Prospective Association of Air-Purifier Usage during Pregnancy with Infant Neurodevelopment: A Nationwide Longitudinal Study—Japan Environment and Children’s Study (JECS)

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
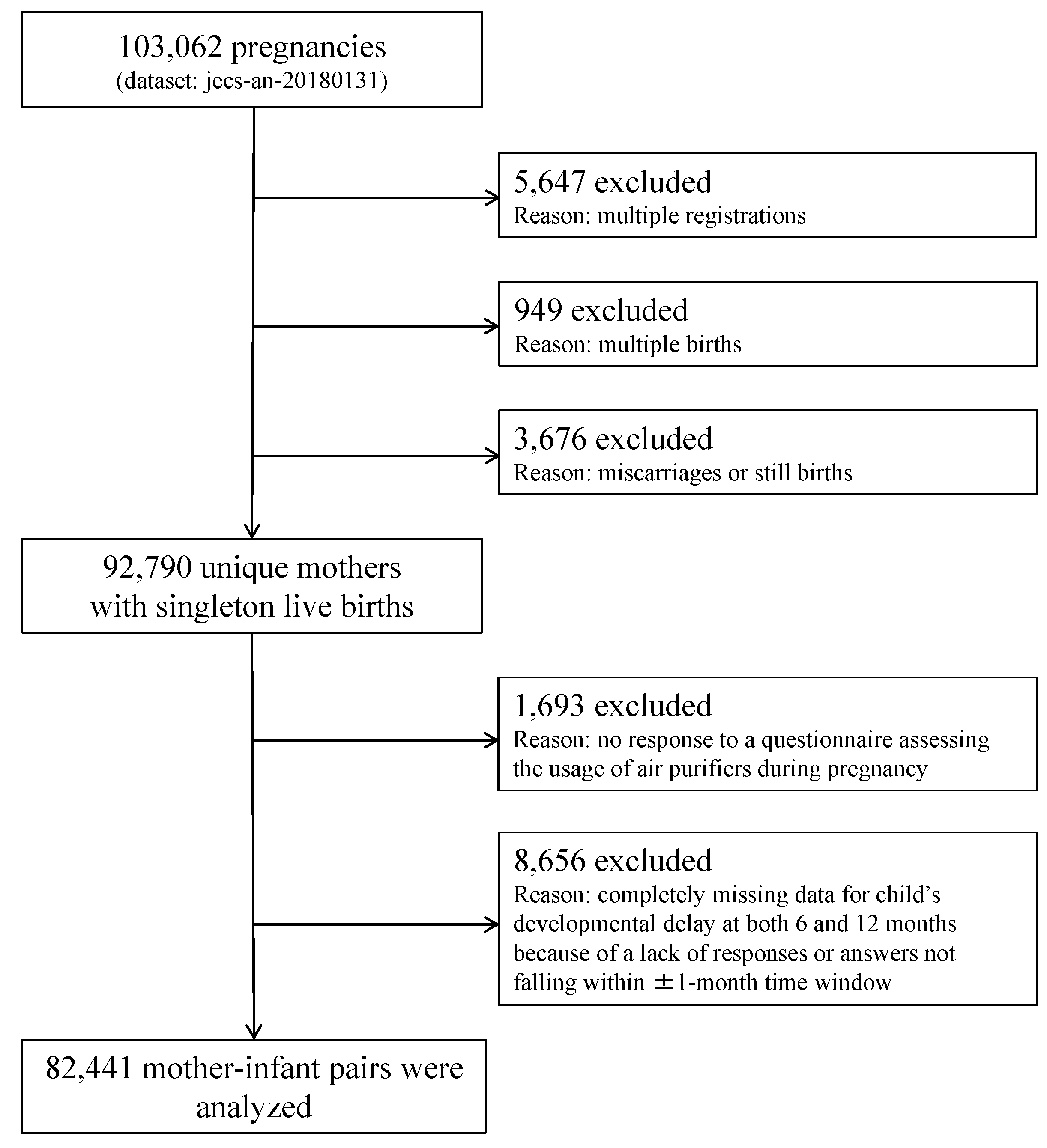
2.1. Study Design and Participants
2.2. Measures
2.2.1. Exposure
2.2.2. Outcomes
2.2.3. Covariates
2.3. Statistical Analysis
2.4. Missing Data
2.5. Sensitivity Analysis
3. Results
3.1. Backgrounds
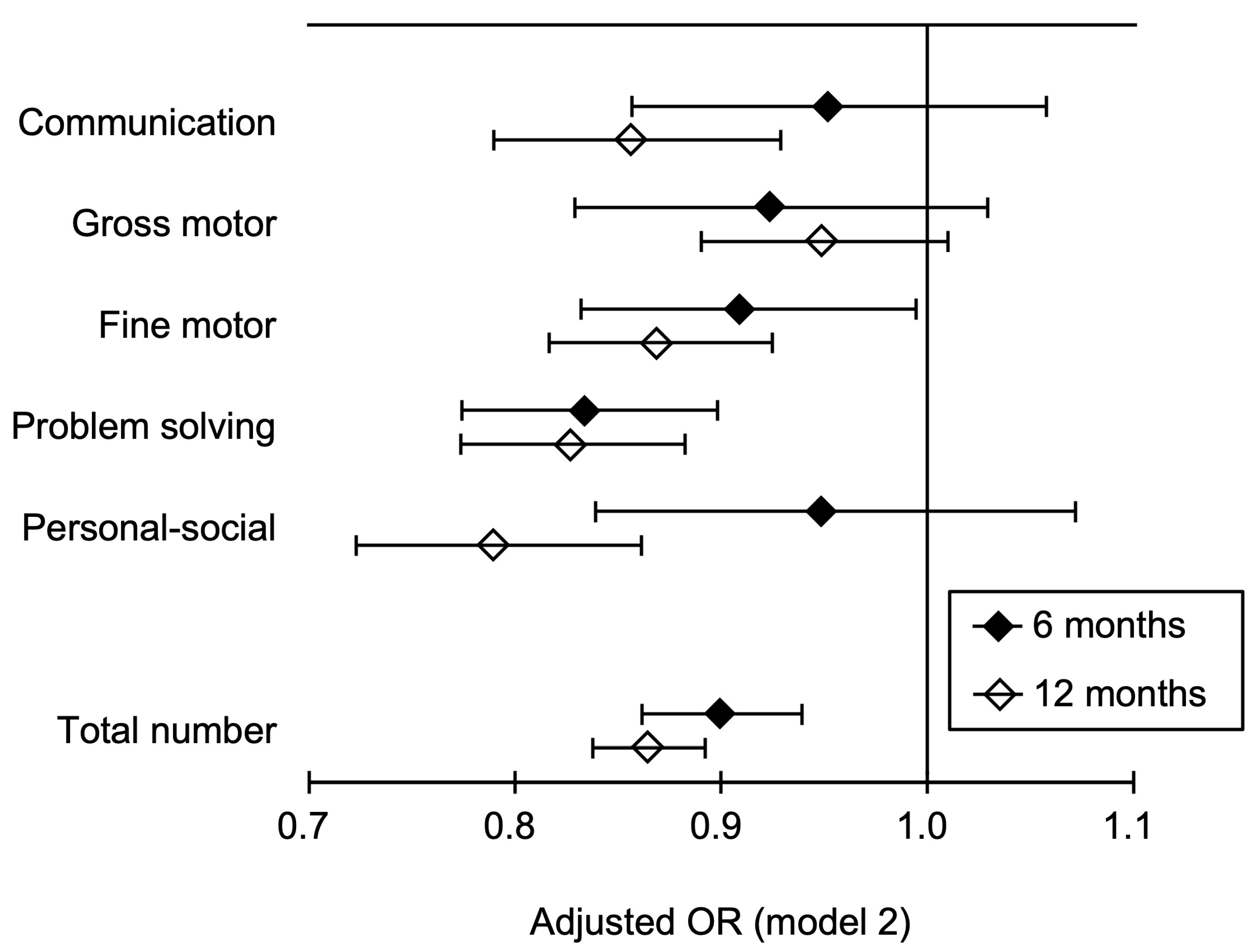
3.2. Main Results
3.3. Results of Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Balde, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef] [Green Version]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Landrigan, P.J. Air pollution and health. Lancet Public Health 2017, 2, E4–E5. [Google Scholar] [CrossRef] [Green Version]
- Suades-Gonzalez, E.; Gascon, M.; Guxens, M.; Sunyer, J. Air pollution and neuropsychological development: A review of the latest evidence. Endocrinology 2015, 156, 3473–3482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brockmeyer, S.; D’Angiulli, A. How air pollution alters brain development: The role of neuroinflammation. Transl. Neurosci. 2016, 7, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Morawska, L.; Ayoko, G.A.; Bae, G.N.; Buonanno, G.; Chao, C.Y.H.; Clifford, S.; Fu, S.C.; Hanninen, O.; He, C.; Isaxon, C.; et al. Airborne particles in indoor environment of homes, schools, offices and aged care facilities: The main routes of exposure. Environ. Int. 2017, 108, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Guxens, M.; Lubczynska, M.J.; Muetzel, R.L.; Dalmau-Bueno, A.; Jaddoe, V.W.V.; Hoek, G.; Van der Lugt, A.; Verhulst, F.C.; White, T.; Brunekreef, B.; et al. Air pollution exposure during fetal life, brain morphology, and cognitive function in school-age children. Biol. Psychiatry 2018, 84, 295–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, F.P.; Li, Z.G.; Whyatt, R.; Hoepner, L.; Wang, S.A.; Camann, D.; Rauh, V. Prenatal airborne polycyclic aromatic hydrocarbon exposure and child IQ at age 5 years. Pediatrics 2009, 124, E195–E202. [Google Scholar] [CrossRef] [Green Version]
- Guxens, M.; Garcia-Esteban, R.; Giorgis-Allemand, L.; Forns, J.; Badaloni, C.; Ballester, F.; Beelen, R.; Cesaroni, G.; Chatzi, L.; de Agostini, M.; et al. Air pollution during pregnancy and childhood cognitive and psychomotor development: Six European birth cohorts. Epidemiology 2014, 25, 636–647. [Google Scholar] [CrossRef] [Green Version]
