Allogeneic Bone Marrow Mesenchymal Stem Cell Transplantation in Tooth Extractions Sites Ameliorates the Incidence of Osteonecrotic Jaw-Like Lesions in Zoledronic Acid-Treated Rats

 ,
,  , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Section
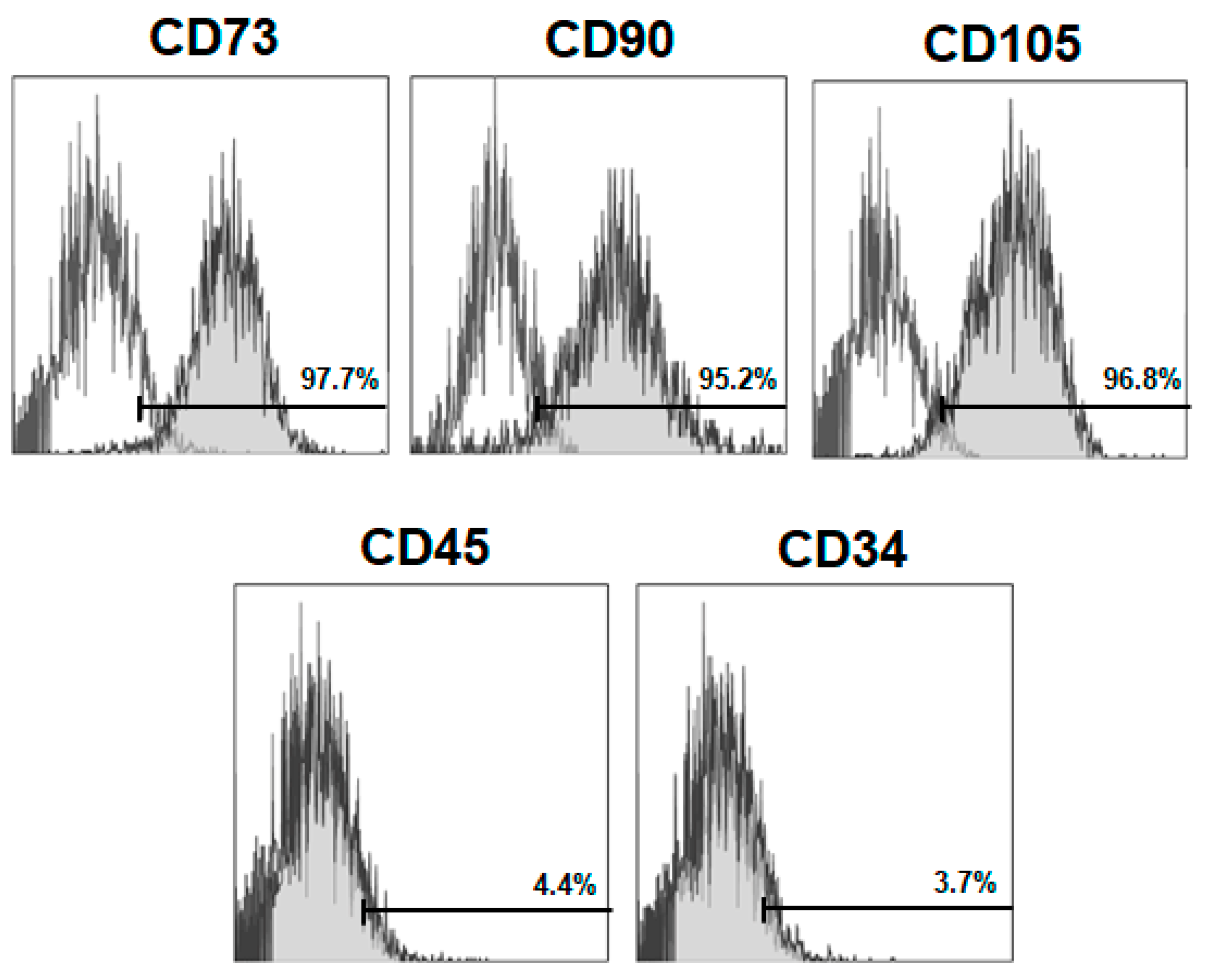
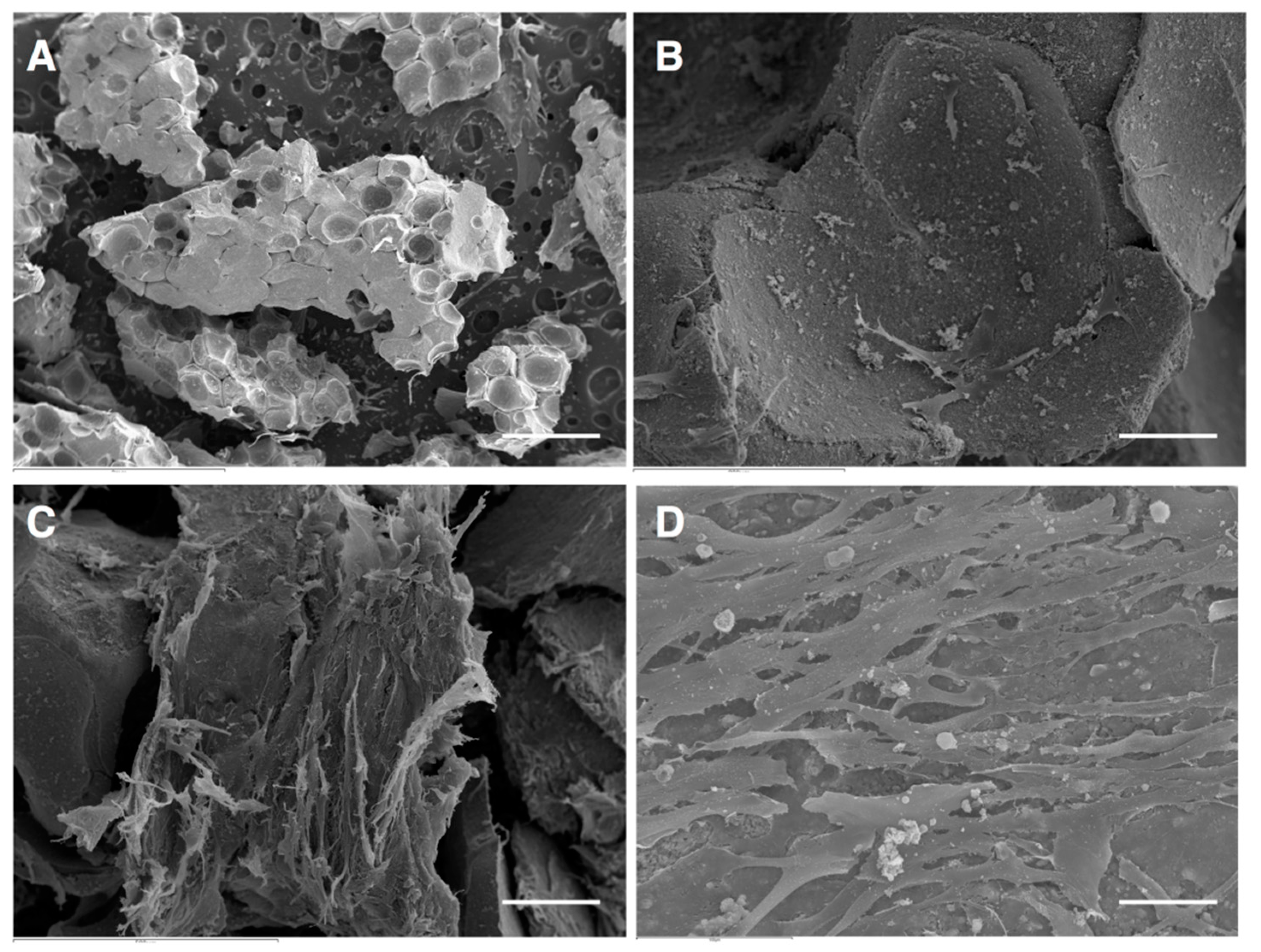
2.1. BM-MSCs Isolation, Characterization and Culture on Scaffolds
2.2. Experimental Design
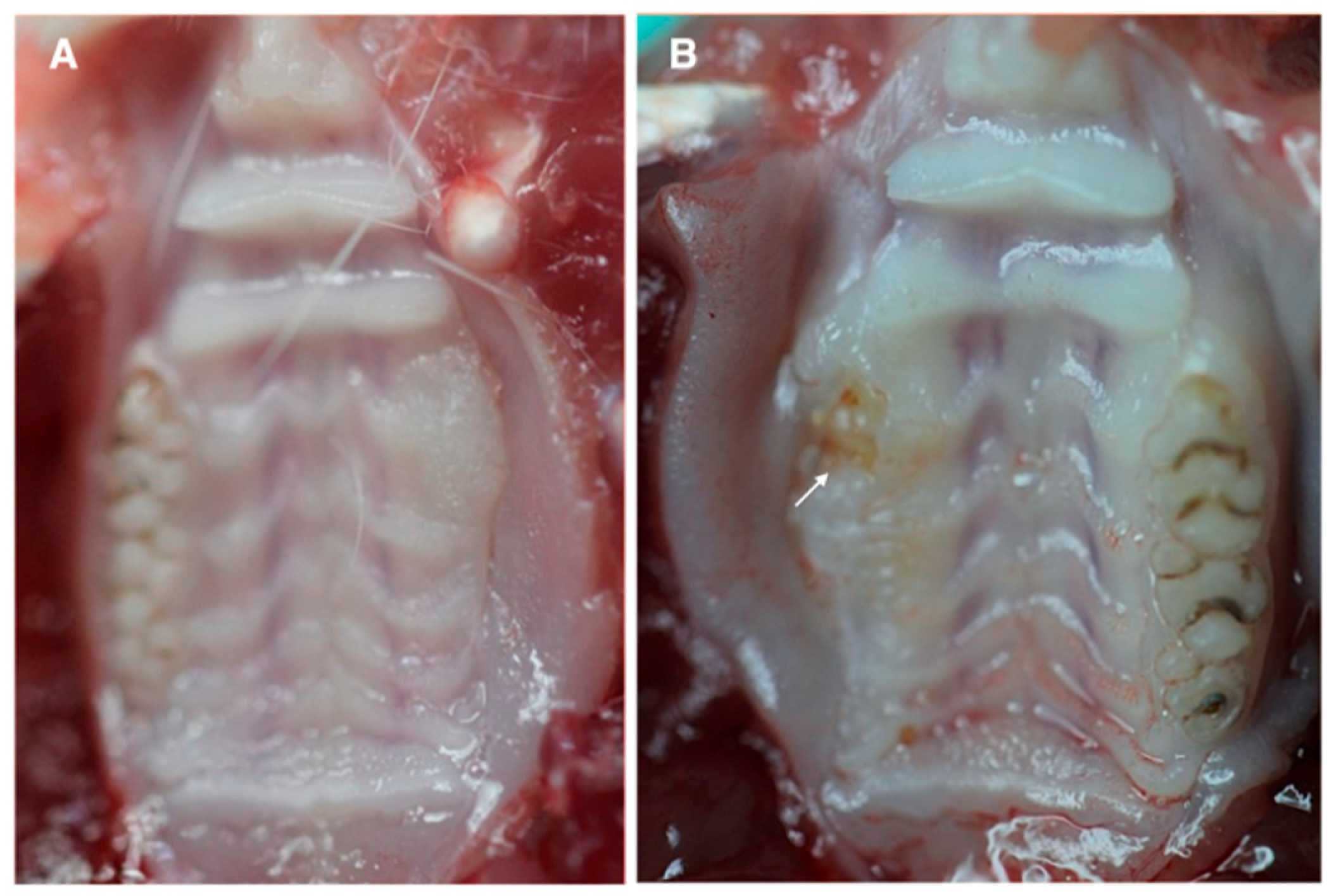
2.3. Macroscopic Analysis
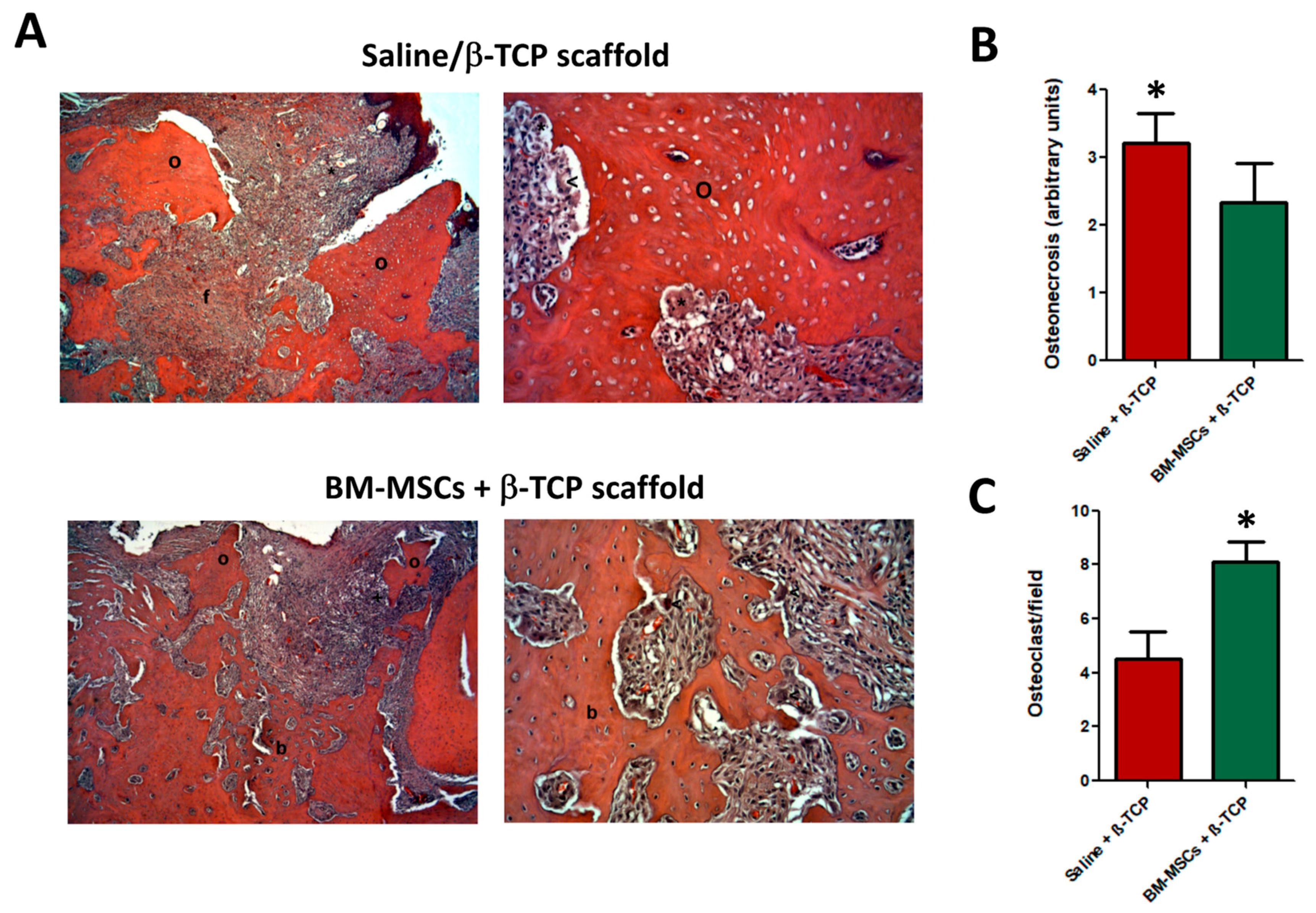
2.4. Histological Observation
2.5. Nested Polymerase Chain Reaction (PCR) Protocol for Y Chromosome-Specific DNA Detection in Rat Decalcified Jaw Samples
2.6. Statistical Analysis
3. Results
3.1. Isolation, Characterization and Culture on Scaffold
3.2. Clinical Visualization of MRONJ
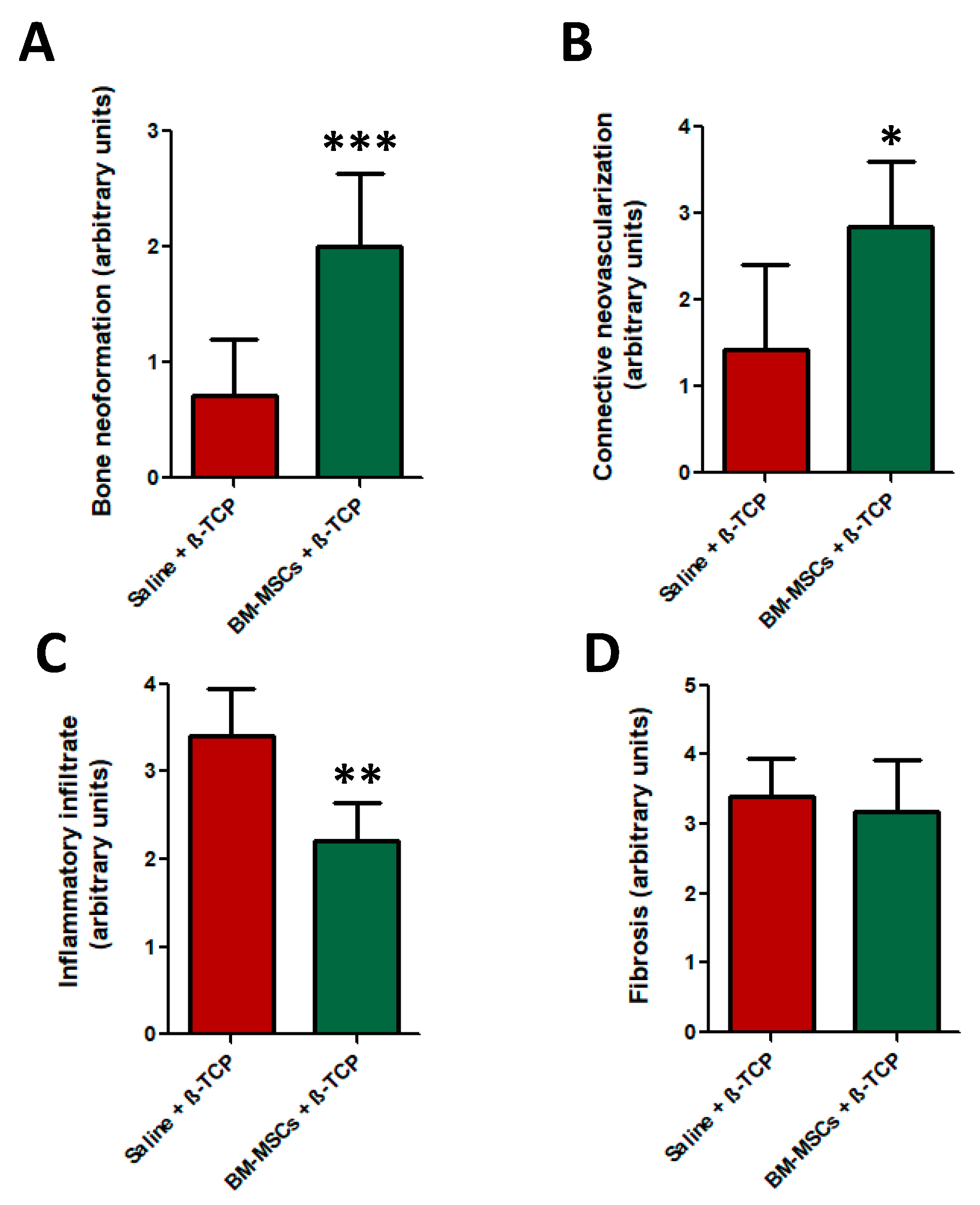
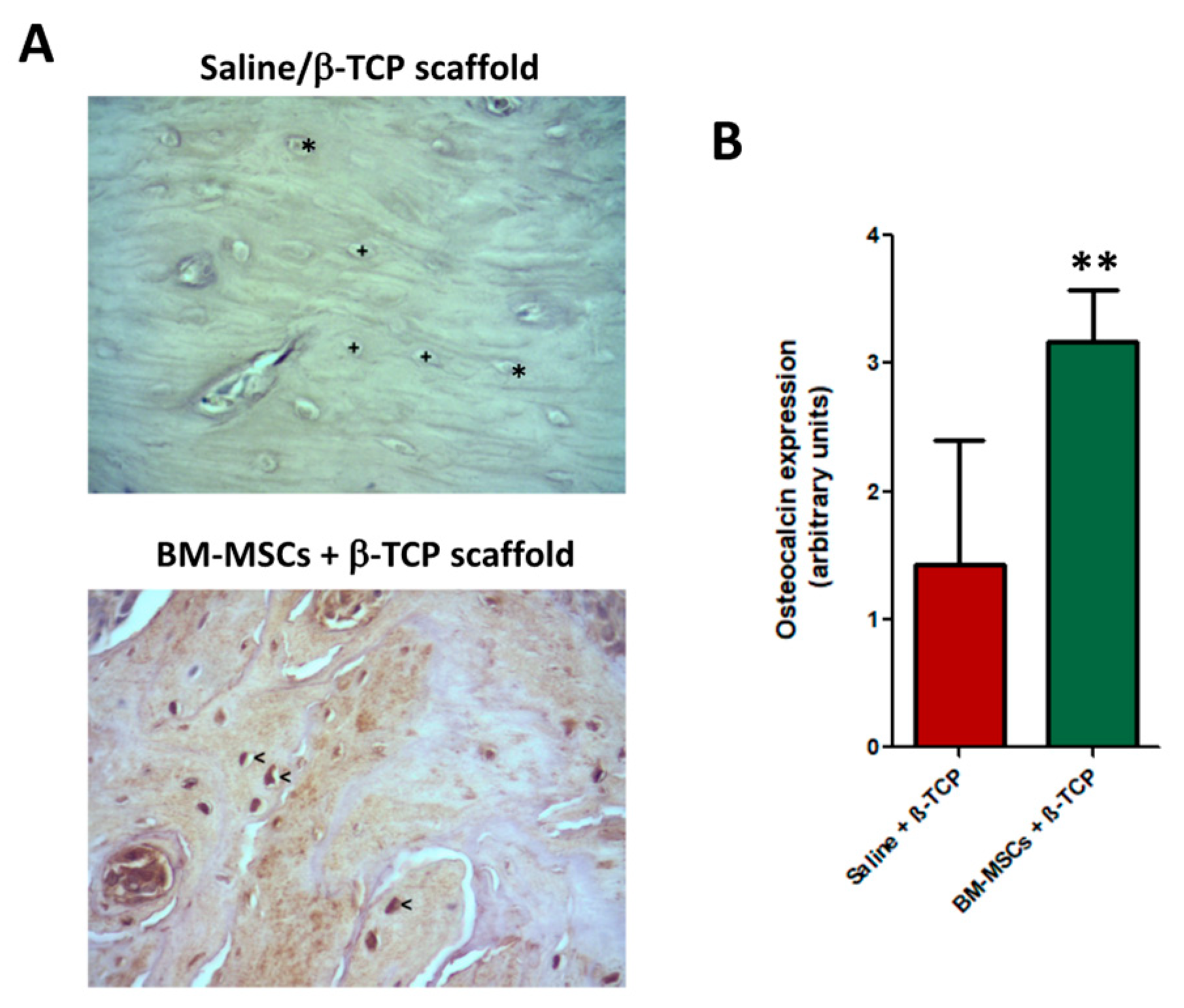
3.3. Histological Analysis
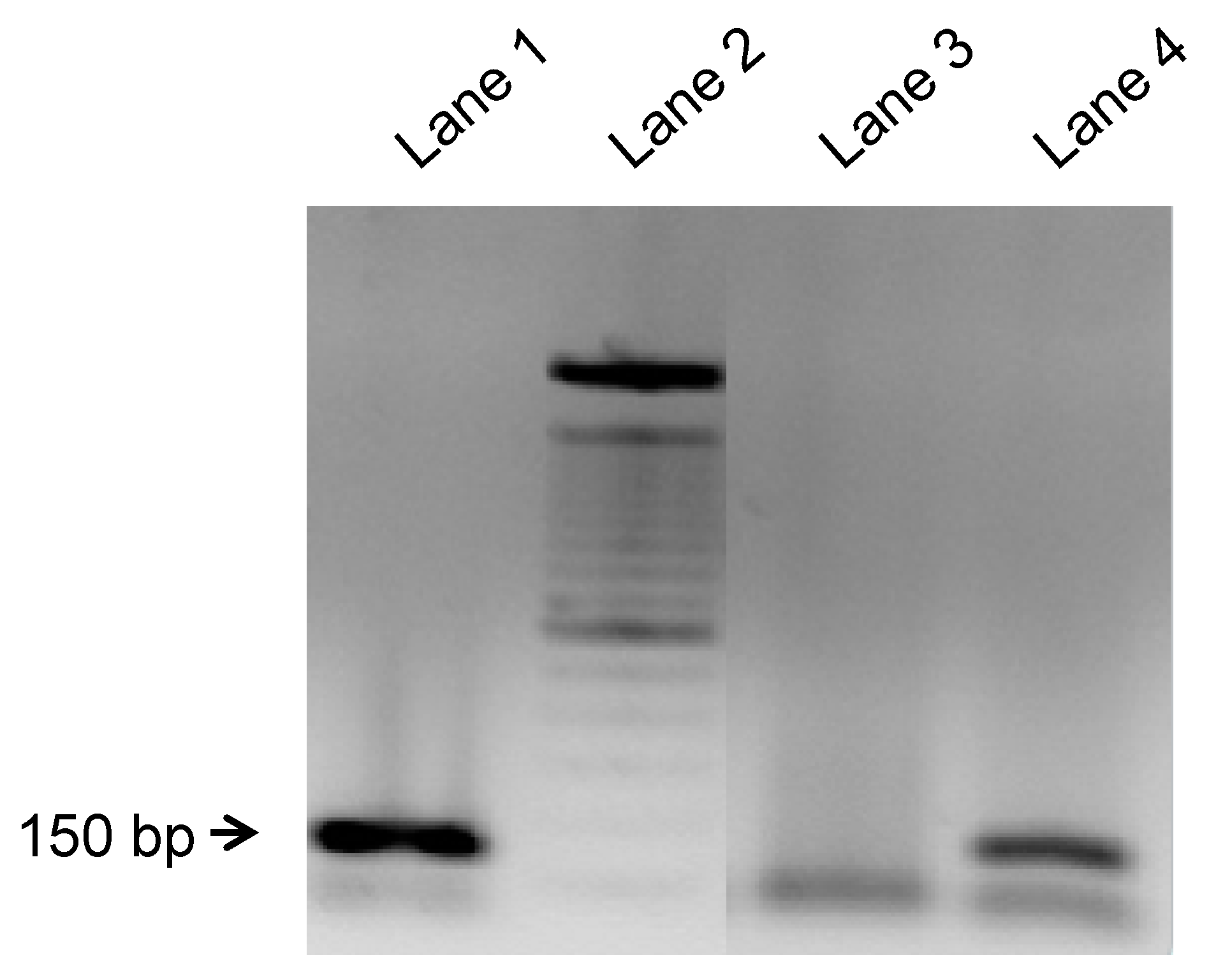
3.4. Y-Chromosome Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Marx, R.E. Uncovering the cause of “phossy jaw” Circa 1858 to 1906: Oral and maxillofacial surgery closed case files-case closed. J. Oral Maxillofac. Surg. 2008, 66, 2356–2363. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Hamadeh, I.S.; Ngwa, B.A.; Gong, Y. Drug induced osteonecrosis of the jaw. Cancer Treat. Rev. 2015, 41, 455–464. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.M.; Dulai, S.; Godfrey, C.; Amanat, N.; Sztynda, T.; Little, D.G. Bolus or weekly zoledronic acid administration does not delay endochondral fracture repair but weekly dosing enhances delays in hard callus remodeling. Bone 2008, 43, 653–662. [Google Scholar] [CrossRef]
