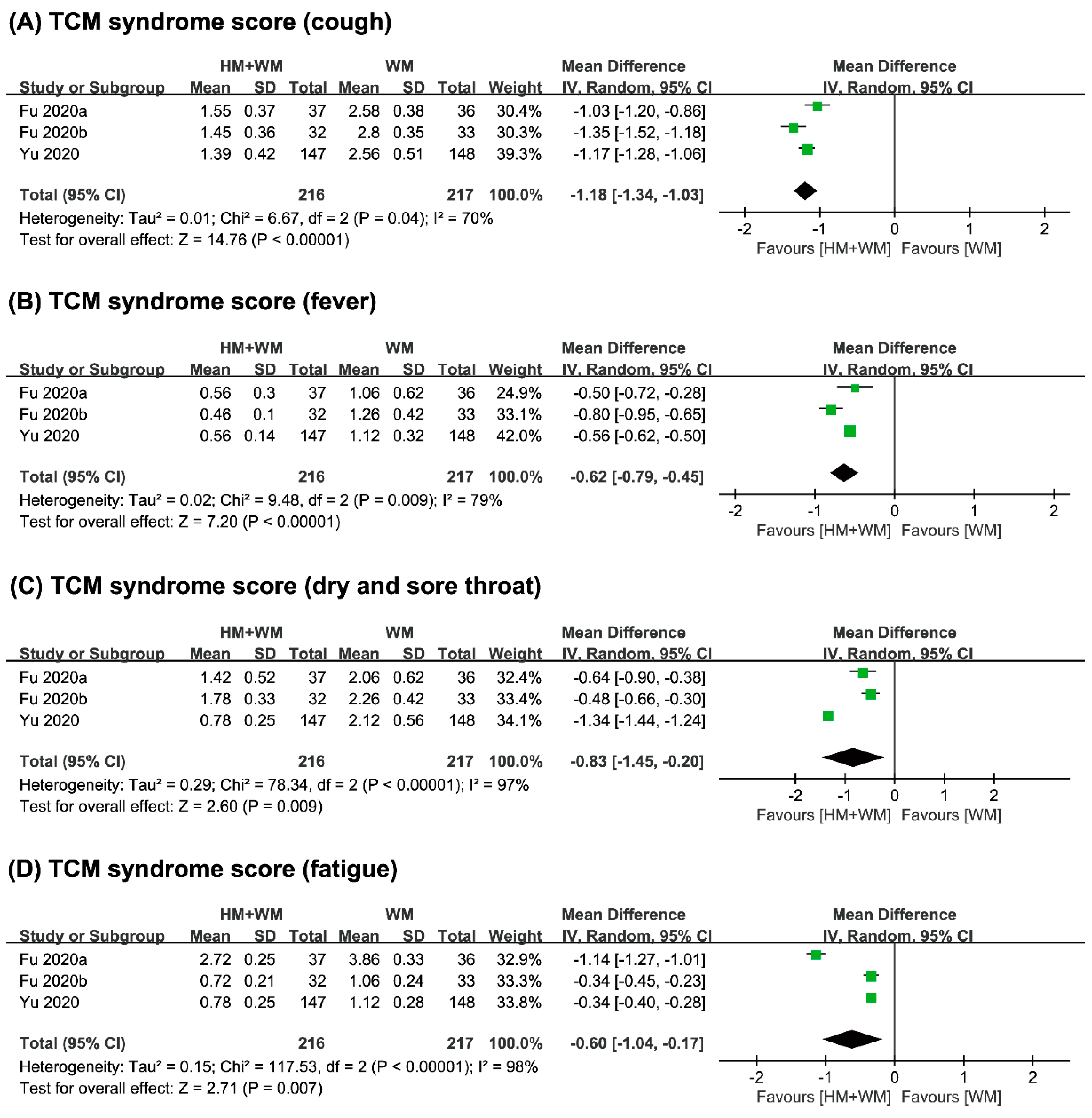
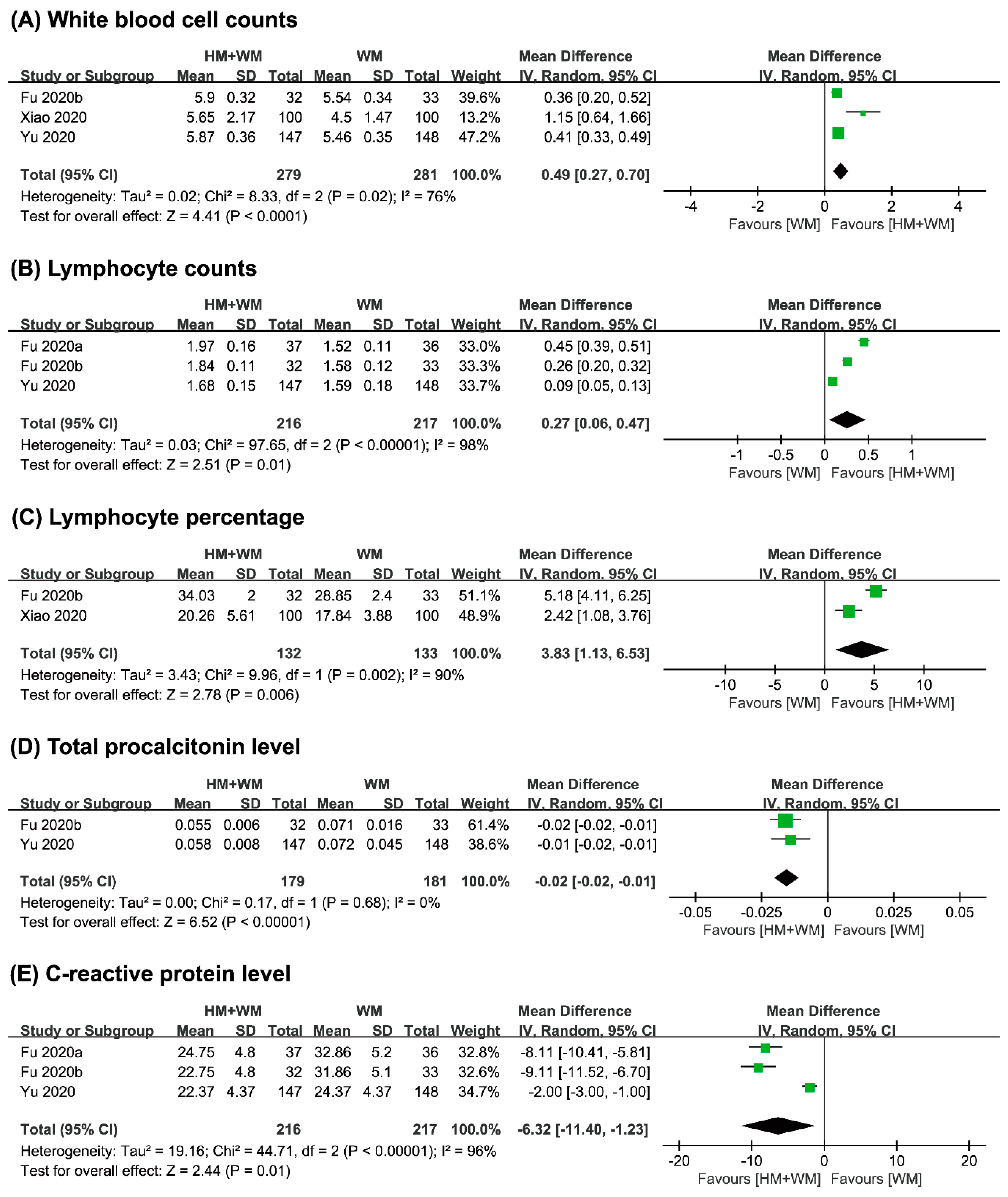
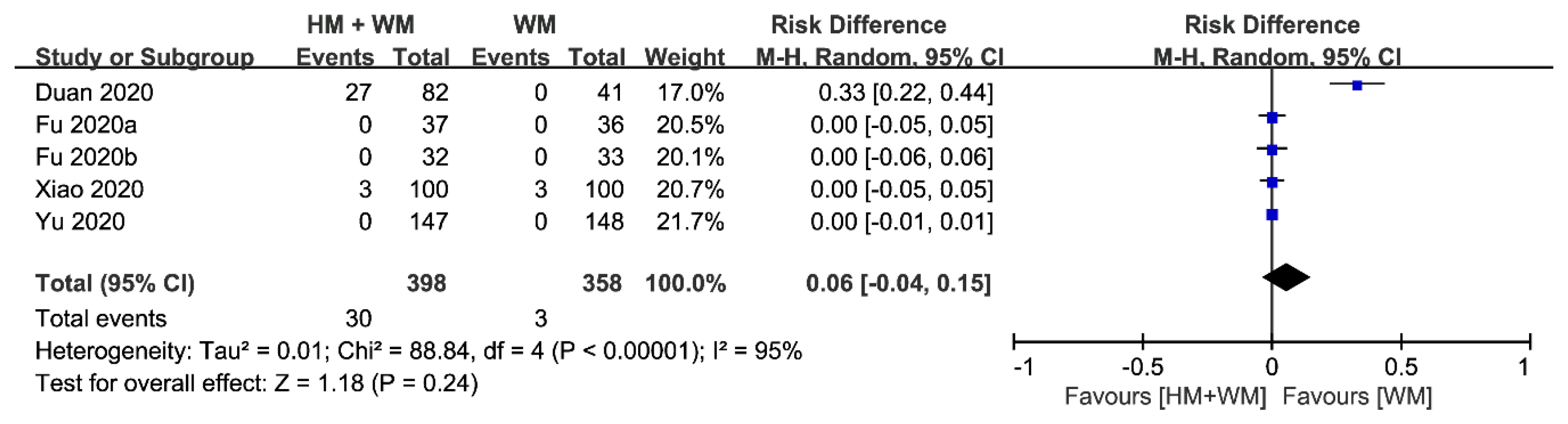
3.4.2. Secondary Outcomes
4. Discussion
4.1. Summary of Evidence
4.2. Advances in the Prior Systematic Review
4.3. Limitations of This Review
4.4. Implications for Clinical Practice
4.5. Implications for Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 19 April 2020).
- Lai, K.K.R.; Wu, J.; Harris, R.; McCann, A.; Collins, K.; Watkins, D.; Patel, J.K. Coronavirus Map: Tracking the Spread of the Outbreak. Available online: https://www.nytimes.com/interactive/2020/world/coronavirus-maps.html?action=click&module=RelatedLinks&pgtype=Article (accessed on 19 April 2020).