- Rice, D.; Barone, S., Jr. Critical periods of vulnerability for the developing nervous system: Evidence from humans and animal models. Environ. Health Perspect. 2000, 108 (Suppl. 3), 511–533. [Google Scholar] [CrossRef]
- Grandjean, P.; Landrigan, P.J. Neurobehavioural effects of developmental toxicity. Lancet Neurol. 2014, 13, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Calderon-Garciduenas, L.; Mora-Tiscareno, A.; Ontiveros, E.; Gomez-Garza, G.; Barragan-Mejia, G.; Broadway, J.; Chapman, S.; Valencia-Salazar, G.; Jewells, V.; Maronpot, R.R.; et al. Air pollution, cognitive deficits and brain abnormalities: A pilot study with children and dogs. Brain Cogn. 2008, 68, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Maher, B.A.; Ahmed, I.A.; Karloukovski, V.; MacLaren, D.A.; Foulds, P.G.; Allsop, D.; Mann, D.M.; Torres-Jardon, R.; Calderon-Garciduenas, L. Magnetite pollution nanoparticles in the human brain. Proc. Natl. Acad. Sci. USA 2016, 113, 10797–10801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fermo, P.; Comite, V.; Falciola, L.; Guglielmi, V.; Miani, A. Efficiency of an Air Cleaner Device in Reducing Aerosol Particulate Matter (PM) in Indoor Environments. Int. J. Environ. Res. Public Health 2019, 17, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanatani, K.T.; Okumura, M.; Tohno, S.; Adachi, Y.; Sato, K.; Nakayama, T. Indoor particle counts during Asian dust events under everyday conditions at an apartment in Japan. Environ. Health Prev. Med. 2014, 19, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia-Ying, L.; Zhao, C.; Jia-Jun, G.; Zi-Jun, G.; Xiao, L.; Bao-Qing, S. Efficacy of air purifier therapy in allergic rhinitis. Asian Pac. J. Allergy Immunol. 2018, 36, 217–221. [Google Scholar] [CrossRef]
- Kawamoto, T.; Nitta, H.; Murata, K.; Toda, E.; Tsukamoto, N.; Hasegawa, M.; Yamagata, Z.; Kayama, F.; Kishi, R.; Ohya, Y.; et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Michikawa, T.; Nitta, H.; Nakayama, S.F.; Yamazaki, S.; Isobe, T.; Tamura, K.; Suda, E.; Ono, M.; Yonemoto, J.; Iwai-Shimada, M.; et al. Baseline profile of participants in the Japan Environment and Children’s Study (JECS). J. Epidemiol. 2018, 28, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Iwai-Shimada, M.; Nakayama, S.F.; Isobe, T.; Michikawa, T.; Yamazaki, S.; Nitta, H.; Takeuchi, A.; Kobayashi, Y.; Tamura, K.; Suda, E.; et al. Questionnaire results on exposure characteristics of pregnant women participating in the Japan Environment and Children Study (JECS). Environ. Health Prev. Med. 2018, 23, 45. [Google Scholar] [CrossRef]