- Weinstein, R.S.; Roberson, P.K.; Manolagas, S.C. Giant osteoclast formation and long-term oral bisphosphonate therapy. N. Engl. J. Med. 2009, 360, 53–62. [Google Scholar] [CrossRef]
- Reid, I.R.; Bolland, M.J.; Grey, A.B. Is bisphosphonate-associated osteonecrosis of the jaw caused by soft tissue toxicity? Bone 2007, 41, 318–320. [Google Scholar] [CrossRef]
- Baumgartner, J.C.; Reid, D.E.; Pickett, A.B. Human pulpal reaction to the modified McInnes bleaching technique. J. Endod. 1983, 9, 527–529. [Google Scholar] [CrossRef]
- Cetinkaya, B.O.; Keles, G.C.; Ayas, B.; Gurgor, P. Effects of risedronate on alveolar bone loss and angiogenesis: A stereologic study in rats. J. Periodontol. 2008, 79, 1950–1961. [Google Scholar] [CrossRef]
- Hansen, T.; Kunkel, M.; Weber, A.; James Kirkpatrick, C. Osteonecrosis of the jaws in patients treated with bisphosphonates–Histomorphologic analysis in comparison with infected osteoradionecrosis. J. Oral Pathol. Med. 2006, 35, 155–160. [Google Scholar] [CrossRef]
- Roelofs, A.J.; Jauhiainen, M.; Monkkonen, H.; Rogers, M.J.; Monkkonen, J.; Thompson, K. Peripheral blood monocytes are responsible for gammadelta T cell activation induced by zoledronic acid through accumulation of IPP/DMAPP. Br. J. Haematol. 2009, 144, 245–250. [Google Scholar] [CrossRef] [Green Version]