- Yang, Y.; Islam, M.S.; Wang, J.; Li, Y.; Chen, X. Traditional Chinese medicine in the treatment of patients infected with 2019-new coronavirus (sars-cov-2): A review and perspective. Int. J. Biol. Sci. 2020, 16, 1708–1717. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, M.; He, L.; Li, Y.P.; Kang, Y.K. Chinese herbs combined with western medicine for severe acute respiratory syndrome (SARS). Cochrane Database Syst. Rev. 2012, 10. [Google Scholar] [CrossRef]
- Luo, H.; Tang, Q.L.; Shang, Y.X.; Liang, S.B.; Yang, M.; Robinson, N.; Liu, J.P. Can Chinese Medicine be used for prevention of corona virus disease 2019 (Covid-19)? A review of historical classics, research evidence and current prevention programs. Chin. J. Integr. Med. 2020, 26, 243–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, L.; Lee, H.W.; Choi, J.Y.; Zhang, J.; Soo Lee, M. Herbal medicine and pattern identification for treating COVID-19: A rapid review of guidelines. Integr. Med. Res. 2020, 9, 100407. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.W.; Wong, V.T.; Tang, S.C.W. Covid-19: An update on the epidemiological, clinical, preventive and therapeutic evidence and guidelines of integrative chinese-western medicine for the management of 2019 novel coronavirus disease. Am. J. Chin. Med. 2020, 48, 737–762. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.Q.; Zou, L.; Yu, X.; Sun, D.; Li, S.B.; Tang, L.; Yang, J.R.; Chen, X.Y.; Wu, Y.G.; Fang, H. Clinical effects of integrated traditional Chinese and western medicine on COVID-19: A systematic review. Shanghai J. Tradit. Chin. Med. 2020, 1–8. [Google Scholar] [CrossRef]
- Qi, G.; Qi, W.; Jiang, Q.; Shen, K.Q.; Zhang, X.; Zhang, L. The Efficacy of Lianhua Qingwen Combined with Western Medicine Scheme on COVID-19 General Type Patients: A Systematic Review. Clin. J. Tradit. Chin. Med. 2020, 1–9. Available online: http://kns.cnki.net/kcms/detail/34.1268.r.20200410.0909.002.html (accessed on 22 May 2020).
- Zhan, Z.L.; Liu, J.; Yang, W.; Wang, Y.G.; Ruan, L.G.; Huang, P.; Guo, L.P.; Bian, Y.J.; Chen, S.P.; Chen, Y.; et al. Exploratory Study on Evaluation Criteria of Chinese Medicine Treatment of New Coronavirus Pneumonia Based on Case Analysis. J. Tradit. Chin. Med. 2020, 1–11. Available online: http://kns.cnki.net/kcms/detail/11.2166.R.20200312.0949.002.html (accessed on 22 May 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, a.t.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X. Guideline of Clinical New Drug Research in Chinese Herbal Medicine; Chinese Medical Science and Technology Press: Beijing, China, 2002. [Google Scholar]
- Jin, X.; Pang, B.; Zhang, J.; Liu, Q.; Yang, Z.; Feng, J.; Liu, X.; Zhang, L.; Wang, B.; Huang, Y.; et al. Core Outcome Set for Clinical Trials on Coronavirus Disease 2019 (COS-COVID). Engineering 2020. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Wang, Y.; Yang, X.; Liu, Y.; Zhang, J.; Feng, Y.; Shang, L.; Zhang, K.; Cheng, Z.; He, X. Preliminary clinical effect analysis of the treatment of novel coronavirus pneumonia by internal administration of traditional Chinese medicine plus fumigation and absorption combined with super dose of vitamin C in treating NOVID-19. J. Xian Jiaotong Univ (Med Sci.) 2020. Available online: http://kns.cnki.net/kcms/detail/61.1399.R.20200320.1045.002.html (accessed on 22 May 2020).
- Lu, R.; Wang, W.; Li, X. Clinical observation on 63 suspected cases of new coronavirus pneumonia treated with medicine Lianhua Qingwen. J. Tradit. Chin. Med. 2020. Available online: http://kns.cnki.net/kcms/detail/11.2166.R.20200215.1633.004.html (accessed on 22 May 2020).
- Liu, M.; Liu, M.; Zhong, H.; Yu, J.; Luo, J.; Ai, K.; Xu, M.; Liu, Q.; Dai, G.; Zhang, W.; et al. Study on the significance and operation mode of moxibustion intervention for home quarantee in close contact with coronavirus disease 2019. Chin. Acupunct Moxibustion 2020, 40, 457–461. [Google Scholar] [CrossRef]
- Yan, B.; Jiang, Z.; Zeng, J.; Tang, J.; Ding, H.; Xia, J.; Qin, S.; Jin, S.; Lu, Y.; Zhang, N.; et al. Large-scale prospective clinical study on prophylactic intervention of COVID-19 intervention in community population using Huoxiang Zhengqi Oral Liquid and Jinhao Jieer Granules. Zhongguo Zhong Yao Za Zhi 2020. [Google Scholar] [CrossRef]
- Sun, H.-M.; Xu, F.; Zhang, L.; Wei, C.; Chen, J.-Y.; Wang, Q.-X.; Jia, Z.-H. Study on clinical efficacy of Lianhua Qingke Granule in treatment of mild and ordinary COVID-19. Zhongguo Shi Yan Fang Ji Xue Za Zhi 2020, 1–8. [Google Scholar] [CrossRef]
- Xiao, Q.; Jiang, Y.J.; Wu, S.S.; Wang, Y.; An, J.; Xu, W.P.; Wu, J.J. The combined therapy of Zhongyao Shufeng Jiedu capsule and Arbidol Hydrochloride Tablets in treating COVID-19 patients. J. Emerg. Tradit. Chin. Med. 2020, 1–3. Available online: http://kns.cnki.net/kcms/detail/50.1102.R.20200309.1528.004.html (accessed on 22 May 2020).