- Squires, J.; Bricker, D. Ages & Stages Questionnaires (ASQ-3): A Parent-Completed Child-Monitoring System, 3rd ed.; Paul H Brookes Publishing Company: Baltimore, MD, USA, 2009. [Google Scholar]
- Korfmacher, J.; Chawla, N. Toolkit of Recommended Curricula and Assessments for Early Childhood Home Visiting. Geneva: UNICEF. Available online: https://www.unicef.org/eca/sites/unicef.org.eca/files/2017-11/Toolkit_of_Recommended_Curricula_and_Assessments_for_Home_Visiting_0.pdf (accessed on 26 April 2020).
- Gao, Y.; Sheng, C.; Xie, R.H.; Sun, W.; Asztalos, E.; Moddemann, D.; Zwaigenbaum, L.; Walker, M.; Wen, S.W. New perspective on impact of folic acid supplementation during pregnancy on neurodevelopment/autism in the offspring children—A systematic review. PLoS ONE 2016, 11, e0165626. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, T.; Michikawa, T.; Suzuki, K.; Takebayashi, T.; Yamagata, Z. Impact of high-rise living on children’s development and health: A critical review of literature. Yamanashi Med. J. 2014, 29, 1–9. [Google Scholar]
- Hamazaki, K.; Takamori, A.; Tsuchida, A.; Kigawa, M.; Tanaka, T.; Ito, M.; Adachi, Y.; Saito, S.; Origasa, H.; Inadera, H.; et al. Dietary intake of fish and n-3 polyunsaturated fatty acids and risks of perinatal depression: The Japan Environment and Children’s Study (JECS). J. Psychiatr. Res. 2018, 98, 9–16. [Google Scholar] [CrossRef]
- Matsumura, K.; Hamazaki, K.; Tsuchida, A.; Kasamatsu, H.; Inadera, H. Education level and risk of postpartum depression: Results from the Japan Environment and Children’s Study (JECS). BMC Psychiatry 2019, 19, 419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Buuren, S. Multiple imputation of discrete and continuous data by fully conditional specification. Stat. Methods Med Res. 2007, 16, 219–242. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley and Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- Guyton, A.C.; Hall, J.E. Human Physiology and Mechanisms of Disease, 6th ed.; Saunders: Philadelphia, PA, USA, 1996. [Google Scholar]
- Miller, E.K.; Cohen, J.D. An integrative theory of prefrontal cortex function. Annu. Rev. Neurosci. 2001, 24, 167–202. [Google Scholar] [CrossRef]