- Borumandi, F.; Aghaloo, T.; Cascarini, L.; Gaggl, A.; Fasanmade, K. Anti-resorptive Drugs and their Impact on Maxillofacial Bone among Cancer Patients. Anticancer Agents Med. Chem. 2015, 15, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Rollason, V.; Laverriere, A.; MacDonald, L.C.; Walsh, T.; Tramer, M.R.; Vogt-Ferrier, N.B. Interventions for treating bisphosphonate-related osteonecrosis of the jaw (BRONJ). Cochrane Database Syst. Rev. 2016, 2, CD008455. [Google Scholar] [CrossRef] [PubMed]
- Kikuiri, T.; Kim, I.; Yamaza, T.; Akiyama, K.; Zhang, Q.; Li, Y.; Chen, C.; Chen, W.; Wang, S.; Le, A.D.; et al. Cell-based immunotherapy with mesenchymal stem cells cures bisphosphonate-related osteonecrosis of the jaw-like disease in mice. J. Bone Miner. Res. 2010, 25, 1668–1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, L.; Oppici, A.; Arbasi, M.; Moretto, M.; Piepoli, M.; Vallisa, D.; Zangrandi, A.; Di Nunzio, C.; Cavanna, L. Autologous bone marrow stem cell intralesional transplantation repairing bisphosphonate related osteonecrosis of the jaw. Head Face Med. 2011, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzálvez-García, M.; Rodríguez-Lozano, F.J.; Villanueva, V.; Segarra-Fenoll, D.; Rodríguez-González, M.A.; Oñate-Sánchez, R.; Blanquer, M.; Moraleda, J.M. Cell therapy in bisphosphonate-related osteonecrosis of the jaw. J. Craniofac. Surg. 2013, 24, e226–e228. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, J.; Mao, L.; Liu, Y.; Gao, R.; Zheng, Z.; Chen, W.; Le, A.; Shi, S.; Wang, S. Allogeneic mesenchymal stem cell therapy for bisphosphonate-related jaw osteonecrosis in Swine. Stem Cells Dev. 2013, 22, 2047–2056. [Google Scholar] [CrossRef] [Green Version]