- Duan, C.; Xia, W.G.; Zheng, C.J.; Sun, G.B.; Li, Z.L.; Li, Q.L.; Li, P.; Zhang, H.L.; Yang, F.W.; Zhang, B.L.; et al. Clinical observation of Jinhua Qinggan Granules in treating COVID-19. J. Tradit. Chin. Med. 2020, 1–5. Available online: http://kns.cnki.net/kcms/detail/11.2166.R.20200323.0853.002.html (accessed on 22 May 2020).
- Fu, X.; Lin, L.; Tan, X. Clinical study on 37 case of COVID-19 treated with integrated traditional Chinese and Western Medicine. Tradit. Chin. Drug. Res. Clin. Pharmacol. 2020, 1–9. Available online: http://kns.cnki.net/kcms/detail/44.1308.R.20200319.1644.002.html (accessed on 22 May 2020).
- Fu, X.; Lin, L.; Tan, X. Clinical study on treatment of cases of COVID-19 with Toujie Quwen Granules. Zhongguo Shi Yan Fang Ji Xue Za Zhi 2020. [Google Scholar] [CrossRef]
- Yu, P.; Li, Y.; Wan, S.; Wang, Y. Observation of therapeutic effect of Lianhua Qingwen Granule Combined with Abidor on mild New Coronavirus Pneumonia. Chin. Pharm. J. 2020. Available online: http://kns.cnki.net/kcms/detail/11.2162.R.20200422.1429.002.html (accessed on 22 May 2020).
- Ye, Y.-A. Guideline-based Chinese herbal medicine treatment plus standard care for severe coronavirus disease 2019 (G-CHAMPS): Evidence from China. medRxiv 2020. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) [Ref] | Sample Size (M/F) Disease Stages * Age (Years) Disease Course (Days) | Intervention (Regimen) | Control (Regimen) | Study Outcomes | Results |
|---|---|---|---|---|---|
| Sun (2020) [19] | 57 (28/29) Mild, moderate A: 45.4; B: 42.0 A: 11.7; B: 13.0 | (A) HM (Lianhua Qingke granules, 1 packet for 3 times daily for 14 days, n = 32), plus B | (B) WM (Lopinavir/ Ritonavir + Alpha interferon injection for 2 times daily, n = 25) | (1) Symptom disappearance rate (2) Improvement of abnormalities in chest CT (3) Oxygenation index | (1) Cough, RR 1.42 (1.03, 1.94), p < 0.05; sputum production, RR 1.66 (1.04, 2.64), p < 0.05; fever, RR 1.00 (0.68, 1.46), NS; fatigue, RR 1.25 (0.90, 1.75), NS; dry throat, RR 1.31 [0.62, 2.80], NS; sore throat, RR 1.00 (0.62, 1.60), NS. (2) RR 1.35 (1.05, 1.73), p < 0.05. (3) MD 73.73 (52.75, 94.71), p < 0.05. |
| Xiao (2020) [20] | 200 (130/70) Mild, moderate A:60.9; B: 60.2 A: 5.5; B:6.4 | (A) HM (Shufeng Jiedu capsule, 4 capsules for 3 times daily for 2 weeks, n = 100), plus B | (B) WM (Arbidol Hydrochloride tablets, 200mg for 3 times daily, n = 100) | (1) Effective rate (2) Symptom disappearance time (day) (3) Changes in WBC cell counts and LYM% (4) Absorption of lesions >50% based on chest CT scans | (1) RR 1.17 (1.03, 1.34) p < 0.05. (2) Fever, MD −0.83 (−1.22, −0.44), p < 0.05; cough, MD 0.28 (−0.40, 0.96), NS; fatigue, MD −0.33 (−0.78, 0.12), NS; vertigo, MD 0.18 (−0.31, 0.67), NS; nasal congestion, MD −0.17 (−0.61, 0.27), NS; rhinorrhea, MD 0.08 (−0.33, 0.49), NS. (3) WBC cell counts, MD 1.15 (0.64, 1.66), p < 0.05; LYM%, MD 2.42 (1.08, 3.76), p < 0.05. (4) RR 1.21 (1.05, 1.40), p < 0.05. |
| Duan (2020) [21] | 123 (62/61) Mild A: 52.0; B: 50.3 A: 2.7; B: 2.5 | (A) HM (Jinhua Qinggan granules, 2 packets for 3 times daily for 5 days, n = 82), plus B | (B) WM (Lopinavir/Ritonavir, 200 mg + Chloroquine Phosphate tablets, 500 mg + Alpha interferon and ribavirin injection for 2 times daily + Arbidol Hydrochloride tablets, 500 mg for 3 times daily, n = 41) | (1) Symptoms disappearance rate (2) Total TCM syndrome score (3) Hamilton Anxiety Scale | (1) Fever, RR 1.51 (1.07, 2.14), p < 0.05; chill, RR 0.99 (0.74, 1.34), NS; myalgia, RR 1.17 (0.73, 1.87), NS; heavy head and limbs, RR 0.84 (0.60, 1.19), NS; fatigue, RR 1.44 (0.98, 2.11), p < 0.05; cough, RR 1.54 (0.97, 2.45), p < 0.05; sputum production, RR 1.85 (1.01, 3.38), p < 0.05; sore throat, RR 1.30 (0.58, 2.87), NS; itchy throat, RR 1.14 (0.60, 2.17), NS; dry throat, RR 0.87 (0.54, 1.42), NS; nasal congestion or rhinorrhea, RR 1.31 (0.57, 3.05), NS; nausea or vomiting, RR 1.17 (0.69, 1.99), NS; diarrhea, RR 0.06 (0.00, 1.03), p < 0.05. (2) MD 1.39 (−0.21, 2.99), p < 0.05. (3) MD 0.34 (−1.14, 1.82), p < 0.01. |