- Itazawa, T.; Kanatani, K.T.; Hamazaki, K.; Inadera, H.; Tsuchida, A.; Tanaka, T.; Nakayama, T.; Go, T.; Onishi, K.; Kurozawa, Y.; et al. The impact of exposure to desert dust on infants’ symptoms and countermeasures to reduce the effects. Allergy 2020, 75, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Martinez, D.; Aguilera, I.; Bustamante, M.; Ballester, F.; Estarlich, M.; Fernandez-Somoano, A.; Guxens, M.; Lertxundi, N.; Martinez, M.D.; et al. Indoor air pollution from gas cooking and infant neurodevelopment. Epidemiology 2012, 23, 23–32. [Google Scholar] [CrossRef]
- Perera, F.P.; Rauh, V.; Tsai, W.Y.; Kinney, P.; Camann, D.; Barr, D.; Bernert, T.; Garfinkel, R.; Tu, Y.H.; Diaz, D.; et al. Effects of transplacental exposure to environmental pollutants on birth outcomes in a multiethnic population. Environ. Health Perspect. 2003, 111, 201–205. [Google Scholar] [CrossRef]
- Peterson, B.S.; Rauh, V.A.; Bansal, R.; Hao, X.; Toth, Z.; Nati, G.; Walsh, K.; Miller, R.L.; Arias, F.; Semanek, D.; et al. Effects of prenatal exposure to air pollutants (polycyclic aromatic hydrocarbons) on the development of brain white matter, cognition, and behavior in later childhood. JAMA Psychiatry 2015, 72, 531–540. [Google Scholar] [CrossRef]
- Ma, Y.; Harrad, S. Spatiotemporal analysis and human exposure assessment on polycyclic aromatic hydrocarbons in indoor air, settled house dust, and diet: A review. Environ. Int. 2015, 84, 7–16. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Category | Air-purifier Usage | |||
|---|---|---|---|---|---|
| Yes | No | ||||
| n (%) | n (%) | ||||
| Overall | 41,883 | (50.8) | 40,558 | (49.2) | |
| Mothers Age, years | <25 | 3661 | (8.8) | 4468 | (11.1) |
| 25–<30 | 12,184 | (29.2) | 11,166 | (27.6) | |
| 30–<35 | 15,379 | (36.9) | 13,840 | (34.3) | |
| ≥35 | 10,500 | (25.2) | 10,937 | (27.1) | |
| Body mass index, kg/m2 | <18.5 | 6748 | (16.2) | 6525 | (16.2) |
| 18.5–<25 | 30,945 | (74.2) | 29,576 | (73.2) | |
| ≥25 | 4017 | (9.6) | 4287 | (10.6) | |
| Parity | Primipara | 17,050 | (40.9) | 19,429 | (48.1) |
| Multipara | 24,668 | (59.1) | 20,968 | (51.9) | |
| Smoking status | Never | 24,257 | (58.5) | 23,708 | (59.1) |
| Former | 15,687 | (37.9) | 14,586 | (36.4) | |
| Current | 1492 | (3.6) | 1797 | (4.5) | |
| Passive smoking status | Almost never | 26,477 | (63.6) | 25,004 | (62.0) |
| Once a week | 5109 | (12.3) | 4731 | (11.7) | |
| 2–3 times a week | 3320 | (8.0) | 3341 | (8.3) | |