- Uccelli, A.; Moretta, L.; Pistoia, V. Mesenchymal stem cells in health and disease. Nat. Rev. Immunol. 2008, 8, 726–736. [Google Scholar] [CrossRef]
- Sun, Y.; Feng, Y.; Zhang, C. The effect of bone marrow mononuclear cells on vascularization and bone regeneration in steroid-induced osteonecrosis of the femoral head. Jt. Bone Spine 2009, 76, 685–690. [Google Scholar] [CrossRef]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage potential of adult human mesenchymal stem cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Kern, S.; Eichler, H.; Stoeve, J.; Kluter, H.; Bieback, K. Comparative analysis of mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose tissue. Stem. Cells 2006, 24, 1294–1301. [Google Scholar] [CrossRef]
- Rodríguez-Lozano, F.J.; Bueno, C.; Insausti, C.L.; Meseguer, L.; Ramírez, M.C.; Blanquer, M.; Marín, N.; Martínez, S.; Moraleda, J.M. Mesenchymal stem cells derived from dental tissues. Int. Endod. J. 2011, 44, 800–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogata, K.; Katagiri, W.; Osugi, M.; Kawai, T.; Sugimura, Y.; Hibi, H.; Nakamura, S.; Ueda, M. Evaluation of the therapeutic effects of conditioned media from mesenchymal stem cells in a rat bisphosphonate-related osteonecrosis of the jaw-like model. Bone 2015, 74, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Barba-Recreo, P.; Del Castillo Pardo de Vera, J.L.; Georgiev-Hristov, T.; Ruiz Bravo-Burguillos, E.; Abarrategi, A.; Burgueno, M.; Garcia-Arranz, M. Adipose-derived stem cells and platelet-rich plasma for preventive treatment of bisphosphonate-related