| Fu (2020a) [22] | 73 (38/35) Moderate A: 45.3; B: 44.7 A: 7.6; B: 8.5 | (A) HM (Toujie Quwen granules, 1 packet per time for 2 times daily for 15 days, n = 37), plus B | (B) WM (Arbidol Hydrochloride tablets, 200 mg + Ambroxol Hydrochloride tablets, 30 mg for 3 times daily, n = 36) | (1) Effective rate (2) TCM syndrome score (3) Changes in WBC cell counts, LYM cell counts, LYM% and CRP level (4) Hospital discharge rate | (1) RR 1.28 (1.01, 1.64), p < 0.05. (2) Fever, MD −0.50 (−0.72, −0.28), p < 0.05; Cough, MD −1.03 (−1.20, −0.86), p < 0.05; Dry throat and sore throat, MD −0.64 (−0.90, −0.38), p < 0.05; Chest tightness and shortness of breath, MD −0.18 (−0.37, 0.01), p < 0.05; Fatigue, MD −1.14 (−1.27, −1.01), p < 0.05. (3) WBC cell counts, MD 0.26 (0.09, 0.43), NS; LYM cell counts, MD 0.45 (0.39, 0.51), p < 0.05; LYM%, MD 3.18 (2.17, 4.19), NS; CRP level, MD −8.11 (−10.41, −5.81), p < 0.05. (4) RR 1.42 (0.76, 2.62), p < 0.05. |
| Fu (2020b) [23] | 65 (36/29) Mild, moderate A: 43.3; B: 43.7 A: 7.6; B: 8.5 | (A) HM (Toujie Quwen granules, 1 packet per time for 2 times daily for 10 days, n = 32), plus B | (B) WM (Arbidol Hydrochloride Tablets, 200 mg + Moxifloxacin, 400 mg + Ambroxol Hydrochloride Tablets, 30 mg for 3 times daily, n = 33) | (1) Effective rate (2) TCM syndrome score (3) Changes in WBC cell counts, LYM cell counts, LYM% and NEU% (4) Changes in level of CRP, PCT, D-Dimer (5) Improvement of abnormalities in chest CT | (1) RR 1.35 (1.06, 1.71), p < 0.05. (2) Fever, MD −0.80 (−0.95, −0.65), p < 0.05; cough, MD −1.35 (−1.52, −1.18), p < 0.05; sputum production, MD −0.46 (−0.71, −0.21), p < 0.05; dry throat and sore throat, MD −0.48 (−0.66, −0.30), p < 0.05; fatigue, MD −0.34 (−0.45, −0.23), p < 0.05. (3) WBC cell counts, MD 0.36 (0.20, 0.52), p < 0.05; LYM cell counts, MD 0.26 (0.20, 0.32), p < 0.05; LYM%, MD 5.18 (4.11, 6.25), p < 0.05; NEU%, MD −4.58 (−5.81, −3.35), p < 0.05. (4) CRP level, MD −9.11 (−11.52, −6.70), p < 0.05; PCT level, MD −0.02 (−0.02, −0.01), p < 0.05; D-Dimer level, MD −42.50 (−84.55, −0.45), p < 0.05. (5) RR 1.30 (0.97, 1.74), NS. |
| Yu (2020) [24] | 295 (171/124) Mild, moderate A: 48.2; B: 47.2 n.r. | (A) HM (Lianhua Qingwen granules, 1 packet per time for 2 times daily for 7 days, n = 147), plus B | (B) WM (Arbidol Hydrochloride Tablets, 200 mg + Ambroxol Hydrochloride Tablets, 30 mg for 3 times daily + Moxifloxacin tablets, 400 mg for 1 time daily, 30 mg for 3 times daily, n = 148) | (1) Effective rate (2) TCM syndrome score (3) Changes in WBC cell counts, LYM cell counts, CRP level and PCT level (4) Improvement of abnormalities in chest CT | (1) RR 1.25 (1.08, 1.44), p < 0.05. (2) Fever, MD −0.56 (−0.62, −0.50), p < 0.05; fatigue, MD −0.34 (−0.40, −0.28), p < 0.05; cough, MD −1.17 (−1.28, −1.06), p < 0.05; dry throat and sore throat, MD −1.34 (−1.44, −1.24), p < 0.05; chest tightness, MD −0.43 (−0.57, −0.29), p < 0.05. (3) WBC cell counts, MD 0.41 (0.33, 0.49), p < 0.05; LYM cell counts, MD 0.09 (0.05, 0.13), p < 0.05; CRP level, MD −2.00 (−3.00, −1.00), p < 0.05; PCT level, MD −0.01 (−0.02, −0.01), p < 0.05. (4) RR 1.10 (0.94, 1.30), NS. |
| Ye (2020) [25] | 42 (7/35) Severe A: 65.0; B: 59.0 A: 9.0; B: 9.5 | (A) HM († Herbal decoction, 2 times daily for 7 days, n = 28), plus B | (B) WM (Lopinavir/ Ritonavir, 200mg for 2 times daily, n = 14) | (1) Changes in the disease severity (2) Overall survival through last day of treatment (3) Proportion of patients without improvement (4) Change in serum PCT level (5) Prevalence of antibiotic use during treatment | (1) OR 0.589 (0.148, 2.352), NS. (2) OR 2.08 (0.12, 35.89), NS. (3) OR 0.44 (0.08, 2.53), NS. (4) MD 0.01 (0.00, 0.01), p < 0.05. (5) OR 1.84 (0.41, 8.33), NS. |
| Trial Identifier | Sample Size Disease Stage No. of Trial Center | Intervention (Regimen) | Control (Regimen) | Primary Outcome Measures | Secondary Outcome Measures | Registration Date Estimate Trial Duration |
|---|---|---|---|---|---|---|
| NCT 04251871 | 150 n.r. Single | (A) HM (TCM granules, 2 times a day, for 14 days, n = n.r.), plus B | (B) WM (Alpha interferon (inhalation), and Lopinavir/ Ritonavir (oral) for 2 times a day, n = n.r.) | (1) Time to complete remission of symptoms (2) Symptoms’ change (fever and cough) | The incidence of dyspnea with low oxygen saturation level and high respiratory rate/Number of subjects who develop complications/Time to virus shedding/Time to improvement of abnormalities in chest imaging/Improvement of TCM syndrome score | 5 February 2020 22 January 2020 to 22 January 2021 |