| 4–6 times a week | 1906 | (4.6) | 2044 | (5.1) | |
| Everyday | 4818 | (11.6) | 5194 | (12.9) | |
| Alcohol intake | Never | 13,816 | (33.4) | 13,455 | (33.5) |
| Former | 26,532 | (64.1) | 25,492 | (63.5) | |
| Current | 1050 | (2.5) | 1195 | (3.0) | |
| Number of hours spent outdoors | <1 | 7310 | (18.2) | 7782 | (20.1) |
| 1–<2 | 19,451 | (48.4) | 18,464 | (47.7) | |
| 2–<3 | 6579 | (16.4) | 5864 | (15.1) | |
| ≥3 | 6882 | (17.1) | 6631 | (17.1) | |
| Physical activity | No | 8929 | (22.1) | 9334 | (23.9) |
| Yes | 31,485 | (77.9) | 29,787 | (76.1) | |
| Quintile of folic acid intake, μg | ≤151 | 7508 | (18.0) | 8486 | (21.0) |
| 152–202 | 8303 | (19.9) | 8159 | (20.2) | |
| 203–256 | 8627 | (20.7) | 7982 | (19.8) | |
| 257–337 | 8641 | (20.7) | 7988 | (19.8) | |
| ≥338 | 8649 | (20.7) | 7792 | (19.3) | |
| Marital status | Married | 40,131 | (96.8) | 37,838 | (94.5) |
| Single | 1080 | (2.6) | 1786 | (4.5) | |
| Divorced or widowed | 233 | (0.6) | 409 | (1.0) | |
| Highest education level, years | ≤12 | 13,469 | (32.4) | 15,275 | (37.9) |
| 12–<16 | 18,555 | (44.6) | 16,286 | (40.4) | |
| ≥16 | 9554 | (23.0) | 8710 | (21.6) | |
| Employed | No | 19,197 | (46.3) | 17,860 | (44.6) |
| Yes | 22,272 | (53.7) | 22,214 | (55.4) | |
| Annual household income, million yen | <4 | 13,798 | (35.3) | 16,430 | (43.8) |
| 4–<6 | 13,593 | (34.8) | 11,922 | (31.8) | |
| ≥6 | 11,697 | (29.9) | 9150 | (24.4) | |
| Dwelling environment type of residence | |||||
| Wooden detached house | 17,390 | (41.9) | 16,338 | (40.6) | |
| Steel-frame detached house | 2936 | (7.1) | 2240 | (5.6) | |
| Wooden multiple dwelling house/apartment | 4780 | (11.5) | 5285 | (13.2) | |
| Steel-frame multiple dwelling house/apartment | 16,032 | (38.6) | 15,943 | (39.7) | |
| Other | 390 | (0.9) | 393 | (1.0) | |
| High-rise living | No | 39,609 | (94.9) | 38,766 | (95.9) |
| Yes | 2122 | (5.1) | 1646 | (4.1) | |
| Number of rooms in the house/apartment | ≤2 | 6990 | (16.8) | 8422 | (20.9) |
| 3 | 13,212 | (31.8) | 13,240 | (32.9) | |
| 4 | 8559 | (20.6) | 7019 | (17.5) | |
| 5 | 6673 | (16.1) | 5602 | (13.9) | |
| ≥6 | 6096 | (14.7) | 5935 | (14.8) | |
| Materials covering the floor of the living room | Tatami (Japanese straw floor covering) | 3893 | (9.4) | 5400 | (13.4) |
| Carpet on tatami | 3237 | (7.8) | 4047 | (10.1) | |
| Wooden flooring / tiles | 15,606 | (37.5) | 13,470 | (33.4) | |