osteonecrosis of the jaw in a murine model. J. Craniomaxillofac Surg. 2015, 43, 1161–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, D.; Hamlet, S.; Petcu, E.; Ivanovski, S. Animal models for bisphosphonate-related osteonecrosis of the jaws–An appraisal. Oral. Dis. 2013, 19, 747–754. [Google Scholar] [CrossRef] [PubMed]
- de Almeida, A.D.; Leite, F.G.; Chaud, M.V.; Rebelo, M.A.; Borges, L.; Viroel, F.J.M.; Hataka, A.; Grotto, D. Safety and efficacy of hydroxyapatite scaffold in the prevention of jaw osteonecrosis in vivo. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 106, 1799–1808. [Google Scholar] [CrossRef]
- Barba-Recreo, P.; Del Castillo Pardo de Vera, J.L.; García-Arranz, M.; Yébenes, L.; Burgueño, M. Zoledronic acid–Related osteonecrosis of the jaws. Experimental model with dental extractions in rats. J. Craniomaxillofac Surg. 2014, 42, 744–750. [Google Scholar] [CrossRef]
- Aguirre, J.I.; Altman, M.K.; Vanegas, S.M.; Franz, S.E.; Bassit, A.C.F.; Wronski, T.J. Effects of Alendronate on Bone Healing After Tooth Extraction in Rats. Oral Dis. 2010, 16, 674–685. [Google Scholar] [CrossRef]
- Koneski, F.; Popovic-Monevska, D.; Gjorgoski, I.; Krajoska, J.; Popovska, M.; Muratovska, I.; Velickovski, B.; Petrushevska, G.; Popovski, V. In vivo effects of geranylgeraniol on the development of bisphosphonate-related osteonecrosis of the jaws. J. Craniomaxillofac Surg. 2017, 46, 230–236. [Google Scholar] [CrossRef]