| ChiCTR 2000029418 | 32 severe Single | (A) HM (n.r., n = 28), plus B | (B) WM (n.r., n = 14) | Percentage of patients progress to critically ill | Oxygenation index/Procalcitonin level/Percentage of antibiotic use | 30 January 2020 3 February to 31 August 2020 |
| ChiCTR 2000029434 | 240 n.r. Multiple (7) | (A) HM (Lianhua Qingwen capsules/granules, 4 capsules or 1 bag for 3 times daily, n = 120), plus B | (B) WM (n.r., n = 120) | Clinical symptoms recovery rate and recovery time (fever, fatigue, cough) | Time and rate to negativity in RT-PCR nucleic acid test/Proportion of aggravation during treatment/Rate of improvement of abnormalities in chest CT/Single symptom disappearance rate and main symptom disappearance time/Disease recovery rate/Routine blood test/Biochemical indicators | 1 February 2020 1 February to 1 December 2020 |
| ChiCTR 2000029438 | 100 severe or critical Single | (A) HM (n.r., n = 50), plus B | (B) WM (n.r., n = 50) | (1) CURB-65 score (2) PSI score (3) Mechanical ventilation time (4) Length of stay in hospital | Time to reduce fever /Pulmonary function/Mortality and recovery rate/Rate of multiple organ dysfunction/Time to negativity in RT-PCR nucleic acid test/Inflammation index/Incidence of AEs | 1 February 2020 1 February 2020 to 1 December 2021 |
| ChiCTR 2000029439 | 120 moderate Multiple (2) | (A) HM (n.r., n = 60), plus B | (B) WM (n.r., n = 60) | (1) Time to reduce fever (2) Time to negativity in RT-PCR nucleic acid test | Pulmonary function/Rate of patients’ progress to severe stage/Inflammation index/Disappearance time of gastrointestinal symptoms/TCM syndrome score/Incidence of AEs | 1 February 2020 1 February to 31 December 2020 |
| ChiCTR 2000029461 | 100 moderate Multiple (2) | (A) HM (n.r., n = 50), plus B | (B) WM (n.r., n = 50) | (1) Pulmonary function (2) Time to reduce fever (3) Time to negativity in RT-PCR nucleic acid test | Disappearance time of cough/Incidence of AEs/St George’s respiratory questionnaire/Modified Barthel Index/6-min walk test | 2 February 2020 3 February to 31 December 2021 |
| ChiCTR 2000029518 | 140 moderate or severe Single | (A) HM (n.r., n = 70), plus B | (B) WM (n.r., n = 70) | (1) Recovery time (2) Ratio and time for the moderate patients to progress to severe (3) Ratio and time for severe patients to progress to critical or death | Improvement of TCM syndrome score/Relief of clinical symptoms (fever, fatigue, gastrointestinal discomfort, etc.) and duration/Lung HRCT score improvement/Average length of hospital stay/Adverse event rate/Quality of life (SF 36) | 3 February 2020 4 February to 30 April 2020 |
| ChiCTR 2000029549 | 400 mild or moderate Single | (A) HM (n.r., n = 200), plus B | (B) WM (n.r., n = 200) | (1) Rate of patient’s progress to severe stage (2) Oxygenation index (3) Time to negativity in RT-PCR nucleic acid test (4) Improvement of abnormalities in chest CT | n.r. | 4 February 2020 3 February to 1 May 2020 |
| ChiCTR 2000029747 | 200 n.r. Multiple (4) | (A) HM (n.r., n = 100) | (B) WM (n.r., n = 100) | (1) Improvement of abnormalities in chest CT (2) Routine blood test (3) Liver and renal function (4) Improvement of TCM syndrome score | n.r. | 11 February 2020 1 February 2020 to 10 February 2021 |
| ChiCTR 2000029755 | 120 mild or moderate Single | (A) HM (Jinyebaidu granule, 1‒2 packets, 3 times daily, n = 60), plus B | (B) WM (n.r., n = 60) | Effective index | Safety index | 12 February 2020 12 February to 30 May 2020 |
| ChiCTR 2000029763 | 408 n.r. Single | (A) HM (n.r., n = 204), plus B | (B) WM (n.r., n = 204) | Rate of patients progress to severe or critical illness | Rate of isolation discharge/Improvement of TCM syndrome score/Body temperature/Blood routine test/Blood biochemical test/Improvement of abnormalities in chest imaging/Psychological outcomes | 12 February 2020 12 February to 31 May 2020 |