| Carpet on wooden flooring/tiles | 18,080 | (43.5) | 16,675 | (41.4) | |
| Other | 798 | (1.9) | 685 | (1.7) | |
| Age of house/apartment building, years | <1 | 2706 | (6.5) | 1943 | (4.8) |
| 1–<3 | 5450 | (13.1) | 3792 | (9.4) | |
| 3–<5 | 4353 | (10.5) | 3426 | (8.5) | |
| 5–<10 | 6799 | (16.4) | 5885 | (14.7) | |
| 10–<20 | 9472 | (22.8) | 9575 | (23.8) | |
| ≥20 | 9433 | (22.7) | 11,071 | (27.6) | |
| Unknown | 3289 | (7.9) | 4480 | (11.2) | |
| House renovation/interior completion after becoming pregnant | No | 40,092 | (96.5) | 39,035 | (97.1) |
| Yes | 1435 | (3.5) | 1164 | (2.9) | |
| Number of years living in the current place of residence | <1 | 2753 | (6.8) | 2691 | (6.9) |
| 1–<3 | 17,758 | (43.8) | 16,714 | (42.7) | |
| 3–<5 | 9581 | (23.6) | 8469 | (21.6) | |
| 5–<10 | 7121 | (17.6) | 7057 | (18.0) | |
| 10–<20 | 1936 | (4.8) | 2336 | (6.0) | |
| ≥20 | 1433 | (3.5) | 1868 | (4.8) | |
| Prevalence | Cases | Total | Crude | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|---|---|---|
| % | n | n | OR | [95% CI] | OR | [95% CI] | OR | [95% CI] | |
| 6 months | |||||||||
| Communication | |||||||||
| AP use | 1.90 | 797 | 41,883 | 0.97 | [0.88, 1.08] | 0.95 | [0.85, 1.05] | 0.95 | [0.86, 1.06] |
| AP nonuse | 1.95 | 791 | 40,558 | Reference | Reference | Reference | |||
| Gross motor | |||||||||
| AP use | 1.75 | 734 | 41,883 | 0.92 | [0.83, 1.03] | 0.93 | [0.83, 1.03] | 0.92 | [0.83, 1.03] |
| AP nonuse | 1.92 | 778 | 40,558 | Reference | Reference | Reference | |||
| Fine motor | |||||||||
| AP use | 2.58 | 1080 | 41,883 | 0.94 | [0.86, 1.02] | 0.91 | [0.83, 0.99] | 0.91 | [0.83, 0.99] |
| AP nonuse | 2.76 | 1120 | 40,558 | Reference | Reference | Reference | |||
| Problem solving | |||||||||
| AP use | 3.48 | 1460 | 41,883 | 0.83 | [0.77, 0.89] | 0.83 | [0.77, 0.90] | 0.83 | [0.77, 0.90] |
| AP nonuse | 4.18 | 1694 | 40,558 | Reference | Reference | Reference | |||
| Personal–social | |||||||||
| AP use | 1.43 | 598 | 41,883 | 0.97 | [0.86, 1.09] | 0.94 | [0.83, 1.06] | 0.95 | [0.84, 1.07] |
| AP nonuse | 1.48 | 598 | 40,558 | Reference | Reference | Reference | |||
| 12 months | |||||||||
| Communication | |||||||||
| AP use | 2.97 | 1245 | 41,883 | 0.83 | [0.77, 0.90] | 0.86 | [0.79, 0.93] | 0.86 | [0.79, 0.93] |
| AP nonuse | 3.50 | 1419 | 40,558 | Reference | Reference | Reference | |||
| Gross motor | |||||||||
| AP use | 5.31 | 2222 | 41,883 | 0.95 | [0.89, 1.01] | 0.95 | [0.89, 1.01] | 0.95 | [0.89, 1.01] |