- Basi, D.L.; Hughes, P.J.; Thumbigere-Math, V.; Sabino, M.; Mariash, A.; Lunos, S.A.; Jensen, E.; Gopalakrishnan, R. Matrix metalloproteinase-9 expression in alveolar extraction sockets of Zoledronic acid-treated rats. J. Oral Maxillofac. Surg. 2011, 69, 2698–2707. [Google Scholar] [CrossRef]
- Yamashita, J.; Koi, K.; Yang, D.Y.; McCauley, L.K. Effect of zoledronate on oral wound healing in rats. Clin. Cancer Res. 2011, 17, 1405–1414. [Google Scholar] [CrossRef] [Green Version]
- Kuehn, B.M. Reports of adverse events from bone drugs prompt caution. Jama 2006, 295, 2833–2836. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Lozano, F.J.; Onate-Sanchez, R.E. Treatment of osteonecrosis of the jaw related to bisphosphonates and other antiresorptive agents. Med. Oral Patol. Oral Cir. Bucal 2016, 21, 595–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aghaloo, T.L.; Kang, B.; Sung, E.C.; Shoff, M.; Ronconi, M.; Gotcher, J.E.; Bezouglaia, O.; Dry, S.M.; Tetradis, S. Periodontal disease and bisphosphonates induce osteonecrosis of the jaws in the rat. J. Bone Miner. Res. 2011, 26, 1871–1882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Lozano, F.J.; Garcia-Bernal, D.; Ros-Roca Mde, L.; Alguero Mdel, C.; Onate-Sanchez, R.E.; Camacho-Alonso, F.; Moraleda, J.M. Cytoprotective effects of melatonin on zoledronic acid-treated human mesenchymal stem cells in vitro. J. Craniomaxillofac Surg. 2015, 43, 855–862. [Google Scholar] [CrossRef]
- Nauta, A.J.; Fibbe, W.E. Immunomodulatory properties of mesenchymal stromal cells. Blood 2007, 110, 3499–3506. [Google Scholar] [CrossRef] [Green Version]