| ChiCTR 2000029769 | 40 severe Single | (A) HM (Babaodan, 6 capsules, 2 times daily, n = 20), plus B | (B) WM (n.r., n = 20) | (1) 28-day survival rate (2) Inflammatory factor levels | n.r. | 13 February 2020 15 February to 30 April 2020 |
| ChiCTR 2000029777 | 160 n.r. Single | (A) HM (Truncation and Torsion Formula, n = 80), plus B | (B) WM (n.r., n = 80) | (1) Responses after 14 days (recovery, improvement, turning critical, death) (2) Improvement of abnormalities in chest CT | Vital signs/Oxygenation index/Routine blood test/Inflammatory biomarkers/Major organ function/Coagulation index/APACHE II | 13 February 2020 1 February to 30 June 2020 |
| ChiCTR 2000029788 | 60 mild Single | (A) HM (n.r., n = 30), plus B | (B) WM (n.r., n = 30) | (1) Time to reduce fever (2) Time to negativity in RT-PCR nucleic acid test (3) Blood gas analysis (4) Improvement of TCM syndrome score | n.r. | 13 February 2020 31 March to 30 December 2020 |
| ChiCTR 2000029790 | 120 n.r. Single | (A) HM (n.r., n = 60), plus B | (B) WM (n.r., n = 60) | Improvement of TCM syndrome score | Rate of patients’ progress to severe or critical illness/Time to negativity in RT-PCR nucleic acid test/Time to reduce fever/Length of stay in hospital | 13 February 2020 17 February to 31 October 2020 |
| ChiCTR 2000029813 | 72 mild or moderate Single | (A) HM (Tanreqing, 3 capsules for 3 times daily, n = 36), plus B | (B) WM (n.r., n = 36) | (1) Time to negativity in RT-PCR nucleic acid test (2) Time to reduce fever | Arterial oxygen saturation/Rate of patients’ progress to severe or critical illness/Inflammation index (CRP)/The disappearance rate and time of cough symptoms/Clinical recovery time | 14 February 2020 14 February to 14 August 2020 |
| ChiCTR 2000029822 | 110 n.r. n.r. | (A) HM (Jinyinhua Tang, n = 70) | (B) Placebo (n.r., n = 40) | Effective rate | Time to reduce fever/Pulmonary symptoms and measure/Length of stay in hospital | 14 February 2020 7 February to 30 April 2020 |
| ChiCTR 2000029869 | 300 n.r. Multiple (3) | (A) HM (Baidu Jieduan formula, n = 150), plus B | (B) WM (n.r., n = 150) | (1) Responses after 14 days (recovery, improvement, turning critical, death) (2) Improvement of abnormalities in chest CT | Pneumonia symptoms/Oxygenation index/Routine blood test/Major organ function/Coagulation index/Inflammatory biomarkers | 15 February 2020 1 February to 30 June 2020 |
| ChiCTR 2000029941 | 200 mild, moderate, or severe Multiple (5) | (A) HM (Zhongyao Fufang granules, n = 100), plus B | (B) WM (n.r., n = 100) | Incidence of aggravation events | Total duration of disease/Length of stay in hospital/Time to total recovery/Time to negativity in RT-PCR nucleic acid test/Time from treatment to the beginning of antipyretic/Time from treatment to complete antipyretic/Improvement of abnormalities in chest imaging/Incidence of AEs | 17 February 2020 1 March to 1 June 2020 |
| ChiCTR 2000029947 | 200 n.r. Multiple (5) | (A) HM (Zhongyao Fufang granules, n = 100), plus B | (B) WM (n.r., n = 100) | Lung function | Total duration of disease/Time to total recovery/Incidence of AEs/Incidence of sequelae/Quality of life (SF 36)/Mental health scale | 17 February 2020 1 March to 1 June 2020 |
| ChiCTR 2000029960 | 100 n.r. Single | (A) HM (n.r., n = 70), plus B | (B) WM (n.r., n = 30) | Improvement of TCM syndrome score | n.r. | 17 February 2020 21 February to 31 May 2020 |
| ChiCTR 2000030034 | 132 n.r. Multiple (7) | (A) HM (n.r., n = 88), plus B | (B) WM (n.r., n = 44) | (1) Body temperature (2) Improvement of TCM syndrome score (3) Murray Score for Acute Lung Injury (4) Time to negativity in RT‒PCR nucleic acid test (5) MuLBSTA score | n.r. | 21 February 2020 1 February to 30 June 2020 |
| ChiCTR 2000030166 | 20 n.r. Single | (A) HM (Qingwen Baidu Yin granules, n = 10), plus B | (B) WM (Lopinavir‒ritonavir tablets + recombinant human interferon alpha 2b injection, n = 10) | (1) Improvement of abnormalities in chest CT (2) Nucleic acid detection of throat secretion | Body temperature/3CL Mpro of Coronavirus/Routine blood test/ Routine urine test/Liver function test/Renal function test/Routine stool test | 24 February 2020 25 February to 14 May 2020 |