| AP nonuse | 5.59 | 2267 | 40,558 | Reference | Reference | Reference | |||
| Fine motor | |||||||||
| AP use | 5.13 | 2148 | 41,883 | 0.86 | [0.81, 0.91] | 0.87 | [0.81, 0.92] | 0.87 | [0.82, 0.92] |
| AP nonuse | 5.96 | 2418 | 40,558 | Reference | Reference | Reference | |||
| Problem solving | |||||||||
| AP use | 4.49 | 1879 | 41,883 | 0.78 | [0.74, 0.84] | 0.82 | [0.77, 0.88] | 0.83 | [0.77, 0.88] |
| AP nonuse | 5.65 | 2291 | 40,558 | Reference | Reference | Reference | |||
| Personal–social | |||||||||
| AP use | 2.65 | 1108 | 41,883 | 0.80 | [0.73, 0.87] | 0.79 | [0.72, 0.86] | 0.79 | [0.72, 0.86] |
| AP nonuse | 3.27 | 1326 | 40,558 | Reference | Reference | Reference | |||
| Mean | SD | Crude | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|---|---|
| OR | [95% CI] | OR | [95% CI] | OR | [95% CI] | |||
| 6 months | ||||||||
| AP use | 0.11 ± | 0.43 | 0.91 | [0.87, 0.95] | 0.90 | [0.86, 0.94] | 0.90 | [0.86, 0.94] |
| AP nonuse | 0.12 ± | 0.45 | Reference | Reference | Reference | |||
| 12 months | ||||||||
| AP use | 0.21 ± | 0.60 | 0.85 | [0.82, 0.87] | 0.86 | [0.84, 0.89] | 0.86 | [0.84, 0.89] |
| AP nonuse | 0.24 ± | 0.65 | Reference | Reference | Reference | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumura, K.; Hamazaki, K.; Tsuchida, A.; Inadera, H.; The Japan Environment and Children’s Study (JECS) Group. Prospective Association of Air-Purifier Usage during Pregnancy with Infant Neurodevelopment: A Nationwide Longitudinal Study—Japan Environment and Children’s Study (JECS). J. Clin. Med. 2020, 9, 1924. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061924
Matsumura K, Hamazaki K, Tsuchida A, Inadera H, The Japan Environment and Children’s Study (JECS) Group. Prospective Association of Air-Purifier Usage during Pregnancy with Infant Neurodevelopment: A Nationwide Longitudinal Study—Japan Environment and Children’s Study (JECS). Journal of Clinical Medicine. 2020; 9(6):1924. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061924
Chicago/Turabian StyleMatsumura, Kenta, Kei Hamazaki, Akiko Tsuchida, Hidekuni Inadera, and The Japan Environment and Children’s Study (JECS) Group. 2020. "Prospective Association of Air-Purifier Usage during Pregnancy with Infant Neurodevelopment: A Nationwide Longitudinal Study—Japan Environment and Children’s Study (JECS)" Journal of Clinical Medicine 9, no. 6: 1924. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061924