- Kuroshima, S.; Sasaki, M.; Nakajima, K.; Tamaki, S.; Hayano, H.; Sawase, T. Transplantation of Noncultured Stromal Vascular Fraction Cells of Adipose Tissue Ameliorates Osteonecrosis of the Jaw-Like Lesions in Mice. J. Bone Miner. Res. 2018, 33, 154–166. [Google Scholar] [CrossRef] [Green Version]
- Otto, S.; Pautke, C.; Martin Jurado, O.; Nehrbass, D.; Stoddart, M.J.; Ehrenfeld, M.; Zeiter, S. Further development of the MRONJ minipig large animal model. J. Craniomaxillofac Surg. 2017, 45, 1503–1514. [Google Scholar] [CrossRef]
- Yalcin-Ulker, G.M.; Cumbul, A.; Duygu-Capar, G.; Uslu, U.; Sencift, K. Preventive Effect of Phosphodiesterase Inhibitor Pentoxifylline Against Medication-Related Osteonecrosis of the Jaw: An Animal Study. J. Oral Maxillofac. Surg. 2017, 75, 2354–2368. [Google Scholar] [CrossRef]
- Beninati, F.; Pruneti, R.; Ficarra, G. Bisphosphonate-related osteonecrosis of the jaws (Bronj). Med. Oral. Patol. Oral. y Cir. Bucal 2013, 18, e752–e758. [Google Scholar] [CrossRef]
- Voss, P.J.; Matsumoto, A.; Alvarado, E.; Schmelzeisen, R.; Duttenhofer, F.; Poxleitner, P. Treatment of stage II medication-related osteonecrosis of the jaw with necrosectomy and autologous bone marrow mesenchymal stem cells. Odontology 2017, 105, 484–493. [Google Scholar] [CrossRef]
- Hadjidakis, D.J.; Androulakis, I.I. Bone remodeling. Ann. N. Y. Acad. Sci. 2006, 1092, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Mergoni, G.; Vescovi, P.; Sala, R.; Merigo, E.; Passerini, P.; Maestri, R.; Corradi, D.; Govoni, P.; Nammour, S.; Bianchi, M.G. The effect of laser therapy on the expression of osteocalcin and osteopontin after tooth extraction in