| ChiCTR 2000030188 | 120 n.r. Single | (A) HM (n.r., n = 80), plus B | (B) WM (n.r., n = 40) | (1) Improvement of TCM syndrome score (2) Time to negativity in RT-PCR nucleic acid test (3) Cure/mortality rate | Major symptom remission time/Blood gas analysis/Indicators of inflammation (CRP, ESR)/Improvement of abnormalities in chest CT | 24 February 2020 15 February to 30 March 2020 |
| ChiCTR 2000030288 | 104 mild or moderate Single | (A) HM (n.r., n = 102), plus B | (B) WM (n.r., n = 102) | Time to negativity in RT-PCR nucleic acid test | The 7-point scale/Rate of patients’ progress to severe or critical illness/Routine blood test/Blood biochemical test | 27 February 2020 27 February to 31 December 2020 |
| ChiCTR 2000030469 | 96 moderate or severe Single | (A) HM (Liu Shen Wan, n = 48), plus B | (B) WM (n.r., n = 48) | (1) Time to reduce fever (2) Effective rate of TCM symptoms | Body temperature/Improvement of abnormalities in chest CT/Time to negativity in RT-PCR nucleic acid test/Oxygen saturation/Length of stay in hospital/Rate of patients’ progress to severe or critical illness/Improvement of TCM syndrome score/Routine blood test | 2 March 2020 27 February to 27 May 2020 |
| ChiCTR 2000030479 | 100 moderate Multiple (3) | (A) HM (Yiqi Huashi Jiedu Fang, n = 50), plus B | (B) WM (n.r., n = 50) | (1) Time to reduce fever (2) Time to negativity in RT-PCR nucleic acid test | Improvement of TCM syndrome score/Changes in inflammation indicators/Changes in SpO2, oxygen saturation, lymphocyte count/Time to clinical recovery/Rate of patients progress to severe or critical illness | 3 March 2020 26 February 2020 to 25 February 2021 |
| ChiCTR 2000030522 | 100 mild or moderateMultiple (3) | (A) HM (Ma Xing Shi Gan Tang, n = 50), plus B | (B) WM (n.r., n = 50), plus Placebo | Time to clinical recovery | Time to reduce fever/Time to negativity in RT-PCR nucleic acid test/Rate of patients’ progress to severe or critical illness/Laboratory tests (white blood cell and lymphocyte count, erythrocyte sedimentation rate, CRP/ Improvement of abnormalities in chest CT/Improvement of TCM syndrome score | 5 March 2020 9 March to 9 September 2020 |
| ChiCTR 2000030759 | 60 n.r. Multiple (3) | (A) HM (n.r., n = 56), plus B | (B) WM (n.r., n = 14) | (1) Time to negativity in RT-PCR nucleic acid test (2) Incidence of aggravation events (3) Time to reduce fever (4) Improvement of abnormalities in chest CT (5) Major symptom remission rate | Blood count/CRP/Blood gas analysis/Routine urine test/Blood lipid, Blood glucose, Coagulation function test/Liver function test, renal function/Myocardial enzymes/Serum procalcitonin, T-lymphocyte subsets, Interleukin | 13 March 2020 15 February to 17 May 2020 |
| ChiCTR 2000030936 | 2840 n.r. Multiple (71) | (A) HM (Xinguan No. 2/Xinguan No. 3, n = 2130), plus B | (B) WM (n.r., n = 710) | (1) Time to reduce fever (2) Disappearance rate of TCM symptoms | n.r. | 18 March 2020 10 March to 10 May 2020 |
| ChiCTR 2000030937 | 144 n.r. Multiple (6) | (A) HM (Gu Shen Ding Chuan Wan, n = 72), plus B | (B) WM (n.r., n = 72) | (1) Changes in TCM syndrome (2) Changes of fatigue assessment scale | n.r. | 18 March 2020 19 March to 30 August 2020 |
| ChiCTR 2000030988 | 204 mild, moderate, or severe Single | (A) HM (Hua Shi Bai Du granules, n = 102), plus B | (B) WM (n.r., n = 102) | Improvement of abnormalities in chest CT | Length of stay in hospital/Incidence of AEs | 20 March 2020 20 March to 31 May 2020 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ang, L.; Song, E.; Lee, H.W.; Lee, M.S. Herbal Medicine for the Treatment of Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 1583. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9051583
Ang L, Song E, Lee HW, Lee MS. Herbal Medicine for the Treatment of Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2020; 9(5):1583. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9051583
Chicago/Turabian StyleAng, Lin, Eunhye Song, Hye Won Lee, and Myeong Soo Lee. 2020. "Herbal Medicine for the Treatment of Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 9, no. 5: 1583. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9051583