rats treated with zoledronate and dexamethasone. Support. Care Cancer 2016, 24, 807–813. [Google Scholar] [CrossRef] [PubMed]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Lozano, F.J.; Oñate-Sánchez, R.; Gonzálvez-García, M.; Vallés-Bergadá, M.; Martínez, C.M.; Revilla-Nuin, B.; Guerrero-Gironés, J.; Moraleda, J.M.; García-Bernal, D. Allogeneic Bone Marrow Mesenchymal Stem Cell Transplantation in Tooth Extractions Sites Ameliorates the Incidence of Osteonecrotic Jaw-Like Lesions in Zoledronic Acid-Treated Rats. J. Clin. Med. 2020, 9, 1649. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061649
Rodríguez-Lozano FJ, Oñate-Sánchez R, Gonzálvez-García M, Vallés-Bergadá M, Martínez CM, Revilla-Nuin B, Guerrero-Gironés J, Moraleda JM, García-Bernal D. Allogeneic Bone Marrow Mesenchymal Stem Cell Transplantation in Tooth Extractions Sites Ameliorates the Incidence of Osteonecrotic Jaw-Like Lesions in Zoledronic Acid-Treated Rats. Journal of Clinical Medicine. 2020; 9(6):1649. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061649
Chicago/Turabian StyleRodríguez-Lozano, Francisco Javier, Ricardo Oñate-Sánchez, Mar Gonzálvez-García, Marta Vallés-Bergadá, Carlos M. Martínez, Beatriz Revilla-Nuin, Julia Guerrero-Gironés, Jose M. Moraleda, and David García-Bernal. 2020. "Allogeneic Bone Marrow Mesenchymal Stem Cell Transplantation in Tooth Extractions Sites Ameliorates the Incidence of Osteonecrotic Jaw-Like Lesions in Zoledronic Acid-Treated Rats" Journal of Clinical Medicine 9, no. 6: 1649. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061649